TOOL FOR THE EVALUATION OF INNOVATIVE THERAPIES
Multi-agent based System
Anastasiya Shtiliyanova, Fabien Feschet
ISIT, Clermont Universit
´
e, 28 Place Henri Dunant, Clermont-Ferrand, France
Pascal Pommier
Centre L
´
eon-B
´
erard, D
´
epartement de Radioth
´
erapie, Lyon, France
Keywords:
Innovative therapies, Modeling, Evaluation, Multi-agent systems.
Abstract:
The paper contains the main lines of the modeling of a prototype for both medical and economical evaluation of
radiotherapy centers using innovative therapies. We consider uncertainties according to patients and hospital
complexes participating in the study. The corresponding part of the tool is called recruitment model. It
evaluates a theoretical number of patients interested in treatments of one center, using spatialization into a
context of competition. Moreover we developed a scheduling model, described briefly here and two shortly
presented economical models in charge of the evaluation of the average price per treatment and the comparison
between different radiotherapy strategies. We present preliminary results of the recruitment model.
1 INTRODUCTION
1.1 Context and Objectives
Innovative therapies used by centers involve un-
certainties according to the installation of facili-
ties and/or the expected therapeutic gain, after the
treatment (as hadrontherapy, stereotaxy, cyberknife).
Medical benefits results are often unknown, and pa-
tients are hostile to choose between a new therapy and
a well known treatment, thus it is a hard decision to
equip a complex, using only economical methods.
We model a generic progressive prototype evalu-
ating the position of a center from both medical and
economical point of view. To proceed we first evalu-
ate a theoretical number of patients interested in these
therapies, then its medical position regarding compe-
tition and medical politics fixed in advance. A recruit-
ment model is in charge of the theoretical number of
patients. It uses a suitable scheduling model to plan
the internal organization of the hospital, giving us the
possibility to have a good response for the demand of
a patient. The general prototype consist of two eco-
nomical models, one evaluating the price per treat-
ment of a therapy in a hospital, and another one used
to compare different strategies of treatment between
them and with the cost reimbursed by the health insur-
ance of a country. Moreover we include the cost per
year gained after a treatment according to a strategy of
treatment. The economical part of the prototype is not
described here. The tool supports the development of
innovative therapies and medical structures.
1.2 Modeling Method
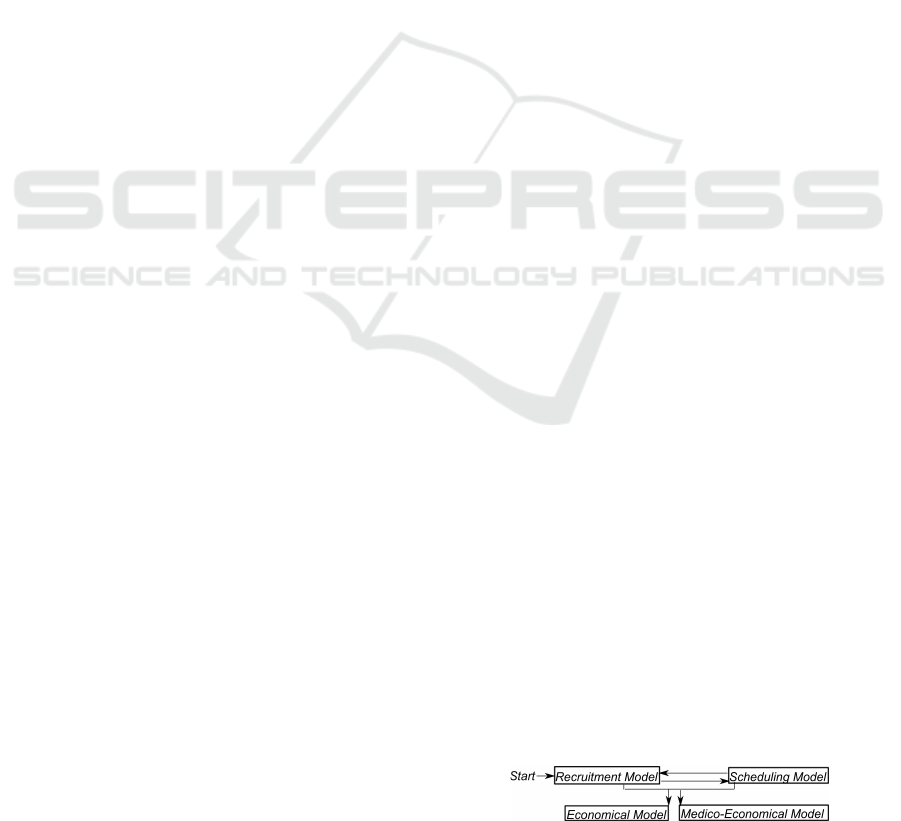
The tool is composed by the four independant models,
thanks to links between them they could be used al-
together (Fig. 1). We implemented them in a generic
way using the multi-agent theory (L.R.Coutinho et al.,
2005) and techniques such as (J.Ferber et al., 2004;
J.F.H
¨
ubner et al., ; Wagner, 2003), to describe the
global system, the interactions and organizational in-
formation system. This provides us a flexible organi-
zation (Nicholas, 2000).
