
STRUCTURING MEDICAL AGILITY
Christoph J. Stettina, Lucas P. J. Groenewegen and Bernhard R. Katzy
CeTIM / LIACS, Leiden University, Niels Bohrweg 1, 2333 CA Leiden, Netherlands
Keywords:
Clinical pathways, Process modeling, Medical teamwork, Knowledge work, Self-adaptation, Documentation,
Dynamic consistency.
Abstract:
Technology is omnipresent in intervention rooms, potentially having enormous impact on workflows and on
flexibility. Despite ICT systems’ more flexible support of medical protocols, the styles of collaborating do not
really match. Intervention support systems are as yet stand alone and not sufficiently interoperable. Taking an
ICT perspective, we seek to understand medical work, how to view the way it is organized and how to improve
its integration with intervention support systems, driven by highly dynamic coordination models embedded in
the framework of clinical pathways.
1 INTRODUCTION
New technologies enable new possibilities in medical
operating rooms. They make interventions noninva-
sive and less risky. Technology in fact is omnipresent
in intervention rooms, having enormous impact on
workflows and their flexibility. However, despite im-
provements in medical support systems and in medi-
cal protocols the styles of collaborating do not match.
Intervention support systems are as yet stand alone
and not interoperable. They lack the support for col-
laboration agility in the medical domain. CT images
from different vendors require different viewing soft-
ware; they regularly are being transferred on portable
media. Complex patient data rendering requires an
approach tailored towards relevant caregivers, either
present at intervention or being elsewhere.
Within the EDAFMIS project the authors investi-
gate the introduction of state-of-the-art medical inter-
vention support systems in medical operating rooms.
A minimal intervention cockpit is being developed to
support automation and navigation of noninvasive in-
terventions in line with a new generation of imag-
ing systems. The project targets at real-time inter-
operability and user interaction, thereby flexibly inte-
grating medical skills with systems rendering patient
data. Within the part of the project described here, we
want to grasp flexibility in medical work, how it is or
could be organized in view of its integration with ICT,
driven by highly agile coordination models embedded
in clinical pathways.
2 PROCESS MODELING AND
MEDICAL WORK
During a medical intervention, several specialists are
involved in different roles; also, various views on pa-
tient data and on treatment workflow are needed. This
is knowledge work, requiring new forms of organiz-
ing. However, the standard concepts of work come
from bureaucratic and hierarchical organizations in
the industrial era and little agreement exists on how
post-bureaucratic organizing could be conceived.
As opposed to industrial work, knowledge work is
valued for the ability to interpret information instead
of performing manual labor. Knowledge work can
especially be found in domains such as health care,
law, education, science or engineering. Information
technology increasingly allows physical operations to
be performed remotely, thus shifting manual work to-
wards knowledge work, done by people governing
machines. This requires new approaches structuring
and studying knowledge work.
Medical doctors and nurses do need agility. Their
tasks include collecting and analyzing patient data in
order to formulate and provide a corresponding treat-
ment, while working under expanded responsibilities
and strict time constrains. Medical agility is difficult
to predict when developing clinical pathways. Quick
reaction to changing information and smooth self-
adaptation is obviously crucial in a life saving envi-
ronment and should be embodied in system as well as
in team processes. To meet clinical effectiveness, ad-
614
J. Stettina C., P. J. Groenewegen L. and R. Katzy B..
STRUCTURING MEDICAL AGILITY.
DOI: 10.5220/0003276406140617
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2011), pages 614-617
ISBN: 978-989-8425-34-8
Copyright
c
2011 SCITEPRESS (Science and Technology Publications, Lda.)
justing has to be done smoothly, quickly and with-
out quiescence. In view of achieving ongoing and
smoothly changing medical collaborations, we want
to apply a new ICT-approach in self-adaptive coordi-
nation.
EDAFMIS aims at extending intervention flexi-
bility by integrating patient specific data and profes-
sional knowledge with an interoperable visual system.
It aims at connecting medical workflow and special-
ist skills to the intervention support system. Here we
aim at bridging the gap between medical pathways
and ICT in terms of structured agility. Facing the
challenges in medical work, we have decided to in-
vestigate the applicability of a highly dynamic coor-
dination modeling language in the setting of clinical
pathways in care planning.
2.1 Clinical Pathways
Clinical pathways first emerged in the 1980s in the
United States aiming at organizational efficiency in
hospitals by uniforming lengths of stay, standardiz-
ing treatment packages and thus enabling predictable
costs (Zander, 1991).
