
Output Matters! Adaptable Multimodal Output
for New Telerehabilitation Services for the Elderly
António Teixeira
1
, Carlos Pereira
1
, Miguel Oliveira e Silva
1
Joaquim Alvarelhão
2
, António Neves
1
and Osvaldo Pacheco
1
1
Dep. Electronics Telecommunications and Informatics, IEETA
University of Aveiro, 3810-193 Aveiro, Portugal
2
Health School, University of Aveiro, 3810-193 Aveiro, Portugal
Abstract. Technologies capable of being used by the older adults, with their
specificities, to provide new services in the areas of telehealth and Ambient
Assisted Living are needed. In this paper, we describe a new service, and its
first prototype implementation, in the area of elderly health support at home.
Special care was taken to improve the usability, adaptability to user and context
and inclusiveness capabilities of the output. The basis for intelligent adaptation
of the multimodal output – called AdaptO – is proposed and first versions of the
needed services and agents were created.
1 Introduction
The continued introduction of technology in the domestic environment is a reality.
Increasingly, the majority of the population sees technology as something natural and
very useful.
Within the older adults group - getting bigger and bigger by each year and
representing a significant percentage of the population at least in developed countries
- this technology can have a positive effect on their living conditions, particularly for
those staying at home, if these technologies for domestic environments are made
accessible and usable. One of the most common problems with elderly people is
mobility. The need to go to a Health facility (ex: clinic) to make a physiotherapy
session or to be monitored for an extended period are factors that have repercussions
in the daily life of these people and of their families.
With suitable natural interfaces and the possibilities offered by next generation
networks, the introduction of technological solutions can facilitate the daily life of the
elderly, fighting isolation and exclusion, increasing their pro-activity, work capacity
and autonomy. Examples of services are multimedia information access and exchange
of personal data; telehealth and automatic medication delivery; support of daily
activities and community, social and civic life; and automatic management of the
environment to improve both the quality of life and security.
Technologies usable by the older adults, with their specificities, to provide new
services in the areas of telehealth and Ambient Assisted Living (AAL) are needed. In
this paper, we present work in progress in such a new service, for telerehabilitation or
Teixeira A., Pereira C., Oliveira e Silva M., Alvarelhão J., Neves A. and Pacheco O..
Output Matters! Adaptable Multimodal Output for New Telerehabilitation Services for the Elderly .
DOI: 10.5220/0003308000230035
In Proceedings of the 1st International Living Usability Lab Workshop on AAL Latest Solutions, Trends and Applications (AAL-2011), pages 23-35
ISBN: 978-989-8425-39-3
Copyright
c
2011 SCITEPRESS (Science and Technology Publications, Lda.)

even telefitness.
This work is part of the Living Usability Lab for Next Generation Networks
project (www.livinglab.pt), LUL for short, a Portuguese industry-academia
collaborative R&D project, active in the field of live usability testing, focusing on the
development of technologies and services to support healthy, productive and active
citizens. The project adopts the principles of universal design and natural user
interfaces (speech, gesture) making use of the benefits of next generation networks
and distributed computing [1].
1.1 Telerehabilitation
Rehabilitation, Training and Assistive Technologies, have been one of the major
concepts in the elderly care sector [2]. From the many ways to define rehabilitation
we adopt the interesting definition used by AAL Forum 2010 Track R5
(Rehabilitation, Training, Assistive Technologies)[2]:
“You must again be the director of your own life! You must train and
rehearse to again be able to help yourself and gain independent living”.
As an example, a typical exercise program for frail elders in seated position [3]
includes four components: Warm-up, Aerobic training, resistance training and cool-
down. Warm-up includes exercises like postural awareness, breathing, joint range of
motion, stretching; Resistance training comprises Body-weight and resistance
exercises; Cool-down includes stretching and relaxation.
Telerehabilitation has some advantages [4]. Particularly relevant for the older
adults are: availability of therapists, rehabilitation at home, reduced therapist cost,
reduced isolation. The disadvantages, also according to [4], are: equipment cost,
network bandwidth, technical expertise, safety at home, sterilization for
redeployment, efficacy studies, psychological factors. The next generation networks
will certainly decrease the problems of network bandwidth; the technical expertise
can be addressed by easy-to-use interaction; costs will certainly drop as the number of
users increase. It is reasonable to expect that some older adults may exercise less
without direct therapist intervention, since they feel they get less attention than they
deserve. It is also reasonable to expect that others will accept perfectly less human
contact [4].
