
Reactive Control System to Manage Strain Situations in Emergency
Departments
Farid Kadri
1
, Sondès Chaabane
2
and Christian Tahon
2
1
PIMM Laboratory, UMR CNRS 800, Arts et Métiers Paris-Tech, Paris, France
2
LAMIH UMRCNRS8201, UVHC, Le Mont Houy, F-59313 Valenciennes, France
Keywords: Emergency Department, Strain Situations, Reactive and Proactive Control, Strain Indicators, Decision
Making.
Abstract: Current dysfunctions observed in emergency departments (EDs) are mainly due to the unsuitable organization,
constraints and changes in their missions, as well as the mismanagement of process flows (patients,
information’s, resources, etc.). This often results in strain situations. ED managers must master these
problems, as well as the internal restructuring reflected by resource pooling, including technical platforms.
To make these decisions, they need an adapted decision support system to anticipate and manage such
situations. This paper focuses on the development of decision-making model for reactive control of strain
situations in EDs. The target is to help ED managers in the choice and the implementation of appropriate
corrective actions to manage each potential occurrence of these situations. A case study is used to evaluate
the reactive management of strain situations in the paediatric emergency department (PED) at Lille regional
hospital centre, France.
1 INTRODUCTION
Emergency departments (EDs) are an important
component of healthcare systems because they
provide immediate and essential medical care for
patients. Thus, these establishments are faced with
increasingly difficulties to carry out their missions.
With the growing demand for emergency medical
cares and the reducing of number of EDs
(Kellermann, 2006), the management of EDs has
become more and more important, but they are also
the most overcrowded component (Boyle et al., 2012;
Kadri et al., 2014a).
Facing at a large number of patient visits but
limited work force, the ED must provide 24-hours
emergency services and must offer a good quality
service (minimizing patients’ waiting times whilst not
compromising the required attention for each patient).
It ensures that valuable resources (e.g., doctors’
utilization and nurses’ time; and treatment
equipment) will be well utilized.
This work is to present a decision-making system
for the reactive management of strain situations in an
ED. The objective is to help ED managers in the
choice and the implementation of appropriate
corrective actions for each potential occurrence of
these situations. This paper is organized in five
sections. Section 2 presents and characterizes a strain
situation and strain indicators. Section 3 presents the
model for reactive control and management of strain
situations in an ED. Section 4 shows obtained results
of case study. The last section provides concluding
comments and future works.
2 EMERGENCY DEPARTMENT
The current dysfunctions observed in EDs are mainly
due to many causes. First concerns the changes in
their missions and the mismanagement of various
process flows. Second, the presence of interference
between planned and unplanned activities, especially
activities unforeseen emergency. Finally, the EDs
must cope with several constraints, in particular,
organizational constraints related to problems of
internal organization, upstream and downstream of
EDs to receive and manage the patient flows.
These problems cause the appearance of strain
situations within the ED that affect patients, medical
staff, and service quality. To handle these problems,
ED managers must anticipate these strain situations
576
Kadri, F., Chaabane, S. and Tahon, C.
Reactive Control System to Manage Strain Situations in Emergency Departments.
DOI: 10.5220/0005988105760583
In Proceedings of the 13th International Conference on Informatics in Control, Automation and Robotics (ICINCO 2016) - Volume 2, pages 576-583
ISBN: 978-989-758-198-4
Copyright
c
2016 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

by forecasting changing in ED demands (patient
flows) and ED behavior, and, if necessary, to react
quickly to the occurrence of these situations. Hence,
EDs must incorporate in their operating mode the
capacity to anticipate, to react and to mobilize
resources for satisfying patients and avoiding strain
situations.
2.1 Definition of Strain Situation in an
ED
Most studies including emergency services have been
addressing several targets:
Improve the quality and performance of care in
emergency departments.
Reduce the waiting time and the residence time of
emergency patient.
Manage the hospital activities and the resources in
emergency services.
The various works presented above are intended
to improve the functioning of an ED. However, gaps
can be seen on the definition and modeling of
situations arising from the aforementioned issues.
The avoidance strategies and management of these
situations are lacking.
According to the literature review presented in
(Kadri, 2014b and 2015), no studies have been
devoted to define, characterize and model strain
situations in hospitals. To remedy this lack,
interviews were conducted with professionals in the
emergency department at the Lille regional hospital.
From a “patient flow” viewpoint, a strain situation in
an ED is defined as a disequilibrium between the care
load flow (demand), and the care production capacity
(supply) over a certain time. In this case, defined
indicators must be controlled to not exceed a
threshold value. The harmful consequences (strain
phenomenon) to the proper functioning of the ED will
be observed, measured and corrected.
