
INTEGRATED ELECTRONIC PRESCRIBING AND ROBOTIC
PHARMACY DISPENSING
Are there Any Benefits?
R. J. Beard
Principal Pharmacist, Sunderland Royal Hospital,
Kayll Road, Sunderland, SR4 7TP, U.K.
Keywords: Electronic prescribing, Automated dispensing Robot, Benefits.
Abstract: Sunderland Royal Hospital (1,000 beds) has used an integrated electronic prescribing (EP) system for 8
years, and recently (2009) linked 2 robotic dispensing machines to the pharmacy module. The impact on
dispensing error rates (quality) and efficiency (costs) were assessed. The implementation delivered staff
efficiencies above expectation, whilst not adversely affecting the dispensing error rates. It was significant
that although the combination of EP plus robot did eliminate dispensing errors, some errors continue to
occur for items not stocked in the robot (e.g. part-packs). In achieving this, the professional pharmacy
model changes.
1 BACKGROUND
In 2005, the Department of Health issued a report
authored by the Chief Pharmacist ‘Building a safer
NHS for patients. –Improving medication safety’
(Smith J. M. 2005). This was a detailed paper on
medication errors, the causes, and potential
remedies, and stemmed from the paper ‘An
Organisation with a memory’ (Donaldson L. 2001).
‘Building a safer NHS for patients’ made many
suggestions to design out errors through use of a
systems approach to medication systems. Electronic
prescribing and robotic dispensing were put forward
as potential tools to help reduce dispensing errors.
However, the advantages of electronic prescribing
and robots are not systematically documented in the
literature, and it remains unclear as to what features
provide the greatest safety. There is a variety of
design in electronic prescribing (EP) and robotic
dispensing systems, and it is important when
surveying the literature to consider the context of the
medication system in a hospital.
The Chief Pharmacist (Smith J. M. 2005) quoted
a study from the dispensing error analysis scheme
[DEAS] published by Cardiff and Vale NHS trust in
his paper. This paper analysed errors from 66
contributing hospitals from 1991 to 2001, and
looked at 7000 errors. As such, it represents one of
the biggest surveys of its kind in the UK. The
following categories of errors was recorded by
frequency as shown in table 1.
Table 1: Frequency and type of dispensing errors.
Type of error Proportion %
wrong drug supplied 23%
wrong strength of correct drug supplied 23%
wrong quantity 10%
wrong warnings or directions 10%
wrong drug name on the label 9%
wrong strength on label 8%
wrong form 7%
wrong patient name on label 7%
Beard (Beard R. J. 2009) described the benefits
of EP, and what features would contribute to the
benefits of EP. His study demonstrated that the
greater the integration of EP with other hospital
systems, the greater the benefit. Similarly, over the
last 10 years, robots have seen increasing use in
hospitals, and whilst some of the benefits seem
obvious, the precise features of a robot which yields
the greatest benefit are yet to be identified. City
Hospitals Sunderland has the following profile;
376
Beard R..
INTEGRATED ELECTRONIC PRESCRIBING AND ROBOTIC PHARMACY DISPENSING - Are there Any Benefits?.
DOI: 10.5220/0003191603760381
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2011), pages 376-381
ISBN: 978-989-8425-34-8
Copyright
c
2011 SCITEPRESS (Science and Technology Publications, Lda.)

Table 2: Types of errors prevented by EP and robots.
Type of error
Proportion % EP prevents
Robot
prevents
EP + Robot
prevents
wrong drug supplied
23% Y Y
wrong strength of correct drug supplied
23% Y Y
wrong quantity
10% Y Y
wrong warnings or directions
10% Y Y
wrong drug name on the label
9% Y Y
wrong strength on label
8% Y Y
wrong form
7% Y Y
wrong patient name on label
7% Y Y
• It serves a general population of 350,000
• It serves a sub-regional population of
750,000
• It has 1,000 acute beds
• It employs 5,000 staff
• It has an income of £300 million
The pharmacy has been operating and integrated
EP system for over 8 years, and recently
implemented a robotic dispensing machine. In doing
so, medication safety was a feature of the business
case. Using EP and robotic dispensing as per
implemented at Sunderland, we can regard
medication errors prevention in the same way as the
DEAS study documented in Table 2.
It follows that provided EP and robotic
dispensing are integrated in a specific way, many
dispensing errors can be ‘designed out ‘by skilful
application of technology.
However, at Sunderland we have realised to
achieve such a system, the professional model for
pharmacy changes. It is the purpose of this report to
identify and document those changes, and to suggest
the pros and cons of such a model.
Traditional Pharmacy Dispensing Models
In the typical dispensing model, and the process is as
follows in the numbered sequence.
