
Helpful but Spooky? Acceptance of AAL-systems Contrasting User
Groups with Focus on Disabilities and Care Needs
Julia van Heek, Simon Himmel and Martina Ziefle
Human-Computer Interaction Center, RWTH Aachen, Campus-Boulevard 57, 52064 Aachen, Germany
Keywords: Ambient Assisted Living, Technology Acceptance, User Diversity, Age, Needs of Care, Needs of
Assistance, Disabled People.
Abstract: Ambient Assisted Living (AAL) technologies present one approach facing the challenges of recent and
rising care needs due to demographic changes in western societies. Beside the technological implementa-
tion, the focus on user acceptance of all stakeholders plays a major role for a successful rollout. As most re-
search deals with age-related issues, this paper emphasizes especially on the sector of disabled persons. In a
qualitative interview pre-study (n=9) and a validating questionnaire study (n=279) the perceived benefits
and barriers of AAL technologies were contrasted in four user groups: healthy “not-experienced” people,
disabled, their relatives, and professional care givers. Results indicate that disabled and care-needy people
show a higher acceptance and intention to use an AAL system than “not-experienced” people or care givers
and that the motives for use and non-use differ strongly with regard to user diversity as well. The results
show the importance to integrate diverse user groups (age, disabilities) into the design and evaluation pro-
cess of AAL technologies.
1 INTRODUCTION
Demographic change represents one of the major
challenges for today’s society. A constantly increas-
ing number of older people and people in need of
care poses exceptional burdens for the care sector
(Bloom & Canning, 2004; Walker & Maltby, 2012).
Concurrently, in particular most of the older people
desire to live at their own home as long as possible
and as autonomously as possible (Wiles et al., 2011).
Age and age-related diseases (e.g., diabetes, de-
mentia, cardiovascular diseases) are enormously
important and increase steadily (Shaw et al., 2010;
Wild et al., 2004; Roger et al., 2011), but represent
only one side of the coin. Age-independent diseases
and disabilities are also of importance and should be
considered as they cause huge needs of care and
assistance as well (Geenen et al., 2003). Additional-
ly, there is the comparably new phenomenon of “old
disabled” people, on the one hand, due to medical
and technical developments in healthcare concerning
new innovative medicines and therapies. On the
other hand, especially in Europe - due to the specific
historical background of euthanasia offenses, in
which disabled people were systematically aborted,
deported, and even murdered (Poore, 2007).
Hence, age, diseases, and disabilities are all rele-
vant factors that have to be considered with regard to
increasing needs of care and related challenges. In
the last decades it is tried to face these challenges
developing various technical single-case solutions
but also complex ambient assisted living systems
(AAL) (Schmitt, 2002).
A huge amount of systems exist that monitor
medical parameters or detect falls as well as facili-
tate living at home using smart home technology
elements (Cheng et al., 2013; Baig & Gholamhos-
seini, 2013; Rashidi & Mihailidis, 2013). Beyond
multiply available single solutions, current research
focuses also on holistic AAL systems, that combine
various functions and are ideally cost-effective,
retrofittable, and adaptable to the individual needs of
diverse user groups.
In particular with regard to different user groups,
the question arises whether and to which extent such
AAL systems are desired and accepted. Which fac-
tors are crucial for acceptance and to what extent
does this evaluation depend on user factors?
Several studies investigate the acceptance of
such and similar technologies focussing on age (e.g.,
Fuchsberger, 2008; Demiris et al. 2008) or gender
(Wilkowska et al., 2010) as presumed influencing
78
Heek, J., Himmel, S. and Ziefle, M.
Helpful but Spooky? Acceptance of AAL-systems Contrasting User Groups with Focus on Disabilities and Care Needs .
DOI: 10.5220/0006325400780090
In Proceedings of the 3rd International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2017), pages 78-90
ISBN: 978-989-758-251-6
Copyright © 2017 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

factors. As disabled people have hardly been consid-
ered so far, this paper investigates the acceptance of
AAL systems with focus on people having experi-
ences with disabilities in different perspectives.
2 AAL & ACCEPTANCE
First, the state of the art concerning AAL technolo-
gies is shortly summarized. Afterwards, the theoreti-
cal background of technology acceptance research is
presented focusing on the influence of user diversity
factors. Further, an overview of current acceptance
research on AAL systems is given.
2.1 AAL Technologies
The use of Information and Communication Tech-
nologies (ICT) in everyday life has been studied
since the 1980s (Silverstone et al., 1989). Different
types of monitoring are enabled by integrating ICT
(e.g., microphones, cameras, and movement sensors)
into people’s living environments. In recent years,
the number of commercially available AAL systems
as well as AAL research projects increased signifi-
cantly. In this context, retrofittable, modularly con-
structed (as required), and multifunctional systems
are offered including -among others - smart home
functions (such as sensors for control of lighting,
heating, doors, and windows), fall detection, and
other health care applications like providing of and
reminder for drugs or blood sugar measuring. These
systems are available for an integration in the home
environment (e.g., Casenio, 2016; Essence, 2016), in
hospitals (EarlySense, 2016), and in nursing homes
(Tunstall, 2016).
Besides commercial solutions, research projects
also focus on the development of holistic AAL sys-
tems (e.g., Sixsmith et al., 2009; Gövercin et al.,
2016). However, in contrast to most of the commer-
cial solutions, these projects attach importance to
consider future users (mainly older people) iterative-
ly in the development process of the AAL system
(Kleinberger et al., 2007). This is of significance in
as much as the user’s perspective is decisive for a
successful integration of AAL systems in their eve-
ryday life. Currently, AAL technologies are not
widely integrated in private home environments,
although they have the potential to facilitate the
everyday life of older, diseased, or disabled people.
To understand the barriers of AAL usage, we have
to focus on potential users of these systems, their
perception, ideas, wishes, and their willingness to
adopt home-integrated ICT.
2.2 Technology Acceptance, User Di-
versity & AAL Systems
AAL technologies as a possible solution for the
challenges of the demographic change were mostly
perceived and evaluated positive and the necessity
and usefulness of technical support were also highly
acknowledged (Beringer et al., 2011; Gövercin et al.,
2016). In particular, the opportunity of staying long-
er at the own home and an independent life are
strong motives to use (or imagine to use) an AAL
system. On the other hand, restraints and acceptance
barriers such as feelings of isolation (e.g., Sun et al.,
2010), feelings of surveillance, and invasion of pri-
vacy (e.g., Wilkowska et al., 2015) were frequently
mentioned when asking people to think about a
concrete implementation of an AAL system in their
living environment.
To understand this trade-off it is necessary to
consider both user diversity and technology ac-
ceptance. In the last years, research became more
aware of the limited suitability of traditional tech-
nology acceptance models like TAM or UTAUT as -
in contrast to conventional ICT - AAL systems ad-
dress especially older, diseased, and frail people
with individual requirements, wishes, and concerns
(Kowalewski et al., 2012). We assume that this con-
currently leads to a different weighting of important
perceived benefits and barriers and a different ac-
ceptance of using an AAL system. Therefore, an
overview of acceptance research findings focusing
on user diversity and different user group perspec-
tives is presented.
2.2.1 Factor Age
The benefits and barriers of AAL technologies for
elderly are widely discussed and researched in the
last decade. To understand the perception of AAL
technologies, numerous focus groups (Demiris et al.,
2004; Ziefle et al., 2011) and interviews (Beringer et
al., 2011) with people aged above 60 show similar
results: elderly remark the benefits of staying at
home longer, understand the imminent lack of care
nurses and the chances of AAL technologies. On the
other side, they fear dependency on technologies
they cannot control, the lack of personal contact,
demur data and privacy concerns. Plentiful surveys
verify these qualitative gained results over time
(e.g., Himmel & Ziefle, 2016). However, the meas-
urement of attitudes towards technologies strongly
depends on the research method and hands-on expe-
rience in real-life scenarios is inevitable to under-
stand older peoples’ actual approach to AAL tech-
Helpful but Spooky? Acceptance of AAL-systems Contrasting User Groups with Focus on Disabilities and Care Needs
79

nologies (Wilkowska et al., 2015). While several
projects for ambient intelligence and ubiquitous
computing in smart homes focused mainly on the
technological implementations, recent projects on
AAL labs, e.g., Philips Research CareLab (de Ruyter
& Pelgrim, 2007), SOPRANO (Sixsmith et al.,
2009), eHealth Future Care Lab (Brauner et al.,
2015), to mention but a few, have understood to
implement the user into the design and evaluation
circle. The role of acceptance, the influence of pri-
vacy and trust, especially of elderly users, is there-
fore extensively investigated.
