
Technologies of Effective Training Control in Amateur Triathlon
Non-Invasive Hemodynamic Measurements and Exercise Testing for Accurate
Training Prescription
Anna Zakharova and Kamiliia Mekhdieva
Institute of Physical Education, Sport and Youth Policy, Ural Federal University
named after the first President of Russia B.N. Yeltsin, Mira Street, Yekaterinburg, Russia
Keywords: Triathlon, Amateur Athletes, Training and Testing, Gas-exchange Measurement, Hemodynamic Indicators.
Abstract: Although issues of training in professional triathlon are well highlighted and studied, the approach to
supply, including medical-pedagogical aspects, still remains under debates in amateur triathlon. The
intensity and volume of exercise loads in amateur triathlon tend to those in professional sports, whereas
there is no consensus on efficient training strategy for active individuals engaged in amateur endurance
sports. The objective of the study was to define the role of cardiovascular testing in training program design
in amateur triathlon. Twenty-four healthy active male amateur triathletes aged 26-43 years participated in
the study. Four trials of testing (hemodynamics and gas-exchange monitoring) were conducted to justify the
amendments to training schedule. Based on significant differences of initial hemodynamic parameters (SV,
SI, EDV, EDI) subjects were divided into 2 groups. Determining of the weak aspects of their functional
state enabled to develop an efficient training schedule at the ongoing experiment stages. The obtained
results of the final testing showed significant increase in VO
2max
, maximal power (P
max
) in cycling stress-test
and LV volume characteristics in amateur triathletes.
1 INTRODUCTION
Triathlon is known as a multiple-stage competition.
It involves three endurance disciplines: swimming,
cycling, and running (O’Tool, 1995). Originated in
the beginning of the 20th century, it started the
Olympic history in 2002. In our days the
International Triathlon Union (ITU) consolidates
119 national federations with more than 100
thousand of triathletes. But what is more interesting,
social phenomena of triathlon popularity has non-
sportive background: triathlon is a new form of reply
to mid-life crisis. The explanation is quite easy:
participating in triathlon is a great opportunity to
change oneself and to become a legend. Nowadays
middle-aged people come in amateur triathlon to
find something challenging but available.
Although population of healthy individuals
engaged in amateur sports gradually increases, there
is quite a broad range of possible health issues that
need to be considered. Considering that professional
athletes are provided by high-quality assistance and
medical-biological supply, aimed to minimize the
possible medical risks (Corrado, 2005), amateurs’
health and well-being are on their own responsibi-
lity. As their training intensity and volume almost
come up to professional sport, hence it is critically
important to prescribe trainings with reasonable
accuracy.
Stated above enabled us to formulate the aim of
the study – to estimate the efficiency of stage fun-
ctional testing based on non-invasive hemodynamics
measurements and exercise testing for accurate and
correct training prescription.
2 ORGANIZATION AND
METHODS
Subjects. Twenty-four healthy male amateur
triathletes aged 26-43 (mean age 33.8±4.74 years,
height – 181±5.66 cm, body mass – 80.8±8.86 kg)
were recruited for the study. The participants of the
study had no professional sports background. All
subjects were free of cardiovascular or any other
chronic disease. The investigation conforms to the
principles of the Declaration of Helsinki of the
World Medical Association. Athletes had been infor-
med of the procedures, methods, benefits and possi-
Zakharova, A. and Mekhdieva, K.
Technologies of Effective Training Control in Amateur Tr iathlon - Non-Invasive Hemodynamic Measurements and Exercise Testing for Accurate Training Prescription.
DOI: 10.5220/0006082000830088
In Proceedings of the 4th International Congress on Sport Sciences Research and Technology Support (icSPORTS 2016), pages 83-88
ISBN: 978-989-758-205-9
Copyright
c
2016 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
83

ble risks involved in the study before their written
consent was obtained. The study was approved by
the Ural Federal University Ethics Committee.