Figure 1: Interaction between mains models.
Let us explain the execution of the global schema:
1. The recruitment model(RM) generates pa-
tients and spreads them out to suitable centers. Items
are located into the geography, thus the distance be-
tween them is known. The RM calculates a theoretical
number of recruited patients per complex. One time
step is equal to one week, according to the common
148
Shtiliyanova A., Feschet F. and Pommier P..
TOOL FOR THE EVALUATION OF INNOVATIVE THERAPIES - Multi-agent based System.
DOI: 10.5220/0003598901480154
In Proceedings of 1st International Conference on Simulation and Modeling Methodologies, Technologies and Applications (SIMULTECH-2011), pages
148-154
ISBN: 978-989-8425-78-2
Copyright
c
2011 SCITEPRESS (Science and Technology Publications, Lda.)
hospital organization.
2. The RM uses the scheduling model (SM) which
gives the response of acceptance or not for the current
patient, according to all constraints (functioning, ca-
pacity, medical politics). The two models are corre-
lated, and the last one could be replaced easily.
3. The use of the economical model (EM) is pos-
sible iff the evaluated center knows the number of re-
cruited patients by disease. It is estimated by the RM
model or done directly by the user. This model com-
putes the cost per treatment using the Activity based
costing method (ABC, 2011; I.Durand-Zaleski, 2005;
K.Kesteloot et al., 2000). We modeled, with medical
experts, the description of a treatment composed by
two phases (preparation and irradiation), each one is
presented by activities included in.
4. The medico-economical model estimates a
price per strategy, using a price per method of treat-
ment (protocol) included in one strategy. One strategy
is composed by multiple protocols describing the path
followed by the patient during his treatment. The user
could use the EM to get a price per treatment or give
an estimation by himself. In addition we compare it
with the cost corresponding to the French Health In-
surance System.
The global representation of the system is close
to the Information Systems As Agents (Hayes-Roth,
1995). Each model could be associated to an institu-
tional agent (Wagner, 2003), thus the communication
between agents is done by the transfer of information
or messages (Genesereth and P.Ketchpel, 1994).
The four main parts are designed as separate
agents, implemented in JAVA. They are acting in a
common environment, represented by a knowledge
dictionary and constructed especially for the tool.
This dictionary embraces all definitions for different
domains (geography, medicine, epidemiology, econ-
omy). We built up the ontology, the kernel of all
links between the four models, using the XML, XSD
properties, to control the quality of the required infor-
mation. The collective interpretation allows common
discussions and interactions. In addition the global
brute space controls the dictionary (J.Ferber et al.,
2009). Moreover the Social level, the knowledge,
is a part of the Structural Specification of the tool
(J.F.H
¨
ubner et al., 2002).
In the rest we present the recruitment model, rules
used to built it up and sub-processes developed in col-
laboration with medical experts. The elaboration pro-
cess is: a response with feasible results is needed for
every situation. We used the medical knowledge to
construct basic rules, which are represented like a n
node tree. A node is a rule and edges are possible ac-
tions to undertake, regarding the constraints. When
the complete tree is constructed, and not resolved
situations exist, we use the main rules again. The
process is repeated until all situations are resolved.
This mechanism belongs to the Cased-Based Rea-
soning methodology (A.Aamodt and E.Plaza, 1994;
S.Onta
˜
non and E.Plaza, 2008). The process of col-
lecting all required data for the prototype is complex,
thus a simpler versions of some hypothesis exist.
2 THE GENERATOR OF
PATIENTS
The generation of patients is a process lead by the RM
during every time step. It depends on the simulated
geography and indications (deseases), and makes the
link with the process of research of centers. It as an
agent, composed by multiple mechanisms, described
in the two following subsections.