2.2.2 Factors Diseases & Disabilities
While research for AAL technologies emphasized
on elderly people with age-related chronic or physi-
cal illnesses, the acceptance of AAL technologies
for disabled persons still needs more and specified
research attention. On the one hand, assistive tech-
nologies could improve the inclusion of people with
disabilities into society, supporting mobility, and
communication as well as holding down a job. On
the other hand, age-related illnesses come along with
already existing disabilities, which is as already
mentioned a quite new phenomenon (Poore, 2007).
Regarding the care sector, besides pediatric nurs-
ing, ageing, diseases, and disabilities are the three
central challenges. Frequently, age, diseases, and
disabilities are summed up and neither investigated
in depth nor separately. How different diseases and
disabilities affect the use of medical technology is
investigated and summarized in occasional studies
(e.g., Harris, 2010; Gentry, 2009). These studies try
to analyze why numerous existing technologies are
abandoned and lie unused. The problem is that re-
search on AAL technology acceptance of diseased or
disabled people is partly comparatively unspecific,
superficial, and on a theoretical level. We assume,
this is mainly due to the fact that especially disabled
people are considered and directly asked for their
opinions, whishes, and needs only in few cases.
However, this is precisely where research is re-
quired: especially disabled people have to be inte-
grated in the design of assistive technologies and the
interaction of age, diseases, and disabilities has to be
focused as these factors constitute the major part of
care needs.
To do especially justice to needs of care and care
in itself, the perspectives of professional care givers
or family care givers have to be considered as well.
Within the research landscape concerning AAL
technologies and their perception, some studies
examined the requirements and professional and
family caregivers’ perspectives on AAL systems and
technologies separately and not comparatively
(López et al., 2015; Mortenson et al., 2013). In these
studies, the effectiveness of different technologies is
focused and guidelines for design and implementa-
tion are derived. Single studies try to concentrate on
the user (care givers and patients) and perceived
concerns regarding in-home monitoring technologies
(Larizza et al., 2014). These studies deliver first
insights into different perspectives on the acceptance
of AAL technologies. However, they do not allow to
directly compare the perspectives of “patients” (old-
er, diseased, or disabled people) with family or pro-
fessional care givers and “not-experienced” people,
as they were each mainly focused on a specific user
group and no equivalent or comparable methodolog-
ical approach was used for the user groups.
So far, there is only little knowledge about the
acceptance of AAL technologies with regard to
disabled people and people with special care needs,
about the interaction of the described user factors
(age, diseases, and disabilities, needs in assistance
and care) as well as about the perspectives of differ-
ent user groups (affected themselves, relatives and
families of people need in care, professional care-
givers). Therefore, these interactions were addressed
in the present study.
3 METHOD
In this section, the research design is presented start-
ing with a short summary of the qualitative inter-
view study, which was taken as a basis for the sub-
sequent quantitative study. Afterwards, the empirical
design of the quantitative study and the sample’s
characteristics are detailed. We choose a multi-
method approach for this study consisting of a quali-
tative interview study and a consecutive quantitative
questionnaire study. Our study addresses three es-
sential research questions:
1. How do the participants evaluate a holistic AAL
system (see 3.3) and which perceived benefits
and barriers are most important for its ac-
ceptance?
2. To which extent do age, experiences with disa-
bilities, and current care needs influence the
AAL system’s evaluation?
3. Are different benefits and barriers decisive for
AAL acceptance depending on diverse user
group perspectives?
ICT4AWE 2017 - 3rd International Conference on Information and Communication Technologies for Ageing Well and e-Health
80

3.1 Research Design
As it was detailed in chapter 2, research on the ac-
ceptance of AAL technologies mostly focused on
older users so far. In contrast, there is only sparse
knowledge about developing AAL technologies for
people with disabilities and rarely research on the
acceptance of AAL technologies focusing on disa-
bled users. Further, other perspectives (e.g., profes-
sional caregivers, relatives, and families of disabled
people) are also of prime importance as they can
support and complete the understanding of potential
user’s needs and wishes. Hence, a qualitative inter-
view study was initially necessary to identify per-
ceived motives and barriers of use as well as use
conditions. Only based on these results it was rea-
sonable to design and conduct a quantitative study
focusing on people having experiences with disabili-
ties (themselves, families and relatives, professional
caregivers).
3.2 Qualitative Pre-study
A preceding interview study was conducted focusing
on people with disabilities (n=7), their relatives
(n=1), and a professional caregiver (n=1) and the
interviews took between 40 and 70 minutes. As the
quantitative study and results should be focused in
this paper (especially perceived benefits and barriers
of AAL systems), only the results of the qualitative
study are presented which were essential for the
conception of the quantitative questionnaire. With
regard to the described holistic AAL-system (scenar-
io similar as detailed in 3.3), the participants dis-
cussed 11 different benefits and 9 potential usage
barriers (Table 1).
These results align with previous research con-
cerning several aspects (e.g., comfort, facilitating
everyday life (e.g., Himmel et al., 2013)), but, to a
larger extent, the results are multifaceted and go
beyond previous findings due to the reference to
disabilities and constraints (e.g., compensation,
reduce confrontation with care needs, to be afraid of
isolation). Hence, these aspects have to be examined
quantitatively to be able to do justice to diverse user
groups.
Further, the participants evaluated the described
AAL system differently: the related person and the
caregiver assessed the scenario rather negative and
critical using words like spooky, lonely, inhuman,
not self-determined, and personal rights; in contrast,
the disabled participants associated it with more
positive and fascinated words such as exciting, luxu-
ry, very useful, helpful and comfortable. These re-
sults showed the importance of differentiating be-
tween different user groups and their considering in
the subsequent study.
Table 1: Overview of discussed benefits and potential
barriers of AAL systems in the interview study.
Perceived Benefits Potential Usage Barriers
Expansion of autonomy Isolation due to the substitution
of care staff by technologies
Reduction of dependency from
others
No real time savings (spend
more time on technology use)
Facilitating the everyday life Only if needed (doing as much
as possible autonomously)
Saving of time Missing relevance as care needs
are often too high
Comfort Functional incapacity (failure
of technology)
Reduction of confrontation with
own care needs
Feeling of surveillance
Increase the feeling of safety Too large proportion of tech-
nology in everyday life
Staying longer at the own home Expectation of a too complicat-
ed handling
Relief of family, relatives, and
caregivers
Transmission of false infor-
mation (e.g., false alarm)
Compensation of mobility
constraints
Enabling a fast data access
3.3 Questionnaire of Quantitative
Study
The questionnaire items were developed based on
the findings of the previous interview study. The
questionnaire consisted of different parts, while the
first part addressed demographic aspects, such as
age, gender, educational level, and income.
In the next part, the participants were asked for
their experiences with disabilities by indicating if
themselves are disabled (1), if they are related to a
disabled person (2), if they are the caregiver of a
disabled person (3), or if they have no experiences
with disabilities (4). Afterwards, the participants
were asked to indicate, whether and to which extent
(care time, type of care, intensity of care) themselves
(1+4) or the person they put themselves in position
with (2+3) is in need of care.
To ensure that all participants pertain to the same
baseline with regard to the evaluation of an AAL
technology, a scenario was designed. Depending on
their background (need of care, experience with
disabilities), the participants were introduced to the
scenario differently. For cases 2-4, the participants
were asked to put themselves in the / a disabled
person’s position (respectively the person they are
related with or they care (2+3)) while answering the
questions concerning the AAL scenario. Participants
who indicated to be not in need of care were asked
to imagine that they would be in need of care.
