
Discussions of a Preliminary Hand Hygiene Compliance Monitoring
Application-as-a-service
Peng Zhang
1
, Marcelino Rodriguez-Cancio
2
, Douglas Schmidt
1
, Jules White
1
and Tom Dennis
3
1
Institute for Software Integrated Systems, Vanderbilt University, Nashville, TN, U.S.A.
2
Research Institute of Computer Science and Random Systems, University of Rennes 1, Rennes, France
3
ZH Solutions, Nashville, TN, U.S.A.
Keywords:
Machine Learning, Deep Learning, Data Mining, Hospital and Healthcare, Hand Hygiene Compliance,
Re-admissions.
Abstract:
Hospital Acquired Infections (HAIs) are a global concern as they impose significant economic consequences
on the healthcare systems. In the U.S. alone, HAIs have cost hospitals an estimated $9.8 billion a year. An
effective measure to reduce the spread of HAIs is for Health Care Workers (HCWs) to comply with recom-
mended hand hygiene (HH) guidelines. Unfortunately, HH guideline compliance is currently poor, forcing
hospitals to implement controls. The current standard for monitoring compliance is overt direct observation
of hand sanitation of HCWs by trained observers, which can be time-consuming, costly, biased, and sporadic.
Our research describes a hand hygiene compliance monitoring app, Hygiene Police (HyPo), that can be de-
ployed as a service to alleviate the manual effort, reduce errors, and improve existing compliance monitoring
practice. HyPo exploits machine learning analyses of handwashing compliance data from a 30-bed intensive
care unit to predict future compliance characteristics. Based on the results, HyPo then provides HWCs with
timely feedback and augments the current monitoring approach to improve compliance.
1 INTRODUCTION
Emerging Concerns in Healthcare. Hospital Ac-
quired Infections (HAIs) are occupational infections
acquired by Healthcare Workers (HCWs) or by pa-
tients in healthcare facilities that appear after patient
discharge (WHO, 2009). HAIs represent significant
health problems, with a considerable economic im-
pact on patients and hospitals worldwide.
Persistent exposures to diseases and lack of appro-
priate hand hygiene (HH) practice can cause HCWs’
hands to become carriers of infections transmitted to
patients or other staff through physical contact. To
reduce re-admission rates, therefore, HCWs are ex-
pected to comply with HH guidelines to prevent the
spread of HAIs in healthcare facilities. The cur-
rent standard practice of compliance monitoring is for
covert human auditors to unobtrusively observe and
record HH compliance of medical workers. Unfor-
tunately, this approach is costly and subject to bias
(Boyce et al., 2009) due to the Hawthorne effect (Eck-
manns et al., 2006), which occurs when subjects of a
study change their behavior due to awareness of being
observed.
Contribution. Based on our preliminary study on
HH compliance characteristics using machine learn-
ing (Zhang et al., 2016), this work proposes a hand
hygiene compliance monitoring app, Hygiene Police
(HyPo), that can be deployed as a service. The goal of
this app is to mitigate the laborious effort and reduce
errors of direct observation.
App Workflow. HyPo is implemented as a Java-
based desktop app that communicates to and from
Bluetooth Low-Energy (BLE) devices equipped at the
facility from our previous study (Zhang et al., 2016).
The schematic in Figure 1 depicts the overall app
workflow, which is divided into the following three
stages (the last two are the core components of HyPo):
1. Data Acquisition, where raw data is acquired
from the BLE devices.
2. Data Mining, where the raw data undergoes a
data mining process provisioned by HyPo to pro-
duce a set of features that is fed to Feature Selec-
tion algorithms to obtain a Sanitized Dataset. The
Feature Selection is done to improve the execu-
Zhang P., Rodriguez-Cancio M., Schmidt D., White J. and Dennis T.
Discussions of a Preliminary Hand Hygiene Compliance Monitoring Application-as-a-service.