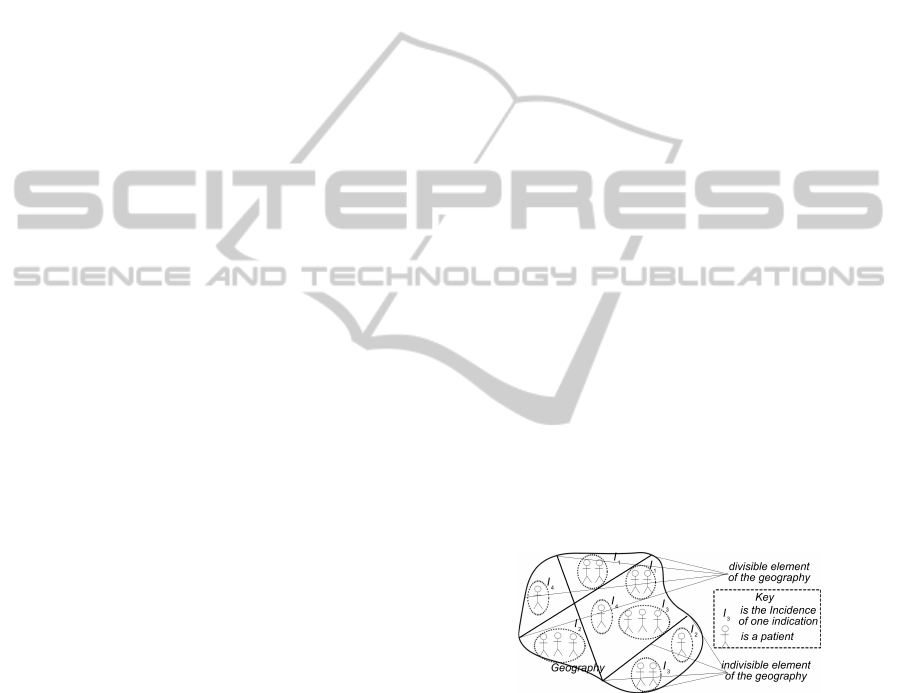
2.1 Geographic Position
To represent the epidemiology data the geography is
composed by different level of details.
Definition: Geography is an hierarchical structure,
composed by items. Items are the smallest non partitionable
elements (Fig. 2).
Every geographic element is referenced by an in-
dication. Epidemiological data couples with well
known statistical laws permits us to generate patients
according to an indication and an item.Thus generated
patients know their geographic position.
Geography
Figure 2: Elements of the geography and Incidences. We
subdivide the geography into indivisible zones, which are
as small as possible.One element of the geography refers to
several indications.
Definition: Incidence is the number of patients ac-
cording to one geographic element (Fig. 2). Incidences
compose the generated population for every time step.
2.2 The Disease Description of a Patient
The patient is described by a couple of [indica-
tion/protocol](IP). The protocol is the description of
the treatment according to technical constraints and
the planning of all sessions. As multiple protocols
TOOL FOR THE EVALUATION OF INNOVATIVE THERAPIES - Multi-agent based System
149

could be coupled with one indication, the chances
for the patient to find one treatment are larger. We
suggest a method to classify them in a specific order,
which facilitates the patient to find a center.
Definition: Priority group The couple IP is char-
acterized by a priority group, combination of the medical
benefit and the proof of the innovative therapy.
The priority group defines a mutable order for
treatments. The patient initially starts the research of
centers with its best priority group.
We suggest a final date for patient, obliging him
to find a center for a treatment before. It allows the
patient to ask centers for a treatment multiple times if
he is not accepted immediately. We introduce in this
way the multi-demand of the patient to centers. So
the final date for the treatment depends on the genera-
tor, which acts at the beginning of every time step. Its
discussions with the recruitment model create the pa-
tients in an environment of competition of radiother-
apy centers. This is an institutional agent operating
with biological agents.
3 THE PROCESS OF RESEARCH
OF CENTERS
The process of research of centers is based on tech-
nical requirements of the disease of the patient, his
general healthy state, his preferences to the existing
offer and geographical position of centers.
3.1 Description of the Center
The choice of the patient is influenced by possible
treatments, available facilities in centers, their geo-
graphic position and their medical politics.
1. The Mechanism of Medical Politics
Definition: Medical Politics represents preferences
of a center to the accepted indications. When it exists, it
gives priority of some treatments and/or eliminates others,
composed by several rules being a part of the planning.
