
CONTEXTUAL ANALYSIS AND MODELING
OF PERSONAL WELLNESS
Antto Seppälä and Pirkko Nykänen
University of Tampere, School of Information Sciences, eHealth Research, Kanslerinrinne 1, Tampere, Finland
Keywords: Personal wellness, Contextual analysis, Information model, Focus group.
Abstract: The healthcare paradigm is progressing towards preventive care and proactive services with holistic and
personalized view on health and wellbeing. The concept wellness has been used to describe this holistic
approach to health and well-being. Different wellness tools have already been introduced and some wellness
applications are available to be used to manage and maintain personal wellness. With the technology
advances like ubiquitous computing the number of different wellness systems will increase rapidly. To
maximize the benefits of the new healthcare paradigm and wellness systems semantic interoperability is a
necessity. Therefore there is a need for a personal wellness ontology which enables sharing of information
between all actors in the wellness ecosystem. This study analyzes the context of personal wellness and starts
the work on the personal wellness ontology by presenting a high-level information model of the domain.
The results of this research help to take into account the different contextual aspects of wellness information
covering also the privacy, confidentiality and security contexts.
1 INTRODUCTION
The healthcare paradigm focused on treatment of
diseases is progressing to the direction of preventive
and proactive care paradigm with distributed
services and a more personalized, holistic and
lifelong view on health and wellness (Nykänen,
2008; Koop et al., 2008). Healthcare delivery is seen
as a broader continuum with empowered citizens
and networked interoperable services. Future
healthcare will focus on health, functioning, and
wellbeing of citizens (Larson, 1999). The current
health information systems and electronic health
records are planned to support hospital-centric care
and thus they are not able to support the
personalized and preventive care paradigm.
The concept wellness has been used to refer to a
holistic approach for health and wellbeing of
citizens. Personalized wellness approaches focus on
improved lifestyle and behavioral choices. Health
promotion and education, and support for wellness
approaches are major trends in the modern world
and are becoming more visible through different
media (Kickbusch and Payne, 2003). Wellness tools
for self-management activities have been widely
studied in different research projects and already
there are several applications intended for
supporting wellness activities (Ahtinen et al., 2009;
Varshney, 2007; Nykänen, 2008).
Wellness informatics focuses on enabling the
citizens to stay well and manage their own health
and wellness even without participation of
healthcare providers. Wellness informatics is a
human-centric approach where citizens are thought
to be both information sources and users (Grinter,
Siek and Grimes, 2010). Wellness informatics aims
at helping citizens to collect their own data from
multiple sources, to reflect their wellness, to support
healthy living, to enable collaboration beyond
provider networks, to allow people to collaborate
with each other and to share their personal wellness
information. Wellness data can include different
measurement data, medical data, behavioral data,
socio-economic and cultural data. It is a challenge to
integrate all this data together and also to
acknowledge the contexts of information (Grinter et
al., 2010).
This study presents research focusing on trusted
personal health and wellness information in
ubiquitous environment (Nykänen et al., 2009). The
aim of this research is to present a trusted context-
aware information model for a lifelong personal
wellness record and a security architecture for
trusted use of multisource heterogeneous personal
202
Seppälä A. and Nykänen P..
CONTEXTUAL ANALYSIS AND MODELING OF PERSONAL WELLNESS.
DOI: 10.5220/0003636902020207
In Proceedings of the International Conference on Knowledge Engineering and Ontology Development (KEOD-2011), pages 202-207
ISBN: 978-989-8425-80-5
Copyright
c
2011 SCITEPRESS (Science and Technology Publications, Lda.)

wellness information. In order to enable semantic
interoperability between the various wellness
systems there is a need to develop an ontology
which creates shared understanding and enables
sharing of heterogeneous information among
different actors and systems (Blobel et al., 2010).
The first objective of our research was to
perform a contextual analysis on the personal
wellness concept, how it is conceptualized and what
kinds of external contexts are related to it. The
second main objective was to create a high-level
information model of personal wellness. In this
paper we present modeling of the wellness concept
and build the basis for the development of a personal
wellness ontology.
2 METHODS
This study had three main methods:
1. A literature analysis to find out how wellness
and personalized health is presented and
defined in the literature and what are the
common characteristics.
2. A contextual analysis to understand what
wellness is and to model the components of
personal wellness.
