
Accurate Level-crossing ADC Design for Biomedical Acquisition
Board
Mariam Tlili
1,2
, Manel Ben-Romdhane
1
, Asma Maalej
1
, Mohamed Chaker Bali
1
, François Rivet
2
,
Dominique Dallet
2
and Chiheb Rebai
1
1
GRESCOM Research Lab., SUP’COM, University of Carthage, Cité Technologique des Communications,
2083 El Ghazala, Ariana, Tunisia
2
IMS Research Lab., University of Bordeaux, Bordeaux INP ENSEIRB-MATMECA, 351 Cours de la Libération,
Bâtiment A31, 33405 Talence Cedex, France
Keywords: Biomedical Sensor, Level-crossing Analog-to-Digital Converter, ECG.
Abstract: The aim of this paper is to present a wireless biomedical system for the acquisition and transmission
(Wibio’ACT) of biomedical signals. This work is a part of the Wibio’ACT project which main purpose is to
ensure the minimum power consumption while diagnose patients continuously and in real time. For the
Wibio’ACT system, the bottleneck is the analog-to-digital conversion (ADC) since it controls the power
consumption of the digital signal processing step as well as the amount of the transmitted data. In fact, in
this work case, the ADC continuously measures the electrical activity of the heart to deliver the
electrocardiogram (ECG) signal. Hence, among conventional ADCs, level-crossing analog-to-digital
converters (LC-ADCs) have been investigated for ECG signals processing. Authors propose some design
consideration of the LC-ADC. This reduces the LC-ADC output samples by 13 % to help to save the power
consumption of the wireless data transmitter. The samples with a small variation are reduced by at least
44%. The performance of the proposed design is measured in terms of percentage root mean square
difference (PRD) applied to the reconstructed signal quality. A PRD of 1% is verified using behavioral
simulations on ECG records extracted from different databases. A timer period T
C
of 0.14 ms ensures an
effective number of bits of 10 bits and a signal to noise ratio of 62 dB.
1 INTRODUCTION
In biomedical engineering field, as the
cardiovascular diseases are at the top of death
causes, many researches focus on the development
of reliable and cost effective system for monitoring
cardiac patients (Mendis, 2011; Gyselinckx, 2006).
One part of these research activities concerns the
acquisition, the processing or the wireless
transmission of the electrical activity of the heart or
any other vital data. Due to the continuous-time
monitoring of the patients, large amounts of data
need to be processed, stored and transmitted. The
key requirements for an efficient high-quality signal
monitoring system are power consumption saving,
data rate enhancement and distortion robustness.
Therefore, in order to reduce the amount of data
after acquisition and before transmission over the
radio channels, electrocardiogram (ECG) signal
compression requires a lot of attention. Many
techniques and algorithms have been proposed
including modulation, coding, cosine and wavelet
transform (Rajoub, 2002; Cox et al., 1968; Miaou et
al., 2005; Ahmed et al., 2009). While many
algorithms are deployed for the data compression,
few works combine the sampling step to the
compression as in level-crossing analog-to-digital
converter (LC-ADC) (Mark et al., 1981; Sayiner et
al., 1996). In the literature, LC-ADCs are essentially
used for audio signal processing particularly speech
and ultrasound signals (Allier et al., 2003; Kozmin
et al., 2009). In fact, since sampling occurs at
irregular times, LC-ADCs are suitable for the
conversion of bursty and sparse signals (Guan and
Singer, 2007). In the most of the applications, it has
been proven that significant performance
improvements can be achieved compared to the
conventional Nyquist converters in terms of power
Tlili, M., Ben-Romdhane, M., Maalej, A., Bali, M., Rivet, F., Dallet, D. and Rebai, C.
Accurate Level-crossing ADC Design for Biomedical Acquisition Board.
DOI: 10.5220/0005855003210326
In Proceedings of the 9th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2016) - Volume 4: BIOSIGNALS, pages 321-326
ISBN: 978-989-758-170-0
Copyright
c
2016 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
321

consumption and surface occupation (Kozmin et al.,
2009; Guan and Singer, 2007; Li et al., 2013).