DOI: 10.5220/0006293705370544
Copyright
c
2017 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
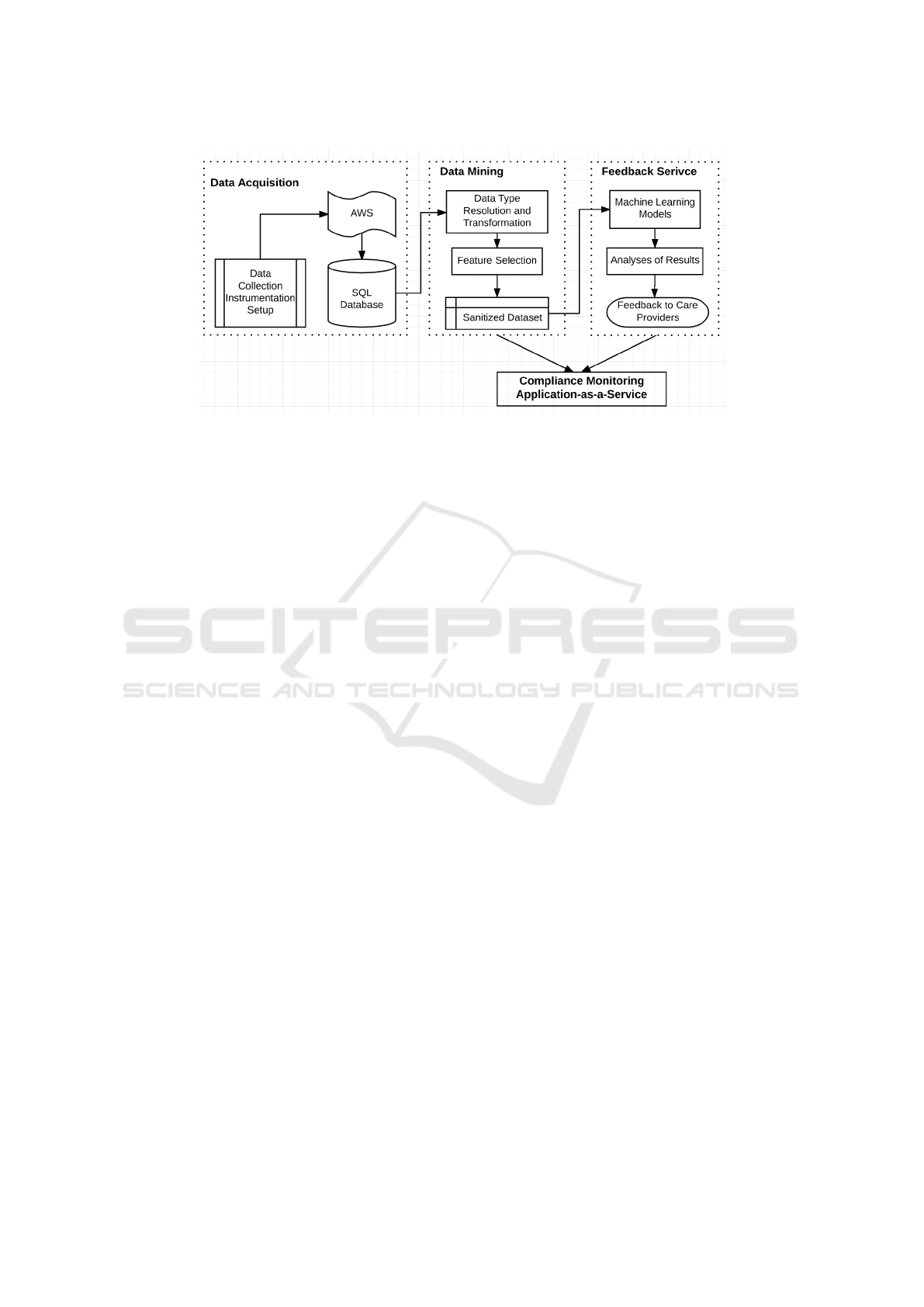
Figure 1: The Overall System Flow: from Data Collection to Post-prediction Analysis and Feedback Service.
tion performance of the Machine Learning (ML)
methods that will follow by determining the most
relevant features and removing the others from the
Sanitized Dataset.
3. Feedback Service, where the ML models are run
over the Sanitized Dataset to produce feature set
that can be used to provide timely feedback to
healthcare providers.
Paper Organization. The remainder of this paper
is organized as follows: Section 2 defines key terms
frequently referenced throughout the paper; Section 3
describes the data collection setup; Section 4 details
the data preparation and mining process; Section 5
describes Hypo’s feedback service and how it com-
plements the direct observation approach; Section 6
surveys and compares existing research in the area of
hand hygiene compliance improvement and monitor-
ing applications; and Section 7 presents concluding
remarks and outlines future extensions of this work.
2 HAND HYGIENE
COMPLIANCE OVERVIEW
This section defines the following terms that are used
frequently in the paper:
1. Hand hygiene opportunity: an opportunity for
hand cleaning is presented before each care
provider’s entry/exit of a patient room.
2. Hand hygiene/handwashing compliance: each
hand hygiene opportunity requires one hand hy-
giene action, which should be a correspond-
ing positive (compliance) or negative (non-
compliance) action (EFORE, 2009).
