
Designing a Social Machine for the Heart Manual Service
Vanessa Hanschke
1
, Areti Manataki
2
, Cristina Adriana Alexandru
2
, Petros Papapanagiotou
2
,
Carolyn Deighan
3
, Louise Taylor
3
and Dave Robertson
2
1
Microsoft, Milan, Italy
2
School of Informatics, The University of Edinburgh, Edinburgh, U.K.
3
The Heart Manual Department, NHS Lothian, Edinburgh, U.K.
Keywords:
Social Machine, Heart Manual, Self-management Rehabilitation, Participatory Design.
Abstract:
Social machines are emerging as a focus of research within the field of informatics as they begin to become the
central administrator of our everyday communications. The difficulty of applying such systems to specialised
contexts, such as healthcare, calls for guidelines on how to design them, so that they become truly useful.
In collaboration with the Heart Manual Department, this project is an attempt at finding suitable methods for
designing social machines in a healthcare context. It suggests that adopting a participatory approach where
stakeholders are active, equal participants throughout the design process leads to a more usable, likeable, and
thus more successful social machine. We describe the process of designing a social machine for the Heart
Manual service, in which requirements were elicited through various participatory design methods and a proof
of concept evaluation was carried out with a prototype. The prototype was received largely positively and
scored highly on the System Usability Scale, indicating the success of the proposed methodology.
1 INTRODUCTION
The Heart Manual (The Heart Manual Department,
2016) is the UK’s leading home-based supported self-
management programme for individuals recovering
from acute myocardial infarction and/or revasculari-
sation. With the help of a team of facilitators (typi-
cally nurses, psychologists or general practitioners),
who are based in different locations nationally and in-
ternationally, it guides patients through a series of ses-
sions which empower them to improve their lifestyle.
Apart from the initial training that facilitators receive,
there is no infrastructure for community building, and
knowledge exchange takes place in an ad-hoc fash-
ion, with individual facilitators contacting the Heart
Manual (HM) team to clarify their questions.
Social machines (Hendler and Berners-Lee, 2010)
can provide an appropriate infrastructure for such in-
teractions. Through a closer interaction between hu-
mans and machines, such systems can support com-
munication and the sharing of experience, and con-
tribute to a sense of community. Despite recent re-
search interest in this topic, there are still no best prac-
tices for designing successful social machines.
In this paper, we propose a participatory approach
to the design of healthcare social machines. We posit
that the involvement of users throughout the design
process can address usability and likeability aspects,
which are key success factors for health technologies.
In particular, we describe our experience in employ-
ing participatory design methods to develop a social
machine for the HM facilitators. Background infor-
mation is provided in Section 2 and our methodology
is introduced in Section 3, followed by an account of
requirement elicitation in Section 4. We next present a
first prototype created to collect quick feedback (Sec-
tion 5) and how this was further adapted and evaluated
by HM facilitators (Section 6). We conclude with an
overview of lessons learnt and future work.
2 BACKGROUND
The Heart Manual (The Heart Manual Department,
2016) is a home based cardiac rehabilitation pro-
gramme, supported by trained facilitators and ev-
idenced by three randomized control trials (Clark
et al., 2011). It consists of six weekly sessions
that include education, exercise, relaxation and stress
management. The programme was digitised in 2015
Hanschke V., Manataki A., Alexandru C., Papapanagiotou P., Deighan C., Taylor L. and Robertson D.
Designing a Social Machine for the Heart Manual Service.
DOI: 10.5220/0006249004350440
In Proceedings of the 10th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2017), pages 435-440
ISBN: 978-989-758-213-4
Copyright
c
2017 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
435

(Deighan et al., 2015), and there is now the oppor-
tunity to extend it with recent advances in large and
distributed open systems, such as social machines.