The main identified factors that may affect this
equilibrium are (Kadri et al., 2014b):
Inputs (patient flow): seasonal epidemics (in
winter: influenza, colds, gastroenteritis,
bronchiolitis, etc.; in summer: trauma), health
crises, cumulative causes such as the aging
population…
Care production capacity: care system
performance, number and competence of medical
staff (capacity, experience feedback, the
availability of physicians downstream), internal
and external transfer capacities (availability of
care services downstream)…
Based on the proposed definition of strain situations
presented above, the ED behavior evolve into two
situations: normal and strain. It characterized by three
states (figure 1) (V
E
is the estimated value of the
measured parameter that characterizes the ED’s
state):
Normal State: the care production capacity is
greater than the care load flow.
Degraded state: The care production capacity
is lower than the care load flow. In this case, the ED
goes from normal to acceptable degraded state of the
strain situation. This state is defined as the threshold
V
Mo
(V
E
≥ V
Mo
) being exceeded. So specific
management must be deployed based on corrective
actions to enable the ED to return to normal state.
Critical state: this state represents the
unacceptable degradation of the strain situation. This
state is defined as the threshold V
Cr
(V
E
≥ V
Cr
) being
exceeded. In this case, ED must deploy corrective
actions in order to attempt to return to acceptable
degraded state or normal state.
2.2 Strain Indicators
According to Luan, (2002), an indicator is defined as
a selected piece of information, associated with a
criterion, aimed at observing the evolution of a
system at well-defined intervals.
A strain indicator in an emergency department
can be characterized by four elements (SI = [C, O,
SV, AV]) as follows:
Context (C): the search of corrective actions
during the occurrence of a strain situation is
strongly guided by the context in which the strain
situation occurs. Three elements can be defined:
events (epidemic, accident…), situation
(degraded or critical) and time (the hour, or
period, or day…);
Objective (O): each strain indicator must have a
clearly defined objective to allow the evaluation
of an event or situation by the ED manager;
State variables (S
V
): the state variables must be
measurable and easy to interpret in order to define
and characterize the different states of the ED;
Action variables (A
V
): the strain indicator is only
useful if one (or several) corrective action(s) are
associated with the exceeding of the predefined
thresholds for each state variable.
Identifying the dynamic state of the ED and
evaluating the threshold values imperatively require
relevant indicators. One can find many types of strain
indicators in the literature: waiting times, current
number of patients present in the ED, length of stay
in the ED (Kadri et al., 2015, 2014b). 33 indicators
has been enumerated. However, the characteristics of
these indicators are not all accessible or usable. They
Reactive Control System to Manage Strain Situations in Emergency Departments
577
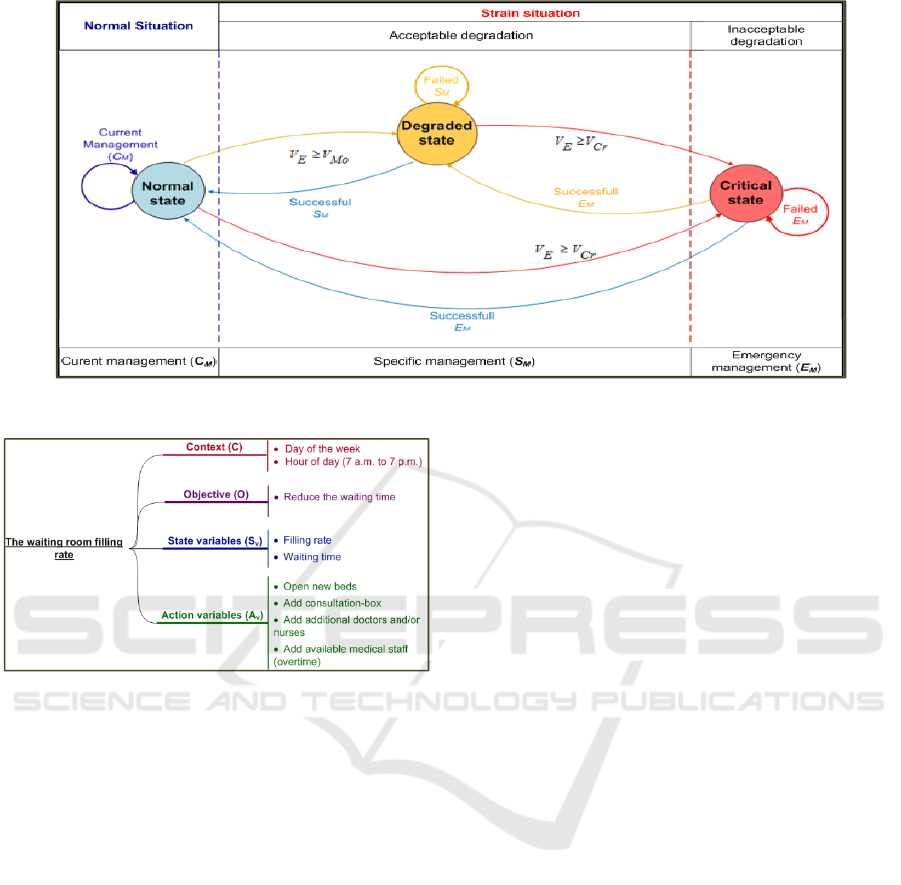
Figure 1: States and transition between states of the ED.
