
An Ontology-driven Proposal for
Semantic Interaction among Heterogeneous
Health Information Systems
Idoia Berges, Jes´us Berm´udez and Arantza Illarramendi
University of the Basque Country, Paseo Manuel de Lardizabal, 1
20018 Donostia-San Sebasti´an, Spain
Abstract. The adoption of Electronic Health Records (EHRs) has brought mul-
tiple advantages to the healthcare area. However, the goal of achieving semantic
interoperability of EHR information between heterogeneous Health Information
Systems has not been accomplished yet. In such scenario, the purpose of this pa-
per is twofold: On the one hand, the presentation of our ontology-based approach
to the problem of EHR interoperability (restricted to the case of medical observa-
tions), which goes one step further with respect to other approaches for the same
goal, and on the other hand, the presentation of two additional features that com-
plement our approach: path mappings for transforming individuals that represent
EHR information and rules for medical knowledge sharing.
1 Introduction
In 2009 the European Community presented a longer-term research and deployment
roadmap that provides the key steps for achieving semantic interoperability in the area
of healthcare[1]. The motivation for that is that nowadays the idea of one person re-
ceiving health assistance from the same medical institution throughout all his life is no
longer realistic. Thus, medical institutions must be prepared to receive patients from
other regions or countries without the quality of service being affected. The incorpora-
tion some years ago of Electronic Health Records to the institutions may be seen as the
first step towards the goal, since, apart from local advantages over manual records such
as avoiding legibility problems due to poor handwriting which may lead to misunder-
standings, they favour a fast exchange of clinical data between different organizations.
However,the fact that most institutions have developedtheir health information systems
in an autonomous way has resulted in a proliferation of heterogeneous health informa-
tion systems, each one with its own proprietary models for representing and storing
EHR information, which difficults the task of interoperating with each other.
In many areas, the adoption of knowledge representation standards stands out as the
most usual approach to solve interoperability problems. This happens also in the health-
care area, where some standards such as openEHR
1
, CEN-13606
2
and HL7-CDA
3
are
1
www.openehr.org
2
www.en13606.org
3
www.hl7.org
Berges I., Bermúdez J. and Illarramendi A..
An Ontology-driven Proposal for Semantic Interaction among Heterogeneous Health Information Systems.
DOI: 10.5220/0003350500440053
In Proceedings of the International Workshop on Semantic Interoperability (IWSI-2011), pages 44-53
ISBN: 978-989-8425-43-0
Copyright
c
2011 SCITEPRESS (Science and Technology Publications, Lda.)

under development for this purpose. All those three follow a dual model-based method-
ology for representing the information that may appear in an EHR: On the one hand, the
Reference Model is a stable model which defines the basic structures for representing
EHR information (such as List, Table, etc.). On the other hand, the Archetype Model
defines specific knowledge elements (such as Respiration Rate) by using and constrain-
ing the elements of the Reference Model. Although the idea of using a standard may
seem suitable for the goal, we think that interoperability does not mean to have a unique
representation but a semantically acknowledgeable equivalent one. This would relieve
medical institutions from being forced to use one standard in the representation of their
knowledge and moreover, since several standards are being developed for the same pur-
pose, the interoperability problem will remain unsolved unless these standards merge
into a single one.
In this paper we present a proposal to move towards the notion of full semantic
interoperability of EHRs, which states that when one particular system receives some
EHR information from another institution, the received information can be seamlessly
integrated into its underlying repository because the differences in the language, in the
representation of the information and in the storing systems do not cause any misun-
derstanding[1]. Our solution is based on the use of semantic technologies, and more
precisely on OWL2[2] ontologies and corresponding reasoners.
In the area of EHRs semantic interoperability a certain number of related works can
be found at present. The works mentioned next also rely on semantic technologies that
facilitate semantic interoperation between heterogeneous information systems as op-
posed to other formats for interchanging data such as XML which do not deal with the
semantics of the exchanged data[3]. [4] provides a solution to achieve semantic inter-
operability between systems that have been developed under the HL7 reference model.