Social machines are technology-enabled social
systems, seen as computational entities governed by
both computational and social processes (Hendler and
Berners-Lee, 2010). They are defined as “Web-based
socio-technical systems in which the human and tech-
nological elements play the role of participant ma-
chinery with respect to the mechanistic realization of
system-level processes” (Smart et al., 2014). Social
machines are a recent research theme, with related
work focusing mostly on analysing existing exam-
ples, such as Facebook, Wikipedia and Stack Over-
flow (Shadbolt et al., 2013; Smart et al., 2014). Lit-
erature on designing social machines is relatively
sparse. Donath (Donath, 2014) approaches this
topic in terms of conceptualising communities and
strengthening ties, while Murray-Rust and Robertson
(Murray-Rust and Robertson, 2015) suggest using ex-
isting social machines that bring together designers
and developers to generate new social machines. Both
approaches push for an understanding of the users and
a close tailoring of the social machine to its partici-
pants. Yet we are still lacking guidelines for practical
requirement elicitation for new social machines.
In healthcare, a number of social machines aim
to bring patients together to help them live health-
ier lives. PatientsLikeMe.com, for instance, con-
nects patients with similar conditions, allowing for
peer support and knowledge sharing, while the Fit-
bit and Nike+ FuelBand online communities operate
as behavioural interventions that complement activ-
ity trackers. However, the majority of such machines
lack a clinical evaluation, and there are concerns
around confidentiality and patient self-diagnosis.
Similarly to the proposed HM social machine,
other machines connect clinicians rather than patients
(e.g. doc2doc.bmj.com). A recent review (Rolls et al.,
2016) explores how social media have helped health
professionals worldwide create virtual communities
where they exchange knowledge and network. How-
ever, the paper does not give a comprehensive re-
view of design methodologies. The closest example
in this literature were the trials for the Midwifery Fo-
rum (Brooks et al., 2004). However, the participatory
design mentioned in the paper was limited to proto-
type evaluation, rather than collaborative design.
3 METHODOLOGY
The lack of guidelines for designing social machines
is a considerable gap, especially in the healthcare con-
text, where technology uptake is relatively slow. In-
cluding the capabilities of the users in the interface
design can have a significant effect on its usability
and, thus, the success of a healthcare social machine.
We thus adopt a participatory approach to the de-
sign of a social machine for the HM facilitators. Par-
ticipatory design is a user-centred design methodol-
ogy, in which the end-user is made a full participant
of the design process, typically by interacting with
mock-ups, prototypes and other tools that represent
developing systems (Schuler and Namioka, 1993; Si-
monsen and Robertson, 2012). We hypothesise that
participatory design is an effective method for the de-
sign of a social machine of health services with re-
spect to system likeability and usability, as measured
by a small-scale evaluation of a web-based prototype.
An iterative development process was followed,
consisting of three main phases: requirements elicita-
tion, low-tech paper-based prototype design and high-
tech wireframe prototype development. Inspired by
the spiral model of software development, each phase
included a repetition of steps, namely planning ob-
jectives, collecting information from users, analysing
their feedback and creating a next level prototype (or
list of requirements, in the case of Phase 1).
4 ESTABLISHING
REQUIREMENTS
We utilised Shadbolt’s constructs for classifying so-
cial machines (Shadbolt et al., 2013; Smart et al.,
2014) to establish a set of questions which provide
a framework for gathering requirements for a social
machine. The questions devised cover the tasks and
purpose of participation, participants and their roles,
as well as motivation and incentives (see Figure 1).
Three main methods were used for establishing re-
quirements, described hereafter:
Training session: We first attended a two-day train-
ing session that prepares healthcare professionals to
become facilitators of the HM programme. This al-
lowed us to gain a clearer understanding of their role
and the challenges they face (e.g. cultural issues that
might impede patients from following dietary restric-
tions). To address such challenges, the session also
made apparent the usefulness of a space for facilita-
tors to discuss their opinions and experiences, share
good practice and provide peer support, especially in
the case of facilitators working in remote areas.
