
A Health Virtual Community Perspective for Peripheral
Arterial Disease
The Need of an E-solution for PAD
Christo El Morr
1
, Peggy Ng
2
, Amber Purewal
3
, Courtney Cole
4
,
Musaad Al Hamza
5
and Mohamed Al Omran
6
1
School of Health Policy and Management, York University, 4700 Keele St, Toronto, Canada
2
School of Administrative Studies, York University, 4700 Keele St, Toronto, Canada
3
School of Health Policy and Management, York University, 4700 Keele St, Toronto, Canada
4
ForAHealthyMe.com, Toronto, Canada
5
University of Toronto, Toronto, Canada
6
Vascular Surgery Division, Saint Michael’s Hospital, Toronto, Canada
Keywords: Peripheral Arterial Disease, Chronic Disease Management, eHealth, Health Informatics, Cardiovascular
Disease, Analytics, Virtual Communities, Health Virtual Communities.
Abstract: This paper summarizes the result of a survey conducted on 239 subject in Toronto to gauge their awareness
of Peripheral Arterial Disease (PAD) and educate them about it. The results show that awareness of PAD is
scarce and that the campaign resulted in a significant increase in awareness. This intervention suggest that an
e-education tool is of paramount importance to address the lack of awareness. The paper argues that a PAD
Virtual Community might play a pivotal role in educating the public about PAD and providing a platform for
awareness and prevention.
1 INTRODUCTION
PAD is a condition caused by blockages of the
arteries that provide blood flow to the extremities.
The ankle-brachial index test compares the blood
pressure measured at the ankle, to the blood pressure
measured at the arm. A lower ankle-brachial index
number represents blockages or narrowing of the
arteries. Since PAD is a condition involving
narrowing and blockages of the arteries, an ankle
brachial index test can help recognize its presence
(Kim et al., 2012).
PAD is defined as an ankle-brachial index of less
than 0.9 (Doraiswamy et al., 2009). The ankle
brachial index is the ratio of the blood pressure in the
lower legs to the blood pressure in the arms. The
ankle-brachial index test is a method of measuring an
individual’s risk for peripheral artery disease and is
non-invasive.
Peripheral Arterial Disease (PAD) is an important
public health problem worldwide. It is a widely
prevalent condition affecting 800,000 Canadians, of
which twelve to twenty-nine percent are elderly
(Lovell et al., 2009). It has been estimated that more
than 200 million people were living with PAD
(Fowkes et al., 2013).
The incidence of PAD increases with age and
exposure to the risk factors of atherosclerosis.
However, PAD is given little attention and is referred
as a ‘silent’ cardiovascular disease, with thousands of
Canadians being at risk for preventable heart attacks.
Approximately one-half of all individuals with PAD
are asymptomatic. Studies show that at least one-third
of individuals with asymptomatic PAD, and with at
least one full blockage in a major artery of the leg. In
Canada, the population-based prevalence of PAD has
not been directly assessed. However, approximately
four percent of the population older than forty years
of age in developed nations have PAD (Lovell et al.,
2009).
PAD is a strong indicator of diffuse
atherosclerotic disease; patients have 4 times higher
risk of developing myocardial infarction, and nearly
triple the risk of getting cerebrovascular events
512
Morr, C., Ng, P., Purewal, A., Cole, C., Hamza, M. and Omran, M.
A Health Virtual Community Perspective for Peripheral Arterial Disease - The Need of an E-solution for PAD.
DOI: 10.5220/0005826405120516
In Proceedings of the 9th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2016) - Volume 5: HEALTHINF, pages 512-516
ISBN: 978-989-758-170-0
Copyright
c
2016 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

compared to the general population (Criqui et al.,
1992; Wilterdink and Easton, 1992). In addition,
patients with intermittent claudication, the usual
initial symptom of PAD, have a 5-year morbidity and
mortality of 20-30% from ischemic events of
atherosclerosis, i.e. myocardial infarction and stroke
(Criqui et al., 1992; McDermott, 2002).
PAD is still not well addressed in practice, even
though peripheral arterial disease is simple to detect
and has severe consequences and even though
treating it, or avoiding it, results in significant health
and economic gain (Al-Omran et al., 2006; Al-Omran
et al., 2011; Chow et al., 2008; Criqui, 2001).