However, this proposal requires that the source system has some prior knowledge about
the target system and moreover, it does not tackle the communication between sys-
tems that use proprietary EHR specifications. In [5] ontology mappings are proposed
between pairs of archetype-based models. Finally, in [6] a model-driven engineering
approach that transforms archetypes of the CEN-13606 standard into OWL models is
presented.
The purpose of this paper is twofold: On the one hand, the presentation of our
ontology-based approach to the problem of EHR interoperability (restricted to the case
of medical observations) and on the other hand, the discussion of some features that
complement the current approach -which may be also relevant to other ontology-based
interoperability solutions. More specifically, we would like to stress two of them: first,
the usefulness of defining a new category of mappings between the elements of two
ontologies -called path mappings- which indicate some kind of relationship between
two property paths in the ontologies and facilitate the transmission of the information
about individuals between two ontologies. Secondly, the convenience of incorporating
SWRL[7] rules to the ontologies to define and share medical knowledge among institu-
tions.
The rest of the paper is divided as follows: first, a general overview of our ontology-
based approach for semantic interoperability of EHRs is presented in section 2. Section
45
3 tackles the complementary features pinpointed above. Finally conclusions are dis-
cussed in section 4.
2 Overview of the Framework
In general, an EHR includes clinical statements such as observations, laboratory tests,
diagnostic imaging reports, treatments, therapies, administered drugs and allergies. In
this paper we focus on the exchangeability of medical observation statements, which
are used to record all notionally objective observations of phenomena and patient-
reported phenomena, such as physical examinations, laboratory results or basic infor-
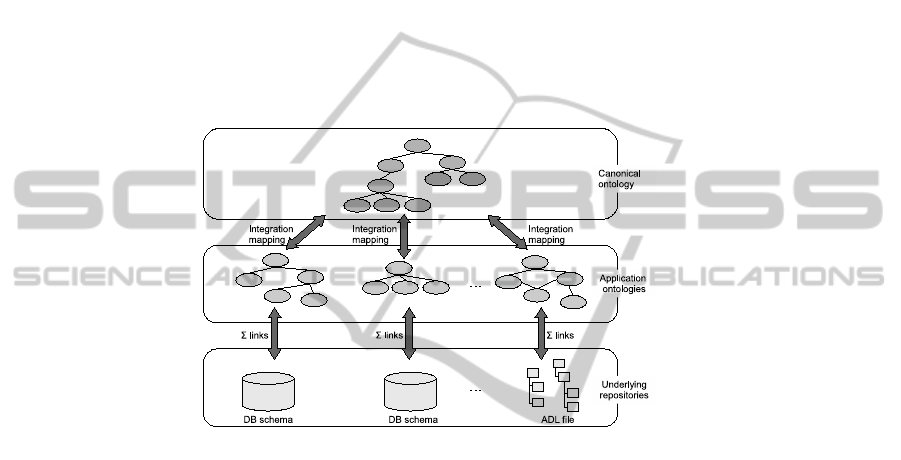
mation about the patient (weight, sex,...). In Fig.1 the architecture of our proposal is
shown.
Fig.1. Architecture of the solution.
This proposal is sustained in one of the approaches for interoperability among sys-
tems described in [8]: Using a canonical model to which the particular systems are
linked. More precisely, we deal with a Canonical ontology that represents medical ob-
servations in a canonical way, that is using a general representation that is independent
from the different conceptualizations of them that can exist. In that ontology we pro-
pose a subdivision of medical observations into two groups: simple observations and
composite observations. Simple observations have a single value and unit of measure-
ment. Additionally, we have also identified three properties that may be relevant at the
time of characterizing an observation: the protocol, which records information about
how the observation process was carried out, either by indicating a particular clinical
protocol (e.g. the Balke protocol for treadmill graded exercise testing) or the medical
device used for taking the measurement (e.g. a stethoscope); the anatomical site, to in-
dicate the specific body location in which the observation was taken; and the state of
the patient, which is intended to record the state of the subject of the observation during
the observation process. In order to represent the information about the protocol in a
controlled way, we advocate for using the terms of an ontology that comprises classes
from the Device and Procedure categories of SNOMED-CT[9]. Moreover, in order to
represent anatomical information, the terms of the Foundational Model of Anatomy
46

ontology[10] are suggested. Finally, we have developed one ontology for describing
information about the state of the patient, which contains 121 classes divided into 28
categories to represent states such as the level of exertion (low, medium, high intensity)
or the position of the patient (standing, sitting,...).