Helpful but Spooky? Acceptance of AAL-systems Contrasting User Groups with Focus on Disabilities and Care Needs
81

The scenario was designed as a very personal
everyday situation wherein the participants should
imagine that an specific, invisible AAL system was
integrated in their home environment and contained
the following functions: setting of the home temper-
ature (via smartphone), automatic opening and clos-
ing of (front) doors and windows (via sensors), au-
tomatic lighting control (via light sensors and posi-
tion localization), hands-free kit for phoning (inte-
grated microphones), monitoring of front door area
(via cameras), and fall detection (sensors in floor
and bed).
Afterwards, they had to evaluate a list of use
conditions, perceived benefits (11 items) of the AAL
system (e.g., to increase autonomy, to reduce de-
pendency on others, to facilitate everyday life, to
relieve fellow people), and perceived barriers (9
items) (e.g., feeling of surveillance, no trust in func-
tionality, to assume a too difficult usage, to be afraid
of isolation) based on the findings of the qualitative
interview study (see 3.2).
Following that, the participants should assess 8
statements regarding the acceptance or rejection of
the described AAL system as well as the behavioural
intention to use such an AAL system. All described
items had to be evaluated on six-point Likert scales
(1 = min: ”I strongly disagree”; 6 = max: “I strongly
agree”).
Finally, the participants were able to reason their
opinions towards the described AAL system on an
optional basis and to provide their feedback concern-
ing the questionnaire and the topic itself. Complet-
ing the questionnaire took on average 15 minutes
and data was collected in an online survey in Ger-
many. Overall, the questionnaire was made available
for 6 weeks in summer 2016.
3.4 Sample Description
A total of 279 participants volunteered to participate
in our questionnaire study, which was distributed
online in social network forums and acquired by
personal contact. Since only complete data sets
could be used for statistical analyses, a sample of
n=182 remained. The participants (62.1% female,
36.3% male, 1.6% no answer) were on average 38.7
years old (SD=13.95; min=20; max=81) and highly
educated with 46.7% holding a university degree
and 14.8% a university entrance diploma. Concern-
ing experience with disabilities, 51 participants indi-
cated to be disabled (28.0%), 12.1% (n=22) were
professional caregivers, 35 participants were rela-
tives of a disabled person (19.2%), and 40.7%
(n=74) had no experience with disabilities. Regard-
ing current needs of assistance and care, 79 (43.4%)
participants indicated to need care or that the person
- they put themselves in position with - needed care
(56.6% were not in need of care). These factors are
related only partially: age is not related with experi-
ence with disabilities (r=-.132; p=.075 >.05) nor
with current care needs (r=-.096; p=.197 >.05). In-
stead, age is related with gender (r=.200; p=.007
<.05; 1=female; 2=male). Not surprisingly, experi-
ence with disabilities correlates with current care
needs (r=.607; p=.000 <.05). Further, the partici-
pants reported to have on average a positive tech-
nical self-efficacy (M=4.5; SD=1.0; min=1; max=6)
and a slightly positive attitude towards technology
innovations (M=3.9; SD=1.0; min=1; max=6). Fur-
ther, they indicated their needs for data security
(M=4.1; SD=0.8; min=1; max=6) and privacy
(M=4.4; SD=0.7; min=1; max=6), which both were
on average positive.
4 RESULTS
Prior to descriptive and inference analyses, item
analyses were calculated to ensure measurement
quality. Cronbach’s alpha > 0.7 indicated a satisfy-
ing internal consistency of the scales. Data was ana-
lysed descriptively, by linear regression analyses
and, with respect to the effects of user diversity, by
(M)ANOVA procedures. The level of significance
was set at 5%.
To analyse the impact of need of assistance and
care on perceived benefits, barriers, and acceptance,
we choose the factors age, experience with disabili-
ties, and acute care needs for further analysis. The
results are structured as follows: first, the results for
acceptance of AAL, perceived benefits, and per-
ceived barriers were presented for the whole sample.
In a second step, the influences of user-specific
characteristics on the perception of benefits and
barriers as well as acceptance of AAL are examined.
4.1 General Acceptance of AAL
As it is shown in Figure 1, acceptance of AAL tech-
nologies was on average positive (M=4.6; SD=1.0).
In particular the items with regard to care needs
(…due to care needs (M=4.7; SD=1.1) and … re-
duce my care needs (M=4.5; SD=1.3) were evaluat-
ed highest. Three items concerning a concrete inten-
tion to use an AAL system were rated rather posi-
tive, while the item I would install… (M=4.3;
SD=1.4) was assessed higher than the aspects I like
ICT4AWE 2017 - 3rd International Conference on Information and Communication Technologies for Ageing Well and e-Health
82

to use… (M=4.0; SD=1.4) and I can imagine to
use…now (M=3.8; SD=1.6).
The three negative acceptance items were reject-
ed similarly (e.g., … AAL technologies are superflu-
ous (M=1.9; SD=1.1). As perceived benefits
(r=.433; p<.01) and perceived barriers (r=-.560;
p<.01) are both significantly related with ac-
ceptance, their evaluations are presented in detail for
the whole sample).
Figure 1: Evaluation of AAL system acceptance.
The evaluation of perceived benefits of the de-
scribed AAL system is shown in Figure 2 and obvi-
ously all aspects were assessed and perceived as
benefits as all values were above the mean of the
scale. The most important benefits were to facilitate
everyday life (M=5.2; SD=0.9), to expand own au-
tonomy (M=5.2; SD=1.0), to extend staying at home
(M=5.1; SD=1.0), and to reduce dependency from
other people (M=5.1; SD=1.0). The aspects to re-
lieve fellow people (M=4.9; SD=1.1), to compensate
reduced mobility (M=4.8; SD=1.0), comfort (M=4.7;
SD=1.2), and to increase the feeling of safety
(M=4.6; SD=1.3) were only little less important.
Comparatively, time savings (M=4.3; SD=1.4), to
enable fast data access (M=4.0; SD=1.4), and to
reduce own conflict with care needs (M=3.9;
SD=1.4) were minor important.
Besides the descriptive analysis of the perceived
benefits, we examined which benefits affect the
acceptance of the described AAL system the most.
Therefore, a stepwise linear regression analysis with
all perceived benefits as independent and the ac-
ceptance sum score as dependent variable was calcu-
lated and revealed two significant models for the
whole sample. The first model predicts 27.2% (adj.
r
2
=.272) variance of acceptance and is based on the
benefit “to expand own autonomy” (β = 0.525; t =
8.279; p < .000), which therefore is the most im-
portant beneficial aspect for the acceptance of this
study’s AAL system. The second model additionally
contains the aspect “time savings” and explains
+2.0% variance (adj. r
2
=.292). Thus “time savings”
Figure 2: Evaluation of benefits with regard to the de-
scribed AAL system scenario.
(β = 0.166; t = 2.459; p < .05) and “to expand the
autonomy” β = 0.462; t = 6.823; p < .000) are the
most important beneficial factors affecting the ac-
ceptance of the AAL system.