Figure 2: Example of strain indicator: the filling rate in the
waiting room.
must be imperatively established and validated by the
EDS professionals. Their effectiveness to identify,
quantify and represent strain situations in an ED in
different contexts must be proved.
A strain indicator (SI) can be a number, measured
directly in the emergency department (e.g.: number of
hospitalization for more than 24 hours) or calculated
from measurements performed in the emergency
department (e.g.; the average length of stay the
urgency in the last 24 hours).
3 REACTIVE MANAGEMENT OF
STRAIN SITUATIONS IN EDS
In order to react quickly to the occurrence of strain
situation at an ED, the proposed system must help ED
manager and take into account the clinical
requirements and manager’s responsibilities. Several
corrective actions must be applied in order to give
many alternatives to the ED manager.
3.1 Reactive Mode
In this case, the ED manager has also to react if a
situation occurs, which must then be processed in a
reactive context (reactive control). Reactive control
occurs in real-time, according to the occurrence of
unanticipated events and/or disturbances. This
control is thus made while the ED is functioning, and
without anticipation. It concerns the very short term
(minute, hour). It is needed when: i) an unforeseeable
and unexpected event occurs, and ii) deviations that
lead to degraded or critical state of the ED are
detected.
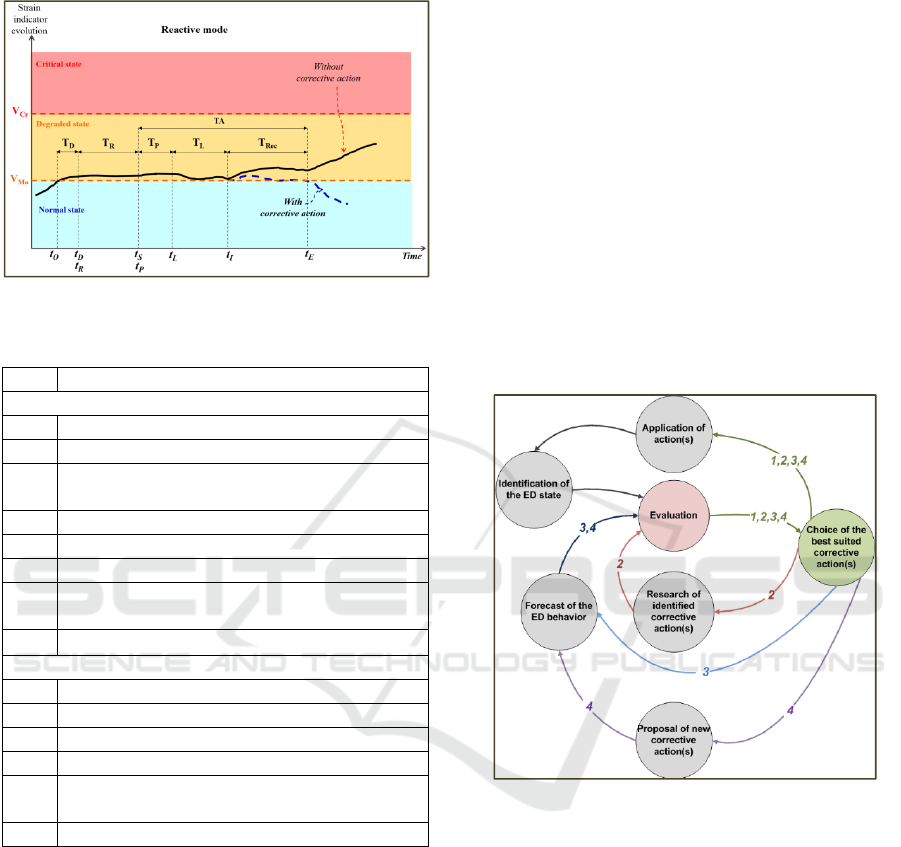
Figure 3 illustrates the case of reactive mode. In
this case, we should ideally be able to set up
corrective action as soon as it is selected (t
S
= t
P
).
Unfortunately, however, the disturbance is not
detected immediately, but after T
D
time (T
D
= t
D
- t
O
).
The search for a corrective action then begins at t
R
=
t
D
. A T
R
time is then required to search corrective
actions (T
R
= t
S
-t
R
). When the action is selected at t
S
and prepared at t
P
, T
P
time is required to set up
selected action. The action is launched during T
L
time.
Finally the ED needs T
Rec
time until to recover its
normal state.
To make such decisions, the Ed’s manager must
follow steps listed above:
Identify the ED state
Research corrective actions in both the short time
and real-time, if a strain situation occurs
Assess the impact of this corrective action on the
behavior of the ED,
Launch the corrective actions if he estimates that
these corrective actions are satisfactory, or search
ICINCO 2016 - 13th International Conference on Informatics in Control, Automation and Robotics
578
for an alternative.
Figure 3: Reactive mode (caption table 1).
Table 1: caption of figure 3.
SI
i
(t)
Strain indicator i value at date t.