3. Entry compliance: hand hygiene compliance ob-
served at staff’s entry to a patient room, deter-
mined by wash on entry.
4. Exit compliance: hand hygiene compliance ob-
served at staff’s exit from a patient room, deter-
mined by wash on exit.
5. Wash on entry: hand hygiene action at patient
room entry that determines entry compliance, true
if performed and false otherwise.
6. Wash on exit: hand hygiene action at patient
room exit that determines exit compliance, true if
performed and false otherwise.
Our previous study collected 60 days of care
providers’ real-time location and handwashing data,
from an intensive care unit (ICU) equipped with 30
beds, and observed two major correlating factors to
compliance: (1) entry compliance has an 89% accu-
racy on predicting exit compliance and (2) exit com-
pliance can predict entry compliance at the next visit
(for the same staff) at an accuracy as high as 77%.
Likewise, location data was observed to have a minor
impact on predicting exit compliance (Zhang et al.,
2016).
Based on this previous study, in the HyPo app we
compiled the following rules of hand hygiene compli-
ance that ICU staff should abide by:
1. All on-duty staff at the ICU were required to wear
a BLE badge.
2. All staff were required to sanitize their hands
within a short interval of 2 minutes upon entering
a patient room and before exiting the same room.
3. Each compliant action should be associated with
an activation of a specific soap dispenser with
disinfectant solution against Clostridium difficile,

a common HAI spread through physical con-
tact (Shrestha et al., 2016). These dispensers are
located both inside and outside each patient room.
These rules only apply to this ICU but can be con-
figured to work with other caregiving settings. The
rest of this paper describes the application of HyPo
using the same device-equipped 30-bed ICU from our
previous study (Zhang et al., 2016) as an example.
3 DATA ACQUISITION
This section describes the data acquisition process,
where real-time location data and handwashing sta-
tion activation data is recorded, and then provides an
overview of the essential data fields extracted from
the collection. The process described in this section
is one approach of obtaining the hand hygiene com-
pliance data to provide input for our app, but it is by
no means the only option to acquire this type of data.
3.1 Instrumentation Configurations
The ICU with HyPo deployment was equipped with a
Bluetooth Low-Energy (BLE) indoor positioning sys-
tem that provides room-level accuracy for reporting
staff locations in real-time. The system produced the
location data for all staff with BLE badges.
The ICU also deployed Gojo Active Monitoring
handwashing stations, which record each dispenser
activation. These activation events were then com-
bined with real-time location data to track individual
staff handwashing compliance. The system expected
to receive at least one handwashing event from ei-
ther a sanitation station inside of the room or a sta-
tion immediately outside the room within two min-
utes prior to entry, abiding the facility rules described
in Section 2. Similarly, two minutes before or af-
ter room exit, the system expected one handwashing
event from either sanitation stations.
Overall, the dataset collected at the studied ICU
contains 8 weeks of events recording activities from
180+ soap dispensers activated by 60 badged nurses
24 hours a day. All raw event data was streamed to a
data storage on Amazon Web Services (AWS), which
was post processed and output to a SQL database. We
then extrapolated the data fields of interest for com-
pliance predictions and analyses.
3.2 Dataset Limitations
Although real-time location data was acquired and
handwashing station activations recorded at the ICU,
the dataset was still an estimate rather than a ground
truth of hand hygiene compliance. The dataset col-
lected has a number of key threats to validity, includ-
ing: (1) not all staff wore their BLE badges at all
times, (2) the system could not differentiate activa-
tions from badged vs. non-badged visitors/staff, and
(3) subsets of the monitoring equipment went offline
at some intervals and prevented data capture in certain
rooms.
However, we did not consider these limitations
as fatal to our study results because we could either
easily eliminate the data entries associated with these
threats or discard the marginal impact that the threats
had on our findings.
3.3 Dataset Schema
From the SQL database we obtained an initial dataset
by omitting certain data fields with extraneous infor-
mation, such as device IDs of the wearable badges,
internally-used identifiers of the patient rooms, etc.
The data fields associated to each patient room visit
event that we deemed essential thus extracted from
the database include:
1. Staff ID - ID of badge worn by the staff who has
been associated with a patient room visit
2. Location - patient room number visited by the
badged staff
3. Entry time - timestamp (in CDT) at which the
badged nurse entered the patient room
4. Exit time - timestamp (in CDT) at which the
badged nurse exited the patient room
5. Wash on entry - a boolean value indicating
whether the staff properly performed hand hy-
giene on patient room entry
6. Wash on exit - a boolean value indicating if the
staff properly performed handwashing on patient
room exit
7. Duration - for how long (in milliseconds) the staff
was in the patient room
4 DATA PREPARATION
This section discusses how we prepared the collected
data to maximize the utilization of our machine learn-
ing classifiers, which is an important capability of-
fered by HyPo. This process is the same as that em-
ployed in (Zhang et al., 2016) to assist the analy-
ses and characterization of hand hygiene compliance.