According to [5] “the one-to-one paradigm of therapy will also change, with one
therapist performing “multiplexed” telerehabilitation. This is expected to reduce
treatment costs while also increasing access to therapeutic care worldwide”. New
technologies can help provide therapy anywhere, anytime, addressing current
limitation due to location, lack of transportation or limited therapist availability [5].
[5] predicts that cloud computing will be extended to cloud rehabilitation, where the
library of disability-specific software simulations or games will reside on a third-party
“cloud”; the clinicians will log on to set up exercises programs, follow up progress,
insure compliance and monitor safety.
1.2 Vision and Hearing in Older Adults
Age-related eye problems are a major cause of vision loss or distortion in people over
24

40. The risk for developing serious visions problems increases, as you get older.
Presbycusis [6, 7] is age-related hearing loss. It becomes more common in people
as they get older. People with this kind of hearing loss may have a hard time hearing
what others say or may be unable to stand loud sounds. The decline is slow; it can
develop at different rates. The degree of hearing loss varies from person to person.
Another common complaint by older adults regarding hearing is their difficulty in
understanding rapid speech. Studies have demonstrated older adults' special
difficulty in encoding rapid speech due to age-related changes in peripheral and/or
central hearing abilities [8].
1.3 Multimodal Adaptive Interaction with the Elderly
According to [9] the current migration from WIMP interfaces towards multimodal
interaction has benefits for seniors. As an example, speech can accompany a text
signal in a warning message box. In this way different capabilities, expertise,
preferences or expectations of the seniors can be accommodated.
The diversity of environments, systems and user profiles leads to a
contextualisation of the interaction. Initially the interaction had to be adapted to a
given application and for a specific interaction context. Nowadays, the interaction has
to be adapted to different situations and to a context in constant evolution [10].
Environment and context of use can have high impact in an application or service
use. For example, when the user is not looking towards a monitor on whom textual
information is presented this can result in a critical failure. Examples of environment
relevant alterations are the increase of ambient noise level and the changes of
illumination. It is essential to determine these variations in context and adapt the
system interaction inputs and outputs accordingly.
Another factor often neglected is the user himself/herself. For example, in a
scenario in which the hearing ability of a user is reduced it makes sense to provide
output for other senses, such as vision, thus increasing the likelihood that system
messages are received and perceived by the user. Without the redundant or alternative
use of vision, the interaction between the application and the user has a strong
possibility of failure.
Efficient multimodal interfaces should be able to take into account the user
requirements and needs. This is particularly relevant for a group such as the older
adults, with some potential additional difficulties.
2 Objective: A New Generation of Remote Rehabilitation Services
for the Elderly
Combining the needs of the elderly to have professionally monitored exercises
without leaving their homes with other factors, such as the availability and costs of
qualified health professionals, a Telerehabilitation Service was considered as one of
the priority new services to develop and test in the scenario of our Living Usability
Lab. The service is based, but not equal, to the rehabilitation service proposed by
project Persona [11]. In very general terms, the service should allow supervised
25
remote exercise sessions at home or community centres, as a mean to maintaining
health and prevent illness. Table 1 presents essential information on the Service.
Table 1. Service description, based on the Persona Remote Rehabilitation Service [11].
Name LUL Telerehabilitation Service with Multimodal Interaction
Description
(What)
Remote and supervised exercise sessions at home or community centres, for
maintaining health and prevent illness. Sessions carried out concurrently at
several sites via networked multimodal applications.
It should be possible for the user to wear biosensors while doing the
exercises/rehabilitation. Eventual use of vibration or similar to give feedback
(ex: to indicate wrong/right execution of the exercise). A health professional
supervises everything from the training centre/hospital, including the
biosensors signals captured remotely and the (multiple) cameras images. The
system also includes mechanisms to request and process information regarding
effort level from the user.
End user People taking rehabilitation sessions at home and people wanting to do exercise
in case it is just training sessions.
Stackeholders
and Roles
(Who)
Health/Sport professionals (physiotherapists, gerontologists, etc) who
configures the sessions and directs them.