Research Design. Participants were divided into 2
groups according to initial functional state, evaluated
by means of hemodynamic measurements. The
experiment was carried out from December 2015 to
August 2016 and included four consecutive trials of
hemodynamics and gas-exchange measurements
(Table 1). Testing schedule was based on training
periods. All tests were conducted in the laboratory
“Sports and health technologies” of the Institute of
Physical education, sports and youth policy, UrFU.
Exercise Testing. All athletes underwent 12-lead
ECG before exercise testing (ET). To evaluate
aerobic capacity of athletes, the stress-system
Schiller AG Cardiovit AT-104 (Schiller AG,
Switzerland) was used. The maximal ramp cycling
test protocol was applied in accordance with
ACC/AHA 2002 guideline update for exercise
testing (2006). VO
2max
was determined by indirect
calorimetry with the use of portable desktop
metabolic system FitmatePro (COSMED, Italy).
After a 1 min warm-up, subjects started at zero load,
continuously increasing by 40 W per minute until
exhaustion in order to determine HR
max
, VO
2max
,
maximum attained load (P
max
), VE
max
, anaerobic
threshold (AT). Heart rate monitoring was carried
out with Garmin Forerunner 305 (Garmin, USA)
during the test and immediate post-exercise period
(5 minutes).
2.1 Hemodynamic Measurements
The hemodynamic monitor MARG 10-01
"MicroLux" (Chelyabinsk, Russia) is usually used in
emergency and operation rooms. The device
functioning is based on such noninvasive methods of
hemodynamic monitoring as impedance cardiogra-
phy and spectrophotometry, electrocardiogram
monitoring (ECG), pulse oximetry monitoring,
reography and central hemodynamics monitoring,
blood pressure and temperature.
Measuring Methods. For the experiment a patient
(athlete) was in supine position. Before recording all
subjects were at rest in supine position during 10
minutes. All measured indicators of the central
hemodynamics were automatically registered with 8
ECG electrodes by MicroLux software with beat-to-
beat record.
Central hemodynamic indicators are presented in
four groups: perfusion (stroke volume, cardiac
output, stroke index, cardiac index), preload (end-
diastolic volume, end-diastolic index), afterload (the
index of total peripheral resistance, stroke index of
total peripheral resistance), contractility and left
ventricular activity (contractility index, ejection
fraction; index of left ventricle activity, stroke index
of left ventricle (LV) activity). To investigate the
functional state of young athletes we chose the most
informative for endurance athletes’ hemodynamic
indicators and indices (Shishkina, 2013):
Heart rate (HR, bpm) is the most accessible and
informative indicator of the development of athletes’
cardiovascular system; stroke volume (SV, ml)
values should be a reference point in examining
athletes in endurance sport; stroke index (SI, ml/m
2
)
is the ratio of stroke volume to body surface area;
end-diastolic volume (EDV, ml) is the maximum
amount of blood received in left ventricle at the end
of diastole; end-diastolic index (EDI, ml/m
2
) is the
ratio of end-diastolic volume to the body surface
area in square meters; end diastolic volume provides
sufficient stroke volume and cardiac output and is
the guarantor of good tolerance to high intensity
load in training and competitive activities; ejection
fraction (EF, %) changes from 57 to 65 and serves
as an indicator of fitness level as well as the
intensity of previous training process.
Hemodynamics is described by three general
indicators: volemia, inotropy, vascular tone. The
above-mentioned indicators are shown at the
monitor as a percentage of normal values. The
deviations of more than 25% are considered too
high/low in healthy people.
2.2 Cardiovascular Monitoring during
Exercise Test
Maximal cycling test is commonly used in
assessment of physical fitness and aerobic capacity.
It is quite informative, relatively safe and easy
reproducible. Gas-exchange measurements during
stress-test enabled to obtain important information
on athletes’ aerobic capacity (Vilikus, 2012) and
accurate values of metabolic changes under stress
conditions.