Brainstorming session: This was organised in the
form of a “Future Workshop” towards idea genera-
tion (Simonsen and Robertson, 2012). Future work-
shops are common in participatory design and consist
HEALTHINF 2017 - 10th International Conference on Health Informatics
436
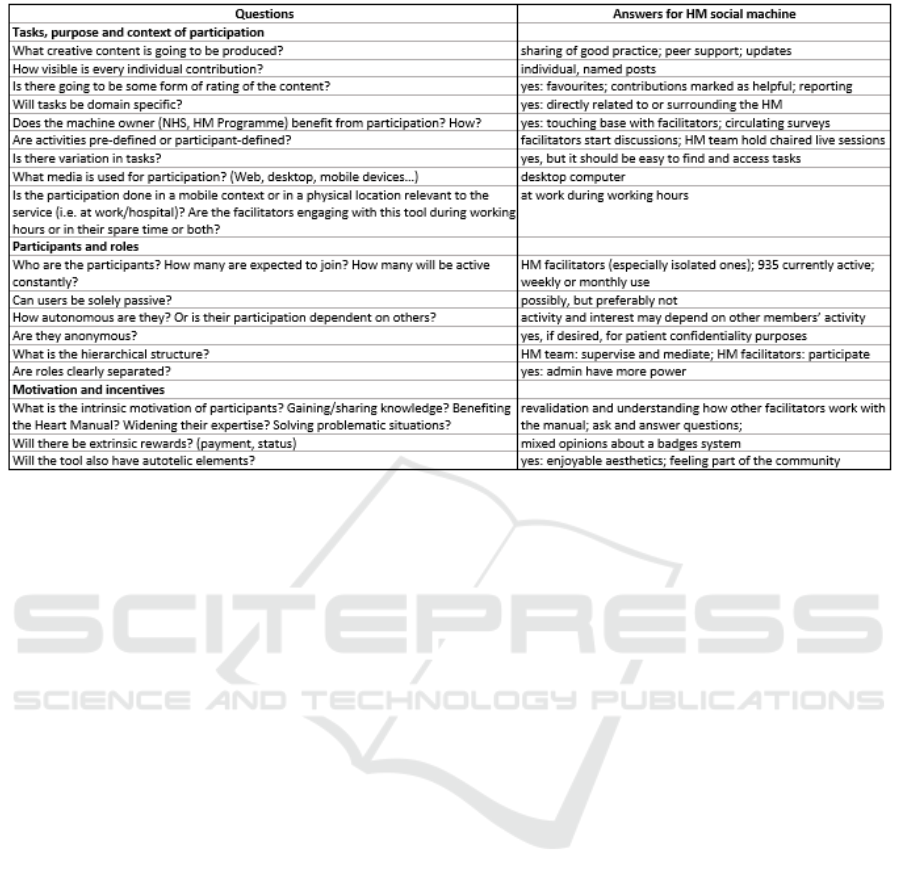
Figure 1: Questions to guide requirement gathering for a social machine, and answers for the HM social machine.
of three stages: i) critiquing the present, ii) envision-
ing the future and iii) implementing - moving from
present to the future. Four clinicians participated in
the workshop: a health psychologist, an assistant psy-
chologist, a specialist nurse who is also an HM facili-
tator, and the lead of the HM team. Following the Fu-
ture Workshop structure, we first focused on existing
communication between clinicians, and then we dis-
cussed the goals of the HM social machine. Based on
these goals, the participants were then asked to devise
dream solutions, unrestricted by technical knowledge
or possibilities. Three examples of social machines
were then presented to them: Facebook, doc2doc and
Stack Overflow. These were carefully chosen, so as to
prompt discussions around different forms of commu-
nication, privacy and confidentiality regulations, as
well as user reputation, respectively. This presenta-
tion initiated a new discussion about the dream solu-
tions, leading to a jointly ordered list of requirements.
Telephone interviews: Three semi-structured inter-
views with additional facilitators were organised so
as to verify some of the ideas collected previously, as
well as to clarify points where participants had dif-
fering opinions. For example, participants gave their
opinion about the motivation for a social machine and
the associated concerns, the need for private groups
or private messaging, anonymous posting, etc.