In this work, an in-depth study of the main
design parameters associated with an LC-ADC is
proposed. The present study consists of a detailed
analysis of two main parameters that affect the
accuracy of the LC-ADC, namely the amplitude
resolution and the timer frequency. Additional
parameters can also affect the LC-ADC output
signal such as the accuracy of the quantization levels
and the comparator delay. As a result of this
analysis, the authors propose a methodology to
select accurate parameters for ECG signals
extraction.
To properly present this work, this paper is
organized as follows. First, the biomedical smart
sensing system architecture is introduced in Section
II. Section III describes the LC-ADC architecture. In
the same section, the authors present the design
considerations for an efficient ECG signal detection
to perform both signal compression and power
consumption reduction. Section IV presents the
results of behavioral simulations on different ECG
signals. The percentage root mean square difference
(PRD) is used to evaluate signal distortion compared
to uniform sampling. Section V concludes the paper.
2 SYSTEM OVERVIEW
The aim of the Wibio’ACT project is to implement a
smart system for biomedical signals acquisition and
transmission. The two main and innovative topics in
this project concern the digitization with an intrinsic
compression step via the use of LC-ADC and the
reconstruction with a minimum complexity in
implementation and a good recovery of the original
ECG signal.
2.1 Wibio’ACT System Presentation
The Wibio’ACT system is presented in Figure 1. An
acquisition of the biomedical signal is firstly done
through the use of non-invasive sensors that
wirelessly transmit signal so as to form a wireless
body area network (WBAN). The received signal,
often a voltage, is amplified and filtered. A classical
ADC, SAR (Long et al., 2014) or Sigma-Delta
(Giroud et al., 2014) architectures, conventionally
performs the digitization of the acquired analog
signals. In this project, LC-ADC is chosen thanks to
its capacity of compressing the acquired data. This
converter allows bypassing the compression of
digital data usually ensured by an algorithm
implemented on microcontroller. The transmitter is a
combination of several functions. They are the
mixing stage with a local oscillator (second input of
the mixer), as well as the amplification and the
filtering stages. At the receiver side, a front end
stage composed of functions such as filtering and
low noise amplification (LNA) is firstly used. In
order to have the original signals, a reconstruction
step is necessary to allow the doctor to visualize,
analyse and make diagnostics from the biomedical
signals.
Besides, the voltage that appears between the
sensor electrodes is conditioned via a front-end
interface. It includes functions such as amplification
using a programmable gain preamplifier (PGA) and
analog filtering with passive off-chip filters. For the
ECG signal acquisition, a PGA gain of 60 dB is
required (Hartmann, 2003). Passive filters including
a high-pass filter (HPF) and a low-pass filter (LPF)
are composed of capacitors and resistors. The HPF is
mainly used to cancel DC-level shift caused by
human skin and its cut-off frequency is set to 20
mHz. The LPF is used to eliminate interferers at
frequencies above those of ECG signals, so its cut-
off frequency is set to 200 Hz. These filtering steps
highly influence the reconstruction algorithm
performances as any noise would distort their
outputs.
The ECG signal acquisition system requires a
signal-to-noise ratio (SNR) of at least 61 dB in order
to detect heart activities precisely (Li et al., 2013).
The ADC to be chosen must have an equivalent
effective number of bits approximately equal to 10.
As the aim of Wibio’ACT is to enhance
transmission and reception of ECG signal with the
minimum power consumption, the authors propose
the use of LC-ADC. In fact, in this case, the
acquisition system exploits the features of the
biomedical signals with a small variation (or
information) rate to reduce the amount of sampled
data. As excepted results, the compression and
decompression blocks of the radio modules will be
removed and the average speed of the converter will
be reduced.
2.2 LC-ADC Principle
An LC-ADC uses level crossing detection to sample
the ECG signal after filtering. The converter’s
architecture shown in Figure 2 consists of two
comparators, a digital-to-analog converter (DAC),
an up/down counter and a time-to-digital converter
(TDC).