Definition: Reserved Time represents reserved slots
in the hospital planning for a number of patients described,
by special characteristics as an indication and a protocol.
We suggest some rules for medical politics, de-
fined as independent structures and not essential for
the functioning of the center, as well as the existence
of the mechanism of medical politics.
- A Reserved Time for a Couple of IP. The center
constitutes a group of couples, composed by reserved
slots for IP treatments. This way the center gives pri-
ority to treatments with a better therapeutic gain.
- A List of Priorities, with reserved slots for one
or multiple priority groups. The last two rules could
introduce a conflict situation. If the priority group and
the couple of the same IP have reserved time, the med-
ical knowledge gives priority to the rule of the couple.
- limit the Usage of Particles such as Carbone, for
hadrontherapy centers. We estimate the annual use of
the particle and control it to not exceed a fixed limit.
2. The Scheduling Model
The scheduling model is a simple model, which plans
treatments and calculates the probability of accep-
tance of one patient according to its time of waiting.
We estimate the probability of acceptance with a mo-
bile mean computed for each IP accepted in a center.
A response is then given to the patient.
We constructed the SM in order to be able to test
the RM. The number of treated patients is maximized
regarding medical politics. We used linear program-
ming in 0, 1 to implement it. Constraints are not listed
here, but we illustrate the use of the model on the Fig.
3. The SM is used whenever the recruitment model
needs to have a response for one patient. It also plans
treatments for patients already in the waiting queue
and when it is not possible, the patient stays in the
waiting queue considering his preferences. The SM is
used for planning treatments for each room and dur-
ing the whole simulation, we use the RLE encoding
(RLE, 2010). It matches each day with the planning
of a room. When the scheduling model doesn’t find
a place for one patient, not corresponding to medical
politics, he is rejected directly and he has to search
for another center. As depicted on Fig. 3 there are
some rules to use during the discussion between the
SM and the agent of the center. We can identify them
in the same way as it has been done in (Wagner, 2003;
Taveter and Wagner, 2001).
Planing of the Centr
e
updates
Waiting queue
scheduling model
according to
the capacity of
the centre
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
Day
1
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
Day
N
Day
2
time
rooms
external pool of patients
patients with
treatment
patients staying
in the waiting
queue
rejected
patients
1
3
2
4
5
Figure 3: Interaction between the SM and the RM. We make
updates during the planning of treatments, in consequence
coming patients are evaluated and accepted or rejected.
3. The Waiting Queue
The waiting queue is a consequence of the mechanism
of medical politics. When a patient being a part from
medical politics arrives with a demand, and no place
is available for him, than if he could ”wait” according
to his final date of treatment, he goes in an waiting
queue if he agrees. The situation of this patient is
evaluated at every time step (Fig. 4). Moreover the
entry of new patients could force the exit of a patient.
A special way of ordering is applied to the waiting
SIMULTECH 2011 - 1st International Conference on Simulation and Modeling Methodologies, Technologies and
Applications
150
time
0
Begining of
the simulation
process
birth
searching
for a center
evaluation of the acceptance in the waiting queue
by the center at each time step
going out of
the waiting queue
probability of
treatment 55%
probability of
treatment 40%
probability of
treatment 10%
entering in a
waiting queue
time
0
entering in a
waiting queue
evaluation of the acceptance in the waiting queue
by the center at each time step
treatment
probability of
treatment 55%
probability of
treatment 70%
probability of
treatment 100%
birth
searching
for a center
Begining of
the simulation
process
Figure 4: Evaluation of the state of the patient in an waiting
queue, rejection or successful issue.
queue, considering the entry date and the priority
group of the patient. The center keeps unchanged the
medical politics and the priority of patients, which
are always planned in the slots of reserved time.
The waiting queue implies waiting possibilities for
a patient. When a center does not consider medical
politics, the waiting queue does not exist and the
patient will not wait for a response.
4. Choice of Patients by the Center
We suggest a mechanism organizing demands of pa-
tients. For every time step of the simulation the mech-
anism groups demands for the same center. Thus the
center receives a group of patients and applies medi-
cal politics. The possible responses are:
- How many patients could be taken for an im-
mediate treatment. Patients evaluated to be probably
placed in the planning are part of medical politics.
When there are places available after the setting of
those patients, the other patients are set up.
- Number of patients directed to the waiting
queue.
- Number of rejected patients, when they are not
a part of medical politics and there is no place in the
planning for them.