Other influencing factors of hand hygiene compliance
may be discovered as more relevant data becomes

available, such as patient admittance details, medi-
cal records of admitted patients, facility regulations
of compliance, etc.
Despite the specificity of the dataset used through-
out this paper, the data mining process provided by
HyPo as described below can be generalized to sup-
port transformations of different forms of data col-
lected in other facilities.
4.1 Data Transformation
Most machine learning (ML) classifiers yield better
results when the input dataset is structured in certain
ways. For example, suppose we want to know if the
day of week (Monday to Sunday) influences compli-
ance, some ML classifiers will yield better results if
we express date as a set of integers ranging from 1
to 7, as opposed to a real continuous stream of times-
tamps expressed in milliseconds.
As another example, our location data consists of
room numbers, which provides little information re-
garding spatial distribution of the rooms. If we want
to know whether compliance decreases in nearby lo-
cations, we must first transform the room numbers
into coordinates on the facility’s floor plan, for in-
stance.
To obtain a transformed schema that can be bet-
ter handled by our classifiers, we took the collected
dataset and performed the following transformations
over it:
1. We converted all event data from the original
timestamp format into an integer field with range
1 to 7 to represent day of week, an integer field
with range 1 to 4 to represent time of day in morn-
ing, afternoon, evening, bedtime, and another in-
teger data field of 0-23 to represent hour of day.
The numeric representations of the original nom-
inal time stamp data will allow our classifiers to
achieve higher classification accuracy.
2. We mapped each patient room on the ICU floor
plan to a set of x and y coordinates to identify the
spacial location. We then extended each entry in
the dataset to include these corresponding coordi-
nates of the patient room.
3. For each data point we added new fields to include
the previous record of the corresponding badged
staff’s handwashing data, i.e., duration, location,
washed on entry, and washed on exit. To ensure
data integrity, we removed all entries that did not
have previous handwashing records.
As a result of these transformations, we obtained
a new schema consisting of a minimal set of features
that our application expects to receive for best accu-
racy:
1. staff ID - integer
2. location (room number) - integer
3. washed on entry - TRUE/FALSE
4. washed on exit - TRUE/FALSE
5. duration (s) - length of patient room visit in sec-
onds, integer
6. entry hour - hour of day on room entry, 0-23
7. exit hour - hour of day on room exit, 0-23
8. entry time - time of day on recorded room entry
in Morning (1), Afternoon (2), Evening (3), and
Bedtime (4)
9. exit time - time of day on recorded patient room
exit, 1-4
10. entry day of week - day of week on recorded pa-
tient room entry, 1-7
11. exit day of week - day of week on room exit, 1-7
12. location X coordinate - x coordinate of patient
room on the ICU floor plan
13. location Y coordinate - y coordinate of patient
room on the ICU floor plan
14. previous duration (s) - duration of the same staff’s
previous patient room visit in seconds
15. previous washed on entry - dispenser activation on
previous room entry TRUE/FALSE
16. previous washed on exit - dispenser activation on
previous room exit TRUE/FALSE
17. previous location - previously visited patient room
number
4.2 Feature Selection
After we transformed the dataset into a features set,
we executed a feature selection process to automat-
ically select feature subsets in our transformed data
that best (1) reduced overfitting of data, (2) improved
classification accuracy, and (3) decreased model train-
ing time (Guyon and Elisseeff, 2003). Although we
do not have a significantly large feature list produced
for this ICU, it is still useful to apply this technique
to select the most relevant subsets of features to help
produce the most accurate feedback in the next step.
To automatically select features from the trans-
formed dataset, HyPo applies a supervised attribute
selection filter from the open source Weka Java li-
brary (Hall et al., 2009). The filter is composed of
two pieces: (1) a feature Evaluator to determine how
features are evaluated and (2) a Search Method to nav-
igate the feature’s search space. Our app runs feature
selection using the following pairs of Evaluators and
Search Methods, as shown in Table 1:
1. Evaluator: CfsSubsetEval that evaluates a subset
of features by considering each feature’s predic-
tive ability and the degree of redundancy between
them.
Search Method: GreedyStepwise with a backward
search through the space of attribute subsets.
2. Evaluator: InfoGainAttributeEval that evaluates
an attribute’s worth by measuring the information
gain with respect to the class variable to classify.