Dates
t
O
Date the disturbance occurs
t
D
Date the disturbance is detected
t
R
Date of starting the research of corrective
action
t
S
Date the corrective action is selected
t
P
Date the corrective action is prepared
t
L
Date the corrective action is launched
t
I
Date the corrective action takes effect within
the ED
t
E
Date the ED returns to normal state
Times
T
D
Time required to detect disturbances
T
R
Time required to search corrective actions
T
P
Time required to set up corrective action
T
L
Time required to launch the corrective action
T
Rec
Time required for the ED to recover its
normal state after the disturbance
T
A
Time required to activate corrective action
3.2 Decision Making Process
Four several types of decisions (figure 4) according
different situations are identified as below:
Direct decision (1): the ED manager identify a
known efficient, corrective action that responds
effectively to the detected situation. In this case,
he makes decisions directly and chooses the
appropriate corrective action(s).
Researching corrective actions (2): the ED
manager seeks to identify a previously executed
action stored in knowledge data base and used in
a similar strain situation. In this case, he can apply
the identified actions that are considered effective,
after evaluation.
Evaluation and validation of an identified
corrective action (3): ED manager identifies
potential corrective actions from knowledge base.
To verify and validate if the identified actions are
relevant in the current context, the manager uses,
in this case, the simulation model.
Searching for new corrective actions (4): if the
knowledge base does not contain any corrective
actions corresponding to the actual strain
situation, manager may propose a new corrective
action. He simulates and evaluates the corrective
actions’ effectiveness by using simulation model.
If the proposed corrective action(s) are effective,
he applies them directly; if not, he proposes other
actions and simulates their effects on the ED
behavior, and so on. These new validated actions
are then stored in the knowledge base.
Figure 4: Generic decision-making model.
4 CASE STUDY: PED OF LILLE
Lille Regional Hospital Centre (CHRU) serves four
million inhabitants in Nord-Pas-de-Calais, a region
characterized by one of the largest population
densities in France (7% of the French population).
The Paediatric Emergency Department (PED) in Lille
regional hospital centre (CHRU) is open 24 hours a
day and receives 23 900 patients a year on average.
Based on the analysis of the questionnaires and
interviews conducted with the PED medical staff, we
established a dynamic model of the care process.
Each stage is characterized by its activity duration,
nature and type of care staff(s) required and the
different waiting times are shown figure 5.
Reactive Control System to Manage Strain Situations in Emergency Departments
579
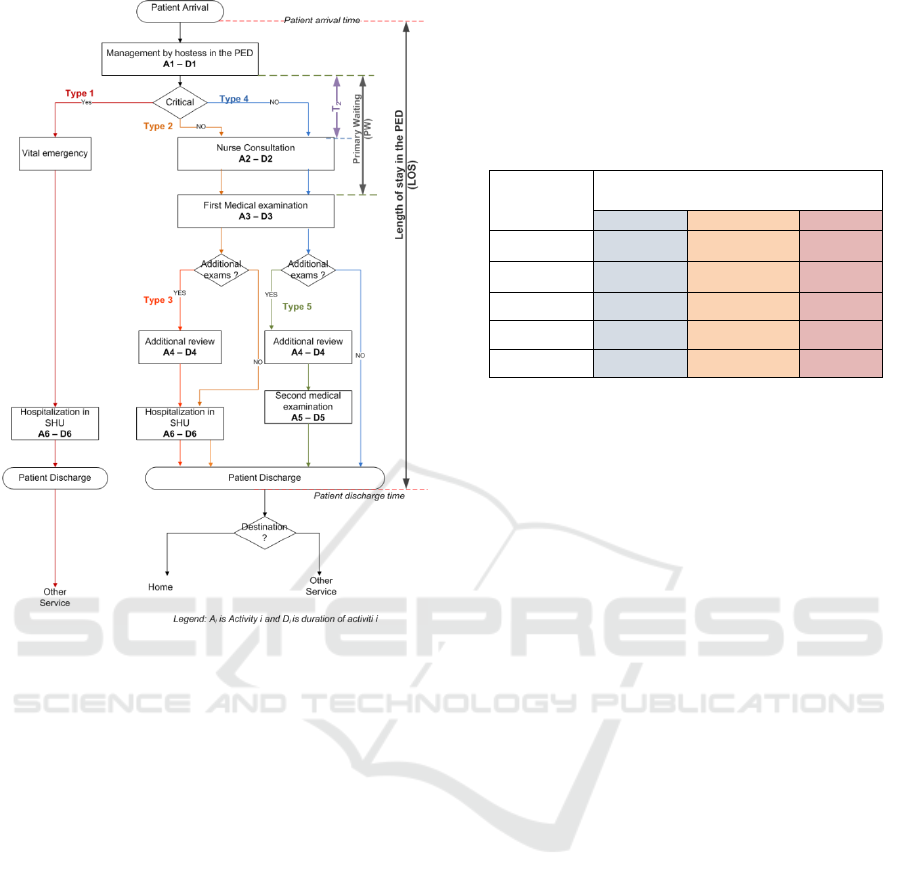
Figure 5: The main activity durations in the care process at
the PED.