On the other hand, composite observations are composed of two or more observa-
tions, either simple or composite. They are intended to represent observations of phe-
nomena such as the Blood Pressure, which is composed of the systolic and diastolic
blood pressures. Below, we present some OWL2
4
axioms that represent the general
terms for representing medical observations
5
:
c:Observation ≡ c:Simple Obs ⊔ c:Comp Obs
c:Simple Obs ≡ =0 c:comp
c:Simple Obs ⊑ =1 c:value ⊓ ≤ 1 c:unit ⊓ ≤ 1 c:protocol.c:Protocol ⊓
∀c:state.c:State ⊓ =1 c:site.c:AnatomicalSite
c:Comp Obs ≡ ≥ 2 c:comp.c:Observation
Specific observations are described as specializations of these general terms.
Other main components of the proposal are Application ontologies, which repre-
sent the observations as they are understood in one particular health information sys-
tem. When such a system wants to join the framework, the following steps must be
followed: first its Application ontology has to be defined on top of its underlying data
repository. One module named Internal2OntoModule has been developed for that task.
In some cases the module will receive as input a database schema and after apply-
ing a set of rules founded on schema features (tables, keys, inclusion, exclusion and
functional dependencies, null values and semantic integrity constraints), it constructs
the corresponding ontology components (classes, properties, relations and restrictions).
More details about the nature of the rules are described in a previous paper of our re-
search group[12]. In other cases, the input will be an archetype description (e.g. of a
EHR standard) written in Archetype Description Language[13] which is transformed to
OWL. Moreover,this module is responsible for creating the Σ links (Fig.1) that regulate
the information flow between the underlying repositories and the Application ontology,
following the guidelines in [14]. Then, the particular system must import the above de-
scribed Canonical ontology and create the integration mapping that relates the terms of
its Application ontology with the terms in the Canonical ontology. A MappingModule
has been developed for this purpose.
Once a particular system A has joined the framework it is prepared to send infor-
mation about observations stored in its underlying repository to another system B in
the framework. Thanks to the Σ links between the underlying repository and the Ap-
plication ontology of system A, the information to be sent is converted into instances
(individuals) of the classes of that Application ontology. Then, all the implicit knowl-
edge (regarding the individuals) that can be inferred from the Applications layer is
made explicit with the help of a reasoner. At this point, the integration mapping that
4
For the sake of conciseness we use the Description Logic (DL)[11] representation of axioms.
5
Throughout the paper, the namespace ’c’ will be used for referring to terms in the Canonical
ontology, and namespaces ’a’ and ’b’ will be used for referring to the ontologies of some
specific systems A and B
47

has been defined between the Application ontology of system A and the Canonical on-
tology comes into play and as a reasoning result, the individuals are also classified as
instances of the concepts of the Canonical ontology. All the inferred knowledge about
the individuals is then sent to system B, which asserts it into its ontology. Since system
B has also imported the Canonical ontology, this is a straightforwardprocess. Moreover,
thanks to the integration mapping between the Application ontology of system B and
the Canonical ontology, the individuals are then recognized as instances of the specific
terms of system B. Finally, the Σ links between the Application ontology of system B
and its underlying repository allow to assert the knowledge into the latter. The whole
process described above is directed by a reasoner.
To sum up, the main features of the framework presented in this section are the
following:
– It is extensible to any model, either standard or proprietary.
– It is not based on peer-to-peer transformations but on the semantic acknowledge-
ment of one instance of a class in the source ontology as instance of another class
in the target ontology.
– The features of any specific system remain unknown to the other systems in the
framework. Acknowledging and using the Canonical ontology as a shared model is
enough.
– Reasoning plays a major role in several parts of the framework.