Two thresholds levels
and
are set to
Smart-BIODEV 2016 - Special Session on Smart Embedded Biomedical Devices for In Situ Physiological Signal Processing
322
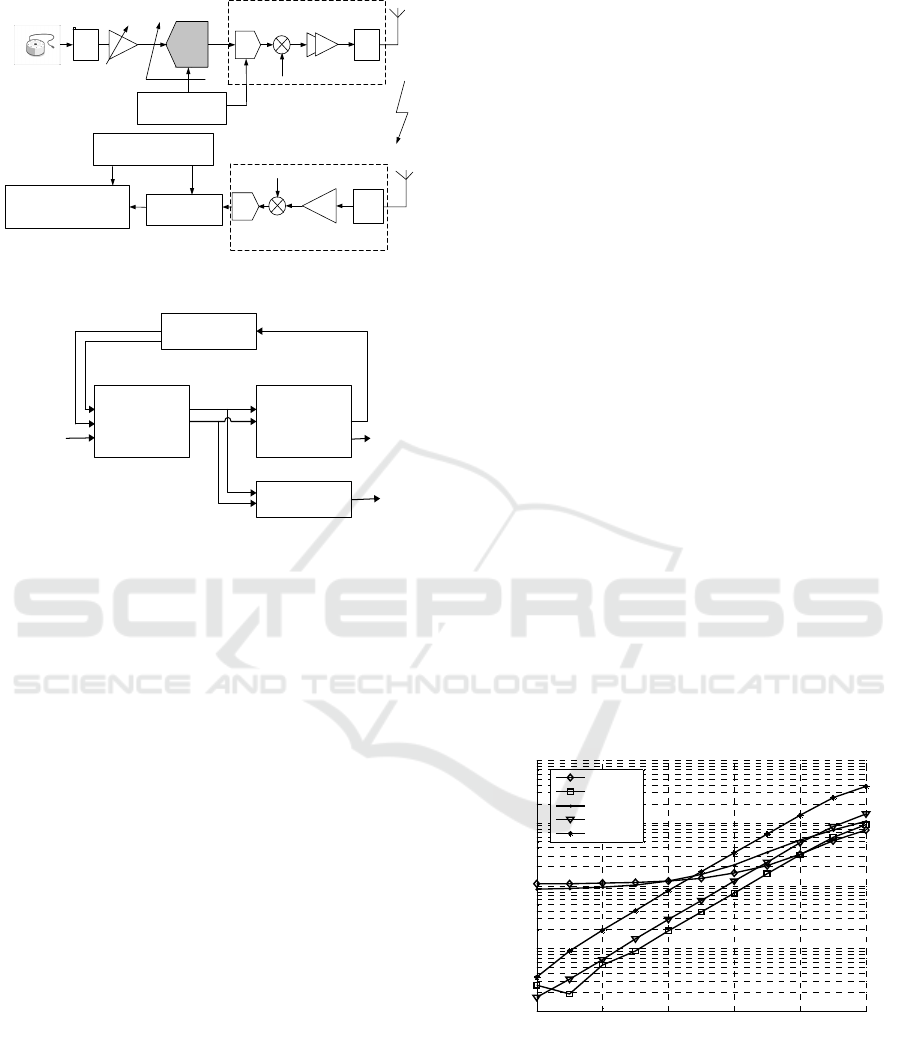
Figure 1: Architecture of Wibio’ACT acquisition board.
DAC
Up/Down
Counter
Timer
Comparators
V
IN
V
+
V
-
b
i
Dt
i
INC
DEC
Figure 2: LC-ADC converter architecture.
identify the signal value
. These signals are
generated via the digital-to-analog converter with a
difference equal to the quantization step. Thereby, in
digital representation, the difference between
and
is equal to 1 LSB. The sampling occurs when the
signal value
is either higher than
or lower
than
. In fact, according to the comparison result,
the increment signal (INC) or decrement signal
(DEC) are exclusively set to “1” and consequently
activate the up/down counter. The counter output is
either incremented or decremented by 1 LSB. This
signal controls the DAC whose generated signals,
and
, will be updated to keep tracking the
input value. LC-ADC samples are equivalent to the
up/down counter output. As long as the signal’s
value
is between
and
, INC and DEC are
both set to “0” and no changes occurs on the counter
or DAC outputs. Thus, no new sample is taken.