3. Focus group meetings to understand how
normal healthy people conceptualize personal
wellness and what kind of concepts are related
to their personal wellness management and
maintenance.
First we made a literature analysis to find out
how wellness and a holistic view on health is seen
and defined in the literature to conclude common
characteristics, concepts and components of
wellness. The focus of was on wellness, but because
health, wellness and well-being are used
interchangeably in the literature we had to concern
also holistic health and well-being models (Kirsten
et al., 2009). In the analysis we focused on holistic
health, wellness or well-being, and on the
components of the future health care paradigm.
After the literature analysis, we performed
contextual analysis of the collected materials. This
analysis helped us to understand what information is
related to wellness and how citizens manage their
wellness. The external contexts and other things
affecting personal wellness were also modeled. As a
result we could define the scope and the contents of
the concept wellness.
Next, we organized two half-day meetings for
small focus group to get empirical information about
how personal wellness is understood and what
contexts are related to it. We were interested to
model how normal healthy people conceptualize
personal wellness. The focus group was composed
on the department staff members, healthy young
persons. Participants for the focus group were
collected with an open call, on voluntary basis, and
the number of persons participating in the meetings
was 5 (1
st
meeting) and 4 (2
nd
meeting).
After the first meeting we created a mind map
based on the discussion. Mind map was chosen as
the tool to represent the information because it is
easy to understand and to follow and most people
are familiar with the technique. Also with the mind
map we were able to do simple categorizations of
concepts and conclude some basic relations in an
understandable format. In the second meeting the
mind map was divided into two, due to the received
feedback that separation of the personal wellness
and the external context would make the mind maps
more understandable.
Based on the performed analyses and the mind
maps we started to elaborate the model into a more
formal representation. We used a modification of the
entity relationship (ER) notation to represent the
necessary concepts, properties and relations. The
model did not follow strictly the ER-modeling
notation because the purpose was to create a model
which would be easy to understand and to modify by
citizens who are not modeling specialists. The
models were then discussed internally with the
project team (4 persons) and based on the feedback
we were able to make some modifications, to reduce
redundancy and the gap in the abstraction levels
between the concepts. The fourth small group
discussion on the models was organized in our
health informatics postgraduate student seminar
where the models were presented and discussed and
the participants (5 persons) were asked to give
feedback and their views on personal wellness.
3 RESULTS
3.1 Literature and Contextual Analyses
In the literature, there exist several wellness
definitions and they vary depending on the context.
Often wellness is thought to be a balanced state of a
healthy body, mind and spirit which creates a
harmonious feeling of complete wellness (Myers
and Sweeney, 2004; Larson, 1999; Oguz-Duran and
Tezer, 2009; Mackey, 2009; Soomlek and
Benedicenti, 2010; Kirsten et al., 2010; Kiefer,
2008). Most wellness models support health
CONTEXTUAL ANALYSIS AND MODELING OF PERSONAL WELLNESS
203

promotion, prevention, and progress towards better
functioning (Larson, 1999; Conrad, 1994; Sterling et
al., 2010). Thus, wellness is seen as a high level
concept integrating multiple domains (Schuster et
al., 2004; Sterling et al., 2010; Kirsten et al., 2010;
Kiefer, 2008). The concept wellness contains
individuals’ functioning as a whole and it
acknowledges lifestyle, behavior, culture, beliefs,
experiences and other issues affecting general life
satisfaction (Oguz-Duran and Tezer, 2009; Mackey,
2009; Soomlek and Benedicenti, 2010; Sterling et
al., 2010; Kiefer, 2008; Ahtinen et al., 2008).
Wellness is described as optimal physical,
psychological and social wellbeing (Els and De La
Rey, 2006; Larson, 1999; Soomlek and Benedicenti,
2010) and it focuses on an individual and on her
specific needs and it may vary depending on the
individual’s age or living culture. Wellness covers
means for changing lifestyles, adopting healthier
behavior, and combining morality and health.
Morality is seen in wellness actions when pursuing
good life one should make decisions between good
and bad actions for their health (Conrad, 1994).