Search Method: Ranker that ranks features by
their individual evaluations with an optional pa-
rameter of 6 features in the output subset
3. Evaluator: WrapperSubsetEval (Kohavi and
John, 1997) with NaiveBayes (John and Langley,
1995) as the basic learning scheme and a 10-fold
cross validation to use for estimating accuracy.
Search Method: GeneticSearch that performs a
search using the simple genetic algorithm (Gold-
berg, 1989)
Table 1: Evaluator and Search Method Pairs Used in Fea-
ture Selection
Evaluator Search Method
CfsSubsetEval GreedyStepwise
InfoGainAttributeEval Ranker
WrapperSubsetEval GeneticSearch
Our previous study (Zhang et al., 2016) observed
two highly correlating factors of compliance using the
data collected in the same 30-bed ICU. We could con-
figure HyPo to select only these two features from
the dataset to use for determining feedback provi-
sion. However, automatic feature selection is an in-
tegral piece because as the dataset increases in size
and dimension, our enhanced app can continuously
combine features or intelligently adjust the correlat-
ing features to maximize classification accuracy.
5 FEEDBACK SERVICE
This section first describes the machine learning mod-
els employed by HyPo and then presents the feedback
service that uses these models to provide timely feed-
back and to complement the direct observation ap-
proach to hand hygiene compliance monitoring.
5.1 Machine Learning Models
After preparing the dataset, we split the data to 65%
for training, 10% for cross validation, and the re-
maining 25% for testing the ML models. Based
on the compliance prediction observations from the
previous study in (Zhang et al., 2016), we em-
ployed the top three classifiers, one from Weka (Hall
et al., 2009) and two deep nets from DeepLearning4J
(DL4J) (Team, 2016) to serve as our models for clas-
sifying washed on entry and washed on exit. HyPo
then uses the results with highest accuracy.
• The Sequential Minimal Optimization (SMO)
implementation of the Support Vector Machine
(SVM), which uses heuristics to partition the
training problem into smaller sub-problems and
uses pairwise linear regression to classify. This
method is usually resilient to data overfitting and
by default normalizes the input data (Platt et al.,
1998).
• The Feed-Forward Neural Network (FFNN),
which is a one direction (from input to output)
artificial neural network that performs classifica-
tions based on weight calculations of the network
nodes (Glorot and Bengio, 2010). Using the DL4J
Java library, we developed a 3-layer FFNN with a
random seed of 6, 1000 iterations, a learning rate
of 0.1, and the Stochastic gradient descent opti-
mization algorithm (Gardner, 1984).
• The Recurrent Neural Network (RNN), which
has a feedback loop whereby the immediately pre-
vious step’s output is fed back to the net to affect
the outcome of the current step. We used a 3-layer
RNN with two Graves’ Long Short-Term Memory
(LSTM) layers (Graves, 2012) (input and hidden)
and an output layer along with the same parame-
ters as the FFNN.
5.2 Just-in-Time Alerting
With our previously characterized predictability of
compliance (Zhang et al., 2016), as described in Sec-
tion 2, and necessary pre-configurations to the data
collection instruments, HyPo can provide just-in-time
alerting to remind HCWs to perform hand hygiene
when they are predicted not to comply, using either a
singular prediction or a chain-prediction scheme, de-
pending on if there is adequate time to provide such
notifications between each hand hygiene opportunity.
Suppose that HyPo has just observed a staff
nurse’s compliance on a patient room entry, then the
ML classifiers will predict the same staff’s exit com-
pliance. For instance, if the staff is predicted to be

non-compliant, an alert of red flashing light can be
sent to either the wearable badge or the device at the
appropriate dispenser activation station as a reminder
to the staff; otherwise, no alert is necessary.
If duration of the visit is too short of an interval
to send the notification signal to the devices, then we
can use the probability chain rule (Schum, 1994) to
provide a backup alert to the same staff if necessary.
In this case, the ML models will use the predicted en-
try compliance for the current visit (from the staff’s
exit compliance of the previous visit) to determine
exit compliance of the current visit at a probability
of 89% * 77% = 69%. It is less ideal, but the likeli-
hood of the visit interval being too short is minimal
because the grace period for compliance is set at two
minutes, and if a room visit is within two minutes,
hand hygiene compliance is not required.
5.3 Recommend Training Material
If a staff member is frequently predicted as non-
compliant over a long observation period, HyPo (with
integrated email capabilities) can recommend hand
hygiene guidelines or appropriate training materials
to the staff via email. The goal is to improve compli-
ance on an individual basis.