In order to (1) raise awareness about PAD in the
Toronto community, (2) measure the level of
awareness of the population about PAD and (3) gauge
the readiness of the population for an Information and
Communication Technology based solution, we have
conducted an intervention that we present its findings
in this paper.
2 THE INTERVENTION
Between September and October 2014 our team has
conducted an awareness campaign in Toronto in 4
different areas of the city that were chosen based on a
convenient sampling approach.
We’ve developed a questionnaire to gauge the
knowledge of a subject on PAD symptoms, risk
factors, preventable measures, treatment modalities
and complications. A total of 239 subject answered a
questionnaire in 3 different areas of Toronto.
The subjects were all asked questions about PAD
and were given an explanation about the disease its
symptoms, risk factors, preventable measures,
treatment modalities and complications. Each subject
was given a score based on her answers. A correct
answer was given one point and an incorrect answer
a zero. We have computed the scores at the baselines
and the scores at follow-up after 6 weeks.
We divided the subjects into two groups
experimental and control. The experimental group
subjects received a pamphlet, the control group
subjects did not. We hypothesized that those who
received a pamphlet will have more retention spam
than those who did not receive one. A follow-up
interview by phone and email was conducted at six
weeks to measure any change in PAD knowledge. In
the follow-up the number of subjects dropped to 76,
38 of which were in the control and 38 in the
experimental.
3 RESULTS
Our convenience sample included 156 female
(65.3%) and 83 male (34.7%) who were interviewed
at three community center and the City Hall.
Most of the subjects (76.1%) were over 41 years
old; 32.2% were 41-60 and 43.9% were over 60 years
old. Only 2.9% were under 20 and 20.9% were
between 21 and 40. It is well known that PAD is
related to age, and our sample did represent the older
age group.
Most of the subject (78.66%) did not hear about
PAD (Figure 1). This confirms a well known fact that
Most Canadians do not know that PAD is a major risk
factor for heart attack, stroke and death (Lovell et al.,
2009)
Figure 1: Subject’s Awareness of PAD.
Most of the subjects were highly educated 90.8% of
the interviewee had a high school or a higher
education degree while 4.2 % attended intermediate
school and 5% attended only primary education
(Figure 2).
Figure 2: Subject’s Education level.
We have used a t-test to test if the difference in scores
between the subjects in the follow-up and their scores
in the baseline. The difference in knowledge scores
was found statistically significant in all 5 aspects of
A Health Virtual Community Perspective for Peripheral Arterial Disease - The Need of an E-solution for PAD
513
PAD between baseline and follow-up for all the 76
subjects. We then tested the significance of change in
scores for each group (experimental and control) for
all the 5 aspect of knowledge. The change was found
to be significant for all 5 aspects in the experimental
group. In the control group that change was only
significant for the knowledge of preventable
measures and treatment modalities.
In terms of questions related to the user’s
readiness in information and communication
technology, the results showed that the younger
population prefer to receive health information via
mobile Apps while elderly prefer usual cell phone and
are wary of Apps. All age groups valued receiving
health information via web pages and email.
In terms of ownership, elderly are prone to have
desktops and laptops more than smartphones iPads
and the like.
High majority of respondents did not appreciate
receiving health information through communication
channels such Facebook, Twitter or YouTube.