Sweeney and Witmer (1991) developed the
Wheel of Wellness model. Based on existing
theories and research they identified factors
influencing healthy living, quality of life, and
longevity (Sweeney and Witmer, 1991). Myers and
Sweeney (2004) elaborated the model further to a
new one - the Indivisible Self which consists of five
factors and sub-factors:
– The Essential Self: spirituality, self-care, gender
identity, and cultural identity,
– The Social Self; friendship and love,
– The Coping Self; realistic beliefs, stress
management, self-worth, and leisure,
– The Creative Self; thinking, emotions, control,
positive humor, and work,
– The Physical Self; exercise and nutrition (Myers
and Sweeney, 2004).
This model has contextual factors which affect an
individual’s wellness and behavior. These are local
(family, neighborhood and community), institutional
(education, religion, government and
business/industry), global (politics, culture, global
events, environment, media and community), and
chronometrical (perpetual, positive and purposeful)
contexts. Contextual factors are important when
trying to understand human behavior (Myers and
Sweeney, 2004; Myers and Sweeney, 2008).
Saylor (2004) has developed the Circle of Health
model which defines health as optimal functioning,
well-being, and quality of life. The model is divided
into two sides. The light side focusing on activity
and performance consists of energy, strength,
fitness, stamina, happiness, enjoyment, satisfaction,
growth and development, occupational and/or social
role, and performance. The dark side is about
renewal and recovery including rest, relaxation,
peacefulness, nourishment, social support, sense of
purpose and meaning, balance, adaption, and
resiliency. This model tries to combine balance,
harmony, mind-body integration with more
traditional western ideas such as physical, mental,
spiritual, social, and role functioning (Saylor, 2004).
Kirsten et al. (2009) have developed an eco-
systemic approach to health, well-being and
wellness. It is based on two assumptions; Humans
are complete persons with some distinguishable
attributes which cannot be separated; and health,
well-being and wellness should be contemplated
multi-dimensionally and multidisciplinary. This
approach consists of three elements and two outside
contexts. The three elements describing the
functioning of a person are biological, psychological
and spiritual. The outside contexts affecting wellness
are ecological context describing living and non-
living physical environments, and metaphysical
context focusing on symbolic abstract environment.
The eco-systemic approach is a holistic and lifelong
view where people, their health and contexts are
distinguishable but inseparable (Kirsten et al., 2009).
All the four examined models acknowledge the
holistic idea of health and wellness. They created a
good basis for our contextual analysis because they
all had a multidimensional view on wellness. Also
they all emphasized both internal and external
contexts and the relations between them: An
exception is Saylor’s (2004) the Circle of Health
which focuses more on body-mind integration with
balance and harmony and inner actions. Important in
these models is the balance between different
aspects of health, wellness and external contexts so
all of them are much wider than the traditional
concept of health. However, all these models had
some deficiencies. They remain general; we needed
more detailed analysis on the concepts, the
properties and the relations. The models are also
high level descriptions with limited conceptual
analysis and they are presented in quite informal
way. The models are created for different purposes
with the focus more on assessment of wellness.
Our analyses result in that personal wellness
seems to be a combination of physical, emotional,
mental, intellectual, social, behavioral, occupational
and spiritual factors which are affected by the
environment and the external contexts. The concept
of personal wellness is highly dynamic and heavily
dependent on the context and cultural background.
KEOD 2011 - International Conference on Knowledge Engineering and Ontology Development
204
People may have different views and emphasis on
personal wellness and it may evolve during lifetime
(Ahtinen et al., 2008). Finally, we concluded some
common characteristics of wellness:
– Wellness is a holistic, multidimensional and
multidisciplinary view on health and wellbeing,
– Wellness is a much wider concept than
traditional view on health defined by healthcare;
it acknowledges also environmental, emotional,
intellectual, occupational, social and spiritual
aspects of wellbeing.
– Wellness focuses on complete health and
wellbeing, prevention and proactive services,
– Wellness is a dynamic and context dependent
concept,
– Wellness is heavily affected by internal and
external contexts and it may change over time.
3.2 Focus Group Work
Aforementioned models were introduced to the
focus groups as a background material. Our analyses
results were presented for the focus groups as two
mind maps, the first one focusing on the personal
wellness, things that are dependent on the person
herself and can be affected, controlled, influenced,
or managed by the person herself, and the second
one focusing on the environment or the external
contexts which affect personal wellness.
In the focus groups we elaborated further the
mind maps and started to model the domain of
personal wellness. We focused on the concepts and
their categorization because they were used as a
basis for the list of concepts related to personal
wellness. These concepts were analyzed and revised
to reduce redundancy and the gap between
abstraction levels, and make them more
understandable. As a result we were able to
conclude a high level view on personal wellness.