4.1 Strain Indicators
The PED staff was involved (by means of
questionnaires and interviews) in the selection and
classification of the relevant strain indicators. The
main strain indicators selected and validated with the
PED medical staff are:
1) Primary waiting time (PW): waiting-period
between the care by the hostess, and the beginning
of first medical examination.
2) T
2
: waiting time between the end of the
management by hostess and the beginning of
nurse consultation.
3) N
p
: the current number of patients present in the
PED at the arrival of a new patient.
4) PP: ratio of the number of patients present in the
PED by the number of physicians.
5) (Q
S
%): the ratio of the actual length of stay
(LOS(t)) by the theoretical length of stay (LOS
th
)
for the non-urgent patients.
The strain indicators and their threshold values
use in this study are tabulated in table 2. The
threshold values were defined and validated by
the pediatric medical staff.
Table 2: Characteristics of the strain indicators used in the
case study.
Strain
indicators
PED states
Normal Degraded Critical
PW(minutes) PW < 60 60 ≤ PW < 90 PW ≥ 90
T
2
(minutes) T
2
< 25 25 ≤ T
2
< 50 T
2
≥ 50
N
P
(number) N
P
< 12 12 ≤ N
P
< 20 N
P
≥ 20
PP (%) PP
< 4 4 ≤ PP < 7 PP ≥ 7
Q
S
(%) Q
S
> 0.8 0.8 ≤Q
S
≤1.5 Q
S
< 1.5
4.2 Corrective Actions
The corrective actions have been defined with the
PED staff according 3 classes:
a) Actions on Human Resources: add a nurse
and/or doctor during a given period (in our case:
two hours).
b) Actions on Material Resources: transform one
room in the Short-term Hospitalization Unit
(SHU) to a consultation box.
c) Actions on the Patient Flow Admitted to the
PED: four rules of priority have been chosen to
manage the patient flow in the waiting room:
1) Rule 0: The classic rule FIFO (First In, First
Out).
2) Rule 1: in ascending order of the type of
patient. The most urgent patient-cases are
given a higher priority.
3) Rule 2: in descending order of time already
spent in the PED. Patients with the highest
residence time are given a higher priority.
4) Rule 3: in ascending order of their
advancement in the care process. Patients
early in their care processes are given a higher
priority.
Three alternatives were defined according to the
launch-time of the corrective action(s) (T
L
). Table 3
summarizes the different characteristics of these
corrective actions. 31 scenarios were defined and
assessed for each alternative A, B, and C (for a total
of 93 scenarios). The results of the different scenarios
were compared and analyzed. In the next sub-section
we present the principal results.
ICINCO 2016 - 13th International Conference on Informatics in Control, Automation and Robotics
580
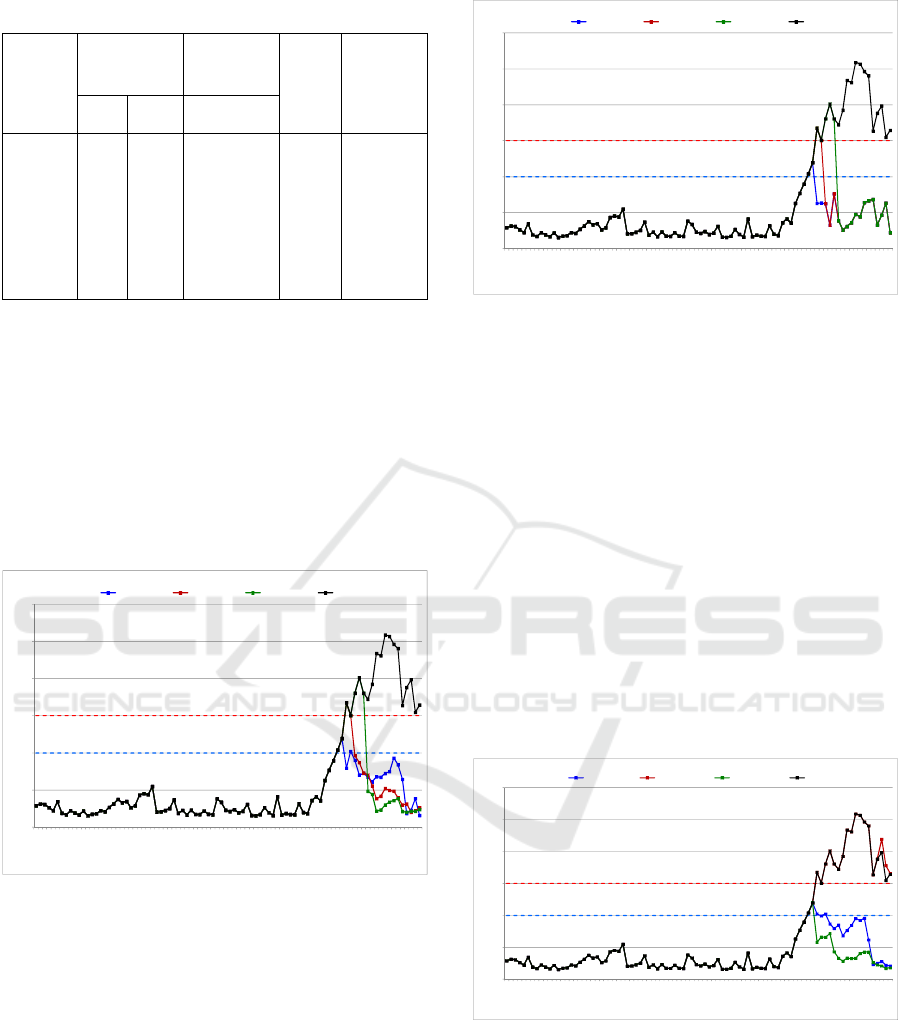
Table 3: Characteristics of the corrective actions.