The following parameters were simultaneously and
continuously recorded during exercise testing:
oxygen consumption (VO
2
, ml/kg/min), heart rate
(HR, bpm), systolic blood pressure (SBP, mm Hg),
diastolic blood pressure (DBP, mmHg), cycling
load(P, W), respiratory ventilation (VE, l/min).
icSPORTS 2016 - 4th International Congress on Sport Sciences Research and Technology Support
84
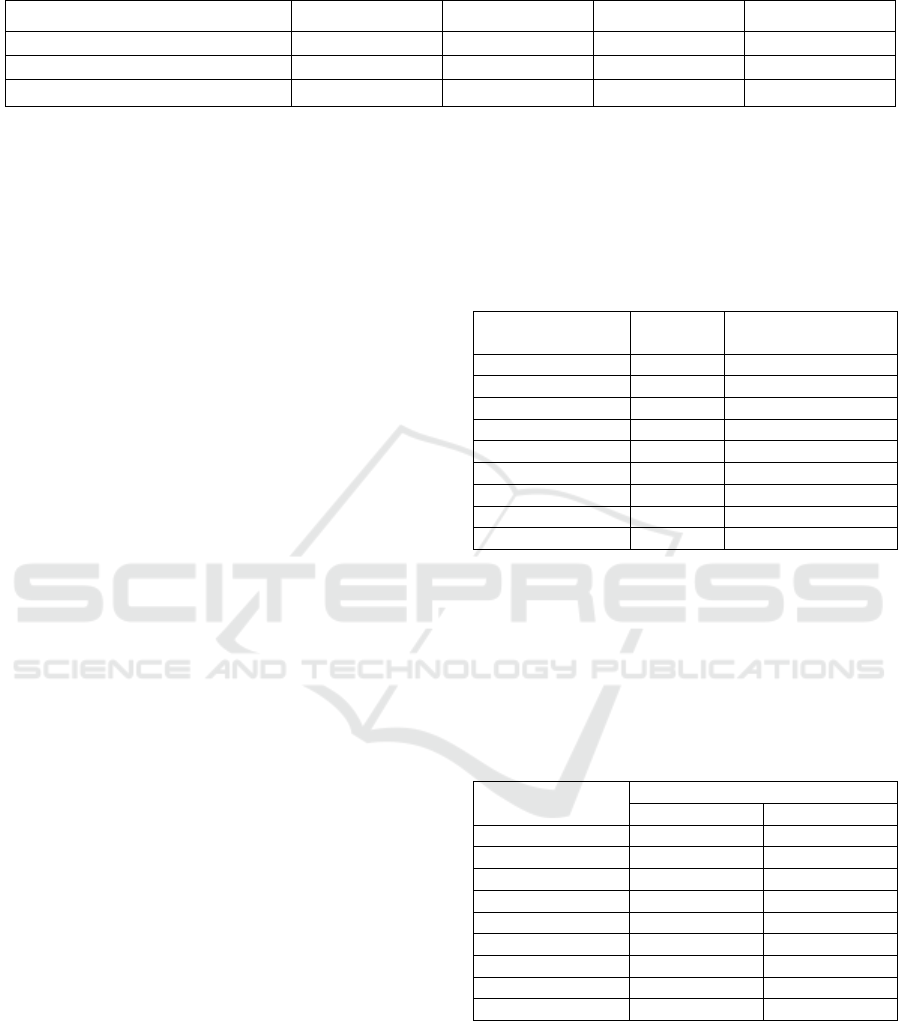
Table 1: Experiment schedule design.
December 2015 March 2016 June2016 August 2016
Hemodynamic monitoring * * * *
The training focus selection * * *
Exercise testing * * *
Immediate post-exercise measurements of HR,
SBP and DBP during 5 minutes of recovery period
were recorded. The current values of all measured
parameters were demonstrated on the metabolic
analyzer screen and saved in the device memory for
ongoing analysis.
VO
2max
and P
max
are the values of maximal
oxygen uptake and attained load the athlete could
reach. It characterizes an athlete’s integral readiness.
In stress-test HR
max
is an indicator of the priority in
the cardiovascular or muscle fitness: if HR
max
is
lower than 180 bpm, then there is cardiovascular
priority. And there is a priority of the muscular
system in “heart-muscle balance” if HR
max
is higher
than 200 bpm. VO
2max
, P
max
and HR
max
allow us to
determine the limiting factors of athlete’s
performance (Seluyanov, 2002). According to
modern concepts in cyclical sports physical
workability can be largely limited by either
cardiorespiratory system or muscular system.