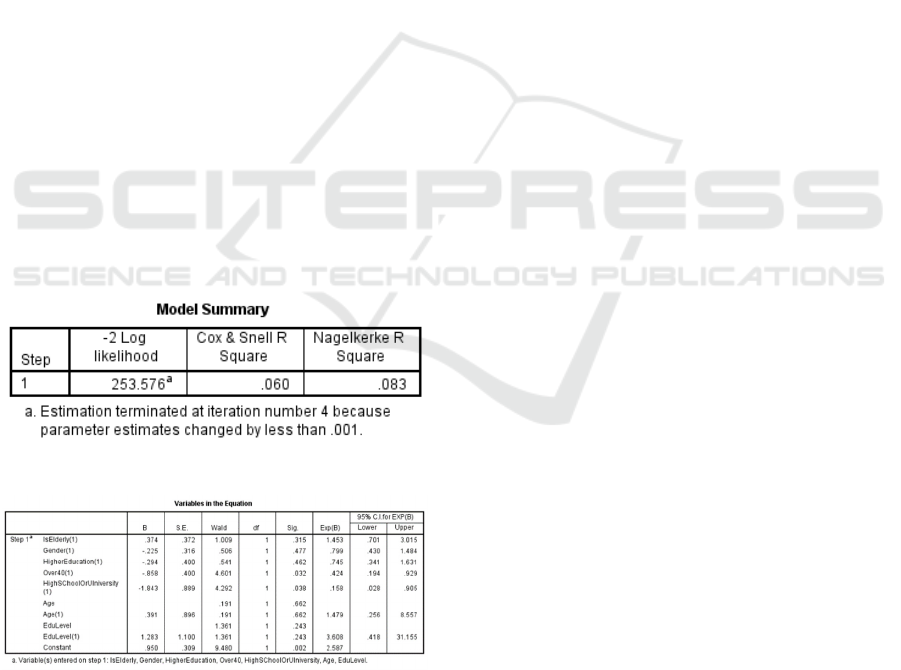
When conducting a logistic regression analysis to
see if age, gender, and education level had an effect
on using a desktop or laptop to connect to the internet,
the analysis showed that both age and the education
level had an effect on the usage of desktops and
laptops. Gender effect was not significant. Being in
the group of people with Age above 40 and people
with Education level high school or university is
significantly correlated with the use of desktops and
laptops to connect to the internet (figure 3 and 4).
Figure 3: Logistic Regression Model Summary.
Figure 4: Logistic Regression Variables.
4 DISCUSSION
The survey showed that a simple intervention with a
simple pamphlet had an effect on the
knowledge/awareness of PAD. The most important is
that even the knowledge of the control group was
enhanced by the simple fact of being exposed to the
verbal explanation during the awareness campaign.
These results suggest that a future e-awareness based
intervention might be more effective and might allow
understand the different characteristics of the people
seeking information and the features that increase the
chance of retention.
On the other hand, since age is a factor affecting
PAD, and people above 40 are correlated with the use
of Desktop and laptops and people above 60 have are
still using cell phones (not smart phones), any
awareness e-tool should take into consideration these
communication channels.
While younger population have a preference
towards Apps; these results were expected. Finally,
less than 5% of all surveyed had preference to
Facebook, Twitter or YouTube, this might indicate
some concerns related to security and confidentiality.
4.1 A Vision of PAD Virtual
Community
A virtual community is a group of people meeting
online to achieve a certain goal, using specific roles
and specific software(Preece, 2000). The concept has
emerged in 1990 with the emergence of the world
wide web. Besides, following the development in the
mobile devices, mobile virtual community were
developed too (El Morr, 2007a, El Morr, 2007b, El
Morr and Kawash, 2007). Soon health related virtual
communities have developed with support to the
healthcare delivery (Gustafson et al., 2001). The
concept of patient centric healthcare delivery
emerged and health virtual community could play an
important role in this field.
Research has demonstrated effectiveness and
efficiency effects linked to VCs for multiple health
conditions (chronic kidney disease, pulmonary
hypertension, cancer) (Bender et al., 2013; El Morr et
al., 2014; Frost et al., 2014; Matura et al., 2013),
especially the engagement of patients in the
management of their own health (Matura et al., 2013;
Vasconcellos-Silva et al., 2013).
A health virtual community for public awareness
of PAD may allow the following advantages over
paper based awareness campaign:
1- It will allow the users to have a tailored and
detailed message that suits the personal
characteristics of the person. For instance, the
information can be communicated using a
language that is most convenient for the potential
HEALTHINF 2016 - 9th International Conference on Health Informatics
514

patient. We have noticed language barrier in a
multicultural city like Toronto. An electronic
delivery system allows the user to choose the
language they want to receive the information.
This is in line with the fact that for example some
immigrant population has a low awareness of
heart disease and stroke (Chow et al., 2008). As a
result, it is possible that PAD is not explained in
the context of different languages and cultures.
2- Besides, the virtual community allows people to
communicate with each other, allowing mutual
support (Welbourne et al., 2013).