Scenarios
Action on
human
resources
Action on
material
resources
Rules of
priority
Launch-
time T
L
Nurse Doctor
Consultation
box
Scenario i 0 or 1 0 or 1 0 or 1
Rule 0
or
Rule 1
or
Rule 2
or
Rule 3
T
L
= 0 min
(Alternative
A)
T
L
= 60 min
(Alternative
B)
T
L
= 90 min
(Alternative
C)
4.3 Results
As an illustration, the results of some simulations are
given below for the strain indicator PW. A0 is defined
as the initial scenario without corrective actions.
a) Actions on Human Resources : Impact of
Adding a Doctor
Figure 6 presents the results of adding one doctor in
different scenarios: A2 (TL=0 min), B2 (TL=60min)
and C2 (TL=90min).
Figure 6: Impact of adding a doctor.
As observed in figure 6, in all cases, adding a doctor
reduces the primary waiting-time (PW) of patients in
the PED. It can be concluded that the addition of a
doctor is always interesting, regardless of the launch-
time (T
L
).
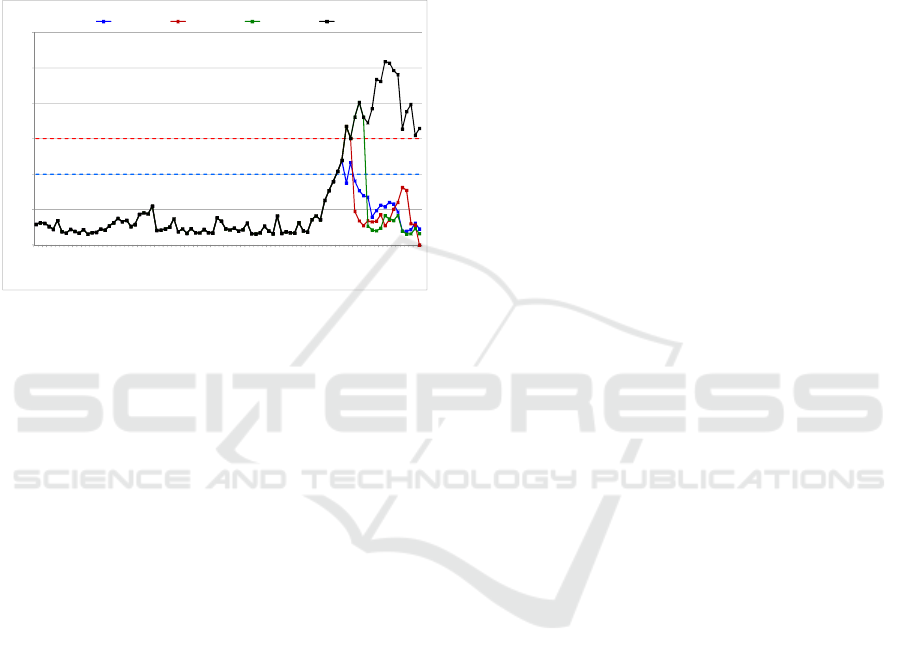
b) Actions on Material Resources: Impact of
Adding a Consultation Box
Figure 7 presents the results of transforming one
room in the SHU into a consultation box in different
scenarios: A3 (TL=0 min), B3 (TL=60min) and C3
(TL=90min).
Figure 7: Impact of adding a consultation box.
The addition of a consultation box, by transforming
one of the SHU rooms, reduces the PW. The
immediate launch of this action (TL = 0) gives the
best results and ensures that the PW does not reach a
critical state (PW = 90 minutes). The addition of a
consultation box is an action already used in the PED,
and it is still an interesting solution.
c) Actions on the Patient Flow Admitted to the
PED: Impact of the Application of a Priority
Rule
We want to observe the behavior of the PED when
applying different priority rules. The idea here is to
see the impact of flow management techniques with
same resources on the ED performance to cope with
strain situations. In this case we used the scenarios of
the alternative A (TL = 0) as follows: A8 (Rule 1),
A16 (Rule 2) and A24 (Rule 3).
Figure 8: Impact of the application of a priority rule.