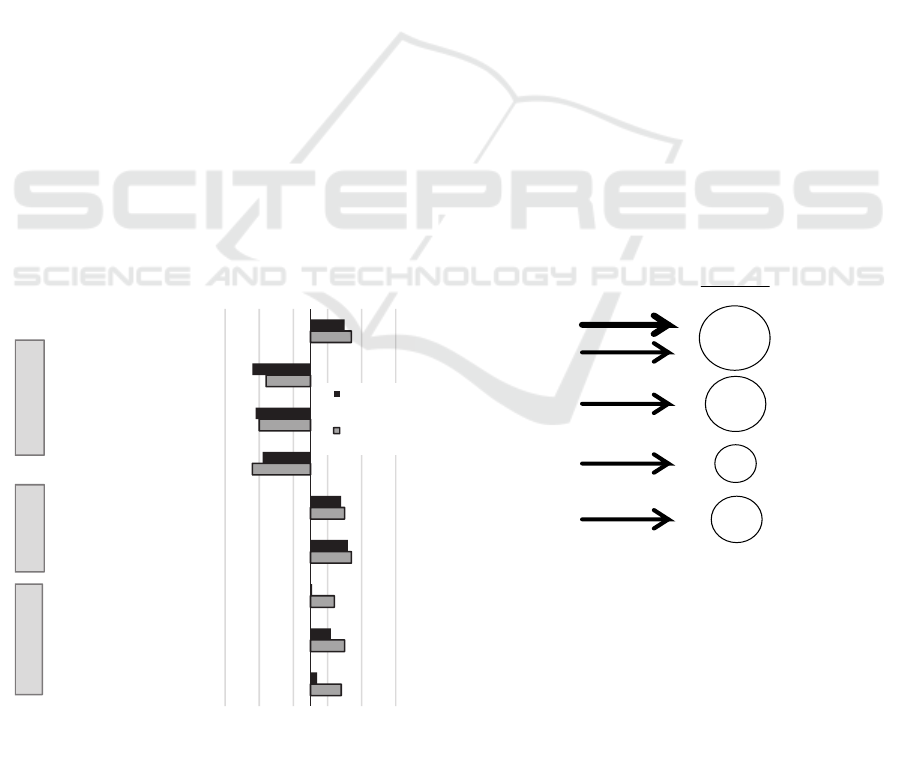
The evaluation of perceived barriers of the described
AAL system is shown in Figure 3. Apparently, none
of the items was perceived as “real” barrier as all
values were below the mean of the scale and thus,
the items were rejected to be barriers of AAL sys-
tems. AAL technologies were not perceived as su-
perfluous (M=1.9; SD=1.0) and irrelevant (M=2.4;
SD=1.1). The usage was not estimated to be too
difficult (M=2.6; SD=1.2) and the participants rather
rejected to have no trust in the functionality (M=2.8;
SD=1.3) of the AAL system. Further, the partici-
pants slightly rejected that the proportion of tech-
nology in everyday life is too high (M=3.0; SD=1.5)
and also to expect to have no “real” time savings
(M=2.9; SD=1.2). The aspect to be afraid of isola-
tion (M=3.2; SD=1.5) was also slightly rejected.
Transmission of incorrect information (M=3.4;
SD=1.3) and feeling of surveillance (M=3.4;
SD=1.5) were rather evaluated neutrally and there-
fore, they represented the most likely as barriers
perceived aspects.
1.9
2.0
2.0
3.8
4.0
4.3
4.5
4.7
4.6
123456
I think AAL technologies
are superfluous
I don´t like to have
AAL technologies in my home
I don´t see an advantage
in using AAL technologies
I can imagine to use
AAL technologies now
I like to use AAL
technologies
I would install AAL
technology/ies in my home
I would like to use
AAL technologies to reduce…
I can imagine to
use AAL technologies…
Acceptance of AAL
technologies
evaluation (min=1; max=6)
rejection agreement
negative positive
in case
of care
needs
3.9
4.0
4.2
4.6
4.7
4.8
4.9
5.1
5.1
5.2
5.2
123456
reduce own conflict with care needs
enable an fast data access
time saving
increase the feeling of safety
comfort
compensate reduced mobility
relieve fellow people
reduce dependency
extend staying at home
expand autonomy
facilitate everyday life
evaluation (min=1; max=6)
rejection agreement
Helpful but Spooky? Acceptance of AAL-systems Contrasting User Groups with Focus on Disabilities and Care Needs
83
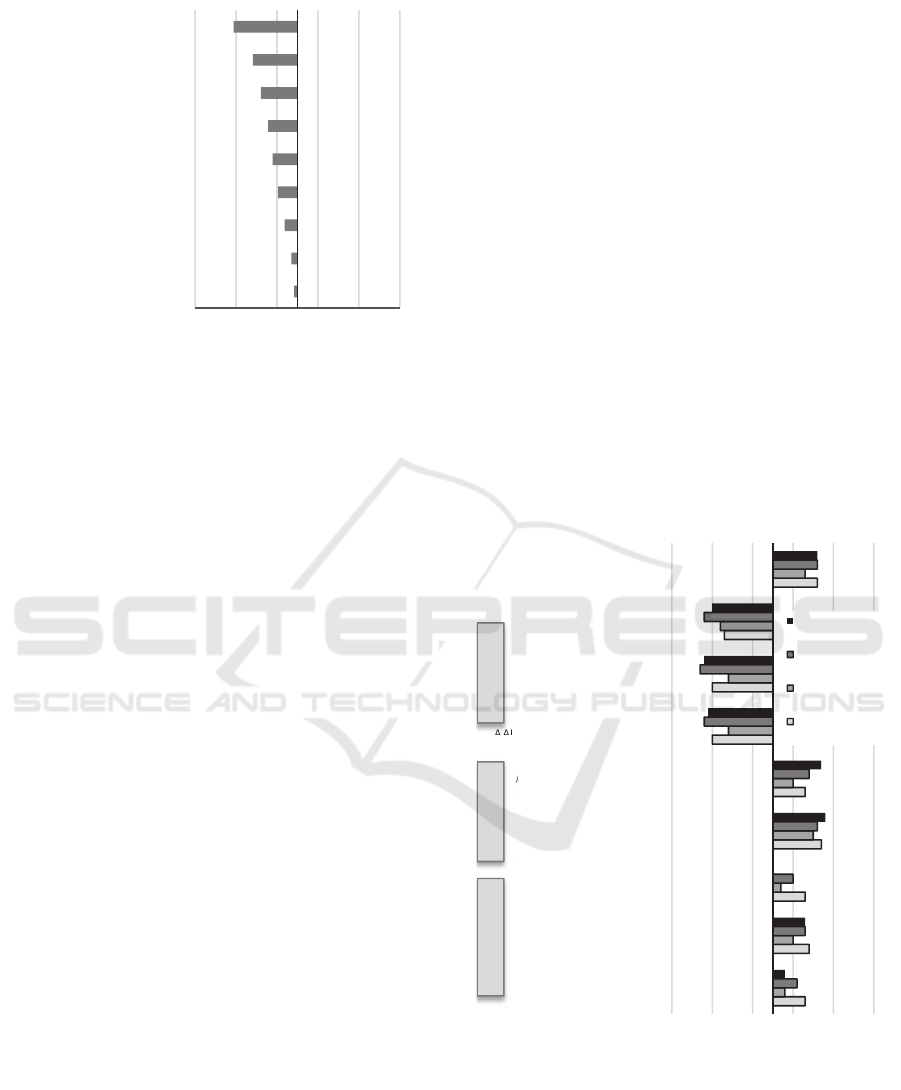
Figure 3: Evaluation of barriers with regard to the
described AAL scenario.
In addition to descriptive analyses, a stepwise
linear regression analysis with perceived barriers as
independent and the acceptance sum score as de-
pendent variable revealed three significant models
for the whole sample. The first model predicts
35.1% variance of the acceptance (adj. r
2
=.351)
based on the barrier “irrelevant” (β = -0.596; t = -
9.945; p < .000), i.e., this barrier - the participants
accept the AAL system only if it is needed and that
they want to do as much as possible autonomously –
affects the acceptance most. The second model
additionally explains +6.6% (adj. r
2
=.417) and con-
tains “proportion of technology in everyday life is
too high” (β = -0.285; t = -4.624; p < .000) besides
“irrelevant” (β = -0.484; t = -7.850; p < .000). The
final model explains +1.2% (adj. r
2
=.429) and in-
cludes “to be afraid of isolation” (β = -.139; t = -
2.151; p < .000) besides “proportion of technology
in everyday life is too high” (β = -0.235; t = -3.591;
p < .000) and “irrelevant” (β = -0.453; t = -7.228; p
< .000). Hence, these three barriers are most im-
portant for acceptance.