The training centre or other health services provider, which should install and
maintain the platform.
Technological
description
(How)
The main user interface is a large size computer monitor (acting as a large size
TV) combined with speakers and video cameras. In addition, it should be
possible to use a set of biosensors. Sensors gather the vital signals from the
patient and send them to the health professional.
Table 2. Analysis of our system according to AMITUDE properties.
Application Type Home rehabilitation system for elderly people. Physician supervision. Agent
based system with context-enabled functionalities.
Modalities Input, health professional: 2D analogue haptics pointing, 2D static
Portuguese typed text, Portuguese spoken conversation.
Output, health professional: Portuguese spoken conversation, Video
imaging, 2D static Portuguese typed text.
Input, elderly user: 2D static Portuguese typed text, Portuguese spoken
conversation, Video Streaming
Output, elderly user: 2D static Portuguese typed text, Portuguese spoken
conversation, 3D dynamic graphics describing exercises and involved
routines.
Interaction Two-way communication (deliberate). Computer-mediated human-human
communication.
User task, other
activity, domain
Task goal: execute a telerehabilitation session
Generic task: complete a session of rehabilitation exercises according to a
defined program, with direct supervision from a professional (ex: physician)
Domain: e-Health
Issues: Context-aware environment, customization
User (Personas) Elderly user. See the description of the Personas in next section.
Devices Input, elderly user: microphone and speech recognition, video camera,
biosensors, context-aware sensors.
Output, elderly user: loudspeaker and text-to-speech, large graphics display.
Input, health professional: microphone and speech recognition, keyboard,
mouse and touch-enabled graphics monitor.
Output, health professional: loudspeakers, graphical display.
26

3 Requirements
Because the user-centred development and usability are central to LUL project, the
method adopted involves user inputs from the requirements stage. The usability will
not be evaluated only at the end of the development process; a first prototype was
developed to integrate even in the requirements stage. To enable the creation of this
prototype as earlier as possible, a first draft version of requirements was obtained
based on the so-called imagination methods [12], particularly by using Personas and
the knowledge of specialists (namely the Gerontologists and Physicians that integrate
the project team). This requirements, summarized below, were obtained based on the
characteristics of the Personas and their goals and descriptions of usage scenarios (not
included due to space limitations), method inspired by the PSG (Persona + Scenario +
Goal) method of [13].
3.1 Personas
Three main Personas were considered essential for service definition and created with
the help of specialists. For the system user Persona, WHO ICF [14] classifications are
used (inside parenthesis).
Mrs Zulmira at age 70, retired secretary from a small company in a semi-rural area
has osteoarthritis (b7102) and hypertension (b4200). Despite her presbyopia (b2150)
and hearing problem (b2304), her family physician (e5800) makes the referral for a
community exercise program (d9201). Their relatives, who live near by, work full
time. The restriction in using public transportation (d4702) prevents her of attending
the exercise class (d9201).
Flávia Conceição, 32 years, is a Gerontologist specialized in adapted physical
activity. She started her career working with frail elders, developing activities and
exercise programs at private charities. She is familiar with the use of the web, such as
Microsoft Messenger and social networks.
Dra Filipa - Physician, specialized in rehabilitation, at a hospital, aged 55, married,
with some responsibilities in taking care of her parents (living in nearby). Professional
use of computer applications (such as email and word processors), but with not much
interest for computer use. She does not have a laptop or smartphone.
3.2 Goals
Personal Goals of the Elderly: to be able to perform fitness exercises or
rehabilitation exercises with health professionals monitoring – speciality dependent of
the exact objective - without the need to abandon their residence; to have faster access
to such services and at the most convenient times according to daily activities; use
this new health service in a attractive, simple and secure way.
Health Professionals Goals: to be able to extend there services outside the limits of
the traditional place they develop their activity; to be able to provide the services to a
larger number of persons, to persons that can not leave their homes easily and even to
rural areas / more isolated regions; to be able to cross borders to provide transnational
27
planning and monitoring of rehabilitation; to have the possibility to easily combine
their competences with other, possibly remote, to create an multidisciplinary
monitoring.