2.3 Statistical Analysis
The statistic software package “SPSS Statistics
17.0” (IBM) was used for statistical analysis. Mean
value (M) and standard deviation (SD) for the used
parameters were calculated, t-test was applied for
comparative analysis. The level of significance was
set at P < 0.05. Pearson and Spearmen correlations
between measured parameters were calculated. Two-
way ANOVA was applied to estimate the impact of
particular hemodynamic indices on aerobic capacity
and athletes’ exercise performance.
3 RESULTS AND DISCUSSIONS
The descriptive analysis of hemodynamic data was
performed to define the weak aspects of athletes’
functional state (Table 2). Thus it was found, that:
i) values of measured parameters varied within a
certain range; ii) mean values of volume parameters
and cardiac indices were lower in reference to
athletic norm.
Based on stated above data from the 1
st
stage of
the proposed study, a group of triathletes was
divided into two groups by the criteria of LV volume
characteristics. It was supposed that the leading
parameter in endurance sport was SV (Zakharova,
2015), as a volumetric indicator, also characterising
LV contractility and heart functional reserve.
Table 2: Hemodynamic parameters at the first stage.
Hemodynamic
indices
Athletic
norm
M±SD
(min-max)
HR at rest, bpm 50-55 62.0±5.95 (51-71)
SV, ml 120-150 113.0±15 (90-131)
SI, ml/m
2
>70 58.8 ±7.96 (50-73)
EDV, ml >190 177±25.1 (144-210)
EDI, ml/m
2
>100 90.67±14.9 (65-115)
EF, % ≥60 63.0±2.04 (60-66)
Volemia, % +21 -20-+21
Inotropy, % > +35 16.36±13.1 (0-+50)
Vascular tone, % < – 30 -15.41±12.6 (0- -43)
The 1
st
group (n=16) was distributed by athletes
with SV < 115 ml, and the 2
nd
group (n=8) – with
SV ≥ 115 ml, respectively. Table 3 demonstrates the
results of comparative analysis of initial
hemodynamic parameters in both groups and
significant differences in selected parameters.
Table 3: Comparative analysis (t-test) of hemodynamic
parameters in groups at the first stage.
Hemodynamic
indices
M±SD
1
st
group 2
n
d
group
HR at rest, bpm 62.33±4.76 61.67±7.4
SV, ml 100.33±9.3 125.5±5.5**
SI, ml/m
2
54.4±4.34 65.67 ±6.3**
EDV, ml 157.3±15.7 197.2±13.7**
EDI, ml/m
2
85.67±7.53 95.67±19.28
EF, % 62.83±1.9 63.17±2.32
Volemia, % 5+16.7 6+10.95
Inotropy, % 6.67±15.01 20±15.81
Vascular tone, % -8.3±8.16 -22±12.77*
*- statistical significance at P < 0.05, ** - P < 0.01.
Before the 1
st
stage testing trainer’s concept of
week training was designed around 2 intensive
workouts per week of 5 or 6 training days. On
Wednesday triathletes usually had repeated short
sprints on track training accompanied with building
whole body and core stability by holistic explosive
Technologies of Effective Training Control in Amateur Triathlon - Non-Invasive Hemodynamic Measurements and Exercise Testing for
Accurate Training Prescription
85

power training. Sunday training was long and took
place principally on highly broken country.
After the primary testing and measurement
analysis several corrections were offered for the first
group training program design. The training process
of the athletes with low heart volume indicators was
supposed to be low intensive (HR=120±10). Sport
walking, cycling, skiing on flat terrain, stationary
bicycle training were recommended for low
intensive endurance training in order to increase
heart volumetric parameters. The objective of the
trainings was to improve dimensional characteristics
of the heart and cardiovascular adaptation to
physical loads. The idea is that while HR is
120±10 bpm the stroke volume tends to its
maximum and provides LV with better diastolic
filling.