1 Decision to discharge patient
2 Doctor writes prescription
3 Prescription delivered to pharmacy
4 Professional check of prescription
5 Prescription dispensed
6 Prescrition checked
7 Prescription placed ready for delivery to ward
This process can take up to 4-8 hours (Beard J.{
not this author} and Wood D. 2010) for non-urgent
items for a variety of reasons. The key point to
remember is that in the pharmacy, the prescription
and dispensed item can always be seen together until
bagged for ward delivery. Below is the process
model at Sunderland is shown in figure 1.
The key points to remember are:
• Because EP is integrated, when the doctor
prescribes the medicine on the computer, he
is also in fact writing the label to attach to
the medicine. This means the label is
always what the doctor requested
• Because the label is always accurate to the
prescription there is no transcription error
• Drugs can only be stored in the robot by bar
code identification. There is a direct
electronic link between the medicine, bar
code, and item selected on the electronic
prescription, and
the label that the robot
applies. These are the crucial links in
deriving safety benefits from technology
• To design in these links is to design out
potential errors.
• Once designed, the system works from
anywhere in the hospital. This allows 60%
of dispensing activity to be triggered
outside the pharmacy at Sunderland
• Automatic labelling is a critical component
of this system
• Once medication has been checked by a
pharmacist (usually at ward level at
Sunderland) the dispensing becomes nearly
instantaneous. The remaining bit of the
process is to get the medication from
pharmacy to the ward.
INTEGRATED ELECTRONIC PRESCRIBING AND ROBOTIC PHARMACY DISPENSING - Are there Any Benefits?
377
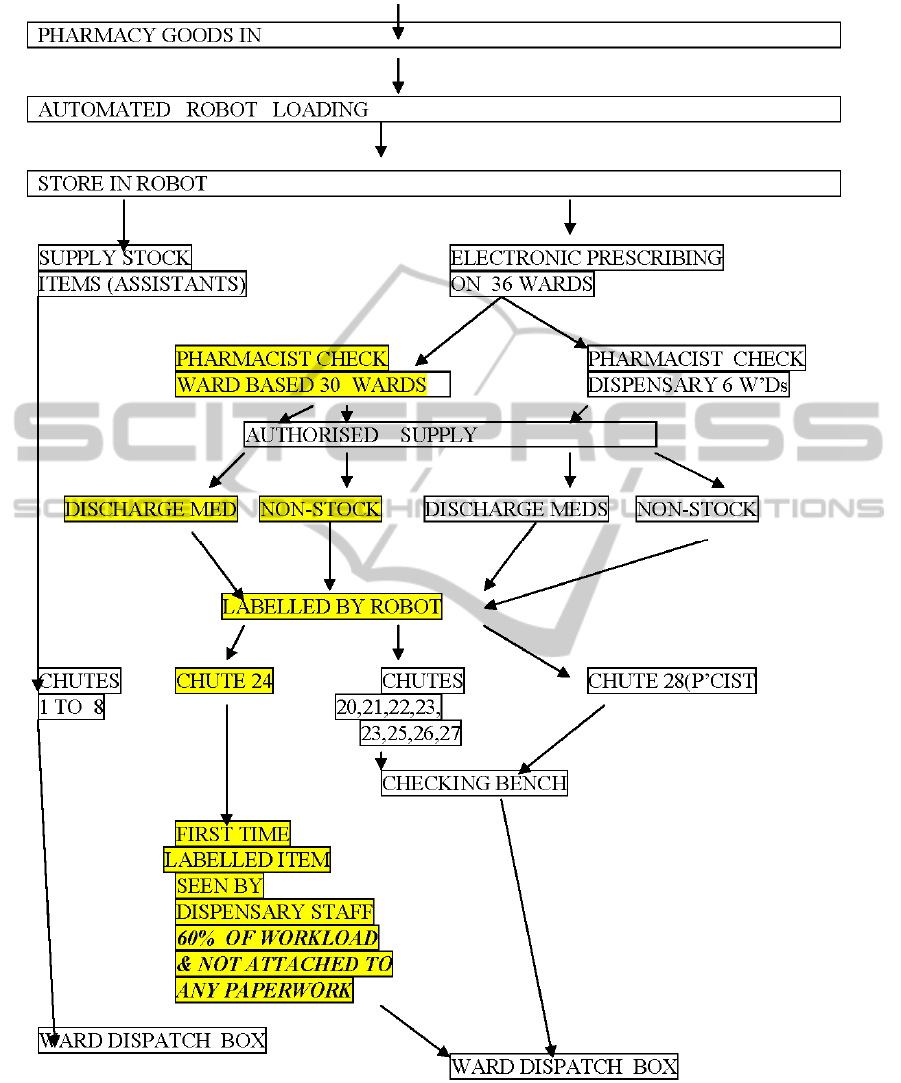
Figure 1: Diagram of dispensing processes at Sunderland.