3 Additional Features for Complementing the Proposal
In this section two additional features that complement our approach will be discussed:
path mappings for transforming information about individuals between two ontologies
and rules for knowledge sharing. The usefulness of these features may be also relevant
to other ontology-based interoperability solutions. Prior to that, subsection 3.1 is in-
tended to present the definitions of the elements that will appear in the examples of the
following subsections.
3.1 Scenario for the Examples
The Revised Trauma Score (RTS)[15] is a physiological scoring system for predicting
death taking into account three measures: the Glasgow Coma Scale value, the Systolic
Blood Pressure and the Respirations Rate. Moreover, the Glasgow Coma Scale(GCS)
is a neurological scale that aims to give a reliable and objective way of recording the
conscious state of a patient[16]. It is calculated from the result of three tests: the eye,
motor and verbal responses.
Subset S
C
of the Canonical Ontology. It contains the definitions of the observations
Revised Trauma Score and Glasgow Coma Scale.
c:RTS ≡ c:Comp Obs ⊓ ∃c:comp.c:GCS ⊓ ∃c:comp.c:SysBP
⊓∃c:comp.c:RespRate
c:GCS ≡ c:Comp Obs ⊓ ∃c:comp.c:EyeR ⊓ ∃c:comp.c:VerbalR
⊓∃c:comp.c:MotorR
c:value ∈ owl:DatatypeProperty
48

Subset S
A
of the Application Ontology of a Specific System A. In this subset only
the observations related to the Revised Trauma Score are considered.
a:RTS ≡ ∃a:hasEyeResp.a:EyeResp
⊓∃a:hasMotorResp.a:MotorResp
⊓∃a:hasVerbalResp.a:VerbalResp
⊓∃a:hasSysBP.a:SysBP ⊓ ∃a:hasRespRate.a:RespRate
a:hasValue ∈ owl:DatatypeProperty
Notice the difference in the representation of the a:RTS class with regard to the c:RTS
in the Canonical ontology. While in the latter the class c:GCS is used in the definition,
in the former the five values that ultimately are necessary to calculate the RTS score are
indicated directly.
Subset S
B
of the Ontology of a Specific System B. In this subset only the observations
related to the Glasgow Coma Scale are considered.
b:GCS ≡ ⊓∃b:hasEyeResponse.b:EyeResponse
⊓∃b:hasVerbalResponse.b:VerbalResponse
⊓∃c:hasMotorResponse.c:MotorResponse
b:hasValue ∈ owl:DatatypeProperty
Integration Mappings.
6
Finally, let us imagine that the following integration mappings
have been established by the MappingModule:
I
AC
= hS
A
, S
C
,
{a:RTS ≡ c:RTS, a:EyeResp ≡ c:EyeR, a:RespRate ≡ c:RespRate, a:hasEyeResp ⊑ c:comp,
a:hasSysBP ⊑ c:comp, a:hasRespRate ⊑ c:comp, a:hasValue ≡ c:value}i
I
BC
= hS
B
, S
C
,
{b:GCS ≡ c:GCS, b:EyeResponse ≡ c:EyeR, b:hasEyeResponse ⊑ c:comp,
b:hasValue ≡ c:value}i
3.2 Path Mappings
As stated in the previous section, the MappingModule is in charge of creating the in-
tegration mapping between the Canonical Layer and the Applications Layer. Thanks
to this integration mapping instances that initially belong to the Application Layer can
be recognized as instances of the Canonical Layer (and viceversa). For example, if the
aforementioned integration mapping I
BC
is considered, given the triples
(b:indGCS rdf:type b:GCS) (b:indGCS b:hasEyeResponse b:indER)
(b:indER rdf:type b:EyeResponse) (b:indER b:hasValue 4)
the reasoner will infer the following statements, which classify all the information about
the individuals b:indGCS and b:indER in the Canonical layer:
6
For the sake of visual clarity, in this integration mapping we indicate only the axioms related
to the eye response component of the Glasgow Coma Scale. Please assume that the other two
components are treated accordingly.