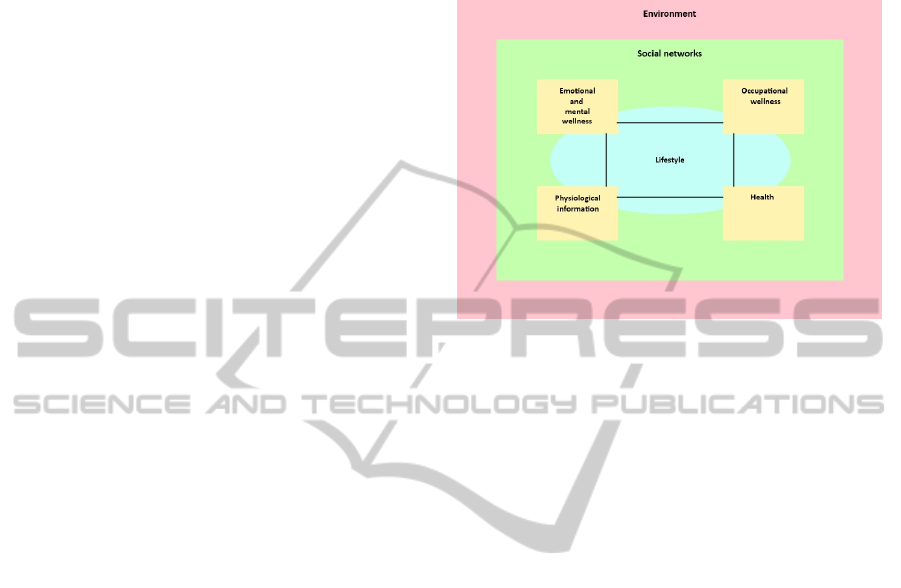
Our contextual view on the personal wellness
(Figure 1) consists of five main concepts which are
lifestyle, emotional and mental wellness,
occupational wellness, physiological information,
and health. All the concepts are interconnected and
they create a holistic view on personal wellness.
These five main concepts are surrounded by two
external contexts, social networks and the
environment, which heavily influence personal
wellness. So, finally our view is based on the seven
main components which interact together creating a
complete and holistic view of personal wellness. The
analyses and the empirical feedback formed the
basis when we started to categorize the concepts into
our view. We concluded the seven main components
that create a high-level information model of the
personal wellness (Figure 2.).
Figure 1: A contextual view on personal wellness.
4 DISCUSSION
Wellness is a research topic in many different
scientific areas e.g. in medicine, public health, social
work, mental health, health management and
economics, and nursing (Mackey, 2009). The
concept wellness is complex and multidimensional.
Wellness is personal but dependent on the context
and the cultural background. People may define and
emphasize personal wellness differently (Ahtinen et
al., 2008). With the analyses we were able to define
the internal and the external contexts and list some
of the main concepts of personal wellness. Also the
multidimensional and multidisciplinary nature of
wellness became very clear. It was important to start
analyzing from a high-level because it enabled us to
understand the scope and boundaries of the domain
before the empirical research and the modeling.