The LC-ADC converter adopts 2
1
levels
equally spaced along the input signal range where
is the converter resolution. Samples
are
generated only when the input signal
crosses the
defined levels. The time interval,
, between two
consecutive samples is measured by a timer of
period
. The conversion results of this LC-ADC
are thus composed of digital codes,
, for the
voltage magnitude and the time intervals,
. The
accuracy of data conversion using LC-ADC is
dependent on two main factors; the reconstruction
condition and the timer frequency.
3 LC-ADC DESIGN
CONSIDERATIONS
The LC-ADC samples are non uniformly taken.
Thus, the sampling frequency is variable. The
number of quantization levels and the signal
variations directly influence the number of samples
and so the average sampling frequency. Figure 3
presents results of average sampling frequency for
different ECG signals when varing the resolution
value . The set of ECG signals used in this
simulation is collected through Apnea-ECG
Database (apneaecg), combined measurement of
ECG Database-Breathing and Seismocardiograms
(cebsdb), Long Term ST Database (lgdb), Non-
Invasive Fetal ECG Database (nifecdb) and PTB
Diagnotic ECG Database (ptbdb) (Moody et al.,
2001). The maximum frequency of the ECG signal
f
max
is fixed to 200 Hz to ensure a good quality of
ECG parameters detection. The given signals are
oversampled and used in digital format in order to
emulate an analog signal. The amplitude signal is
scaled to the LC-ADC full-scale amplitude. The
ECG signal is sampled using the LC-ADC with
different resolution values, . The irregular
sampling instants are stored to compute the average
sampling frequency.
Figure 3: Average sampling frequency versus resolution
for ECG signals.
It can be noticed from Figure 3 that the average
sampling frequency depends of the LC-ADC
resolution . To satisfy Shannon theorem that
imposes the use of a sampling frequency at least
equal to the double of the input frequency, the
Biomedical
sensor
Amplifier
Digital
reconstruction
Filter
Filter
DAC
Filter
Power
amplifier
Mixer
Transmitter
Human-Machine Interface
for drawing the biomedical
signal
Receiver
LNA
Mixer
Microcontroller
(µC)
Central Processing
Unit(CPU)
ADC
LC-ADC
2 4 6 8 10 12
10
1
10
2
10
3
10
4
10
5
Resolution (Bits)
Average Sampling Frequency (Hz)
apneaecg
cebsdb
ltdb
nifecgdb
ptbdb
Accurate Level-crossing ADC Design for Biomedical Acquisition Board
323
minimum required average sampling frequency is
equal to 400 Hz. At this frequency, and according to
the input signal, a minimum of 7 bits is needed to
recover the original signal after LC-ADC
digitization.
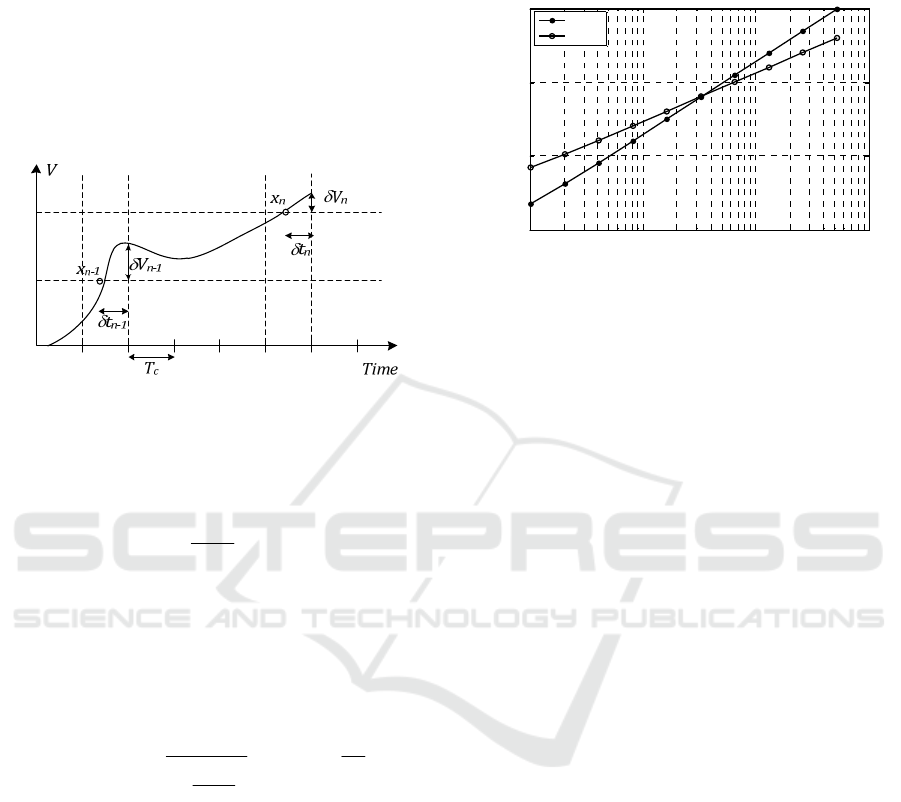
The second factor in the LC-ADC design
consideration is the timer frequency. Quantization
noise is added to the signal due to the inexact time of
the sampling instants resulting in jitter noise as
presented by Figure 4.