5.4 Assist Direct Observation
The compliance prediction results can also be used to
assist the current standard practice of direct observa-
tion. With predicted non-compliance reoccurring at a
certain location (i.e., a patient room), HyPo can de-
ploy a human auditor (e.g., by sending a notification)
to observe compliance at the location that should be
given most attention.
6 RELATED WORK
Due to worldwide high demands of HAI prevention, a
number of other researchers have studied approaches
to improve hand hygiene compliance. Although the
gold standard monitoring method is human-centric
(WHO, 2009), (Gould et al., 2011), a wide rage of
studies propose electronic or electronically assisted
hand hygiene compliance monitoring and interven-
tion systems (Ellingson et al., 2014), (Ward et al.,
2014). This section compares our work on the HyPo
app with common electronic intervention systems in-
cluding (1) technology-assisted direct human obser-
vation, (2) counting systems, and (3) automated mon-
itoring systems.
Technology-assisted Human Observation. Direct
observation is the most precise way of controlling
compliance. Several studies use technologies such as
handheld devices and cameras to aid human observa-
tion, aiming at reducing input errors, costs, and time
consumption. Handheld devices are used for data en-
try, and video cameras provide opportunities to reduce
the Hawthorne effect and observe locations that are
remote or hard to access.
Chen et al (Chen et al., 2013), used wireless data
entry devices and a website to allow human observers
to audit compliance. University of North Carolina
Hospitals implemented a “clean-in, clean-out” system
that allowed covert observers and designated nurses to
track compliance using a mobile app and a web portal
(Sickbert-Bennett et al., 2016).
Cameras have been used by Armellino (Armellino
et al., 2013) to increase compliance in an ICU. The
study connected motion sensors near the sinks that
would activate cameras being monitored by remote
auditors. The study by Davis (Davis, 2010) placed
a discreet camera at the entrance of a ward and as-
sessed compliance before and after a sink was placed
pointing to the dispenser.
Unfortunately, these methods still require human
interaction and can bias the results, as the medi-
cal workers know they are being directly observed.
Moreover, audits require trained personnel who are
regularly monitored to ensure quality control.
Counting Systems. Installing counting devices to
measure the remaining sanitation product volume or
the number of dispenser activation times is a quiet
method that is not subject to the Hawthorne effect.
A counter may detect usage patterns and frequency
changes.
Marras (Marra et al., 2010) used dispenser coun-
ters along with direct observation to assess whether
positive deviance in hand hygiene behaviors could
have an impact on reducing HAIs. A downside to
this approach, however, is that counter systems can-
not tell who used the dispensers and therefore are un-
able to evaluate compliance by itself. Morgan et al
(Morgan et al., 2012) provided evidence to support
the claim that dispenser usage data could be more re-
liable than direct human observation to estimate hand
hygiene compliance.
Automated Monitoring Systems using Wearables.
Many automated monitoring systems are capable of
producing feedback or reminders in real or near real
time without human intervention, similar to our ap-
proach.

Fakhry used a motion-triggered system with au-
dible hand washing reminders at each medical de-
partment entrance (Fakhry et al., 2012). Sahud and
Bhanot developed an electronic hand hygiene feed-
back device that reports real-time compliance rate on
a liquid-crystal display visible to all staff in the in-
tervention unit (Sahud and Bhanot, 2009). Edmond
et al installed a sensor network using a credit-card
sized sensor badge on each alcohol dispenser, which
when not activated on room entry or exit beeped with
a red indicating light (Edmond et al., 2010). Simi-
larly, Marra et al employed a wireless network with
sensors on the alcohol dispensers that provide real-
time flashing light feedback to HCWs for hygiene ac-
tivity detection (Marra et al., 2014). Most recently,
Ellison et al proposed a prospective electronic hand
hygiene room entry/exit audible reminder system (El-
lison et al., 2015) that provides a combination of 24-
hour-a-day recording of hand hygiene activities and
real-time computer monitor performance feedback.
Differentiating Factors of Our Approach. All the
prior research we reviewed collected data to propose
strategies that increased hand hygiene performance or
gather conclusions regarding the efficacy of a specific
approach. Our HyPo app is unique since it uses the
gathered data to predict future compliance behavior
instead of notifying appropriate caregivers after non-
compliance has been detected. Other approaches re-
act to non-compliance, while ours predicts compli-
ance ahead of time.
We presented a novel methodology using ML al-
gorithms, which is also unique to our work. Hence,
the aim of our work is also a differentiating factor.
In particular, HyPo evaluates the prediction capabili-
ties of different ML algorithms to predict compliance
ahead of time.