Health Institutions and the National Health System: to be able to sent people home
earlier from hospitals by assuring control over rehabilitation plan at home; to improve
the health of relevant groups of the population, reducing health problems and
increasing productivity.
3.3 Functional Requirements for the Service
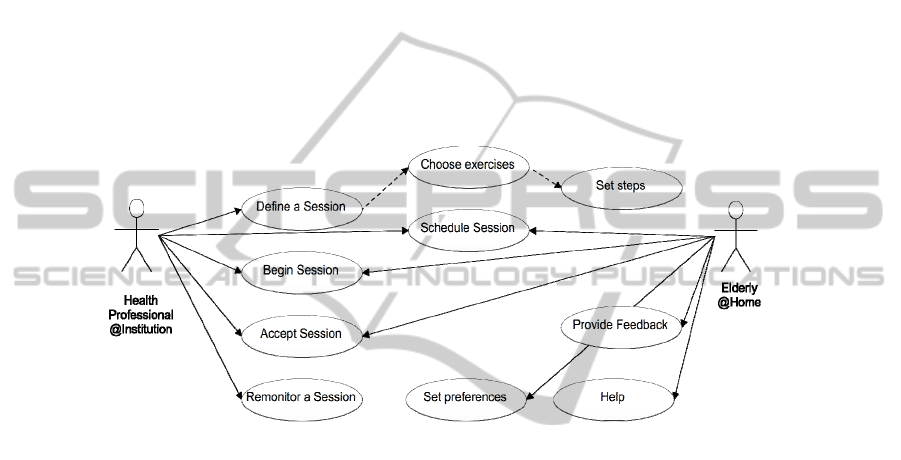
The diagram in Fig. 1 represents the first, simplified version, of the functional
requirements for the service, elaborated based on the scenario and goals already
presented.
Fig. 1. Main functionalities for the Service.
3.4 Non-functional Requirements
There are many non-functional requirements that can be applied to this service. We
will only present the ones considered most relevant:
1. Reliable communications with enough Bandwidth - In order for the prototype to
work and connect all participants, the system must be supported with enough
bandwidth;
2. System must be reliable - Given the type of operations being performed, it is
crucial that the system remains operational and stable; it is crucial for the system to
possess fault-tolerant capabilities in order to continue operating even in the event of a
failure.
3. Distributed and heterogeneous computing environment – to cover the
geographically distributed nature of the service and to avoid the need for specific
computing environments;
4. The system must be scalable and extensible - It must be ready to grow in the future
and to be capable of integrating new functionalities. The future inclusion of new input
and output modalities should be easy;
28

5. The system must log all system and users activities - This is crucial for the Living
Lab paradigm;
The system must be highly usable. This is without doubt the most important of all
non-functional requirements to us. All of the goals proposed should be easy for the
users (elderly and health professionals) to achieve; the user must be comfortable
interacting with the system; the system should be simple and natural to him. If it is
not, then probably the purpose of the system will eventually fail. This requirement is
further detailed below.
Human Computer Interaction (HCI) focused non-functional requirements given
the high interaction needed for our service:
1. The text interface should be readable at a distance, have large and clear text
capable , and adapting itself according to the user's distance;
2. Interaction with users must use simple words and sentences;
3. An highly adaptable and intelligent multimodal output system, able to adapt itself
to changing environment conditions (light, noise, distance, etc.) and to its users needs,
limitations and personal choices:
− Redundancy of modalities must be used in order to increase the chances of
message delivery;
− Output modalities with capabilities, based on the environment and user, to decide
to activate/deactivate themselves. Ex: there is no reason to keep active an Text-to-
Speech (TTS) output when the user is deaf;
− Use of several output modalities to make the system usable by speech and hearing
impaired persons;
− Output characteristics, such as the volume of the synthesized speech, must adjust
themselves according to the user and the environment (ex: distance to speakers, noise
level and users hearing acuity);
− Speech rate must be adapted to listener and listening conditions;
− Based on their preferences, allow users to be informed through their preferred
modality(ies).
4. Multi-touch input should be available on the health professional side in order to
allow him to easily access some information or quickly select a course of action.