49
(b:indGCS rdf:type c:GCS) (b:indGCS c:comp b:indER)
(b:indER rdf:type c:EyeR) (b:indER c:value 4)
This is a quite straightforward process since the representation of the concept GCS
is similar in both the Canonical ontology and the Application ontology of system B (i.e.
in both cases the class GCS is directly related to each of its three components via an
object property). The problem arises when the representation of the same concept in the
source and target ontology is more heterogeneous than just different names for classes
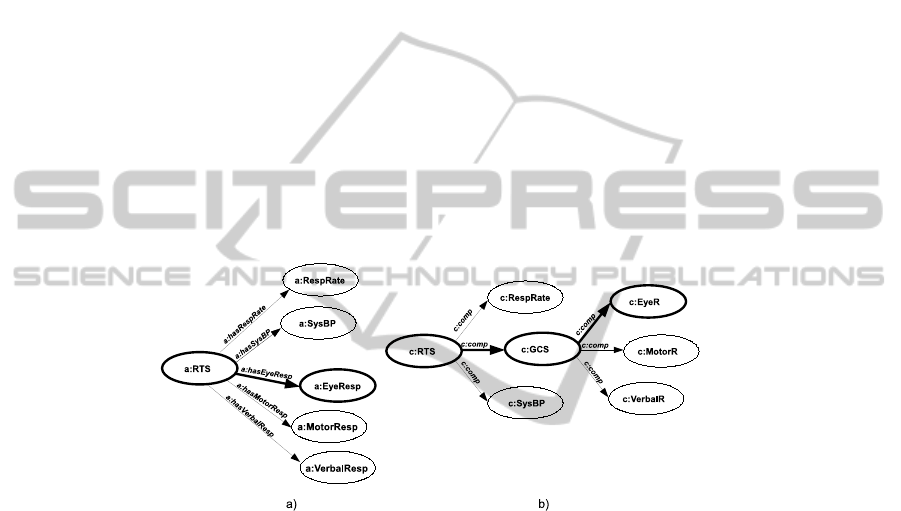
or properties. Let us compare the definitions of classes a:RTS and c:RTS in section
3.1. Looking at the description of a:RTS, it can be seen (Fig.2) that any individual
belonging to that class will be directly related to an individual of the class a:EyeResp
via the role a:hasEyeResp (assume the same intuition for the case of the motor and
verbal responses). However, in the case of the descriptions in the Canonical ontology, it
turns out that classes c:RTS and c:EyeR are not directly related, but indirectly: first
c:RTS is related to the class c:GCS via the role c:comp and then the class c:GCS is
related to the class c:EyeR again via the role c:comp. Then it could be stated that there
is a simple path between classes a:RTS and a:EyeResp (Fig.2a) and a composite path
between classes c:RTS and c:EyeR (Fig.2b).
Fig.2. Structurally different but semantically equivalent ontology paths.
Intuitively, those two paths could be regarded as equivalent, since their only dif-
ference is from the structural point of view caused by the heterogeneous origin of the
ontologies, not from a semantic point of view. Let us denote those equivalences with the
following statements where the expressions on both sides of the ≡
p
symbol represent a
path. Each expression begins with a class name that is followed by (one or more) pairs
propertyName[className]:
a:RTS.a:hasEyeResp[a:EyeResp] ≡
p
c:RTS.c:comp[c:GCS].c:comp[c:EyeR]
a:RTS.a:hasMotorResp[a:MotorResp] ≡
p
c:RTS.c:comp[c:GCS].c:comp[c:MotorR]
a:RTS.a:hasVerbalResp[a:VerbalResp] ≡
p
c:RTS.c:comp[c:GCS].c:comp[c:VerbalR]
For that reason, we have decided to incorporate a new kind of mappings to our
framework: the so called path mappings, which establish equivalence or subsumption
relations between two ontology paths. Path mappings are useful at the time of trans-
forming individuals from one ontology so that they meet the requirements of the target
50

ontology. The implementation of path mappings is done by using SWRL rules. For
example, the path mappings shown before would be implemented using the following
rule:
a:RTS(?r) ∧ c:RTS(?r) ∧ a:hasEyeResp(?r,?e) ∧ a:hasMotorResp(?r,?m)
∧ a:hasVerbalResp(?r,?v) ∧ swrlx:createOWLThing(?g,?r)
→ c:comp(?r,?g) ∧ c:GCS(?g) ∧ c:comp(?g,?e)∧ c:comp(?g,?m) ∧ c:comp(?g,?v)
Let us look at what happens when system A wants to send the following triples
about a RTS reading to another system
7
:
(a:indRTS rdf:type a:RTS) (a:indGCS a:hasEyeResp a:indER)
(a:indER rdf:type a:EyeResp) (a:indER a:hasValue 4)
Following our proposal, thanks to the integration mapping I
AC
in the first place
the individuals will be classified in the Canonical ontology. For example, individuals
a:indRTS and a:indER will be recognized as instances of the classes c:RTS and
c:EyeR respectively. In order to comply with the specification of the class c:RTS,
there should be an individual of the class c:GCS that acts as a connection between
individuals a:indRTS and a:indER. That individual is created by the SWRL rule
above, which fires as soon as a:indRTS is recognized as instance of the class c:RTS
(because the rest of the clauses in the body of the rule are also fulfilled).