Based on the obtained data and defined
weaknesses of participants the training focus
selection was made: the 1
st
group was prescribed
low intensity training. The training strategy of the
2
nd
group was a combination of short intervals at
high-intensity trainings and statodynamic low
intensive strength workouts (Seluyanov, 2002), high
volume trainings were excluded.
The second stage of the study included
hemodynamic measurements, exercise performance
evaluation and amendments to the training strategy
as the results of functional state evaluation
demonstrated no significant changes in major
parameters in both groups. 2.5 months of amateur
athletes efforts were without results.
The conducted further correlative analysis
enabled us to estimate the relations between
hemodynamic parameters and exercise performance.
It was found that VO
2max
correlated with HR
at rest
(r=-
0,48; P < 0.01), SV (r=0.578; P < 0.01), SI (r=0.56;
P < 0.01), EDV (r=0.56; P < 0.01), as well as with
P
max
(r=0.676; p<0.01). Positive correlations
between volume indices and aerobic capacity may
serve as a proof of better cardiovascular adaptation
to exercise loads and effectiveness of heart function
in athletes with the increased LV volume and
contractility.
Impact of P
max
on both the exercise performance
and cardiac functional state indices was estimated by
factor analysis results. It was found that factor P
max
had significant impact on variables VO
2max
(P <
0.001) and EDV (P < 0.001).
Thus, it was found out that specific strength
development and, hereafter muscular endurance
improvement may significantly influence on VO
2max
,
i.e. on performance endurance in amateur triathletes
(Cormie, 2011; Caleb, 2015).
The training guidelines for the next training
period of triathletes (March-May) was rather
different. The second group for maximal power
production enhancement were subjected strength
training for hypertrophy (7-12 reps at 60-80 percent
of 1 RM, three sets per exercise, 2 session per week,
3 weeks). Aerobic middle- and low-volume trainings
with triathlon – specific activities were used to
maintain the technique, improve movement pattern
and keep the aerobic capacity.
In April and May there was high-volume training
for metabolic adaptations, movement efficiency and
nerve system tolerance to enduring work. The power
training component was presented by HIIT overall
strength exercises, mainly with plyometric nature.
Ballistic and TRX training were included for core
stability and psychomotor training as a great
stimulus for improving maximal power in complex
triathlon movements.
For the 1st group athletes low intensive strength
training (Seluyanov, 2002; Shishkina, 2013) aimed
on hypertrophy of slow-twitch muscles was used
instead of intensive strength one. The main idea of
exercises performance is doing them slowly without
leg (arm, back) extension feeling “fire” in muscles
thus organizing specific state for hypertrophy in
slow-twitch motor units.
The aerobic and strength components in April
and May were the same as in the 2nd group but there
was the task to limit HR, not exceeding 180 bmp
during workouts.
In June-August there were more high-intensity
training in both groups. A short-term period of high-
intensity interval training (2 per week) consisting of
repeated exercise bouts performed close to or well
above the maximal oxygen uptake intensity,
interspersed with low-intensity triathlon activities.
Also thanks to participation in triathlon and other
competitions amount of prolonged submaximal
exercise and moderate and long periods of training
“threshold” formed 10-15% of total training volume.
After 3 months of training the final testing
including hemodynamic research and exercise
testing was carried out. Fig.1 and 2 demonstrate the
results of analysis of initial and reached values (4
th
stage – August 2016) of exercise performance. One
can see that athletes from both groups had positive
changes in VO
2max
and power production. Moreover,
participants from the 1
st
group also attained the
values of aerobic capacity with no significant
difference in comparison to the 2
nd
group.
One can see that athletes from both groups had
positive changes in VO
2max
and maximum power.