The brainstorming session and telephone inter-
views were recorded (with the written consent of the
participants), transcribed and analysed following top-
down thematic analysis, as guided by the questions in
Figure 1. Outputs included explicit answers to these
questions (presented in the same figure), leading to
a list of functional and non-functional requirements.
Among functional requirements, we distinguish the
following elements: discussion forum, quizzes, sur-
veys, blogs, events and notepad. Posting anony-
mously and tagging content as helpful were deemed
desirable, but setting up groups or private messaging
were not. The list of non-functional requirements in-
cluded high levels of security and privacy, low main-
tainability and the option to report forum abuse.
5 FIRST PROTOTYPE AND ITS
EVALUATION
Following best practices in participatory design (Si-
monsen and Robertson, 2012) and based on the re-
quirements gathered, we created a low-fidelity, paper-
based website prototype, so as to quickly obtain feed-
back and generate ideas at an early stage of the design
process, before committing to design decisions that
would be harder to change later on. A set of pages
were designed to capture the main functionality of the
website: i) homepage, ii) discussions, iii) submitting
a discussion (see Figure 2) and iv) user profile.
A prototyping session was organised to collect
feedback, with the partaking of the four participants
from the brainstorming session. Each participant was
questioned individually around two activities. In the
first activity, they were given a set of cut out items
(e.g. buttons and taskbars) which they could arrange
Designing a Social Machine for the Heart Manual Service
437
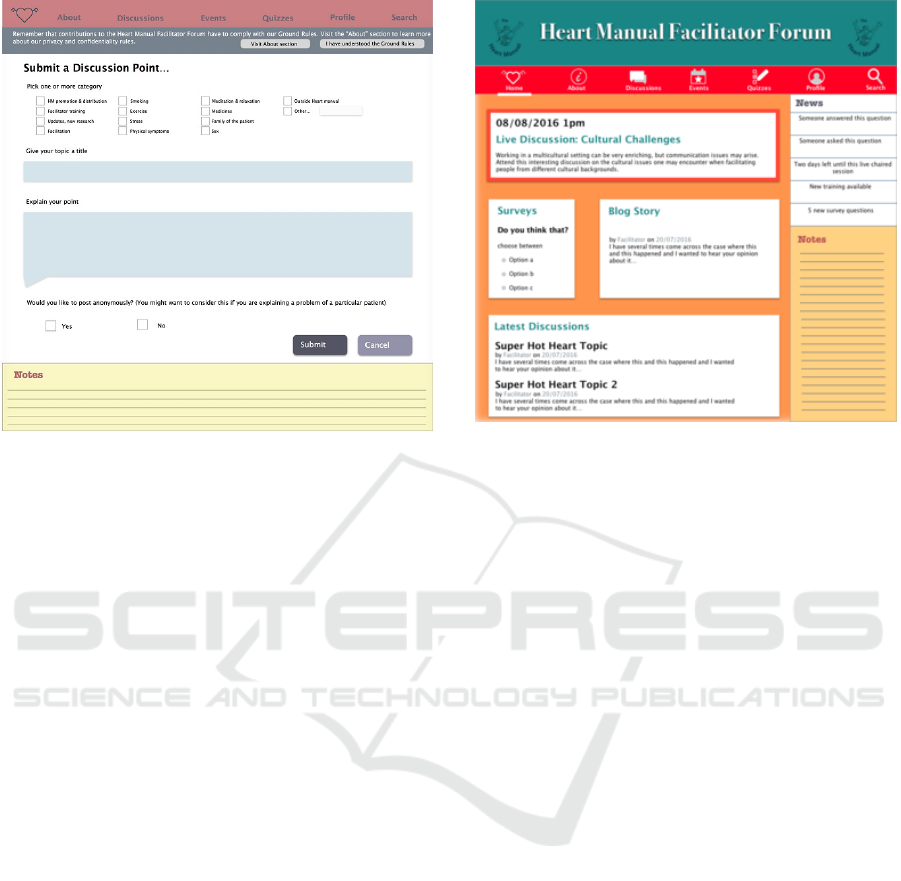
Figure 2: Paper-based prototype for submitting a discus-
sion.