3.3 Knowledge Rules
Up to know, we have presented a solution that allows the interoperability of data about
medical observationsbetween Health Information Systems. However we think that once
this framework is set up, its potential could be enhanced to solve a more ambitious
problem: the possibility of defining and sharing medical knowledge among those sys-
tems. It is widely known that EHRs hold great potential for clinical decision support,
for example by translating practice guidelines into automated reminders and actionable
recommendation[17] which can improve the quality and safety of healthcare as sub-
stantial evidence suggests[18]. Usually, medical experts are in charge of performing
those translation tasks and of incorporating them into their systems, without sharing
them outside their local context. However, it would be interesting to have the option
to spread that knowledge from one ontology to another. For example, widely accepted
knowledge directives could be integrated into the Canonical ontology, and due to the
mappings between the Canonical ontology and the Application ontologies, spread to
the diverse Application ontologies. This could incorporate valuable knowledge into the
systems without too much effort on their part. Accordingly, a specific system could
define knowledge directives in its Application ontology and spread them to the Canon-
ical ontology and in consequence to other Application ontologies, although in this case
some supervision should be carried out to avoid that one system infects other systems
with knowledge that is relevant locally but not necessarily relevant for other systems.
An appropriate way of modelling knowledge directives related to diagnoses and
treatment of illnesses is by using rules expressed in a declarative form, since they are
7
Accordingly for the remaining components of a:RTS.
51

suitable for obtaining conclusions from a set of data. More precisely, we have chosen
again SWRL as language for representing these rules. For example, one of the rules
that could be defined in the Canonical ontology is shown next. This rule is intended to
calculate the Glasgow Coma Scale value of a patient as the sum of the values of each
of the three components (Eye, motor and verbal response). The result is stored as the
value of the c:value property of the corresponding c:GCS reading.
c:GCS(?g) ∧ c:comp(?g,?e) ∧ c:EyeR(?e) ∧ c:value(?e,?ev) ∧ c:comp(?g,?m)
∧ c:MotorR(?m) ∧ c:value(?m,?mv) ∧ c:comp(?g,?v) ∧ c:VerbalR(?v) ∧ c:value(?v,?vv)
∧ swrlb:add(?emv,?ev,?mv) ∧ swrlb:add(?emvv,?emv,?vv) → c:value(?g,?emvv)
4 Conclusions
In the first part of this paper we have presented a framework which has the following
main features: First, it favors the notion of semantic interoperability among health in-
formation systems by using formal ontologies as canonical conceptual models, which
allow to focus on semantic aspects that are independent of the languages or technologies
used to describe EHRs. This reasoning-drivenapproach avoids the need of peer-to-peer
transformations and in addition, the features of any specific system remain unknown to
the other systems in the framework. Moreover, it favors the notion of extensibility to
different models, since any medical institution can create its own Application ontology
and relate it to the terms of the Canonical layer via an integration mapping. Finally it
facilitates this seamless adaptation by providing of one module that facilitates the task
of obtaining the definitions of the Application ontology from a particular underlying
system and another module that facilitates the task of linking definitions of the Appli-
cation ontology to definitions of the Canonical ontology. In the rest of the paper some
features that complement the proposal have been discussed: the usefulness of path map-
pings in the transformation of ontology individuals and the convenience of using rules
for knowledge representation and sharing.