4 A First Prototype
In order to introduce as early as possible the elderly in the development loop and
usability evaluation of the new service we opted to start by creating a minimally
functional prototype, capable of enabling the interaction between a health care
professional (in the hospital for example) and an elderly at home or institution. Use of
this prototype by seniors will provided the needed information for a first refinement
of the requirements.
Creation of a prototype for the service depends on: (1) the development of two
application with suitable Human Computer Interaction, one for the elderly at home,
other for the health professional planning, monitoring and evaluating the session; (2)
the necessary network connections and services (ex: to transmit video); (3) the
29
existence of the health professionals and elderly to provide and use the service. Here
we will only address the first.
The two applications use multimodal input and output, with particular emphasis in
the use of speech and text. The use of speech derives from its potential to be usable by
visually disabled people and to enable interaction hands free and at some distance
from the devices. This capability of receiving information and giving commands to a
computer at a couple of meters of the TV/computer display is essential when the aim
is making all body movement exercises.
4.1 Architecture and Services
The main characteristics of the first prototype's architecture is its SOA (Service
Oriented Architecture) approach, implemented with Jade [15], the decentralization
and autonomy of all its service agents, and its adaptability to changing environment
conditions (context) and user preferences and limitations.
The choice of using an agent based platform seemed one of the best available
options, because it is a mature and quite stable technology, able to provide us a
solution for a distributed heterogeneous system, supported on a standard
communication protocol (FIPA), which may simplify future integration of third party
services supporting new input and output devices.
Agents also provided us a versatile solution for the need of a decentralized,
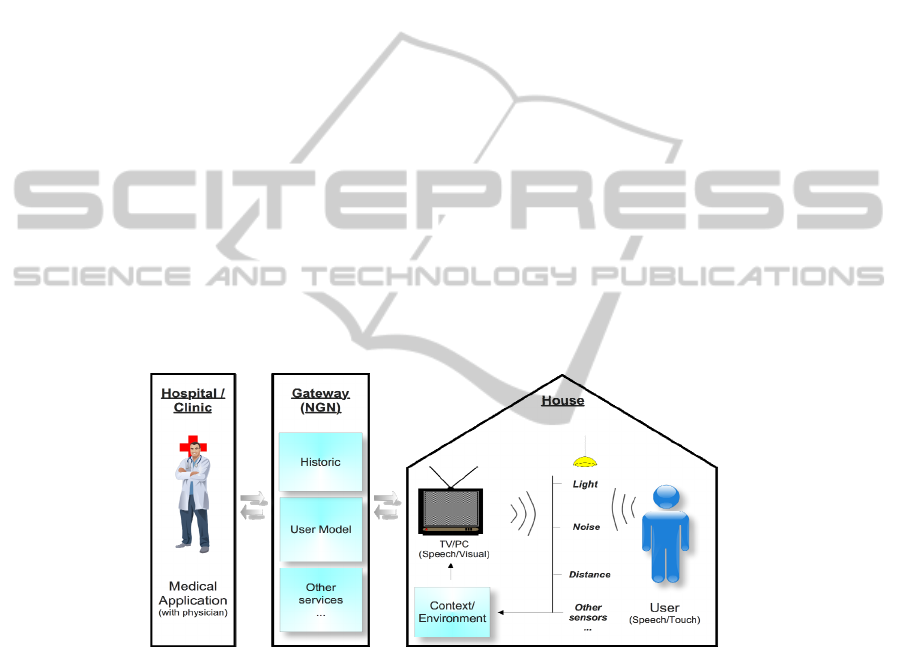
scalable, adaptable, and intelligent system. Fig. 2 presents a global view of the
prototype.
Fig. 2. General view of the service architecture.
To provide a solution to the adaptability of our applications to changing
environment conditions we have defined a context service. This service, implemented
as an agent, is responsible to register, in real-time, all the relevant environment
conditions such as noise, light, distance of the user to the output devices, etc.. The
information for this service comes from a set of specialized producer agents that, in
general, are connected, directly or indirectly, to sensors, such as microphones and
cameras.
A user model service is also provided, in order to register and fetch specific user
related capabilities and preferences. Examples of capabilities are vision and hearing
30

acuity and mobility capabilities. As preferences we can have, for example, the
personal preference for receiving information visually or for a specific color for text.