The response by the center is a result of the interac-
tion of the agents of medical politics, the SM and the
RM. They are using the common knowledge and ac-
cording to the environment they discuss on the possi-
ble actions to undertake. The full description of the
center is a part of the mind of the center reflection the
decisions taken during discussions with other agents
in the system.
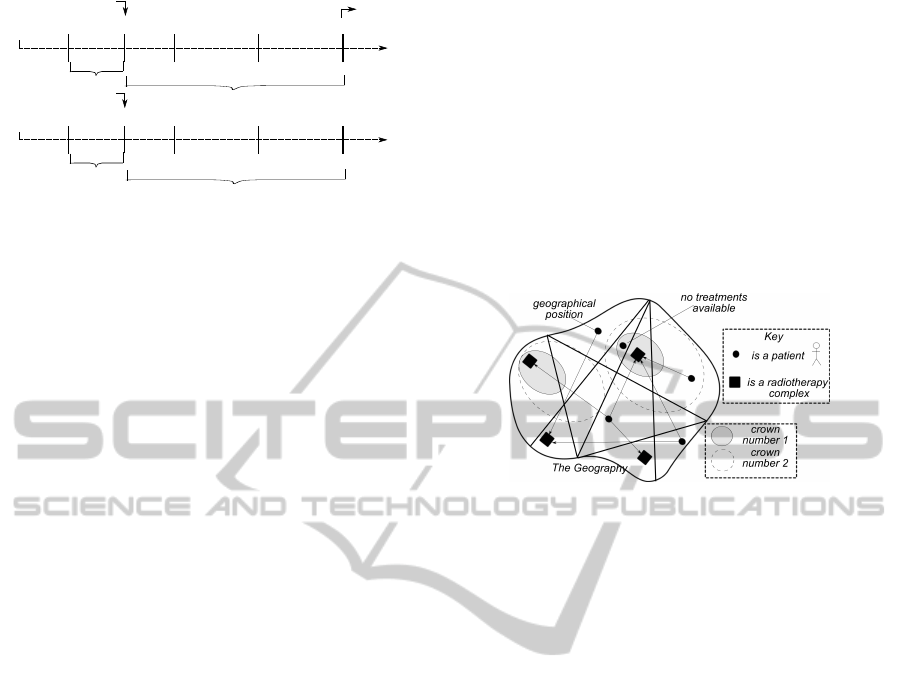
3.2 Characterize the Distance and the
Attractivity
As the geographic distance is an important parameter,
we define crowns of influence over each center repre-
senting the hesitation of the patient.
Definition: Crown of Influence (Zone) is composed
of one or multiple geographic elements. Over the center one
can find multiple crowns. The influence is smaller when the
crown is distant from the center.
In consequence when the patient is in the first
crown the center is more attractive, than if he is in an-
other crown (Fig. 5). The patient prefers centers situ-
ated nearly, thus we introduce a list of center around
him, ordered according to the geographic distance.
This model of crowns is mutable.
We mentioned the healthy state of the patient, in
consequence the medical benefit of the treatment de-
pends on. This medical parameter is part of a mecha-
nism called attractivity.
Key
is a patient
Figure 5: Spatialization for patients and center.
Definition: Attractivity is a combination between the
level of proof the treatment and the priority group of the
couple IP attributed to a patient.
We use the attractivity coefficient as a test if a pa-
tient wants to go to one center capable to treat him.
The result of the use of the geographic distance in the
attractivity, is a list obtained by a patient for all cen-
ters around him and capable to treat him. The mech-
anism of the attractivity is a part of the process of re-
search of centers, which is the leading agent of the
RM. All links for this process are connected with the
global environment of competition (Fig. 5).
3.3 The Patient and his Actions
We use the laws of Poisson and Gauss from the Epi-
demiological data to generate patients with a couple
of IP attributed to every one. The patient changes
his states during the simulation. He appears in the
beginning of one time step and starts searching of a
radiotherapy centers. When he founds one, he could
go in for a treatment, using the attractivity coefficient.
In some cases the patient does not find a hospital
complex, because he does not suit to the medical
politics included in the study and/or there is no avail-
able place. For well known techniques the patient
is treated out of the system, thus we evaluate only
the participation of new and innovative techniques
in the therapy center. The next figure 6 resumes the
set of states of the patient during the simulation,
related to the RM and the process of search of centers.
TOOL FOR THE EVALUATION OF INNOVATIVE THERAPIES - Multi-agent based System
151

Wait
Acceptance
treatment
time
Birth
Placed
treated out
of the system
Questioning
query
change or get a
new priority group
Figure 6: States of the patient: genesis, searching process,
waiting queue, acceptance of a treatment and the modifica-
tion of the priority group.