The focus groups were a good method to approach
the domain of personal wellness. With limited
amount of participants we could approach the huge
and complex domain in an organized manner and
keep the discussions on track. However, the focus
group work had some limitations. The group
consisted of quite homogenous participants who
were all quite young, healthy and educated persons
so our model might lack the needed multi-
perspective view. In the further empirical research
we need to include more heterogeneous participants
CONTEXTUAL ANALYSIS AND MODELING OF PERSONAL WELLNESS
205
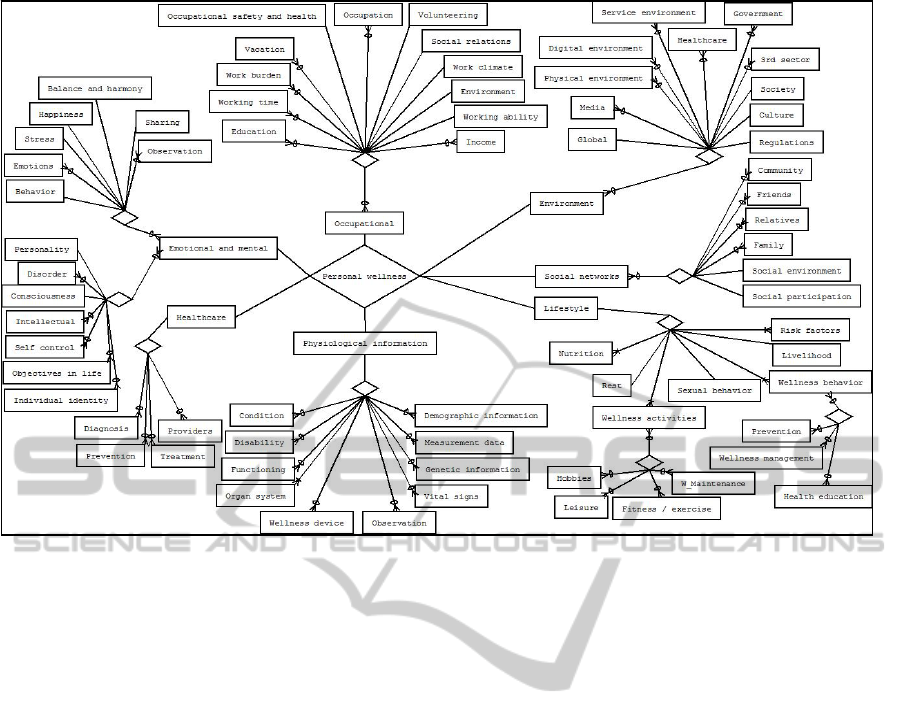
Figure 2: A high-level model of personal wellness.
to ensure that the model will acknowledge different
needs and perspectives. We need people from
different age groups, with different backgrounds and
with different health statuses. The two mind maps
developed with the focus groups described at a high-
level how wellness can be conceptualized and what
kinds of contexts are related to it. The mind maps
showed how complex the concept is and how it
covers more than just being healthy or free of
diseases. Although the mind maps had their
deficiencies we were able to utilize them with the
analyses and start creating a high-level model of the
personal wellness domain.
Our model divides the domain into seven main
components. We have already categorized many of
the related concepts, but the model is still quite
informal. We need to analyze further and in more
detail the different relations inside components and
how cross-border concepts affect each other. The
domain of personal wellness is challenging to model
because it is dynamic and multidimensional and very
context-dependent, it varies a lot between
individuals and cultures. Our results will shed some
light over the context of personal wellness and we
can see what kinds of concepts exist and how they
can be categorized and attributed.
In our research we have started to analyze the
context of personal wellness with informal models
because they can be understood by people without
modeling experience, though the concepts are quite
abstract and the domain is complex. From these
models we can find the core characteristics and
scope of the personal wellness and we can proceed
with our research into more formal modeling. The
results of this phase enable us to do more empirical
research with more participants in order to define the
concepts and the relationships in more formal and
detailed way. The goal is to integrate heterogeneous
data in the ubiquitous wellness environment and to
give us information how shared use of wellness
information affects citizens’ wellness management
and how citizens can control and manage the use of
their information (Nykänen et al., 2009).
The final objective of this research is to develop
a context aware personal wellness ontology which
takes into account the different contextual aspects of
wellness information and also the privacy,
confidentiality and security aspects. We need to
model these as part of the ontology because most
information is personal, private and confidential, and
their processing is regulated by the legislation. The
contextual aspects of all information entities need to
be covered in the ontology because wellness concept
is related to a multi-user and multi-system
environment with heterogeneous data sources. When
we include the privacy and the security aspects in
the ontology we can ensure that citizens and other
actors can dynamically control processing and
disclosure of their information. An essential part of
our further work is the validation and evaluation of
KEOD 2011 - International Conference on Knowledge Engineering and Ontology Development
206

the developed models and the resulting ontology.
We need to compare our results with the recent
research results and to perform empirical evaluation
with new participants in real life situations.
ACKNOWLEDGEMENTS
We acknowledge the funding of this Trusted eHealth
and eWelfare Space (THEWS) research project by
the Finnish Academy of Sciences in the MOTIVE
Research Programme during years 2009-2012.
REFERENCES
Ahtinen A., Mattila E., Vaataner A., Hynninen L.,
Salminen J., Koskinen E. and Laine K. (2009). User
Experiences of Mobile Wellness Applications in
Health Promotion User Study of Wellness Diary,
Mobile Coach and Self Relax. 3rd Int Conference on
Pervasive Computing Technologies for Healthcare.