on a sheet of paper to reflect their idea of the home-
page. In the second activity, they were presented sug-
gestions for the design of the screens to elicit opinions
and given screen print-outs to annotate. Topics dis-
cussed included the notes facility and the presentation
of ground rules for participating in the discussions, so
as to avoid misinformation and breach of confiden-
tiality. The prototyping session was audio-recorded,
handwritten notes were taken and any visual material
created was documented with photographs. These re-
sources were analysed qualitatively using a combina-
tion of top-down and bottom-up thematic analysis. In
general, it was found that participants were pleased
with the layout that was presented to them. Opinions
were evenly split on the presentation of the ground
rules and on a simple versus busy look of the home-
page. A pop-up window and a busy feel, respectively,
were chosen by the designer for the next version of
the prototype, which would be further evaluated, thus
reducing the associated risk.
6 FINAL PROTOTYPE AND ITS
EVALUATION
A hi-fi web-based prototype was developed by adapt-
ing the first prototype given the feedback gathered.
It was presented on a browser and made from linked
screens to generate a feel of the interactions that
would take place (see Figure 3). Its main difference
to the first prototype was that users could interact with
the system and see its dynamics in operation. The pro-
Figure 3: The home page in the final prototype.
totype was not fully functional, but a proof of concept.
It was designed to work for certain scenarios that were
set up for the evaluation: 1) starting a discussion, 2)
entering a discussion point, 3) marking a contribution
as helpful, 4) reporting a contribution as harmful, 5)
entering an event, 6) adding items to favourites, and
7) accessing favourites.
The prototype was tested with seven potential
users (five members of the HM team and two facil-
itators) for usability and likeability. Three of the HM
team members had participated in the first prototyp-
ing session, while the remaining two had not been in-
volved in any of the prior activities. The two addi-
tional facilitators had been interviewed for establish-
ing requirements. The evaluation was divided in two
main activities (i.e. think aloud and questionnaire),
while a survey was set up for carrying it out remotely.
Think Aloud and Short Structured Interviews: For
this part of the evaluation, participants were presented
with the prototype on a laptop. They were given four
sets of tasks: i) submit a new discussion, ii) find a dis-
cussion, mark it as a favourite, mark and report a con-
tribution, iii) find an event and mark it as a favourite
and iv) revisit favourites. The participants were asked
to “think aloud” while completing these tasks, i.e.
explain their thought process, so as to make explicit
where they were stuck and why, what they were look-
ing for, what their expectations were, etc. Following
their think aloud, participants gave their opinion about
the presented features and their intuitiveness.
Questionnaire: Participants were next presented
with a questionnaire around usability and likeabil-
ity, which included three sets of questions: i) SUS
scale (Brooke, 2013), ii) how often (in a scale from 1,
HEALTHINF 2017 - 10th International Conference on Health Informatics
438

Figure 4: Accuracy and completeness in Think Aloud tasks.
i.e. never, to 5, i.e. very often) participants thought
they would use certain features and iii) whether they
thought certain aspects were particularly enjoyable,
unenjoyable or concerning and why.
Survey: Participants who performed the evaluation
remotely were emailed an online survey containing
the same questionnaire and Think Aloud tasks, and
a link to the prototype. They were also asked to put
remarks in comments if they were stuck at any point,
especially if they were unable to complete the task.
The five participants of the HM team carried out
the different evaluation activities in the presence of
the researcher. One of the facilitators completed the
evaluation using the survey, while the other completed
it remotely, with the researcher on the phone and
watching the screen navigation in real time.
The Think Aloud sessions and structured inter-
views were audio recorded (with the participants’ per-
mission), transcribed and, together with the survey
data, analysed qualitatively using a combination of
top-down and bottom-up thematic analysis. Inter-
view or on-line survey replies on intuitiveness were
attributed a ranking from 1 to 5. During the Think
Aloud session, the time for completing each task
was recorded, and notes were taken about whether it
was completed successfully and the number of errors.