We observed that there is a significant impact in the
choice of the priority rule, on the PW values. This
leads us to conclude that avoiding these tense
situations can be achieved not only through increased
resources, but also by reflecting on the impact of the
PED’s internal organization. In some cases, applying
simple priority rules should help better manage tense
0
30
60
90
120
150
180
00:21:48
00:58:21
01:16:10
01:43:03
02:41:31
05:47:13
07:06:28
09:30:48
09:52:36
10:21:24
10:27:03
11:00:47
11:18:11
11:24:02
11:51:47
12:20:52
12:37:21
13:22:48
13:37:08
13:57:46
14:33:21
14:54:34
14:56:02
15:14:14
15:41:19
16:02:13
16:11:28
16:33:07
17:05:35
17:48:41
18:19:05
18:46:43
19:02:29
19:24:48
20:00:44
20:26:33
21:09:40
21:53:23
22:12:48
22:48:11
23:15:46
23:46:18
00:12:00
00:40:42
01:11:51
Primary wainting, PW(minutes)
Time (24-h period)
Normal Dégradé PW_Scenario A2 PW_Scenario B2 PW_Scenario C2 PW_Scenario A0
Critical state
Degraded state
Normal state
0
30
60
90
120
150
180
00:21:48
00:58:21
01:16:10
01:43:03
02:41:31
05:47:13
07:06:28
09:30:48
09:52:36
10:21:24
10:27:03
11:00:47
11:18:11
11:24:02
11:51:47
12:20:52
12:37:21
13:22:48
13:37:08
13:57:46
14:33:21
14:54:34
14:56:02
15:14:14
15:41:19
16:02:13
16:11:28
16:33:07
17:05:35
17:48:41
18:19:05
18:46:43
19:02:29
19:24:48
20:00:44
20:26:33
21:09:40
21:53:23
22:12:48
22:48:11
23:15:46
23:46:18
00:12:00
00:40:42
01:11:51
Primary waiting, PW(minutes)
Time (24-h period)
Normal Dégradé PW_Scenario A3 PW_Scenario B3 PW_Scenario C3 PW_Scenario A0
Critical state
Degraded state
Normal state
0
30
60
90
120
150
180
00:21:48
00:58:21
01:16:10
01:43:03
02:41:31
05:47:13
07:06:28
09:30:48
09:52:36
10:21:24
10:27:03
11:00:47
11:18:11
11:24:02
11:51:47
12:20:52
12:37:21
13:22:48
13:37:08
13:57:46
14:33:21
14:54:34
14:56:02
15:14:14
15:41:19
16:02:13
16:11:28
16:33:07
17:05:35
17:48:41
18:19:05
18:46:43
19:02:29
19:24:48
20:00:44
20:26:33
21:09:40
21:53:23
22:12:48
22:48:11
23:15:46
23:46:18
00:12:00
00:40:42
01:11:51
Primary wainting, PW (minutes)
Time (24-h period)
Normal Dégradé PW_Scenario A8 PW_Scenario A16 PW_Scenario A24 PW_Scenario A0
Critical state
Degraded state
Normal state
Reactive Control System to Manage Strain Situations in Emergency Departments
581
situations. We noted that Rule 1 and Rule 3 have a
positive impact on PW values. Rule 2 was not a
successful experiment. Therefore, the patient’s length
of stay is not considered as a priority parameter.
d) Combination of the Corrective Actions
Figure 9 presents the results of the scenarios where 1
nurse, 1 doctor and 1 extra box are added and Rule 3
is applied: A31 (TL=0 min), B31 (TL=60min) and
C31 (TL=90min)
Figure 9: Impact of the combination of corrective actions.
As expected, the combination of corrective actions
(human and material resources), and priority rules,
reduced the PW.
From the results presented above, we observed
the impact of various corrective actions on the
behavior of the PED. The launch-time of corrective
actions plays a key role in some cases. The series of
experiments conducted on the priority rules applied to
patients flow showed their interest. They are therefore
to be considered to increase the availability of
resources to the PED manager.
5 CONCLUSIONS
The objective of this work is to improve the
management of strain situations that may occur in an
emergency department (ED). To achieve this goal, we
defined the ED transition states, the strain situations,
the strain indicators and the associated corrective
actions in the case of the Paediatric Emergency
Department (PED) in Lille regional hospital centre
(CHRU), France. To manage these strain situations
we proposed an operating process for reactive control
of these perturbations. The preliminary results show
the interest to have such system. It should also be
noted that if we tested a large number of scenarios, it
will also be necessary to analyze those which can
really be implemented in reality, taking into account
the organization of human resources, as well as the
regulation and economic aspects.
The perspective of the work in the immediate
future consists in the specification and design of a
decision support system (DSS) for the proactive and
reactive control of ED activities. The main function
of this DSS have i) to improve the reception of
emergency patients, and facilitate the work of staff,
ii) avoid the occurrence of strain situations, and also
limit their impact if they do occur, and iii) help to
better adapt an organization in terms of human and
material resources. The second issue must concern
the application of this DSS in other EDs and study the
impact of organizational culture on its application.