As the perceived benefits and barriers were not
evaluated very differently, it is of major importance
to analyse if these factors differ evenly more in their
assessment with regard to diverse user groups.
Equally, it has to be analysed to which extent the
acceptance of AAL systems differs depending on
users with different needs for assistance.
4.2 User-specific Characteristics
To analyse a potential influence of different assis-
tance and care needs on the acceptance and evalua-
tion of AAL systems, the factors age, experiences
with disabilities and current needs of care were ex-
amined as independent variables.
4.2.1 User-specific Acceptance of AAL
Systems
Overall, MANOVA analyses revealed significant
influences of age (F(16,308)=2.104; p<.01), experi-
ences with disabilities (F(24,465)=2.060; p<.01),
and current care needs (F(8,153)=3.779; p<.01) on
the acceptance of AAL systems. In the following,
the most striking results are presented.
With regard to age, middle-aged and older peo-
ple especially indicated a higher intention to install
AAL technology in their home than younger people
(F(2,162)=4.708; p<.05).
The influence of the factor experiences with
disabilities on all items concerning the acceptance of
AAL technologies is shown in Figure 4. Overall, the
acceptance of AAL technologies was rated rather
similar, except for the group of professional caregiv-
ers who showed comparatively the lowest ac-
ceptance scores (F(3,162)=2.646; p<.1).
Figure 4: Evaluation of AAL acceptance depending on
experience with disabilities.
Two of the negative statements (… superfluous
F(3,162)=2.895; p<.05 and … don´t like to have
AAL technologies in the own home F(3,162)=4.907;
3.4
3.4
3.2
3.0
2.9
2.8
2.6
2.4
1.9
123456
feeling of surveillance
transmission of incorrect
information
be afraid of isolation
proportion of technology in
everyday life is too high
no "real" time savings
no trust in functionality
usage seems to be too dificult
AAL technologies are irrelevant
perceive AAL technologies as
superfluous
evaluation (min=1; max=6)
rejection agreement
4.3
4.4
4.3
4.7
4.3
2.0
2.0
2.3
4.6
3.8
4.0
3.7
4.5
4.0
2.4
2.4
2.2
4.3
4.1
4.3
4.0
4.6
4.4
1.8
1.7
1.8
4.6
3.8
4.3
3.5
4.8
4.7
1.9
1.8
2.0
4.6
123456
I like to use AAL
technologies
I would install AAL
technology/ies in my home
I can imagine to use
AAL technologies now*
I can imagine to
use AAL technologies
due to care needs
I would like to use
AAL technologies to reduce
my care needs*
I don´t like to have
AAL technologies in my home**
I think AAL technologies
are superfluous*
I don´t see an advantage
in using AAL technologies
Acceptance of AAL
technologies
evaluation (min=1; max=6)
rejection agreement
(*p<.05; **p<.01)
no experience
relatives of
disabled person
professional care
givers
disabled person
NegativePositive
in case of care
needs
ICT4AWE 2017 - 3rd International Conference on Information and Communication Technologies for Ageing Well and e-Health
84
p<.01) were lowest rejected by the group of the
professional caregivers. Thus, this group showed in
tendency a higher negative attitude towards AAL
systems than the other three user groups. This pat-
tern was also reflected in the evaluation of the inten-
tion to use AAL technologies to reduce care needs
(F(3,162)=2.981; p<.05). On average, all user
groups agreed to these both statements, while the
professional caregivers comparatively showed the
lowest agreement. Interestingly, the group of not
experienced participants showed the highest agree-
ment scores of the “in case of care needs”-
statements. This evaluation changed with regard to
the more concrete item I can imagine to use AAL
technologies now: here, the not experienced partici-
pants (M=3.5; SD=1.7) showed a clearly lower
agreement than the group of disabled people
(M=4.3; SD=1.3; p<.05, post-hoc-tests: Tukey’s
HSD).
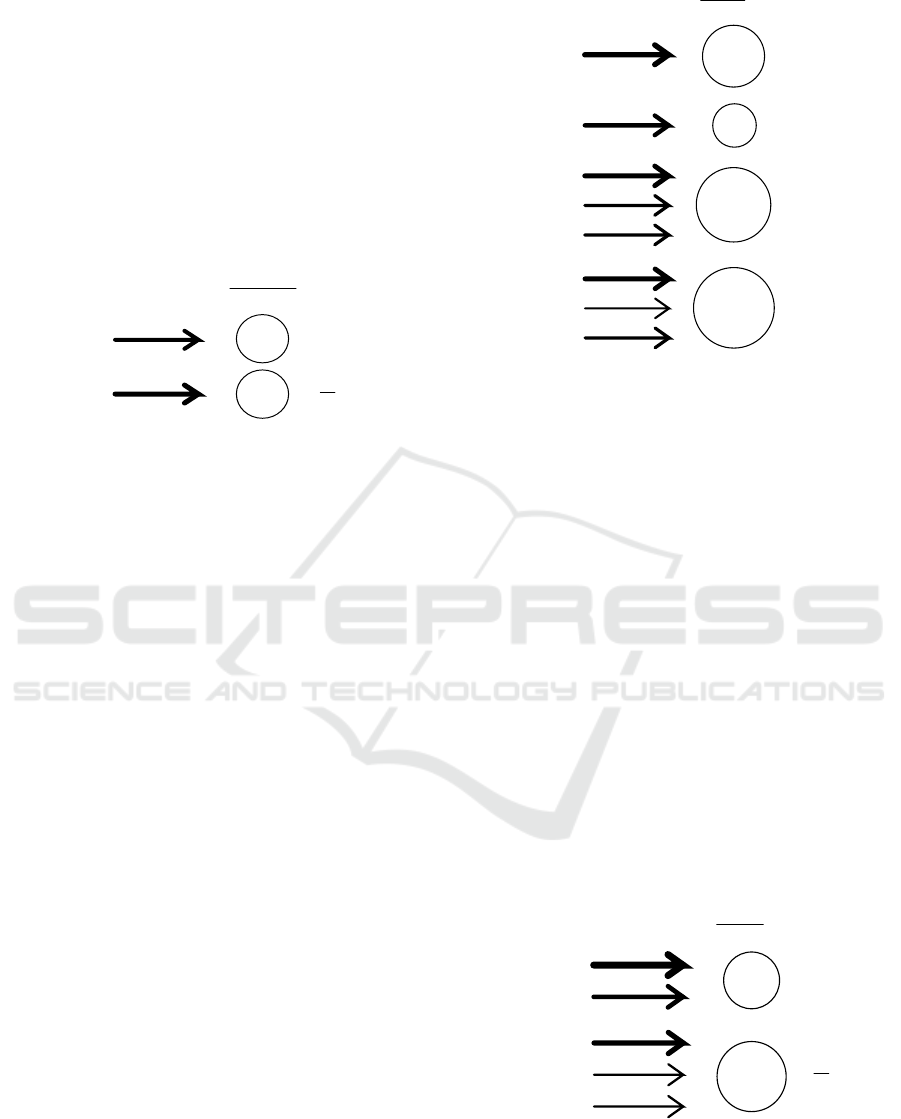
With regard to current care needs, most of the
items concerning the acceptance of the AAL system
differed significantly (see Figure 5). The overall
acceptance of AAL systems is slightly higher for
people with current care needs (M=4.7; SD=1.0)
than for people without current care needs (M=4.5;
SD=1.0; F(1,162)=7.309, p<.01). With regard to the
negative aspects, especially the item I don´t like to
have AAL technologies in my home was significantly
more rejected by people with current care needs
(F(1,162)=10.187; p<.01).
Figure 5: Evaluation of AAL acceptance depending on
current care needs.
Both items regarding care needs (to reduce care
needs F(1,162)=5.321, p<.05 and due to care needs
F(1,162)=4.441; p<.05) are only slightly more ac-
cepted by people with current care needs than by
people without current care needs. The group differ-
ences became more obvious concerning the positive
intention-to-use-statements: here, people with care
needs clearly assessed the items I would install AAL
technologies in my home (M
care
=4.5; SD
care
=1.3;
M
no
=4.1; SD
no
=1.5; F(1,162)=7.107; p<.01) and I
like to use AAL technologies (M
care
=4.4; SD
care
=1.3;
M
no
=3.7; SD
no
=1.4; F(1,162)=13.592; p<.01) higher
than the participants without current care needs.