Figure 4: Quantization error due to inexact sampling time.
This error in time, , causes an error to the
output voltage as in (1), where the derivative of
with respect to is the slope of the input signal.
t
d
t
dV
V
IN
(1)
In this case, the SNR of such system is defined as
the ratio of the signal power, computed according to
value, to the noise power depending of . The
theoretical value for the LC-ADC case can be
computed as in (2), where
is the timer clock
period which determines (Allier et al., 2003).
C
10
IN
IN
10dB
T
log
dt
dV
P
VP
log 10=SNR
1
20
12
(2)
According to (2), the SNR no longer depends on the
bit resolution of the ADC but instead depends on the
timer period
and the statistical properties of the
input signal
. In Figure 5, the SNR and the
effective number of bits (ENOB) are plotted versus
for ECG signal.
In the irregular sampling scheme, the SNR can
be computed from the power density spectrum
(PSD) of the reconstructed ECG signal. In this
paper, the cubic spline interpolation is the
reconstruction algorithm. Doubling the counter
frequency results in 6 dB increase of SNR. In fact, to
reach an ENOB of 10 bits, a timer frequency of 71
MHz, equivalent to a period
of 0.14 s is
considered. Hence, an SNR of 62 dB is ensured by
this LC-ADC. From Figure3, with an ENOB equal
to 10 bits, the average sampling frequency for the
selected database signals is between 3 to 15 kHz.
Figure 5: SNR and ENOB versus timer frequency for ECG
signal.
Additional factors can influence the performance
of the LC-ADC such as the the variation of the
comparator delay, the accuracy of the quantization
levels and the reconstruction errors due to spline
interpolation. Those errors might be taken into
account in future work to avoid SNR degradation
(Ravanshad et al., 2013).
4 SIMULATIONS RESULTS ON
ECG SIGNALS
The LC-ADC can compress the sampled data for the
same level of performance measured by SNR in case
of uniform sampling. It is highly important to
accurately choose the design specifications of the
converter that are evaluated through the quality of
the reconstructed signals. To demonstrate the
efficiency of the proposed design in detecting ECG
signals, the LC-ADC converter was simulated using
a Simulink model for various ECG records obtained
from different databases (Moody et al., 2001). The
simulation parameters are 0.14 s for
and 10 bits
for the resolution M. Since level-crossing is an
irregular sampling and in order to use the standard
distorsion mesure which is the percentage root mean
square difference (PRD), the signal reconstruction
based on spline interpolation was performed.
Figure 6 shows the temporal representaion of
PTB Diagnotic ECG Database (ptbdb) signal at the
input and the output of the LC-ADC. A
reconstruction scheme is applied on the output, and
presented in the second curve of Figure 6.