These data were analysed quantitatively with regards
to efficiency, task accuracy and completeness. Ques-
tionnaires were also analysed quantitatively.
Figure 4 presents the accuracy and completeness
measured during the Think Aloud session. All partic-
ipants were able to complete all tasks independently,
except for one participant who required further expla-
nations on two tasks. The errors observed had to do
with misunderstanding instructions and with the fact
that the search bar lacked functionality at this stage.
Regarding efficiency, the average time in seconds
for each of Tasks 1-4 was: 57.4 (SD 57.4), 67.4 (SD
43.5), 21 (SD 8) and 35 (SD 19.4), respectively. Note
that the standard deviations here are inevitably large,
given the small number of participants recruited.
Based on participant remarks and answers during
the Think Aloud session and the short structured in-
terviews, all tasks scored highly on intuitiveness: the
average intuitiveness score (on a scale from 1 to 5) for
Tasks 1-4 was 4.6, 4.4, 5 and 3.7, respectively.
The average SUS score was 86.4 (SD 18.02), indi-
cating “excellent” satisfaction, according to published
grade rankings of SUS scores (Bangor et al., 2009).
With the exception of one participant who gave a
score of 50 (i.e. “ok”), the rest of the scores ranged
from 80 (i.e. “Good”) to 100 (i.e.“Best imaginable”).
The results to the question of how often partici-
pants would use certain features ranged from 3 (i.e.
every now and then) to 4.43 (i.e. between regularly
and very often). The former was assigned to the use
of the notepad for keeping personal notes, while the
latter to reading discussions and looking up events.
A variety of features were found to be enjoyable.
Discussions, in particular, were mentioned by five out
of the seven participants. For instance, a facilitator
mentioned: “Starting a discussion. I liked that. And
I liked it because if I know I’ve got a thought in my
head and I can put it out there and see what my col-
leagues and counterparts have. So it can validate the
ideas I might have”. Three facilitators mentioned that
the favourites feature also seemed very useful. No
feature was pointed out as unenjoyable or concerning.
7 CONCLUSIONS
Based on the quantitative measures presented in Sec-
tion 6, the hi-fi prototype was a great success, per-
forming well on both satisfaction and effectiveness.
The SUS score was very positive, corresponding to
an “excellent” usability grade. Only one user was un-
able to complete two tasks independently, totalling an
overall average of 92% success per user. The overall
error rate was low, with no errors on many tasks and
less than one error on average for tasks with errors.
Some of the errors, such as accessing the search bar
(which was not yet functional), are easily resolvable.
The efficiency of the tasks can only be compared be-
tween each other, as we do not have an absolute mea-
sure of how long these should take. A learning effect
between Tasks 1 and 3 can be noted, as they take a
similar amount of clicks, but the latter is faster.
The system seemed to have a high level of accep-
tance, as most features were marked to be used be-
tween “every now and then” and “very often”. This
shows that the features proposed in the prototype were
in line with the expectations of the participants. This
is also demonstrated by the fact that discussions were
highlighted as a particularly enjoyable feature.
Designing a Social Machine for the Heart Manual Service
439

This interdisciplinary project highlighted several
themes which we expect to be recurring when design-
ing social machines for health professionals, given the
general characteristics of the domain. Firstly, design-
ing for time constraints is crucial, given that clini-
cians are very busy. Hence, an easily learnable inter-
face is recommended, where all features are directly
accessible on display. Security is another important
theme, and access control aspects should be carefully
thought out. Furthermore, social machines that sup-
port knowledge sharing should allow users to identify
misinformation, which is critical in healthcare.
The choice of participatory design allowed us to
identify these themes and concerns, which might not
have been addressed without input from the users.