Acknowledgements
This work is supported by the Spanish Ministry of Education and Science (TIN2007-
68091-C02-01) and the Basque Government (IT-427-07). The work of Idoia Berges is
supported by the Basque Government (Programa de Formaci´on de Investigadores del
Departamento de Educaci´on, Universidades e Investigaci´on).
References
1. Kalra, D., Lewalle, P., Rector, A., Rodrigues, J.M., Stroetmann, K.A., Surjan, G., Ustun, B.,
Virtanen, M., Zanstra, P.E.: Semantic Interoperability for Better Health and Safer Healthcare.
Technical report, European Commission (2009)
2. OWL2 Web Ontology Language (2009) http://www.w3.org/TR/owl2-overview/.
3. Hefflin, J., Hendler, J.: Semantic Interoperability on the Web. In: Proceedings of Extreme
Markup Languages 2000, Graphic Communications Association (2000) 111–120
52

4. Kilic, O., Dogac, A.: Achieving Clinical Statement Interoperability using R-MIM and
Archetype-based Semantic Transformations. IEEE Transactions on Information Technol-
ogy in Biomedicine, 13 (2009) 467–477
5. Bicer, V., Kilic, O., Dogac, A., Laleci, G.B.: Archetype-Based Semantic Interoperability
of Web Service Messages in the Health Care Domain. Int’l Journal on Semantic Web &
Information Systems 1 (2005) 1–22
6. Mart´ınez-Costa, C., Men´arguez-Tortosa, M., Valencia-Garc´ıa, R., Maldonado, J., Fern´andez-
Breis, J.T.: A Model-driven Approach for Representing Clinical Archetypes for Semantic
Web Environments. Journal of Biomedical Informatics 42 (2009) 150–164
7. Swrl (2009) Available at http://www.w3.org/Submission/SWRL/.
8. Kashyap, V., Sheth, A.P.: Semantic and schematic similarities between database objects: A
context based approach. The Very Large Databases Journal 5 (1996) 276–304
9. SNOMED (2009) Available at http://www.ihtsdo.org/snomed-ct/.
10. Rosse, C., Mejino, J.L.V.: A Reference Ontology for Biomedical Informatics: the Founda-
tional Model of Anatomy. Journal of Biomedical Informatics 36 (2003) 478–500
11. Baader, F., Calvanese, D., McGuinness, D., Nardi, D., Patel-Schneider, P., eds.: The De-
scription Logic Handbook. Theory, Implementation and Applications. Cambridge University
Press (2003)
12. Blanco, J.M., Illarramendi, A., Go˜ni, A.: Building a Federated Relational Database Sys-
tem: An Approach Using a Knowledge-Based System. International Journal on Cooperative
Information Systems 3 (1994) 415–456
13. The openEHR Foundation: Archetype Definition Language (2007)
14. Mena, E., Illarramendi, A., Kashyap, V., Sheth, A.: OBSERVER: An Approach for Query
Processing in Global Information Systems based on Interoperation across Pre-existing On-
tologies. International journal on Distributed And Parallel Databases 8 (2000) 223–272
15. Champion, H.R.: A Revision of the Trauma Score. The Journal of Trauma 29 (1989) 623–
629
16. Teasdale, G., Jennett, B.: Assessment of Coma and Impaired Consciousness. a Practical
Scale. Lancet 2 (1974) 81–84
17. Hoffman, L.: Implementing Electronic Medical Records. Communications of the ACM 52
(2009) 18–20
18. Kawamoto, K., Houlihan, C.A., Balas, E.A., Lobach, D.F.: Improving clinical practice using
clinical decision support systems: a systematic review of trials to identify features critical to
success. BMJ 330 (2005) 765–768
53