7 CONCLUDING REMARKS
This paper presented a hand hygiene monitoring app
called Hygiene Police (HyPo) that can be deployed as
a service to complement the current monitoring ap-
proach and improve compliance. We showed an ex-
ample data collection process taken place at a 30-bed
ICU where we acquired the handwashing compliance
data. We also described the data transformation pro-
cess HyPo employs to maximize the utilization of the
selected machine learning (ML) classifiers.
Combining the results of real-time compliance
predictions using the correlations identified in (Zhang
et al., 2016), HyPo can provide three types of ser-
vices: (1) just-in-time alerting to remind predicted
non-compliant staff to perform hand hygiene, (2)
recommending training materials to habitually non-
compliant staff via email, and (3) assisting the direct
observation approach by deploying human auditors at
the opportune time and place when and where non-
compliance is frequently predicted to occur. We also
compared our app to related research work and found
that our approach predicted future compliance behav-
ior instead of reacted to non-compliance as in other
approaches. Our methodology using ML algorithms
is unique and is the only work that evaluates ML pre-
diction capabilities in this domain.
In future work, we plan on collecting more com-
pliance data, ideally using the same process as dis-
cussed in the paper. We will use this data to fine tune
the parameters in our ML classifiers to increase the
prediction accuracy. We will also run simulations that
test whether our HyPo app can improve compliance in
general and if the improvement can be sustained over
time in a range of caregiving settings.
REFERENCES
Armellino, D., Trivedi, M., Law, I., Singh, N., Schilling,
M. E., Hussain, E., and Farber, B. (2013). Replicating
changes in hand hygiene in a surgical intensive care
unit with remote video auditing and feedback. Ameri-
can Journal of Infection Control, 41(10):925–927.
Boyce, J. M., Cooper, T., and Dolan, M. J. (2009). Evalua-
tion of an Electronic Device for Real-Time Measure-
ment of Alcohol-Based Hand Rub Use. Infection Con-
trol & Hospital Epidemiology, 30(11):1090–1095.
Chen, L. F., Carriker, C., Staheli, R., Isaacs, P., Elliott,
B., Miller, B. A., Anderson, D. J., Moehring, R. W.,
Vereen, S., Bringhurst, J., Rhodes, L., Strittholt, N.,
and Sexton, D. J. (2013). Observing and improving
hand hygiene compliance: Implementation and refine-
ment of an electronic-assisted direct-observer hand
hygiene audit program. Infection control and hospi-
tal epidemiology: the official journal of the Society of
Hospital Epidemiologists of America, 34(2):207–210.
Davis, C. R. (2010). Infection-free surgery: how to improve
hand-hygiene compliance and eradicate methicillin-
resistant Staphylococcus aureus from surgical wards.
Annals of the Royal College of Surgeons of England,
92(4):316–319.
Eckmanns, T., Bessert, J., Behnke, M., Gastmeier, P., and
R
¨
uden, H. (2006). Compliance with antiseptic hand
rub use in intensive care units the hawthorne effect.
Infection Control, 27(09):931–934.
Edmond, M. B., Goodell, A., Zuelzer, W., Sanogo, K.,
Elam, K., and Bearman, G. (2010). Successful use of
alcohol sensor technology to monitor and report hand
hygiene compliance. The Journal of Hospital Infec-
tion, 76(4):364–365.
EFORE, B. (2009). Hand hygiene technical reference man-
ual.

Ellingson, K., Haas, J. P., Aiello, A. E., Kusek, L., Mara-
gakis, L. L., Olmsted, R. N., Perencevich, E., Pol-
green, P. M., Schweizer, M. L., Trexler, P., VanAm-
ringe, M., and Yokoe, D. S. (2014). Strategies to Pre-
vent Healthcare-Associated Infections through Hand
Hygiene. Infection Control and Hospital Epidemiol-
ogy, 35(8):937–960.
Ellison, R. T., Barysauskas, C. M., Rundensteiner, E. A.,
Wang, D., and Barton, B. (2015). A Prospective
Controlled Trial of an Electronic Hand Hygiene Re-
minder System. Open Forum Infectious Diseases,
page ofv121.
Fakhry, M., Hanna, G. B., Anderson, O., Holmes, A., and
Nathwani, D. (2012). Effectiveness of an audible re-
minder on hand hygiene adherence. American Journal
of Infection Control, 40(4):320–323.
Gardner, W. A. (1984). Learning characteristics of
stochastic-gradient-descent algorithms: A general
study, analysis, and critique. Signal Processing,
6(2):113–133.
Glorot, X. and Bengio, Y. (2010). Understanding the dif-
ficulty of training deep feedforward neural networks.