4.2.2 User-specific Evaluation of AAL
Benefits
Overall, MANOVA analyses revealed no significant
omnibus effects of age, current care needs, and ex-
periences with disabilities on the evaluation of AAL
system benefits. However, single benefit items were
rated significantly different depending on the user
factors experiences with disabilities and current care
needs. To examine these differences and to investi-
gate which benefits are most acceptance-relevant for
which user group, a stepwise linear regression anal-
ysis was conducted. First, the regression results
concerning the experience with disabilities user
groups are presented followed by the results for
people with and without current care needs.
Figure 6: Results of regression analysis – benefits & ac-
ceptance for experience with disabilities groups.
As illustrated in Figure 6, the final regression
model for the group of disabled participants predict-
ed 50.5% (adj. r
2
=.505) of AAL acceptance and was
based on the benefits to expand autonomy (β = .985)
and to facilitate everyday life (β = -.564). For the
group of relatives of disabled people the model ex-
plained 37.5% of variance (adj. r
2
=.375; β = .535)
and for the not experienced group 25.5% (adj.
r
2
=.255; β = .633) each based on the benefit to facili-
4.4
4.5
4.2
4.7
4.5
1.8
2
2.2
4.7
3.7
4.1
3.6
4.6
4.4
2.1
1.9
1.8
4.5
123456
I like to use AAL
technologies**
I would install AAL
technology/ies in my home**
I can imagine to use
AAL technologies now
I can imagine to
use AAL technologies
due to care needs*
I would like to use
AAL technologies to reduce
my care needs*
I don´t like to have
AAL technologies in my home**
I think AAL technologies
are superfluous
I don´t see an advantage
in using AAL technologies
Acceptance of AAL
technologies**
evaluation (min=1; max=6)
rejection agreement
*=p<.05; **=p<.01
no current
care needs
current care
needs
negative
In case of
care needs
positive
p
redictor
51 %
Disabled
.99
-.56
expand
autonomy
facilitate
everyday life
Relatives
38 %
.54
facilitate
everyday life
Care givers
15 %
.54
relieve
fellow people
26 %
.54
facilitate
everyday life
not
experienced
acceptance
explanation
experience
groups
Helpful but Spooky? Acceptance of AAL-systems Contrasting User Groups with Focus on Disabilities and Care Needs
85
tate everyday life. For the professional care givers
the final regression model explained only 15.4%
(adj. r
2
=.154) and was affected by the benefit to
relieve fellow people (β = .399).
Concerning the current care need groups, a com-
parable pattern was found for the prediction of AAL
acceptance by benefits (Figure 7). AAL acceptance
could be partly explained by the benefit to expand
autonomy for the current care need group (adj.
r
2
=.312; β = .519) and by the benefit to facilitate
everyday life for the group without current care
needs (adj. r
2
=.324; β = .612).
Figure 7: Results of regression analysis – barriers & ac-
ceptance for current care needs groups.
4.2.3 User-specific Evaluation of AAL
Barriers
Overall, MANOVA analyses revealed significant
omnibus effects of age (F(18,310)=1.939; p<.05) on
the evaluation of AAL barriers. Tukey’s HSD post-
hoc tests revealed significant differences between
the younger and both older age groups (p<.05):
younger participants (M=3.8; SD=1.4) had stronger
concerns about a transmission of incorrect infor-
mation than the middle-aged (M=3.1; SD=1.2) or
old (M=3.0; SD=1.0) participants and they (M=3.9;
SD=1.6) also feared the feeling of surveillance
significantly more than the middle-aged (M=3.2;
SD=1.5) and old participant group (M=3.1;
SD=1.3). For experiences with diseases (F(27,468)=
1.502; p<.1) and current care needs (F(9,154)=
1.894; p<.1) groups differences were in the looming.
Since single barrier items were rated significantly
different depending on these user factors, further
regression analyses were conducted in order to find
out which barriers were most decisive for acceptance
for which user group. Figure 8 illustrates the results
of the final linear regression analyses for all experi-
ences with disabilities groups.
Figure 8: Results of regression analysis – barriers & ac-
ceptance for experience with disabilities groups.
For the groups of relatives, the model predicted
only 23.1% of variance of AAL acceptance (adj.
r
2
=.231) and was affected by concerns that the pro-
portion of technology in everyday life is too high (β
= -.376). For the group of disabled participants, the
model explained 39.9% of AAL acceptance variance
(adj. r
2
=.399) based on the barrier to perceive AAL
technologies as superfluous (β = -.649). Further, the
final model predicted 58.3% (adj. r
2
=.583) of vari-
ance for the professional care giver group and was
affected by the barriers usage seems to be too diffi-
cult (β = -.494), to perceive AAL technologies as
superfluous (β = -.293), and to be afraid of isolation
(β = -.249). For the not experienced group, the final
model explained 60.2% of AAL acceptance variance
based on the three barriers to perceive AAL technol-
ogies as superfluous (β = -.520), to expect no “real”
time savings (β = -.154), and the concerns that the
proportion of technology in everyday life is too high
(β = -.227).
Figure 9: Results of regression analysis – barriers & ac-
ceptance for current care needs groups.
p
redictor
32 %
.52
expand
autonomy
.61
facilitate
everyday life
acceptance
explanation
user
groups
current
care needs
32 %
no current
care needs
p
redictor
40 %
Disabled
-.65
perceived as
superfluous
Relatives
23 %
-.38
proportion of
technology too high
Care givers
barriers
explanation
experience
groups
-.49
-.29
-.25
usage seems
too difficult
afraid of
isolation
menu design
58 %
-.52
-.15
-.23
perceived as
superfluous
no „real“
time savings
60 %
not
experienced
proportion of
technology too high
p
redictor barriers
explanation
user
groups
current
care needs
no current
care needs
51 %
40 %
.99
-.56
perceived as
superfluous
afraid of
isolation
-.43
-.15
-.19
perceived as
superfluous
no „real“
time savings
proportion of
technology too high
ICT4AWE 2017 - 3rd International Conference on Information and Communication Technologies for Ageing Well and e-Health
86

Regarding the current care need groups, a com-
parable pattern was found for the prediction of AAL
acceptance by barriers (Figure 9). AAL acceptance
could be partly explained (39.7%) by the barriers to
perceive AAL technologies as superfluous (β = -
.422) and to be afraid of isolation (β = -.216) for the
current care need group (adj. r
2
=.397). For the group
without current care needs, the final model predicted
48.9% variance of AAL acceptance (adj. r
2
=.489)
and was affected by the three barriers to perceive
AAL technologies as superfluous (β = -.426), the
concern that the proportion of technology in every-
day life is too high (β = -.189), and the expectation
of no “real” time savings (β = -.153).
5 DISCUSSION
This study revealed insights into acceptance patterns
concerning AAL systems in home environments. In
order to understand specific needs of diverse future
users, we considered and compared different user
perspectives regarding distinct experiences with
respect to disabilities and care needs. The results
provide valuable insights into user-specific ac-
ceptance-decisive factors of AAL systems and
should be taken into account for development, de-
sign, and configuration of AAL systems as well as in
future studies concerning the acceptance and adop-
tion of AAL systems.
5.1 Acceptance of AAL Systems
Align with previous research results (e.g., Gövercin
et al., 2016) our results show that a holistic AAL
system with a wide spectrum of functions (see 3.3)
is generally accepted and rated positive by all user
groups. Especially in the context of care needs, the
intention to use such a system is universally present
and differs only slightly with regard to the different
user perspectives. Whenever hypothetical care needs
are mentioned in an intention-to-use-statement, they
are more important than other wishes or concerns
and the AAL system would be used in this context.