Pathways usually consist of several forms com-
bining the nursing care plan with medical notes, and
some sort of a process diagram visualizing the pro-
cess. The diagrams provide a global view, while the
loose forms guide the respective medical journey and
embed the reports. Implemented through broader na-
tional agendas, pathways aim to improve efficiency,
quality and local flexibility (Pinder et al., 2005; DOH,
1997) by continuous improvement based on best prac-
tice while reducing variations (Campbell et al., 1998).
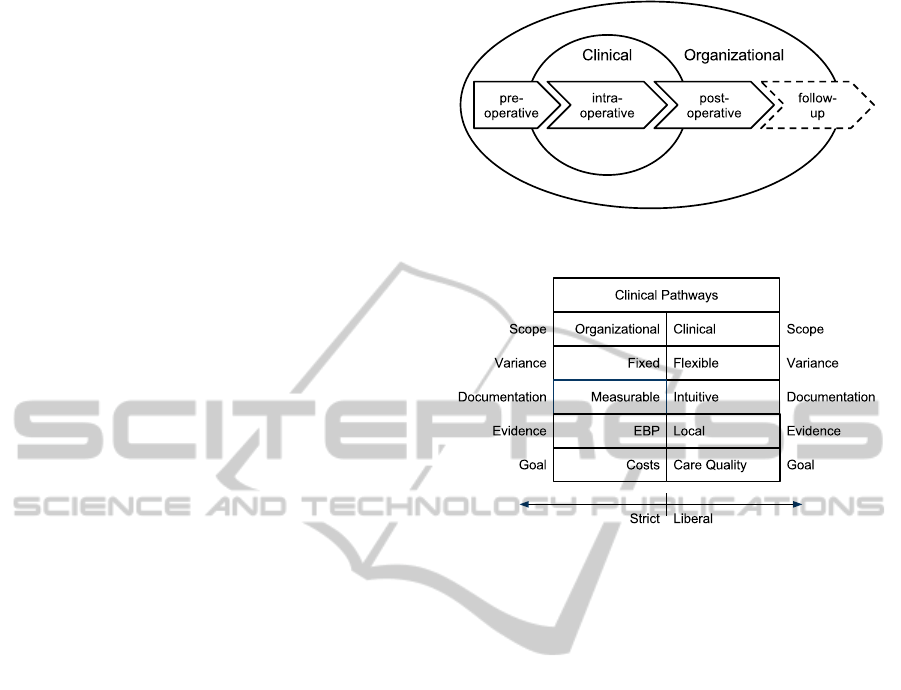
There are two main approaches of pathway proto-
cols in terms of their scope, see Figure 1. From the
broader organizational perspective pathways define
content such as discharge planning, nutrition man-
agement, pain management and patient education.
Taking the clinical perspective, pathways deal with
the sequencing and timing of care, specifying each
step of a medical intervention (Hunter and Segrott,
2008). From a modeling point of view pathways aim-
ing at the clinical scope are descendants of Critical
Path Methods (CPM) and Program Evaluation Re-
view Techniques (PERT) and Gantt charts (Zander,
1991).
Literature reveals quite some discussion regarding
different pathway approaches and how they should
be designed. Apart from the organizational scope of
pathways and their tightly aligned goals, it is most
notably the level of flexibility in the approach being
discussed, as represented in Figure 2.
We understand such recent variants in path-
Figure 1: Different Scopes of Clinical Pathways.
Figure 2: Aspects of Clinical Pathway Implementations.
way literature regarding nomenclature and definition
(Hunter and Segrott, 2008; Vanhaecht et al., 2006) as
a pointer at lacking standardization. Within this re-
search we aim to bridge the gap between the existing
medical pathways and ICT solutions, to improve our
understanding of possibilities for integration. Thus,
we hope to contribute to protocol improvement by
incorporating flexibility into the skeleton of clinical
pathways.
2.2 Coordination and Self-adaptation
Dynamic adaptation, consisting of interactive, usu-
ally distributed components, heterogeneous and with
a varying configuration, obviously adds significant
complexity to the overall system. Dynamic adaptive
systems (DAS) thus must be safety-critical: no fail-
ure is to be accepted, since it could result in loss of
life. In literature adaptation is viewed conceptually
as a three-layered architecture (Kramer and Magee,
2007; Garlan and Schmerl, 2002).
As many systems today, medical equipment is af-
fected by dynamic changes in its operational environ-
ment. Such systems cannot be simply shutdown to
be changed, updated or upgraded and restarted again.