3- Virtual Communities proved to be excellent tools
for the evaluation of the physical health status of
a community member, which includes objective
clinical indicators and subjective assessment of
coping ability (Seçkin, 2013). This will allow a
more targeted awareness content and eventually
clinical follow-up.
4- A PAD virtual community will have the
advantage of collecting huge amount of data about
individuals with PAD which constitute a great
source for analytics and new findings.
5- A PAD virtual community allows the content to
be tailored to different delivery channels that suits
the profile of the user (e.g. Apps, web pages, cell
phone short messages). The impact of a tailored
messaging would enhance awareness.
In a PAD virtual community one can allow
patients to receive information and to produce
information (e.g. blood pressure, glucose level in the
blood). Once the healthcare providers receive this
information, they can adjust their treatment or advise
the patients to adjust in a certain way (e.g. life style,
medication).
In a PAD-oriented health virtual community the
PAD awareness would be much more effective and
efficient, having a direct impact on the population
health in terms of prevention or chronic disease
management (Winkelman and Choo, 2003; World
Health Organization, 2005). The economic impact
and social impact would be tremendous.
5 CONCLUSIONS
We conducted a PAD awareness campaign that
measures the knowledge of a sample of the
population in Toronto about PAD as well as their IT
readiness. We followed up the sample after 6 weeks
showed that the experimental group (group that
received a pamphlet) showed significant
enhancement in knowledge of PAD in terms of
symptoms, risk factors, preventable measures,
treatment modalities and complications. We have
observed that even the control group showed
enhanced knowledge in preventable measures and
treatment modalities. It is encouraging that awareness
– even verbally- brings enhanced knowledge in the
preventive measures that can be taken by an
individual.
The sample showed clear preference to the use of
desktop and laptops for browsing internet and
searching for health information. Cell phone was a
mode of communication preferred by elderly. A
Health Virtual Community could have an impact in
the under-served field of PAD and have impact on the
health, social and economic aspects of the disease.
ACKNOWLEDGEMENTS
We would like to acknowledge the Ontario Center of
Excellence for funding this study.
REFERENCES
Al-Omran, M., Lindsay, T. F., Major, J., Jawas, A., Leiter,
L. A., Verma, S. and Systematic Assessment of
Vascular Risk, I. (2006) Perceptions of Canadian
vascular surgeons toward pharmacological risk
reduction in patients with peripheral arterial disease.
Ann Vasc Surg, 20(5), pp. 555-63.
Al-Omran, M., Verma, S. and Lindsay, T. F. (2011)
Suboptimal use of risk reduction therapy in peripheral
arterial disease patients at a major teaching hospital.
Ann Saudi Med, 31(4), pp. 371-5.
Bender, J. L., Jimenez-Marroquin, M. C., Ferris, L. E.,
Katz, J. and Jadad, A. R. (2013) Online communities
for breast cancer survivors: a review and analysis of
their characteristics and levels of use. Support Care
Cancer, 21(5), pp. 1253-63.
Chow, C. M., Chu, J. Y., Tu, J. V. and Moe, G. W. (2008)
Lack of awareness of heart disease and stroke among
Chinese Canadians: results of a pilot study of the
Chinese Canadian Cardiovascular Health Project. Can
J Cardiol, 24(8), pp. 623-8.
Criqui, M. H. (2001) Peripheral arterial disease--
epidemiological aspects. Vasc Med, 6(3 Suppl), pp. 3-7.
Criqui, M. H., Langer, R. D., Fronek, A., Feigelson, H. S.,
Klauber, M. R., McCann, T. J. and Browner, D. (1992)
Mortality over a period of 10 years in patients with
peripheral arterial disease. N Engl J Med, 326(6), pp.
381-6.
Doraiswamy, V. A., Giri, J. and Mohler, E. (2009)
Premature peripheral arterial disease – difficult
diagnosis in very early presentation. The International
Journal of Angiology : Official Publication of the
International College of Angiology, Inc, 18(1), pp. 45-47.
A Health Virtual Community Perspective for Peripheral Arterial Disease - The Need of an E-solution for PAD
515

El Morr, C. (2007a) Mobile Virtual Communities. in
Taniar, D., (ed.) Encyclopedia in Mobile Computing &
Commerce: Information Science Reference. pp. 632-
634.