However, if a concrete intention to use is men-
tioned without the context of care needs, significant
differences between the user perspectives become
apparent: in tendency, older people, disabled people,
and people in need of care indicate a clearly higher
intention to like to use an AAL system currently or
to want to install an AAL system in their home envi-
ronment than presumably healthy people without
experiences with disabilities or care needs. Hence,
the facts that people are concerned with health issues
and needy influences the intention to use an AAL
system. Concerning age, this aligns with previous
research results where older participants also indi-
cated higher acceptance scores of assisting technol-
ogies than younger people (e.g., Wilkowska et al.,
2012). In contrast, this is a comparatively new phe-
nomenon with regard to diseases and disabilities.
With regard to the different user perspectives,
the group of professional care givers is striking con-
cerning their evaluations: in comparison with all
other groups they indicated to have a more negative
attitude towards AAL systems (Klack et al., 2013).
This was also true for the evaluations in the preced-
ing interviews, where AAL systems were partly
described as spooky or inhuman. In line with previ-
ous research results, we assume that this group takes
a critical attitude due to concerns to be replaced by
technology, a lower general trust in technology, and
maybe also due to concerns about a difficult han-
dling of technology (see 5.2).
In conclusion, this study’s results show that the
acceptance of AAL systems depends on the user
factors, age, experience with disabilities, and current
care needs. Equally, reasons for use or non-use of an
AAL system differ with respect to user diversity.
5.2 Acceptance-Decisive Factors
The evaluation of motives to use and perceived
barriers not to use an AAL system differed with
regard to user diversity.
Disabled people and participants with current
care needs described the within the scenario pictured
AAL system in particular as helpful, comfortable,
and very useful. For this people, it is most important
that applied technologies help to expand their au-
tonomy. Facilitation of everyday life is comparative-
ly incidental or even not desired as most people of
this groups want to cope with as much everyday
tasks as possible on their own. Hence, in this way
AAL systems could be very enriching for those
people helping them to help themselves. Concurrent-
ly, it is striking for this group, that the main per-
ceived benefits carry greater weight than the per-
ceived barriers. The most important barrier for this
people represents the aspect that AAL systems are
seen as superfluous which refers to concerns that the
technology undertakes tasks the people would like to
do autonomously. Thus, this aspect is the most im-
portant benefit’s counterpart and emphasizes the
importance of autonomy for this specific user group.
The perspective of relatives of disabled people
can be best compared with the disabled people’s
Helpful but Spooky? Acceptance of AAL-systems Contrasting User Groups with Focus on Disabilities and Care Needs
87

perspective: for them, also the perceived benefits are
in tendency more important than the perceived barri-
ers.
In contrast, in line with previous results (Himmel
et al., 2013) for people without current care needs
and also the other experience with disabilities
groups, the benefits facilitation of everyday life and
relief of fellow people are the main motives to use
AAL systems. Moreover, for the not experienced
group and the group of professional care givers, the
most perceived barriers carry clearly more weight
than the perceived benefits of AAL systems. This
fits the pattern, that the professional care givers
described the scenario’s AAL system primarily as
spooky and undesirable (see 3.2 and 5.1). However,
the perceived barriers differ between these two
groups. The care givers are especially worry about a
difficult usage of the technology as they maybe
assume that the workflow is affected and slowed
down by difficulties due to handling the system. In
contrast, the not experienced group doubts about if
the technology is necessary and a too high propor-
tion of technology.
On the basis of these results, we suggest to in-
clude disabled people into early development stages
of AAL technologies in order to reach technical
solutions that are personalized and sufficiently
adapted to individual requirements. Thus, not only
facilitating and management of everyday life at
home can be ensured but also the inclusion in work-
ing and leisure time within the whole society.
5.3 Limitations and Future Research
Our empirical approach provided valuable insights
into the acceptance of AAL systems considering
different user perspectives. However, some limita-
tions concerning the applied method and sample
should be taken into account. As the present study
was a first approach to compare different user per-
spectives, it had to be concentrated on the general
acceptance of a holistic AAL system and the evalua-
tion of crucial benefits and barriers. In future stud-
ies, we will consider other aspects, e.g., relationship
between privacy and safety, trade-off between per-
ceived benefits and maybe perceived intrusion of
privacy, that have not been taken into account so far.
Further, the evaluation referred to a holistic AAL
system with different functions and technologies, as
this study aimed for an assessment of a whole sys-
tem and not of single technologies, which are largely
researched. In future studies, it has to be examined if
scenarios with slightly divergent descriptions (e.g.,
adding or changing functions) of a holistic AAL
system will be evaluated differently.
It has also to be mentioned that the evaluation
was based on a scenario and thus, on a fictional and
not on a real AAL system. At a later stage, an evalu-
ation of the real AAL system and also a comparison
between the scenario and the real system evaluation
would be very interesting.
Also some aspects concerning the sample could
be enhanced and pursued in future follow-up studies:
first, this study’s sample size was adequate, but the
study should be replicated in even larger and espe-
cially more representative samples. In particular this
was true for gender: as this study contained a higher
number of women than men, future studies should
focus on more gender-balanced samples. Second,
correlations revealed that age was not related to
disabilities or current care needs. Hence, our study
reached similarly younger as well as older people
with disabilities. To be able to focus on the new
phenomenon of “old” disabled people (Poore, 2007),
future studies should also try to reach a higher pro-
portion of old and disabled people. Nevertheless,
this study enabled a first analysis of the relationship
and influences of age, experiences with disabilities,
and current care needs on the acceptance of AAL
systems. This relationship should also be addressed
in future studies and with regard to aspects that were
not considered in detail in this study, e.g., the trade-
off between safety and privacy or attitudes towards
data security and privacy.
Finally, as this study focused German partici-
pants, it represents a perspective of only one specific
country with a specific health care system. For fu-
ture studies, our approach should be applied in other
countries to compare AAL acceptance and future
users needs depending on different countries, their
specific health care systems, and cultures.
ACKNOWLEDGEMENTS
The authors thank all participants for their patience
and openness to share opinions on a novel technolo-
gy. Furthermore, the authors want to thank Lisa
Portz for research assistance. This work was funded
by the German Federal Ministry of Education and
Research project Whistle (16SV7530).
ICT4AWE 2017 - 3rd International Conference on Information and Communication Technologies for Ageing Well and e-Health
88

REFERENCES
Baig, M. M., Gholamhosseini, H. (2013). Smart Health
Monitoring Systems: An Overview of Design and
Modeling. J Med Syst., 37(2), 1-14.
Beringer, R., Sixsmith, A., Campo, M., Brown, J.,
McCloskey, R. (2011). The “acceptance” of ambient
assisted living: Developing an alternate methodology
to this limited research lens. In Proceedings of the In-
ternational Conference on Smart Homes and Health
Telematics, Toward useful services for elderly and
people with disabilities. Springer, pp. 161–167.
Bloom, D. E., & Canning, D. (2004). Global Demograph-
ic Change: Dimensions and Economic Significance
National Bureau of Economic Research. Working Pa-
per No. 10817.
Brauner, P., Holzinger, A., Ziefle, M. (2015). Ubiquitous
computing at its best: serious exercise games for older
adults in ambient assisted living environments–a tech-
nology acceptance perspective. EAI Endorsed Trans.
Serious Games, 15, 1–12.
Casenio. (2016). Homepage: Casenio - intelligente Hilfe-
& Komfortsysteme [intelligent support and comfort
systems]. Retrieved from https://www.casenio.de/
Cheng, J., Chen, X., Shen, M. (2013). A Framework for
Daily Activity Monitoring and Fall Detection Based
on Surface Electromyography and Accelerometer Sig-
nals. IEEE J Biomed Health Inform., 17(1), 38–45.
Demiris, G., Hensel, B. K., Skubic, M., Rantz, M. (2008).
Senior residents’ perceived need of and preferences
for “smart home” sensor technologies. Int J Technol
Assess Health Care, 24(1), 120–124.