This is particularly important for a live saving envi-
ronment in which adaptation has to be done smoothly,
quickly and without quiescence to support ongoing
collaboration and meet clinical effectiveness. We ar-
STRUCTURING MEDICAL AGILITY
615

gue that clinical pathways as currently formulated, do
not allow for agility needed within complex medical
interventions supported by ICT; we however conjec-
ture, such pathways can be used as a process skeleton
suited for being enriched with agility.
The coordination modeling language Paradigm
(Andova et al., 2010), as a possible approach, ad-
dresses coordination of collaborating components in
terms of dynamic constraints. Its component McPal
(Andova et al., 2009) allows the addition of new be-
havior, and, subsequently, gradually adapts the sys-
tem dynamics without quiescence. We would like to
model agile patterns observed in medical teamwork in
this manner,thus enriching the existing process skele-
ton as provided by organizational pathways.
3 STRUCTURING AGILITY IN
MEDICAL INTERVENTIONS
As outlined in the introduction, the goal of EDAFMIS
is the development of a well-integrated ICT solution.
This study contributes to the integration of the ICT
system into medical practice and, more specifically,
to the agile coordination of a medical team and its
ICT-support. Thus, this research seeks to understand
medical work: how to view the way it is organized
and how to improve its integration with state-of-the-
art medical equipment.
There is ongoing discussion, calling for new con-
cepts regarding working in flexible conformity to the
knowledge dynamics. There is little agreement on
how post-bureaucratic organizing should look like
and we start looking back at work studies of Scientific
Management (Taylor, 1911) and of detailed ethno-
graphic studies of work (Barley and Kunda, 2001).
Knowledge work is different from Scientific Manage-
ment where every step of a worker can be measured
according to quantitative criteria. To circumvent diffi-
culties in registering and measuring knowledge work
rather strictly, we investigatethe suitability of a highly
flexible coordination modeling language.
Process models for automation of work processes
could be a possible direction for our research. Our
particular goal is understanding flexible knowledge
work were smoothly changing collaborations remain-
ing ongoing. In addition this should be integrated
with likewise smoothly changing as well as ongo-
ing ICT support. Process models and ICT are natu-
ral partners, providing new opportunities to support
knowledge work. Their common strengths, however,
have not yet been fully exploited in practice (Giaglis,
2001). We aim at contributing to research how to
structure knowledge-oriented medical work and its
ICT support, while keeping flexibility via dynami-
cally adaptable coordination models applied.
In the remainder of this section we explain the re-
search method we have chosen to investigate the use
of highly dynamic process models in the medical do-
main.
3.1 Research Method
In order to understand the co-evolutionary impacts of
technology on human teamwork practice, a system-
atic approach needs to be incorporated into this re-
search, capturing human behavior in clinical settings
and its connection to ICT (Morrison et al., 2007).
As it is difficult to predict all possible events within
the initial development phase and as ideas materi-
alize within ongoing development, we organize our
research in an iterative manner. Thus we propose
an exploratory study of five phases embedded in a
case study design: Orientation, Investigation, Iden-
tification, Modeling and Verification. We outline the
phases briefly.
Orientation: As a first step we discuss the problem
domain. A literature review is conducted to review
the current knowledge. It is important as a prepara-
tion and it helps us to stay focused during the next
steps. Hereby we reflect on the current literature in a
structured manner.
Investigation: To study human teams and their in-
teraction with technology different sociological mod-
els and theories have been developed. Literature sug-
gests ethnographic and other qualitative methods for
detailed studies of work. Due to the exploratory na-
ture of this research, we conduct participant observa-
tion accompanied by semi-structured interviews, in
view of exploring the medical work domain on site,
particularly its dynamics in intervention rooms.
Identification: In this step we prepare and analyze
the data in order to be able to identify re-occurring
routines. After having cleaned the data, we use it to
find appropriate groupings and patterns.
Modeling: We research dynamic coordination
models within a domain governed by tacit knowledge,
and generally not well-aligned to ICT. Concerns of
medical personnel need to be addressed (Lapointe and
Rivard, 2005). Readability of models and flexibility
and self-adaptation as perceived by the medical per-
sonnel, is very important. Here we investigate to what
extent Paradigm can be used or has to be extended.
Verification: The process models we develop, are
presented within focussed group sessions of medical
specialist and interviews. The insights gained will be
used to re-evaluate and to improve the models. Possi-
bly, formal analysis might be carried out in combina-
HEALTHINF 2011 - International Conference on Health Informatics
616

tion with Paradigm, thus contributing to verification
even further.