El Morr, C. (2007b) Mobile Virtual Communities in
Healthcare: Managed Self Care on the move. in
International Association of Science and Technology
for Development (IASTED) - Telehealth
(2007),Montreal, Canada.
El Morr, C., Cole, C. and Perl, J. (2014) A Health Virtual
Community for Patients with Chronic Kidney Disease.
Procedia Computer Science, 37, pp. 333–339.
El Morr, C. and Kawash, J. (2007) Mobile Virtual
Communities Research: A Synthesis of Current Trends
and a Look at Future Perspectives. International
Journal for Web Based Communities, 3(4), pp. 386-
403.
Fowkes, F. G., Rudan, D., Rudan, I., Aboyans, V.,
Denenberg, J. O., McDermott, M. M., Norman, P. E.,
Sampson, U. K., Williams, L. J., Mensah, G. A. and
Criqui, M. H. (2013) Comparison of global estimates of
prevalence and risk factors for peripheral artery disease
in 2000 and 2010: a systematic review and analysis.
Lancet, 382(9901), pp. 1329-40.
Frost, J., Vermeulen, E. I. and Beekers, N. (2014)
Anonymity Versus Privacy: Selective Information
Sharing in Online Cancer Communities. J Med Internet
Res, 16(5), pp. e126.
Gustafson, D. H., Hawkins, R. P., Boberg, E. W.,
McTavish, F., Owens, B., Wise, M., Berhe, H. and
Pingree, S. (2001) CHESS: 10 years of research and
development in consumer health informatics for broad
populations, including the underserved. in Patel, V. L.,
Rogers, R. and Haux, R., (eds.) The 10th World
Congress on Medical Informatics (Medinfo
2001),London,UK: IOS Press. pp. 1459-1463.
Kim, E. S., Wattanakit, K. and Gornik, H. L. (2012) Using
the ankle-brachial index to diagnose peripheral artery
disease and assess cardiovascular risk. Cleve Clin J
Med, 79(9), pp. 651-61.
Lovell, M., Harris, K., Forbes, T., Twillman, G., Abramson,
B., Criqui, M. H., Schroeder, P., Mohler, E. R., 3rd and
Hirsch, A. T. (2009) Peripheral arterial disease: lack of
awareness in Canada. Can J Cardiol, 25(1), pp. 39-45.
Matura, L. A., McDonough, A., Aglietti, L. M., Herzog, J.
L. and Gallant, K. A. (2013) A virtual community:
concerns of patients with pulmonary hypertension. Clin
Nurs Res, 22(2), pp. 155-71.
McDermott, M. M. (2002) Peripheral arterial disease:
epidemiology and drug therapy. Am J Geriatr Cardiol,
11(4), pp. 258-66.
Preece, J. (2000) Online Communities: Designing Usability
supporting Sociability, USA:
John Wiley & Sons Ltd.
Seçkin, G. (2013) Satisfaction with health status among
cyber patients: testing a mediation model of electronic
coping support. Behaviour & Information Technology,
32(1), pp. 91-101.
Vasconcellos-Silva, P. R., Carvalho, D. and Lucena, C.
(2013) Word Frequency and Content Analysis
Approach to Identify Demand Patterns in a Virtual
Community of Carriers of Hepatitis C. Interactive
Journal of Medical Research, 2(2), pp. e12.
Welbourne, J. L., Blanchard, A. L. and Wadsworth, M. B.
(2013) Motivations in virtual health communities and
their relationship to community, connectedness and
stress. Comput. Hum. Behav., 29(1), pp. 129-139.
Wilterdink, J. L. and Easton, J. D. (1992) Vascular event
rates in patients with atherosclerotic cerebrovascular
disease. Arch Neurol, 49(8), pp. 857-63.
Winkelman, W. J. and Choo, C. W. (2003) Provider-
sponsored virtual communities for chronic patients:
improving health outcomes through organizational
patient-centred knowledge management. Health
Expectations, 6(4), pp. 352-358.
World Health Organization (2005) Preventing Chronic
Disease: A Vital Investment. Geneva, Switzerland:
World Health Organization (WHO).
HEALTHINF 2016 - 9th International Conference on Health Informatics
516