Our overall experience of using participatory design
in healthcare was greatly positive. Participants were
very motivated and gave thorough and careful feed-
back. On the other hand, recruiting participants was
the biggest issue, as healthcare professionals are gen-
erally very busy and communication channels tend to
be controlled. We worked around this issue by ensur-
ing that different types of stakeholders were involved
in the study, from experienced to new facilitators and
from isolated workplaces to busy hospitals.
The range of participatory design methods used
provided us with a wealth of both quantitative and
qualitative data and allowed for a good level of user
engagement and interaction. The two-hour brain-
storming session, which resulted in 26 pages of tran-
script, allowed participants to exchange and visualise
ideas, and thus served as a good basis for establish-
ing requirements. The phone interviews did not pro-
vide the same level of idea generation, but carrying
them out separately with each facilitator provided a
safe space for them to express their personal views on
a HM machine. Furthermore, the paper-based proto-
typing session was found to be very useful, as it al-
lowed us to concretise ideas at an early stage.
The questions presented in Figure 1 were partic-
ularly useful for designing the HM social machine.
They guided the requirement elicitation process, from
structuring the brainstorming session to analysing the
qualitative data obtained. We would, hence, recom-
mend their use to other social machine designers.
In the future, we wish to continue using the partic-
ipatory design methodology and implement the feed-
back received as part of the current study. In order
to create a truly usable social machine for the Heart
Manual service, we plan to include more participants
and to investigate new topics, such as the moderat-
ing role of the HM team. Applying the methodology
presented in this paper to the design of other social
machines is another exciting avenue for future work.
ACKNOWLEDGEMENTS
This research was supported by the EPSRC SociaM
project under grant EP/J017728/1.
REFERENCES
Bangor, A., Kortum, P., and Miller, J. (2009). Determining
what individual SUS scores mean: Adding an adjec-
tive rating scale. J. Usability Studies, 4(3):114–123.
Brooke, J. (2013). SUS: a retrospective. Journal of usability
studies, 8(2):29–40.
Brooks, F., Pospopa, C., and Schott, P. (2004). Midwifery
on the net: new communication technology. British
Journal of Midwifery, 12(2):107–110.
Clark, M., Kelly, T., and Deighan, C. (2011). A system-
atic review of the heart manual literature. European
Journal of Cardiovascular Nursing, 10(1):3–13.
Deighan, C., Pagliari, C., Michalova, L., Elliott, J., Brook-
mann, F., and Taylor, L. (2015). Digital heart manual:
making technology accessible with a user-friendly re-
source. In Health Informatics Scotland Conference.
British Computer Society.
Donath, J. (2014). The social machine: designs for living
online. MIT Press.
Hendler, J. and Berners-Lee, T. (2010). From the seman-
tic web to social machines: A research challenge for
AI on the world wide web. Artificial Intelligence,
174(2):156–161.
Murray-Rust, D. and Robertson, D. (2015). Bootstrapping
the next generation of social machines. In Crowd-
sourcing, pages 53–71. Springer.
Rolls, K., Hansen, M., Jackson, D., and Elliott, D. (2016).
How health care professionals use social media to cre-
ate virtual communities: An integrative review. Jour-
nal of Medical Internet Research, 18(6):e166.
Schuler, D. and Namioka, A., editors (1993). Participatory
Design: Principles and Practices. L. Erlbaum Asso-
ciates Inc., Hillsdale, NJ, USA.
Shadbolt, N. R., Smith, D. A., Simperl, E., Van Kleek, M.,
Yang, Y., and Hall, W. (2013). Towards a classification
framework for social machines. In Proceedings of the
22nd International Conference on World Wide Web,
pages 905–912. ACM.
Simonsen, J. and Robertson, T. (2012). Routledge Interna-
tional Handbook of Participatory Design. Routledge.
Smart, P., Simperl, E., and Shadbolt, N. (2014). A taxo-
nomic framework for social machines. In Social Col-
lective Intelligence, pages 51–85. Springer.
The Heart Manual Department (2016). The Heart Manual.
http://www.theheartmanual.com.
HEALTHINF 2017 - 10th International Conference on Health Informatics
440