4 CONTRIBUTIONS
We contribute to the quality of medical teams by flex-
ibly integrating medical support systems into nonin-
vasive intervention activities.
Medical pathways for noninvasive interventions
exist today and we extend their organizational skele-
ton with more detailed, but flexible descriptions, as
provided by the Paradigm-McPal approach for self-
adaptive coordination. Thereby we follow the itera-
tive set-up of an ethnographic study, to improve our
understanding of applying highly agile coordination
embedded in clinical pathways. We conduct a de-
tailed study of medical work and use recorded rou-
tines to gather data about and acquire insight into
structuring medical knowledge work. Our findings
will be used to refine the coordination approach to-
wards highly agile medical team work, to be carried
out in conformity to relevant clinical pathways and
supported by well-integrated ICT systems.
In addition, this is related to coordination of
knowledge work in general, so it will lead to new
insight into knowledge work. We consider medi-
cal workflows and clinical pathways as a good em-
pirical case and starting point to address highly dy-
namic knowledge work modeling. By establishing
a bridge-head for understanding and supporting flex-
ibility within medical team work, we see great op-
portunities for generalizing such insight towards non-
medical fields.
ACKNOWLEDGEMENTS
This research has been kindly supported by the
EDAFMIS project in the framework of ITEA2.
REFERENCES
Andova, S., Groenewegen, L. P. J., and de Vink, E. P.
(2010). Dynamic consistency in process algebra:
From Paradigm to ACP. Science of Computer Pro-
gramming. 45pp, to appear.
Andova, S., Groenewegen, L. P. J., Stafleu, J., and de Vink,
E. P. (2009). Formalizing adaptation on-the-fly. Elec-
tron. Notes Theor. Comput. Sci., 255:23–44.
Barley, S. R. and Kunda, G. (2001). Bringing work back in.
ORGANIZATION SCIENCE, 12(1):76–95.
Campbell, H., Hotchkiss, R., Bradshaw, N., and Porteous,
M. (1998). Integrated care pathways. British Medical
Journal, 316(7125):133–137.
DOH (1997). The New NHS: Modern, Dependable. HMSO,
London.
Garlan, D. and Schmerl, B. (2002). Model-based adaptation
for self-healing systems. In WOSS ’02: Proceedings
of the first workshop on Self-healing systems, pages
27–32, New York, NY, USA. ACM.
Giaglis, G. M. (2001). A taxonomy of business process
modeling and information systems modeling tech-
niques. International Journal of Flexible Manufac-
turing Systems, 13(2):209–228.
Hunter, B. and Segrott, J. (2008). Re-mapping client jour-
neys and professional identities: a review of the liter-
ature on clinical pathways. International Journal of
Nursing Studies, 45(4):608–25.
Kramer, J. and Magee, J. (2007). Self-managed systems:
an architectural challenge. In FOSE ’07: 2007 Fu-
ture of Software Engineering, pages 259–268, Wash-
ington, DC, USA. IEEE Computer Society.
Lapointe, L. and Rivard, S. (2005). A multilevel model of
resistance to information technology implementation.
MIS Quarterly, 29(3):461–492.
Morrison, R., Balasubramaniam, D., Kirby, G., Mickan,
K., Warboys, B., Greenwood, R., Robertson, I., and
Snowdon, B. (2007). A framework for supporting dy-
namic systems co-evolution. Automated Software En-
gineering, 14:261–292.
Pinder, R., Petchey, R., Shaw, S., and Carter, Y. (2005).
What’s in a care pathway? Towards a cultural car-
tography of the new NHS. Sociology of Health and
Illness, 27(6):759–779.
Taylor, F. W. (1911). The Principles of Scientific Manage-
ment. Harper and Brothers, New York.
Vanhaecht, K., Bollmann, M., Bower, K., Gallagher,
C., Gardini, A., Guezo, J., Jansen, U., Massoud,
R., Moody, K., Sermeus, W., Zelm, R. V., Whit-
tle, C., Yazbeck, A., Zander, K., and Panella, M.
(2006). Prevalence and use of clinical pathways in
23 countries-an international survey by the european
pathway association. Journal of Integrated Care Path-
ways, 10:28–34.
Zander, K. (1991). What’s new in managed care and case
management. The New Definition, 6:1–2.
STRUCTURING MEDICAL AGILITY
617