Demiris, G., Rantz, M., Aud, M., Marek, K., Tyrer, H.,
Skubic, M., & Hussam, A. (2004). Older adults’ atti-
tudes towards and perceptions of “smart home” tech-
nologies: a pilot study. Med Inform Internet, 29(2),
87–94.
EarlySense. (2016). Homepage: EarlySense All-in-One
System. Retrieved from http://www.earlysense.com/
Essence. (2016). Homepage: Smart Care - Care@ Home
Product Suite. Retrieved from http://www.essence-
grp.com/smart-care/care-at-home-pers.
Fuchsberger, V. (2008). Ambient assisted living: elderly
people’s needs and how to face them. In Proceedings
of the 1st ACM international workshop on Semantic
ambient media experiences, ACM, pp. 21–24.
Geenen, S. J., Powers, L. E., Sells, W. (2003). Under-
standing the Role of Health Care Providers During the
Transition of Adolescents With Disabilities and Spe-
cial Health Care Needs. J Adolesc Health, 32(3), 225–
233.
Gentry, T. (2009). Smart homes for people with neurolog-
ical disability: State of the art. NeuroRehabilitation,
25(3), 209–217.
Gövercin, M., Meyer, S., Schellenbach, M., Steinhagen-
Thiessen, E., Weiss, B., Haesner, M. (2016).
SmartSenior@home: Acceptance of an integrated am-
bient assisted living system. Results of a clinical field
trial in 35 households. Inform Health Soc Care
, 1–18.
Harris, J. (2010). The use, role and application of ad-
vanced technology in the lives of disabled people in
the UK. Disabil Soc, 25(4), 427–439.
Himmel, S., Ziefle, M. (2016). Smart Home Medical
Technologies: Users’ Requirements for Conditional
Acceptance. I-Com, 15(1).
Himmel, S., Ziefle, M., Lidynia, C., & Holzinger, A.
(2013). Older Users’ Wish List for Technology At-
tributes. In A. Cuzzocrea, C. Kittl, D. E. Simos, E.
Weippl, L. Xu (Eds.), Availability, Reliability, & Se-
curity in Information Systems and HCI, Springer Ber-
lin Heidelberg, pp. 16–27.
Klack, L., Ziefle, M., Wilkowska, W., Kluge, J. (2013).
Telemedical versus conventional heart patient moni-
toring: a survey study with German physicians. Int J
Technol. Assess Health Care, 29(4), 378–383.
Kleinberger, T., Becker, M., Ras, E., Holzinger, A., Mül-
ler, P. (2007). Ambient Intelligence in Assisted Liv-
ing: Enable Elderly People to Handle Future Interfac-
es. In Universal Access in Human-Computer Interac-
tion. Ambient Interaction, Springer Berlin Heidelberg,
pp. 103–112.
Kowalewski, S., Wilkowska, W., Ziefle, M. (2012). Ac-
counting for user diversity in the acceptance of medi-
cal assistive technologies. In Electronic Healthcare,
Springer, pp. 175–183.
Larizza, M. F., Zukerman, I., Bohnert, F., Busija, L.,
Bentley, S. A., Russell, R. A., Rees, G. (2014). In-
home monitoring of older adults with vision impair-
ment: exploring patients’, caregivers’ and profession-
als’ views. J American Medical Informatics Associa-
tion, 21(1), 56–63.
López, S. A., Corno, F., Russis, L. D. (2015). Supporting
caregivers in assisted living facilities for persons with
disabilities: a user study. Universal Access in the In-
formation Society, 14(1), 133–144.
Mortenson, W. B., Demers, L., Fuhrer, M. J., Jutai, J. W.,
Lenker, J., DeRuyter, F. (2013). Effects of an assistive
technology intervention on older adults with disabili-
ties and their informal caregivers: an exploratory ran-
domized controlled trial. American J of Physical Med-
icine & Rehabilitation/Assoc of Academic Physiatrists,
92(4), 297–306.
Poore, C. (2007). Disability in Twentieth-century German
Culture. University of Michigan Press.
Rashidi, P., Mihailidis, A. (2013). A Survey on Ambient-
Assisted Living Tools for Older Adults. IEEE J Bio-
med Health Inform, 17(3), 579–590.
Roger, V. L., Go, A. S., Lloyd-Jones, D. M., Adams, R. J.,
Berry, J. D., Brown, T. M., et al. (2011). American
Heart Association Statistics Committee and Stroke
Statistics Subcommittee. Heart disease and stroke sta-
tistics--2011 update: a report from the American Heart
Association. Circulation, 123
(4), e18–e209.
Ruyter, B. de, & Pelgrim, E. (2007). Ambient Assisted-
living Research in Carelab. Interactions, 14(4), 30–33.
Schmitt, J. M. (2002). Innovative medical technologies
help ensure improved patient care and cost-
effectiveness. J Med Mark: Device, Diagnostic and
Pharmaceutical Marketing, 2(2), 174–178.
Helpful but Spooky? Acceptance of AAL-systems Contrasting User Groups with Focus on Disabilities and Care Needs
89

Shaw, J. E., Sicree, R. A. Zimmet, P. Z. (2010). Global
estimates of the prevalence of diabetes for 2010 and
2030. Diabetes Res Clin Pract, 87(1), 4–14.
Silverstone, R., Morley, D., Dahlberg, A., & Livingstone,
S. (1989). Families, technologies and consumption:
the household information and communication tech-
nologies.
Sixsmith, A., Meuller, S., Lull, F., Klein, M., Bierhoff, I.,
Delaney, S., Savage, R. (2009). SOPRANO – An Am-
bient Assisted Living System for Supporting Older
People at Home. In M. Mokhtari, I. Khalil, J. Bauchet,
D. Zhang, & C. Nugent (Eds.), Ambient Assistive
Health and Wellness Management in the Heart of the
City, Springer Berlin Heidelberg, pp. 233–236.
Sun, H., De Florio, V., Gui, N., Blondia, C. (2010). The
missing ones: Key ingredients towards effective ambi-
ent assisted living systems. J Ambient Intell Smart En-
viron, 2(2), 109–120.
Tunstall. (2016). Homepage: Tunstall - Solutions for
Healthcare Professionals. Retrieved from
www.tunstall healthcare.com.au.
Walker, A., Maltby, T. (2012). Active ageing: A strategic
policy solution to demographic ageing in the European
Union. Int J Social Welfare, 21, 117–130.
Wild, S., Roglic, G., Green, A., Sicree, R., King, H.
(2004). Global prevalence of diabetes: estimates for
the year 2000 and projections for 2030. Diabetes
Care, 27(5), 1047–1053.
Wiles, J. L., Leibing, A., Guberman, N., Reeve, J., Allen,
R. E. S. (2011). The Meaning of “Ageing in Place” to
Older People. The Gerontologist, gnr098.
Wilkowska, W., Gaul, S., & Ziefle, M. (2010). A Small
but Significant Difference–The Role of Gender on Ac-
ceptance of Medical Assistive Technologies. In: Sym-
posium of the Austrian HCI and Usability Engineering
Group, Springer Berlin Heidelberg, pp. 82-100.
Wilkowska, W., Ziefle, M., & Himmel, S. (2015). Percep-
tions of Personal Privacy in Smart Home Technolo-
gies: Do User Assessments Vary Depending on the
Research Method? In Int Conference on Human As-
pects of Information Security, Privacy, Trust, Spring-
er, pp. 592–603.
Wilkowska, W., Ziefle, M., Alagöz, F. (2012). How user
diversity and country of origin impact the readiness to
adopt E-health technologies: an intercultural compari-
son. Work (Reading, Mass.), 41 Suppl 1, 2072–2080.
Ziefle, M., Himmel, S., Wilkowska, W. (2011). When
Your Living Space Knows What You Do: Acceptance
of Medical Home Monitoring by Different Technolo-
gies. In Information Quality in e-Health, Springer Ber-
lin Heidelberg, pp. 607–624.
ICT4AWE 2017 - 3rd International Conference on Information and Communication Technologies for Ageing Well and e-Health
90