Moreover, participants from the 1
st
group also
icSPORTS 2016 - 4th International Congress on Sport Sciences Research and Technology Support
86
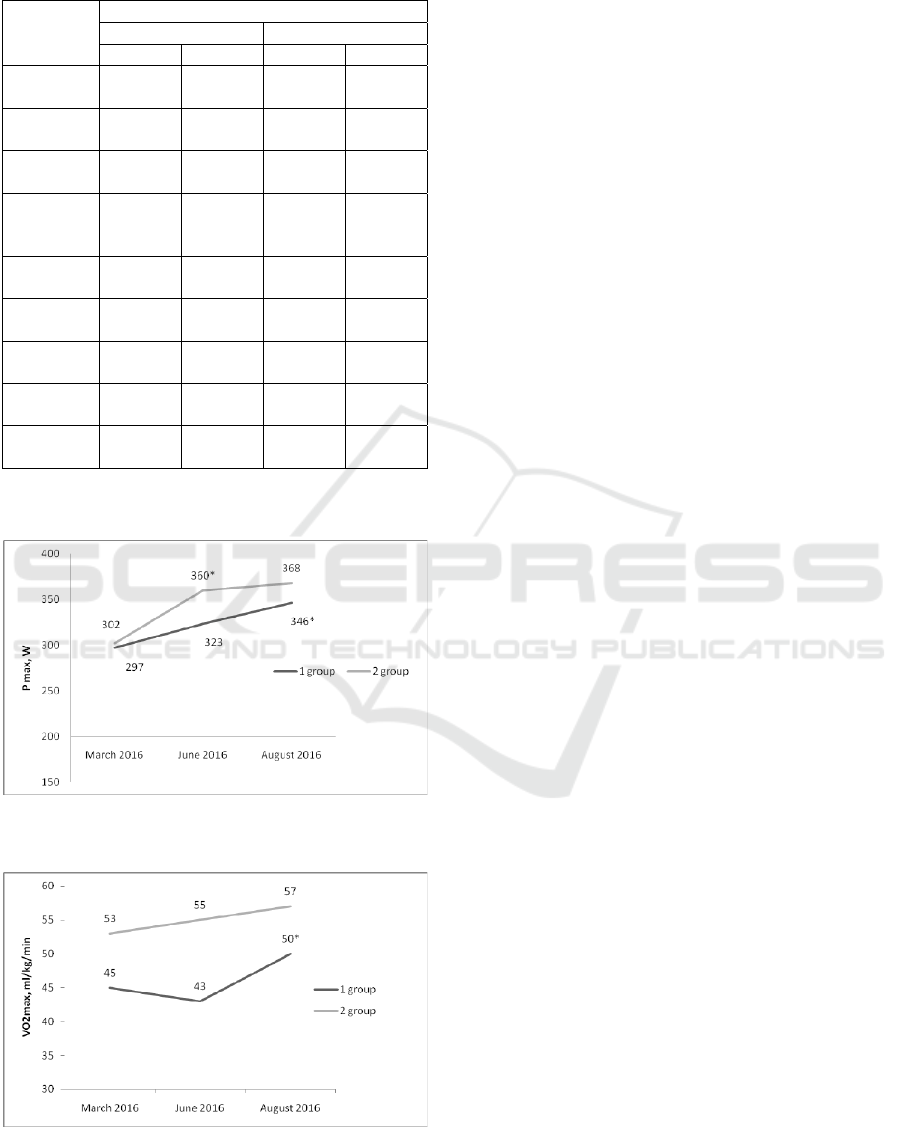
Table 4: Hemodynamic parameters at the first and final
stage.
Parameter M±SD
1
st
group 2
n
d
group
Initial Final Initial Final
HR at rest,
bpm
62.33±
4.76
62.62±
9.74
61.67±
7.4
57.67±
11.55
SV, ml
100.33±9
.3
112.5±
15.61*
125.5±
5.5
121.5±
7.78
SI, ml/m
2
54.4±
4.34
55.88±
7.36
65.67
±6.3
59.67±
6.11
EDV, ml
157.3±
15.7
176.13±
26.97*
197.2±
13.7
187±
25.46
EDI, ml/m
2
85.67±
7.53
88.38±
12.1
95.67±
19.28
92.33±
11.15
EF, %
62.83±
1.9
63.5±
1.41
63.17±
2.32
63.3±
1.5
Volemia,
%
5+16.7 -1.5±
23.5*
6+10.95 3.3±
21.5
Inotropy,
%
6.67±
15.01
3±14.47 20±5.81 21.67±
2.89
Vascular
tone, %
-8.3±
8.16
3±14.47 -22±
12.77
-19±
11.53
* - Significant differences between hemodynamics
parameters at the 1
st
and 4
th
stage P < 0.05.