1. The order of Couples Describing the Disease
and the Treatment, The Choice of Lower Priority
Group
One indication is coupled to more than one protocol,
thus the patient has more chances to find a treatment.
The research of centers starts with his best couple IP.
All the couples are ordered according to their priority
group, describing a different ways of treatment. We
model the behaviour of the patient as a multiple de-
mands to all centers corresponding to the treatments
(protocols), of the given priority group. When this sit-
uation appears the patient evaluates the responses of
each center and send them back a response. The eval-
uation is based on the date of treatment done by the
center, the distance and the attractivity. When the pa-
tient is accepted by one center and he accepts to go in,
the other centers with a positive responses are alerted
by a mechanism, lead by the RM.
When the patient does not find a center capable to
treat him, he could degrade the current priority group,
taking the next available in his list. If a lower priority
group does not exist, then he has to search with the
current one, or he has to choose to take a well known
treatment and to be treated out of our system.
To model the degradation of the priority group,
we use a decision parameter based on a probability
law, combination of the number of weeks available
for waiting and the priority group. An example of the
graph of this curve is shown on the Fig. 7. In the
example there are 51 time steps period and 6 priority
groups.
In consequence the probability law is used by the
agent of the patient as a measure to estimate his need
to change his priority group and search for new treat-
ments. Less time available implies a faster choice of
lower priority group.
2. The Waiting State, Waiting Queue and Priority
Groups
The waiting state of the patient corresponds to an
awaiting queue. This is possible when the patient is
scouring for center and he is a part of medical poli-
tics of one center. If the designed center does not find
Figure 7: Curve of the probability function used by the pa-
tient to estimate the degradation of his priority group.
enough place for a treatment, then the patient goes au-
tomatically in a waiting queue. When multiple centers
are available for the patient, and he is a part from their
medical politics, then he goes in the waiting queues
of all centers. The first complex that finds a place
for a treatment is referred for the patient. When this
situation appears the other centers are informed by a
message that they have to liberate the place.
The evaluation of the place of the patient at every
time step is a process described in the previous sec-
tion for the center. When the center evaluates that the
patient has no chances to be treated before his limit
date, the patient is forced to quit the waiting queue. In
addition when the patient has available time to wait,
he could stay in the waiting queue of the hospital for
several weeks. When he waits too long time, he could
decided to exit it. This mechanism makes a link be-
tween the waiting time of the patient and its priority
group. When the patient is in a waiting queue, he
could choose to stay in and start to search centers for
a less advantageous treatment. This action degrades
his priority group but gives him more chances for a
treatment (Fig. 7). A patient in an queue, is described
by a passive state, i.e. he doesn’t change its priority
group. At each time step his need to pass from the
passive state to a searching state is evaluated using
the probability law. Thus the agent uses a rule, which
validation implies the change of the state. When he
passes in an active state, i.e. keeps its current place in
the queue, he can try to find centers with a new lower
priority group ( Fig. 8).
Waiting state and the
decision of the patient
Figure 8: The rule for changing the state of the patient.
The patient is a biological agent (Wagner, 2003))
acting into the RM with his beliefs and goal. His men-
tal components (Shoham, 1993) force him to discuss
and interact with other agents present in the global
system. The environment creates the resources and
the conditions for resolving the situations that ap-
SIMULTECH 2011 - 1st International Conference on Simulation and Modeling Methodologies, Technologies and
Applications
152
pears. According to the context the mind of the pa-
tient decides for the best action to do (J.Ferber, 1999;
Dignum, 2009).