Ahtinen A., Ramiah S., Blom J. And Isomursu M. (2008).
Design of mobile wellness applications: identifying
cross-cultural factors. OZCHI '08: Designing for
Habitus and Habitat.
Blobel B., González C., Oemig F., Lopéz D., Nykänen P.
and Ruotsalainen P. (2010). The role of architecture
and ontology for interoperability. Stud Health Technol
Inform., 155, 33-39
Conrad P. (1994). Wellness as Virtue: Morality and the
Pursuit of Health. Culture, Medicine and Psychiatry
18, p.385-401.
Els D. A. and De La Rey R. P. (2006). Developing a
Holistic Wellness Model. SA Journal of Human
Resource Management, 4 (2), 46-56.
Grinter R. E., Siek K. A. and Grimes A. (2010). Is
Wellness Informatics a Field of Human-Centered
Health Informatics? Interactions 17, 1, 76-79.
Kickbusch I. and Payne L. (2003). Twenty-first century
health promotion: the public health revolution meets
the wellness revolution. Health Promot Int 18,4: 275-8.
Kiefer R. A. (2008). An Integrative Review of the Concept
of Well-Being. Holist Nurs Pract. 2008 Sep-Oct;
22(5):244-52.
Kirsten T. G. J. C., van der Walt H. J.L. and Viljoen C. T.
(2009). Health, well-being and wellness: An
anthropological eco-systemic approach. Health SA
Gesondheid 14, 1, 1-7.
Koop CE, Mosher R, Kun L, Geiling J, Grigg E, Long S,
Macedonia C, Merrell R, Satava R, Rosen J (2008).
Future delivery of health care: Cybercare. IEEE Eng
Med Biol Mag. Nov-Dec;27(6):29-38.
Larson J. S. (1999). The Conceptualization of Health. Med
Care Res Rev 56, 123-136.
Mackey S. (2009). Towards an ontological theory of
wellness: a discussion of conceptual foundations and
implications for nursing. Nurs Philos.10 (2): 103-12.
Myers J. E. and Sweeney T. J. (2004). The Indivisible
Self: An Evidence-Based Model of Wellness. The
Journal of Individual Psychology, Vol. 60, 2.
Myers J. E. and Sweeney T. J. (2008). Wellness
Counseling: The Evidence Base for Practice. Journal
of Counseling and Development, 86, 482-493.
Nykänen P. (2008), Requirements for user friendly
personal ehealth information systems, In Studies in
Health Technology and Informatics, 137:367-72.
IOSPress.
Nykänen, P., Ruotsalainen P., Blobel B., Seppälä A.
(2009), Research on trusted personal health and
wellness information in ubiquitous health information
space. In: IFMBE Proceedings 25/12, 432-435.
Oguz-Duran N. and Tezer E. (2009). Wellness and Self-
esteem Among Turkish University Students. Int J Adv
Counselling, 31, 32–44.
Saylor C. (2004). The Circle of Health: A Health
Definition Model. J Holist Nurs, 22, 2, 97-115.
Schuster T. L., Dobson M., Jauregui M. and Blanks R. H.
I. (2004). Wellness Lifestyles I: A Theoretical
Framework Linking Wellness, Health Lifestyles, and
Complementary and Alternative Medicine. J Altern
Complement Med, Vol. 10, 2, 349–356.
Soomlek C. and Benedicenti L. (2010). Operational
Wellness Model: A Wellness Model Designed for an
Agent-Based Wellness Visualization System. The
Second International Conference on eHealth,
Telemedicine, and Social Medicine, eTELEMED.
Sterling E. W., von Esenwein S.A., Tucker S., Fricks L.
and Druss B. G. (2010). Integrating Wellness,
Recovery, and Self-management for Mental Health
Consumers. Community Ment Health J, 46:130–138.
Sweeney T. and Witmer J. M. (1991). Beyond social
interest: Striving toward optimum health and wellness.
Individual Psychology 47, 527-540.
Varshney U (2007), Pervasive Healthcare and Wireless
Health Monitoring. Mobile Netw Appl, 12:113-127.
CONTEXTUAL ANALYSIS AND MODELING OF PERSONAL WELLNESS
207