When considering possible approaches to incorporate the different input and
output devices we were faced with two basic choices. The first one was to make them
simple dummy devices responsible only for sending input information to the system
and to receive output messages already adapted to the context and user from it. This
approach has several serious problems, such as the need for a complex fission
coordination service very knowledgeable of all the available output devices, and able
to coordinate all the relevant context and user conditions in order to generate proper
outputs. Also, that approach would make it more difficult to scale and extend out
multimodal applications to new input and output devices.
To avoid these problems, it was decided to provide intelligent agent output
devices, able to adapt themselves to changing context and user conditions. To remove
from the context and user services the knowledge of all the available output and input
devices, those services are implemented as simple reactive information repositories in
which the device agents register themselves to be listeners of specific variables. For
instance, a speech output device may register itself in the user model service to
become aware of possible hearing or comprehension user problems, and register in
the context service to receive changes in the user distance. With such knowledge, this
device may change the volume of the sound, and the rate of the speech to maximize a
successful transmission of the messages required.
There are also two more important services (also implemented as agents): a logger
service able to register all the relevant history information for latter uses, such as for
the creation of user specific information for the user model. A coordination fission
service able to ensure the reliability of the application as a whole. This service would
be able to ensure fault tolerance, notifying the application when an output was not
transmitted (for example, due to the unavailability of proper output devices).
4.2 Implementation
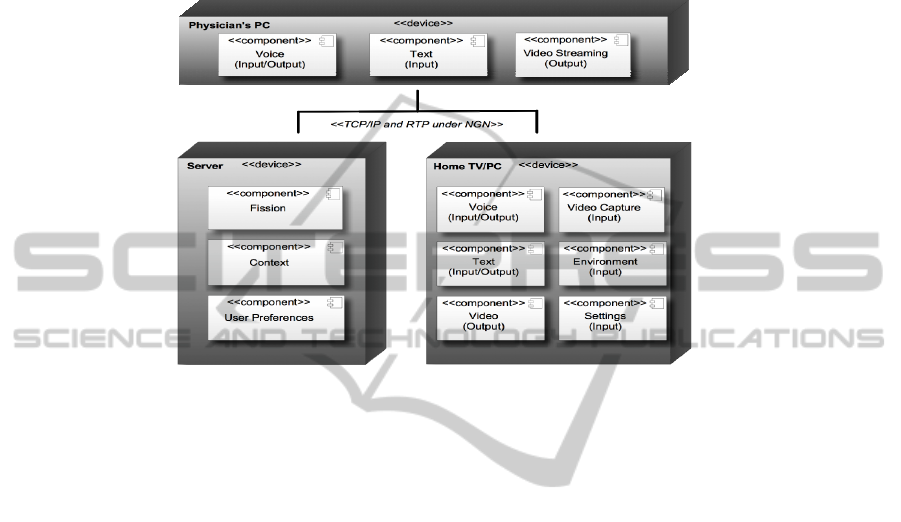
Our prototype implementation (Fig. 3) includes three main blocks, running in 3
different networked computers, resulting from the subdivision of the application at the
elderly side in two: one, in a more capable device (a server), including the more
performance demanding operations; the other (in the Home TV/ Personal PC)
responsible by interaction and the devices for environment monitoring.
Besides the main computing devices, the system includes input and output devices
such as microphones, speakers and video cameras, required for the interaction
between the users and the platform, and sensors to detect environment factors. In
order to facilitate interoperability, all communication processes are done using TCP
and RTP protocols over IP networks.
Agents (JADE) communicate with each other via FIPA messages. A FIPA
message normally includes a destination agent, a title, an attachment and a flag that
indicates the type of message. This last one became important to us because it allowed
us to filter the messages according to its type and process the response more easily.
In order to facilitate the search for agents, JADE provides a service-registration
index upon which the agents may inscribe themselves. This was very useful to us in
respect to output agents. If an agent perceives that it can resolve some types of output
31
messages (such as text), then he inscribes himself under the registry for that given
action. This allows other agents that may need to output some message to instantly
search and find an agent that may answer their request. Vice-versa, if the output
agents that perceive that they can't no longer perform a given action to unsubscribe
themselves thus reducing possible miscommunication or system errors.
Fig. 3. Deployment diagram.