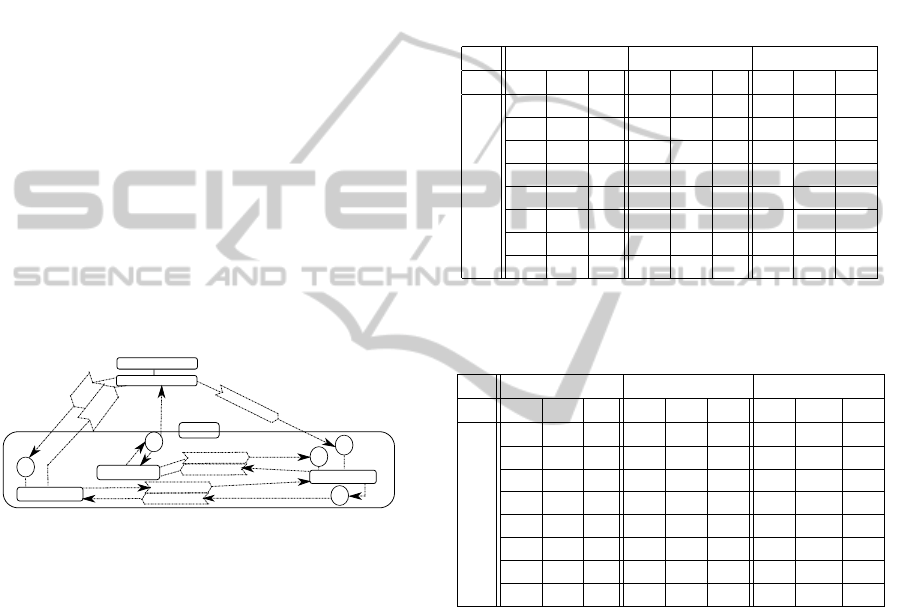
4 THE GLOBAL PROCESS, FIRST
RESULTS AND CONCLUSIONS
The global process of the recruitment model is an in-
stitutional agent, he guides all discussions (R.Searle,
1995). The rules are illustrated on the Fig. 9. We use
the schema introduced by (Wagner, 2003). The algo-
rithm modeled for the RM is:
- Initialization and preparation of the environment.
- Generation of patients. The patient is described
by four elements: geographic element, indication,
protocol and priority group.
- Creation of a list of centers, for every patient, ca-
pable to accept him and according to the geographic
distance and the attractivity.
- Updates for the waiting list of all centers.
- The medical politics are activated for centers.
- Choice by the patient from the available centers.
- The SM plans treatments of accepted patients.
Center
Medical Politics
R
3
Scheduling Model
requestPlace
confirmPlace
R
4
asking
Patients
responding
Center
Waiting Queue
requestUpdates
R
1
confirmUpdates
selfUpdates
R
2
rejectedPatients
R
5
planPatients
Generator of patients
Population of patients
Figure 9: Rules according to the general institutional pro-
cess of the recruitment model.
The first results obtained by the prototype use data
from the three French radiotherapy centers: CPO (C),
NICE (N) and ETOILE (E), with corresponding ca-
pacities 489920 hours, and tree treatment rooms, for
C and E, and 16554 and one treatment room for N.
The geography included in the study is the territory of
France, divided into 23 geographic elements. There
are 24 indications and 22 protocols with average du-
ration for the whole treatment spread out over 10 ses-
sions. The couples IP are organized into 8 priority
groups. We use both, the recruitment and the schedul-
ing model for one year simulation time. Our results,
based on a week with 5 days of working time, show
that when there is more time before the start of the
treatment, the recruitment is more important. Details
are shown in the next tables. We present results re-
garding the full capacity and according to every pri-
ority group, being a part of medical politics of the
centers. The results present different situations of re-
cruitment with 0
w
, 3
w
and 20
w
weeks of delay before
the treatment. The tables are also ordered according
to the possible number of patients recruited for the
first priority group. When the limit of recruitment of
patients for the first priority group is more important,
the recruitment increase. CPO and ETOILE increase
the number of treated patients for different values of
accepted capacity of the first priority group. We sug-
gest that medical politics have to be planed carefully,
in order to have a well structured recruitment.
Table 1: Treated patients by centers for one year. The first
priority group is 12% of the global planning for C and E.
0
w
3
w
20
w
PG C E N C E N C E N
1 30 1 84 35 10 97 28 11 105
2 26 19 - 24 12 - 26 23 -
3 - - - - - - - - -
4 23 33 - 63 115 - 125 113 -
5 11 23 - 90 132 - 0 165 -
6 - - - - - - 70 - -
7 140 327 - 524 797 - 477 902 -
8 - - - 25 50 - 31 49 -
Table 2: Treated patients by centers for one year. The first
priority group is 42% of the planning for C and E.
0
w
3
w
20
w
PG C E N C E N C E N
1 50 43 95 49 42 105 47 34 117
2 42 46 - 42 47 - 49 61 -
3 20 - - 18 - - 27 - -
4 24 76 - 63 123 - 127 138 -
5 12 22 - 87 153 - 97 160 -
6 - - - - - - - - -
7 152 368 - 607 917 - 522 1151 -
8 - - - 22 41 - 27 51 -
1. Conclusion
We use concepts from multi-agent systems for the
construction of a reusable and independent tool pre-
sented in this paper. The different models used for
it are presented as separate agents, thus they are
reusable and could be replaced. The link between
them is done by the ontology presented in the global
environment. The dictionary is related to multiple
fields such as medicine, economy or informatics. All
input data respect the structure of the ontology and
results were validated by medical experts.