In Aistats, volume 9, pages 249–256.
Goldberg, D. E. (1989). Genetic algorithms in search, opti-
mization and machine learning. Addison-Wesley.
Gould, D. J., Drey, N. S., and Creedon, S. (2011). Rou-
tine hand hygiene audit by direct observation: has
nemesis arrived? The Journal of Hospital Infection,
77(4):290–293.
Graves, A. (2012). Supervised sequence labelling. In Super-
vised Sequence Labelling with Recurrent Neural Net-
works, pages 5–13. Springer.
Guyon, I. and Elisseeff, A. (2003). An introduction to vari-
able and feature selection. Journal of machine learn-
ing research, 3(Mar):1157–1182.
Hall, M., Frank, E., Holmes, G., Pfahringer, B., Reutemann,
P., and Witten, I. H. (2009). The weka data min-
ing software: an update. ACM SIGKDD explorations
newsletter, 11(1):10–18.
John, G. H. and Langley, P. (1995). Estimating continuous
distributions in bayesian classifiers. In Eleventh Con-
ference on Uncertainty in Artificial Intelligence, pages
338–345, San Mateo. Morgan Kaufmann.
Kohavi, R. and John, G. H. (1997). Wrappers for feature
subset selection. Artificial Intelligence, 97(1-2):273–
324. Special issue on relevance.
Marra, A. R., Guastelli, L. R., Arajo, C. M. P. d., Santos,
J. L. S. d., Lamblet, L. C. R., Silva, M., Lima, G. d.,
Cal, R. G. R., Paes, n. T., Neto, M. C., Barbosa, L.,
Edmond, M. B., and Santos, O. F. P. d. (2010). Pos-
itive Deviance A New Strategy for Improving Hand
Hygiene Compliance. Infection Control & Hos-
pital Epidemiology, 31(1):12–20.
Marra, A. R., Sampaio Camargo, T. Z., Magnus, T. P.,
Blaya, R. P., Dos Santos, G. B., Guastelli, L. R.,
Rodrigues, R. D., Prado, M., Victor, E. d. S., Bo-
gossian, H., Monte, J. C. M., dos Santos, O. F. P.,
Oyama, C. K., and Edmond, M. B. (2014). The use
of real-time feedback via wireless technology to im-
prove hand hygiene compliance. American Journal of
Infection Control, 42(6):608–611.
Morgan, D. J., Pineles, L., Shardell, M., Young, A., Elling-
son, K., Jernigan, J. A., Day, H. R., Thom, K. A., Har-
ris, A. D., and Perencevich, E. N. (2012). Automated
hand hygiene count devices may better measure com-
pliance than human observation. American Journal of
Infection Control, 40(10):955–959.
Platt, J. et al. (1998). Sequential minimal optimization: A
fast algorithm for training support vector machines.
Sahud, A. G. and Bhanot, N. (2009). Measuring hand hy-
giene compliance: a new frontier for improving hand
hygiene. Infection Control and Hospital Epidemiol-
ogy, 30(11):1132.
Schum, D. A. (1994). The evidential foundations of proba-
bilistic reasoning. Northwestern University Press.
Shrestha, S. K., Sunkesula, V. C., Kundrapu, S., Tomas,
M. E., Nerandzic, M. M., and Donskey, C. J. (2016).
Acquisition of clostridium difficile on hands of health-
care personnel caring for patients with resolved c. dif-
ficile infection. Infection Control & Hospital Epi-
demiology, 37(04):475–477.
Sickbert-Bennett, E. E., DiBiase, L. M., Schade Willis,
T. M., Wolak, E. S., Weber, D. J., and Rutala, W. A.
(2016). Reducing health careassociated infections by
implementing a novel all hands on deck approach for
hand hygiene compliance. American Journal of Infec-
tion Control, 44(5, Supplement):e13–e16.
Team, D. D. (2016). Deeplearning4j: Open-source dis-
tributed deep learning for the jvm. Apache Software
Foundation License, 2.
Ward, M. A., Schweizer, M. L., Polgreen, P. M., Gupta,
K., Reisinger, H. S., and Perencevich, E. N. (2014).
Automated and electronically assisted hand hygiene
monitoring systems: A systematic review. American
Journal of Infection Control, 42(5):472–478.
WHO (2009). A guide to the implementation of the WHO
multimodal hand hygiene improvement strategy.
Zhang, P., White, J., Schmidt, D., and Dennis, T. (2016). A
preliminary study of hand hygiene compliance char-
acteristics with machine learning methods. (ISIS-16-
101).