Figure 1: Maximal attained load (P
max
) during exercise
testing at 3 consecutive stages.
Figure 2: VO
2max
(ml/kg/min) value obtained during
exercise testing at 3 consecutive stages.
attained the values of aerobic capacity with no
significant difference in comparison to the 2
nd
group
(Table 4).
4 CONCLUSIONS
Cardiovascular functional state monitoring enables
to define the main strategy for training prescription.
Combination of hemodynamic and gas-exchange
measurements with simultaneous HR registration
during exercise testing provides with valuable
information for developing a training concept. It is
useful for both correct physical loads dozing and
sufficient cardiac adaptation to increasing exercise
loads, thus it aids amateur athletes to benefit from
sports activity and minimize possible medical risks.
ACKNOWLEDGEMENTS
The work was supported by Act 211 Government of
the Russian Federation, contract № 02.A03.21.0006.
REFERENCES
ACC / AHA 2002 guideline update for exercise testing:
summary article: a report of the American College of
Cardiology / American Heart Association Task Force
on Practice Gudelines. J Am Coll Cardiol; 2006:
48: 1731 pp.
Caleb, D. B., et al., 2015. Strength training for endurance
athletes: theory and practice in Strength and
Conditioning J: 37(2): www.nsca-scj.com.
Cormie, P., McGuigan, M. R. and Newton, R. U., 2011.
Developing neuromuscular power: Part 1 – Biological
basis of maximal power production (review), In J
Sport Med: 41(1): 17-38.
Cormie, P., McGuigan, M. R. and Newton, R. U., 2011.
Developing neuromuscular power: Part 2 – Training
considerations for improving maximal power
production In J Sport Med: 41(2): 125-146.
Corrado, D., 2005. Cardiovascular preparticipation
screening of young competitive athletes for prevention
of sudden cardiac death: proposal for a common
European protocol. Consensus Statement of the Study
Group of Sport Cardiology of the Working group of
Myocardial and Pericardial Diseases of the European
Society of Cardiology. In Eur. Heart J; 26: 516–524.
O’Tool, ML, 1995. Applied physiology of triathlon. In
Sports Med: 19(4): 251-67.
Seluyanov, V., 2002. Intuition is blind without knowledge,
In Skiing Sport: 23: 62-67.
Shishkina, A., Tarbeeva, N., Alimpieva, O., Berdnikova,
A., Tarbeeva, A., Miasnikova, T., 2014. Hemodyna-
Technologies of Effective Training Control in Amateur Triathlon - Non-Invasive Hemodynamic Measurements and Exercise Testing for
Accurate Training Prescription
87

mics Monitoring in Sport- Using Hemodinamics
Monitor for Sport Training Planing. icSPORTS 2014:
In Proceedings of the 2nd International Congress on
Sports Sciences Research and Technology Support,
Rome, Italy: 103-110.
Shishkina, A., Tarbeeva, N., 2013. Cross-country skiing:
specific strength training for endurance success. In
18th Annual Congress of the European College of
Sport Science Book of Abstracts; Barcelona, Spain.
610.
Vilikus, Z., 2012. Functional Diagnostics. Col Phy Edu
and Sport Palestra.
Zakharova, A., Tarbeeva, N., Tarbeeva, A., Miasnikova,
T., 2015. Healthsaving technologies for young cross
country skiers. Cardiovascular system testing for sport
training program design. In icSPORTS 2015:
Proceedings of the 3rd International Congress on
Sports Sciences Research and Technology Support;
2015: 139-144.
icSPORTS 2016 - 4th International Congress on Sport Sciences Research and Technology Support
88