The future works must be conducted with
researchers in ergonomics and psychology to cope
with exogenous factors such as: discomfort, fatigue
and psychological stress faced by nurses and
physicians …. In strain situations.
REFERENCES
Aboueljinane, L., Sahin, E., Jemai, Z., Marty, J., 2014. A
simulation study to improve the performance of an
emergency medical service: Application to the French
Val-de-Marne department. Simul. Model. Pract. Theory
47, 46–59.
Al-Refaie, A., Fouad, R. H., Li, M.-H., Shurrab, M., 2014.
Applying simulation and DEA to improve performance
of emergency department in a Jordanian hospital.
Simul. Model. Pract. Theory 41, 59–72.
Beaulieu, H., Ferland, J. A., Gendron, B., Michelon, P.,
2000. A mathematical programming approach for
scheduling physicians in the emergency room. Health
Care Manag. Sci. 3, 193–200.
Boyle, A., Beniuk, K., Higginson, I., Atkinson, P., 2012.
Emergency Department Crowding: Time for
Interventions and Policy Evaluations. Emerg. Med. Int.
2012, 1–8.
Doyle, S. L., Kingsnorth, J., Guzzetta, C. E., Jahnke, S. A.,
McKenna, J. C., Brown, K., 2012. Outcomes of
implementing rapid triage in the pediatric emergency
department. J. Emerg. Nurs. 38, 30–35.
Gonzalez, C. J., Gonzalez, M., Ríos, N.M., 1997.
Improving the quality of service in an emergency room
using simulation-animation and total quality
management. Comput Ind Eng 33, 97–100.
Kadri, F., Chaabane, S., Bekrar, A., Tahon, C., 2015.
Resilience-Based Performance Assessment of Strain
Situations in Emergency Departments. Presented at the
Industrial Engineering and Systems Management
(IESM), 2015 International Conference on, Seville, pp.
609–618.
Kadri, F., Chaabane, S., Harrou, F., Tahon, C., 2014a. Time
series modelling and forecasting of emergency
department overcrowding. J. Med. Syst. 38:107, 1–20.
0
30
60
90
120
150
180
00:21:48
00:58:21
01:16:10
01:43:03
02:41:31
05:47:13
07:06:28
09:30:48
09:52:36
10:21:24
10:27:03
11:00:47
11:18:11
11:24:02
11:51:47
12:20:52
12:37:21
13:22:48
13:37:08
13:57:46
14:33:21
14:54:34
14:56:02
15:14:14
15:41:19
16:02:13
16:11:28
16:33:07
17:05:35
17:48:41
18:19:05
18:46:43
19:02:29
19:24:48
20:00:44
20:26:33
21:09:40
21:53:23
22:12:48
22:48:11
23:15:46
23:46:18
00:12:00
00:40:42
01:11:51
Primary waiting, PW(minutes)
Time (24-h period)
Normal Dégradé PW_Scenario A31 PW_Scenario B31 PW_Scenario C31 PW_Scenario A0
Critical state
Degraded state
Normal state
ICINCO 2016 - 13th International Conference on Informatics in Control, Automation and Robotics
582

Kadri, F., Chaabane, S., Tahon, C., 2014b. A simulation-
based decision support system to prevent and predict
strain situations in emergency department systems.
Simul. Model. Pract. Theory 42, 32–52.
Kadri, F., Pach, C., Chaabane, S., Berger, T., Trentesaux,
D., Tahon, C., Sallez, Y., 2013. Modelling and
management of the strain situations in hospital systems
using un ORCA approach, IEEE IESM, 28-30 October.
RABAT - MOROCCO, p. 10.
Kellermann, A.L., 2006. Crisis in the Emergency
Department. N. Engl. J. Med. 355, 1300–1303.
Litvak, N., van Rijsbergen, M., Boucherie, R.J., van
Houdenhoven, M., 2008. Managing the overflow of
intensive care patients. Eur. J. Oper. Res. 185, 998–
1010.
Luan, J., 2002. Contrôle de la qualité-MSP, analyse des
performances et contrôle de réception., Technique et
Ingénierie, Dunod/L’Usine Nouvelle. Dunod.
Oddoye, J.P., Jones, D. F., Tamiz, M., Schmidt, P., 2009.
Combining simulation and goal programming for
healthcare planning in a medical assessment unit. Eur.
J. Oper. Res. 193, 250–261.
Yeh, J.-Y., Lin, W.-S., 2007. Using simulation technique
and genetic algorithm to improve the quality care of a
hospital emergency department. Expert Syst. Appl. 32,
1073–1083.
Zeng, Z., Ma, X., Hu, Y., Li, J., Bryant, D., 2012. A
simulation study to improve quality of care in the
emergency department of a community hospital. J.
Emerg. Nurs. JEN Off. Publ. Emerg. Dep. Nurses
Assoc. 38, 322–328.
Reactive Control System to Manage Strain Situations in Emergency Departments
583