In order to measure the signal quality, the PRD
of the reconstrcuted signal is measured. The LC-
10
3
10
4
10
5
10
6
20
40
60
80
Timer Fre
q
uenc
y
(
Hz
)
Signal-to-Noise Ratio (dB)
10
3
10
4
10
5
10
6
0
5
10
15
ENOB
SNR
ENOB
Smart-BIODEV 2016 - Special Session on Smart Embedded Biomedical Devices for In Situ Physiological Signal Processing
324
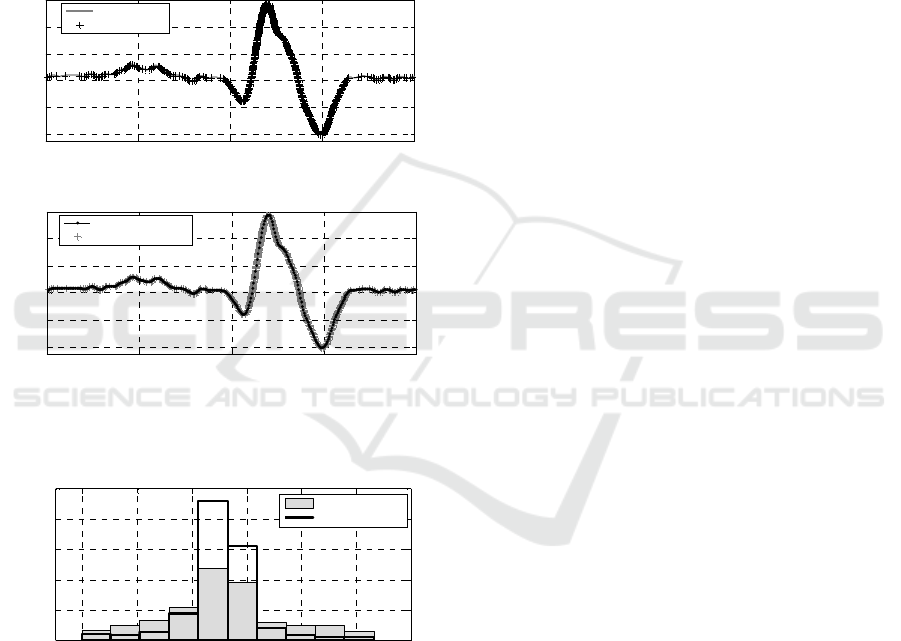
ADC ensures a PRD of 1%. For a lifestyle
application, a PRD value lower than 2% is
considered to be adequate as it corresponds to a
‘very good’ reconstruction quality (Zigel et al.,
2000). For the same level of SNR and compared to
uniform sampling, the LC-ADC compresses the
sampled data. As it is show in Figure 7, the LC-
ADC reduces the number of low changing voltage
sample. In fact, the number of samples representing
the small variation between 0.2 and 0 mV are
reduced by almost 44%. The total number of
samples are reduced by 13%.
(a)
(b)
Figure 6: LC-ADC input and output signals (a) and the
reconstructed signal after LC-ADC digitization (b).
Figure 7: Number of samples in the case of uniform
sampling and irregular sampling using LC-ADC.
5 CONCLUSIONS
As demonstrated in this paper, LC-ADC compresses
the signal in case of low changing amplitudes. This
work investigates the use of LC-ADC to digitize the
ECG signals while ensuring an SNR of 62 dB. In
fact, it defines the design specification of the LC-
ADC converter in order to guarentee a good
representation of such vital biomedical signal. To
measure the reconstructed signal quality, the PRD
parameter is selected. The computed PDR is equal of
1%. Such value is considered to be adequate in
biomedical signal processing field. As future work,
the LC-ADC circuit implementation can be realized
in CMOS process for the proposed values of design
specifications. The comparators are hysteretic and
can also be implemented as Schmitt triggers. The
DACs can be implemented by using the capacitors
or the resistor-capacitor hybrid. The digital blocks
are simple and can also be designed off-chip.
In addition, future work is necessary to design
and implement an adaptive LC-ADC architecture
that aims to obtain higher compression rates and
more significant power reduction compared to the
conventional LC-ADC.
ACKNOWLEDGEMENTS
The authors would like to thank the CMCU (Comité
Mixte de Coopération Universitaire) to financially
support this project. The funding program is
Partenariat Hubert-Curien Utique (PHC-Utique)
2015 N°15G1407.
REFERENCES
Ahmed, S. M., Al-Ajlouni, A. F., Abo-Zahhad, M., Harb,
B., 2009. ECG signal compression using combined
modified discrete cosine and discrete wavelet
transforms, Journal of Medical Engineering and
Technology.