The recruitment model, the main part of the pro-
totype, takes into account the situation of competition
between radiotherapy centers and the spatialization
of centers and patients in the geography. With our
model it is possible to evaluate the right geographic
location of a treatment center in order to optimize the
recruitment. We show preliminary results obtained
TOOL FOR THE EVALUATION OF INNOVATIVE THERAPIES - Multi-agent based System
153

by the collaboration of the recruitment model and the
scheduling model. In future works we plan to replace
the existing scheduling model with a complex one,
including definitions of staff and taking into account
critical resources.
Compare to the actual economical methods we
evaluate the efficiency of a center using its potential
recruitment. Our prototype could be used as a deci-
sion making tool for new innovative facilities, thus al-
lowing to test different scenarios with respect to staff
or treatment capacity as well as medical politics.
REFERENCES
(2010). RLE, http://en.wikipedia.org/Run-length encoding.
(2011). Activity based costing.
http://en.wikipedia.org/wiki/Activity-based costing.
A.Aamodt and E.Plaza (1994). Case-Based Reasoning:
Foundational Issues, Methodological Variations, and
System Approaches. AI Communications, 7:39–59.
Dignum, V., editor (2009). Multi-agent Systems: Semantics
and Dynamics of Organizational Models. IGI.
Genesereth, M. R. and P.Ketchpel, S. (1994). Software
agents.Communication of the ACM, 37(7):48–53.
Hayes-Roth, B. (1995). An architecture for Adaptive Intel-
ligent Systems. Artificial Intelligence, 72:329–365.
I.Durand-Zaleski (2005). Economic evaluation of radio-
therapy: methods and results. Cancer/Radiotherapy,
pages 449–451.
J.Ferber (1999). An Introduction to Distributed Artificial
Intelligence. Addison Wesley.
J.Ferber, O.Gutknecht, and M.Fabien (2004). From Agents
to Organisations: an Organizational View of Multi-
agent Systems. Agent Oriented Software Engineering
(AOSEIV), (LNCS 2935):214–230.
J.Ferber, T.Stratulat, and J.Trainer (2009). Towards an in-
tegral approach of organizations in mutlti-agent sys-
tems: the MASQ approach.
J.F.H
¨
ubner, J.S.Sichman, and O.Boissier. S-moise+: A
middleware for developing organised multi-agent sys-
tems. International Workshop on Organizaions in
Multi-agent Systems: From Organizations to Organi-
zation Oriented Programming, pages 107–120.
J.F.H
¨
ubner, J.S.Sichman, and O.Boissier (2002). A Model
For the Structural, Functional, and Deontic Specifica-
tion of Organizations in Multiagent Systems.
K.Kesteloot, Y.Lievens, and E.Schueren (2000). Improved
management of radiotherapy departments through ac-
curate cost data. Radiotherapy and Oncology, pages
251–262.
L.R.Coutinho, J.S.Sichman, and O.Boissier (2005). Model-
ing Organiszation in MAS: A Comparison of Models.
First Workshop on Software Engineering for Agent
Oriented Systems.
Nicholas, R. (2000). On agent-based software engineering.
Artificial Intelligence, pages 277–296.
R.Searle, J. (1995). The Construction of Social Reality.
Shoham, Y. (1993). Agent Oriented Programming. Artifi-
cial Intelligence, 60:51–92.
S.Onta
˜
non and E.Plaza (2008). Learning Information Ex-
change, and Joint-Deliberation through Argumenta-
tion in Multi-agent Systems. OTM Workshops, (LNCS
5333):150–159.
Taveter, K. and Wagner, G. (2001). Agent-oriented enter-
prise modeling based on business rules. In Proceed-
ings of the 20th International Conference on Concep-
tual Modeling: Conceptual Modeling, number 2224
in Lecture Notes In Computer Science, pages 527–
540. Springer Publishing London.
Wagner, G. (2003). The agent-object-relationship meta-
model: towards a unified view of state and behavior.
Information Systems, 28(5):475–504.
SIMULTECH 2011 - 1st International Conference on Simulation and Modeling Methodologies, Technologies and
Applications
154