Text-to-Speech and Speech-to-Text European Portuguese capabilities of the
system, made available by a speech recognizer and a text synthesizer separated
agents, are implemented using Microsoft's Speech Platform [16]. Video streaming
between the participants was also enabled using JMF (Java Media Framework) over
RTP (Real Time Protocol).
At the time of writing, 3 environment monitoring agents are available: an
environment background “noise” level, implemented by using and event of the speech
recognizer, AudioLevelUpdated; one on the light conditions; a third one, providing an
estimate of the distance of the user to the screen/display. The light conditions are
evaluated based on statistical measures - Mean Sample Value (MSV) - of the
intensities histogram calculated on the acquired image. The distance is obtained using
algorithms based on background subtraction to estimate the position of the person in
the image. Using the properties of the vision system (position, camera and lens
properties, etc.), it is possible to estimate the position of the person related to the
camera.
5 AdaptO – Adaptive Multimodal Output
Focus on the communication between the system and the user - multimodal output - is
the main novelty of our architecture and prototype. In general, systems in this area of
application incorporate various modalities to communicate with the user (such as
voice, text or images) but they are completely devoid of any autonomy, i.e. simply
32
output the messages they receive using default definitions. In the proposed model, it is
intended that these modalities have some independence and self-adaptability to user
and context of use (ex: environment).
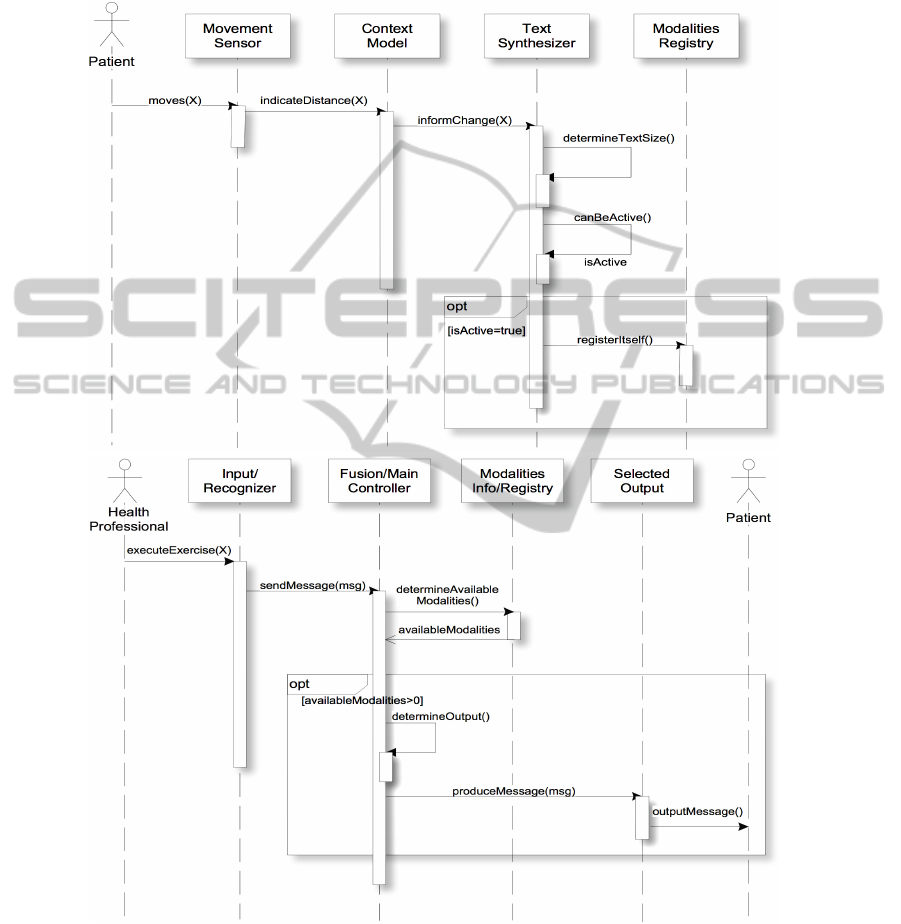
Fig. 4. Sequence diagrams of actions in response to: user movement relative to screen (at top);
instructions regarding a new step of the exercises program sent by the health professional
(bottom).