Allier, E., Sicard, G., Fesquet, L., Renaudin, M., 2003. A
new class of asynchronous A/D converters based on
time quantization, International Symposium on
Asynchronous Circuits and Systems, IEEE.
Cox, J. R., Nolle, F. M., Fozzard, H. A., Oliver, C. G.,
1968. AZTEC, a preprocessing program for real time
ECG rhythm analysis, IEEE Transactions on
Biomedical Engineering.
Giroud, F., Persechini, P., Ruedi, P.-F., Viemon, F.,
Masson, F., 2014. ECG sensor interface in a low
power SoC for wireless portable ECG monitoring,
Biomedical Circuits and Systems Conference, IEEE.
Guan, K., Singer, A., 2007. Opportunistic sampling of
bursty signals by level-crossing—An information
theoretical approach, 41st Annual Conference on
Information Sciences and Systems.
Gyselinckx, B., Vullers, R.J.M., Van Hoof, C., Ryckaert,
J., Yazicioglu, R.F., 2006. Human++: Emerging
Technology for Body Area Networks, VLSI-SoC.
Hartmann, E., 2003. ECG front-end design is simplified
0,4 0,5 0,6 0,7 0,8
-0.6
-0.4
-0.2
0
0.2
0.4
Time (s)
Amplitude (mV)
LC-ADC input
LC-ADC output
0.4 0.5 0.6 0.7 0.8
-0.6
-0.4
-0.2
0
0.2
0.4
Time
(
s
)
Amplitude (mV)
Reconstructed signal
LC-ADC output
-0.6 -0.4 -0.2 0 0.2 0.4 0.6
0
1000
2000
3000
4000
5000
Variation (mV)
Number of samples
Irregular sampling
Uniform sampling
Accurate Level-crossing ADC Design for Biomedical Acquisition Board
325

with microconverter, Analog Dialogue.
Kozmin, K., Johansson, J., Delsing, J., 2009. Level
crossing ADC performance evaluation toward
ultrasound application, IEEE Transactions on. Circuits
and Systems I: Regular Papers.
Li, Y., Zhao, D., Serdijn, W. A., 2013. A sub-microwatt
asynchronous level-crossing ADC for biomedical
applications, IEEE Transactions on Biomedical
Circuits and Systems.
Long, Y., Harpe, P., Pamula, V.R., Osawa, M., Harada,
Y., Tamiya, K., Van Hoof, C., Yazicioglu, R.F., 2014.
A 680 nA ECG Acquisition IC for Leadless
Pacemaker Applications, IEEE Transactions on
Biomedical Circuits and Systems.
Mark, J. W., Todd, T. D., 1981. A nonuniform sampling
approach to data compression, IEEE Transactions on
Communications.
Mendis, S., Puska, P., Norrving, B., 2011. Global atlas on
cardiovascular disease prevention and control, World
Health Organization.
Miaou, S.G., Chao, S.N., 2005. Wavelet-based lossy-to-
lossless ECG compression in a unified vector
quantization framework, IEEE Transactions on
Biomedical Engineering.
Moody, G. B., Mark, R. G., Goldberger, A. L., 2001.
PhysioNet: a web-based resource for the study of
physiologic signals, IEEE Engineering in Medicine
and Biology Magazine.
Rajoub, B., 2002. An efficient coding algorithm for the
compression of ECG signals using the wavelet
transform, IEEE Transactions on Biomedical
Engineering.
Ravanshad, N., Rezaee-Dehsorkh, H., Lotfi, R., 2013.
Detailed study of the time estimation in level-crossing
analog-to-digital converters, Iranian Conference
Electrical Engineering.
Sayiner, N., Sorensen, H. V., Viswanathan, T. R., 1996. A
level-crossing sampling scheme for A/D conversion,
IEEE Transactions on Circuits and Systems II, Analog
and Digital Signal Processing.
Zigel, Y., Cohen, A., Katz, A., 2000. The weighted
diagnostic distortion (WDD) measure for ECG signal
compression, IEEE Transactions on Biomedical
Engineering.
Smart-BIODEV 2016 - Special Session on Smart Embedded Biomedical Devices for In Situ Physiological Signal Processing
326