33

The current agents capable of transmitting information from the system to the user
– synthesizers in multimodal interaction literature - include two important
mechanisms: The first is capable of deciding if, in the current environment conditions
and taking in consideration user capabilities, it is in a position to be active and fulfill
the request. For example, if the user is hearing impaired or the noise level is too high
the synthesizer deactivates itself.
The second changes some of the properties of the message to be transmitted also
based on contextual and user information. Presently, and as proof of concept, the text
synthesizer varies, using simple heuristics, font size as function of user vision
capacity, environment lighting conditions and distance of the user to the screen. The
speech synthesizer is capable of varying both volume and speech rate. This increases
the chances that the message is received and understood. The context and user
models, implemented as services, are crucial to make possible these two mechanisms.
Illustration of the mechanisms in action is presented in fig. 4 using an UML
sequence diagram. The diagram presents the sequence of most relevant actions in
response to a change in user position and when the health professional sends
information on how to execute a part of an exercise.
6 Conclusions
In this paper, we present the description of a new service in the area of elderly health
support at home and of the first prototype implementation. As was considered crucial
to make the service accessible and usable by the target group – older adults – despite
their visual and hearing capabilities, one of the more worked aspects of the
development so far relates to the adaptability and inclusiveness capabilities of output.
The basis for an intelligent adaptation of output – that we called AdaptO, a
Portuguese word meaning adapt – was proposed and first versions of the needed
services and agents were created. In addition, particular attention was given to the
definition of the architecture and on the use of services and agents to create an
implementation. In the near future real user test on the service and applications will be
performed. The interaction aspects of the applications for the health professionals and
elderly at home and the evaluation plan are being finished.
Acknowledgements
This work is part of the COMPETE - Programa Operacional Factores de
Competitividade and the European Union (FEDER) under QREN Living Usability
Lab for Next Generation Networks (http://www.livinglab.pt/).
References
1. LUL Consortium. Living Usability Lab for Next Generation Networks. 2010; Available
from: www.livinglab.pt.
34

2. AAL Forum. Track R - Robotics enabled Assistive Living. 2010; Available from:
http://www.aalforum.eu/page/track-r-robotics-enabled.
3. Best-Martini, E. and K. BOTENHAGEN-DIGENOVA, Exercises for frail Elders. 2008:
Human Kinetics.
4. Burdea, G. C., Virtual rehabilitation--benefits and challenges. Methods Inf Med, 2003.
42(5): p. 519-23.
5. Burdea, G. C., Rubber Ball to Cloud Rehabilitation - Musing on the Future of Therapy in
Virtual Rehabilitation International Conference. 2009: Haifa, Israel p. 50-50.
6. NIDCD. Presbycusis. Available from: http://www.nidcd.nih.gov/health/hearing/
presbycusis.html.
7. Huang, Q. and J. Tang, Age-related hearing loss or presbycusis. European Archives of Oto-
Rhino-Laryngology, 2010. 267(8): p. 1179-1191.
8. McCoy, S. L. et al., Aging in a Fast-Paced World: Rapid Speech and Its Effect on Under-
standing. The ASHA Leader., 2005.
9. O'Connell, T. A., The Why and How of Senior-Focused Design, in Universal Usability, J.
Lazar, Editor. 2009, Wiley.
10. Rousseau, C., Y. Bellik, and F. Vernier, Multimodal output specification / simulation
platform, in Proceedings of the 7th international conference on Multimodal interfaces.
2005, ACM: Torento, Italy. p. 84-91.
11. Persona, User Requirements and AAL Service Specification. 2008, Person Consortium.
12. Bernsen, N. O. and L. Dybkjaer, Multimodal Usability. 2009: Springer.
13. Aoyama, M. Persona-Scenario-Goal Methodology for User-Centered Requirements
Engineering. in 15th IEEE Int. Requirements Eng. Conference. 2007: IEEE.
14. World Health Organization (WHO). International Classification of Functioning, Disability
and Health (ICF). 18 October 2010]; Available from: http://www.who.int/
classifications/icf/en/.
15. Bellifemine, F. et al., JADE (Java Agent DEvelopment Framework) - A White Paper, in
exp. 2003.
16. Microsoft. Developing Speech Applications. 2010; Available from:
http://www.microsoft.com/speech/developers.aspx.
35