• In achieving ‘instantaneous dispensing’ the
role of the pharmacist changes. No longer
are pharmacists directly in control over
the whole dispensing process. It is akin to
craftsmen producing goods being replaced
by production lines where quality control is
through process control, and each
individual is responsible for a part of the
overall process, not all of it.
HEALTHINF 2011 - International Conference on Health Informatics
378

2 MEASURING THE BENEFITS
Setting. Sunderland Royal Hospital is a 1,000 bed
hospital in Northern England. The hospital operates
2 dispensaries, including a smaller discrete out-
patients pharmacy dispensing around 5000 items per
month. Control charts have been widely used by
industry for many years to manage process variation,
but the literature for healthcare in Europe suggests
this method of process control is less widely used.
This paper uses of control charts to look at the
impact on out-patient dispensing errors when robotic
dispensing and skill mix reductions are introduced.
Method. Dispensing errors per month was plotted
on a control chart for 12 months prior and
subsequently to the installation of the first
dispensing robot ( March 09). On installation, staff
was reduced by 1.4wte ( in line with business case).
Skill mix was also adjusted (not in business case) to
meet overall operation needs of the department. All
NHS Hospitals in the UK pay staff on a banding
system that equates all jobs on their value. The
higher the job band, the more highly skilled the post.
The job band and whole time equivalents for staff
were determined, and used as a measure of the
‘quantity of skill’ to run the Outpatient pharmacy.
The monetary value of the ‘skill quantity’ changes is
calculated from the mid-point salary scale.
Results. The change in skill mix was 50% ; (Table.
3). On installing the robot, band 5 technical staff
could be replaced with lower banded dispensing
staff, without adversely affecting the quality of the
dispensing process. This was 16% more efficient
than the business case required.
Discussion. Changes in skill mix equates to an
additional saving on top of staff reduction more than
the business case. Early data from the control chart
suggests de-skilling the dispensary workforce using
robots has a no worse impact on dispensing errors.
However, towards the end of 2009, there was an
increase in dispensing errors. This is where control
charts are useful to monitor the processes, when
dealing with small numbers. There is no EP function
at present in the Out-patient pharmacy, and analysis
of the ‘blip’ was undertaken by looking at the errors
and other factors. An audit of the prescriptions
received was undertaken, revealing that 25% of the
written prescriptions required further clarification by
the pharmacist.
It should be noted that the out-patient dispensary
does not yet have EP, but uses traditional pharmacy
prescriptions. The impact on errors, efficiency and
skill mix apply without any of the EP benefits. A
previous paper (5) listed the different types of
dispensing methods at CHS, and the error rates
associated with them. The same approach has been
taken for looking at errors for in-patient dispensing.
The results to date are shown in figure 2.
Figure 2 shows a spike in errors just after
installation. Error analysis showed them to be non-
robot errors,i.e. they were picking errors from those
shelves of the pharmacy where items cannot go into
robots ( part packs, round tubs of medicines, or
items too small (e.g. eye drop bottles) to be labelled
by robot.
Significantly, we have found zero errors for the
robot plus EP system combined, based on around
800,00 items per annum. Potentially a huge benefit
in safety. However, dispensing is not risk-free, since
not all items are supplied and labelled from the
robot. Clearly though, the opportunity for errors is
significantly reduced.
Turn Around Time for Prescriptions. Speed of
turnaround time taken from clinical check is nearly
instantaneous, very different from many hospitals.
At busy periods dispensing times can rise to up to 20
to 30 minutes, but this situation tend not to last
beyond about half an hour. Normally dispensing
times can often be up to 4 hours for non-urgent
dispensing. (Beard J. and Wood D 2010). These
authors quotes how be using lean processes they
reduced the dispensing time of the prescription from
4 hours to around 2 hours. ( These times include the
time it takes a signed prescription to get from ward
to pharmacy.). This is not untypical of non-EP –
robotic system. The concept of instantaneous
dispensing is not currently part of hospital pharmacy
culture, nor is dispensing triggered from over 36
different points in the hospital.
Dispensing Rate. Whittlesea (7) quotes a Welsh
benchmark of 10 items per person per hour.
Sunderland dispenses a maximum of 360 items per
hour, equating to 36 dispensing staff. The in-patient
pharmacy operates with around 10 dispensary staff.
Sunderland’s robot chute 24 issues 60 % of the
dispensing activity, which is from the ward based
pharmacy staff. Ours is not a directly comparable
situation. However if one takes the figure of 360
items an hour the pharmacy can dispense, it has
therefore a capacity of 57,000 items per month. To
INTEGRATED ELECTRONIC PRESCRIBING AND ROBOTIC PHARMACY DISPENSING - Are there Any Benefits?
379
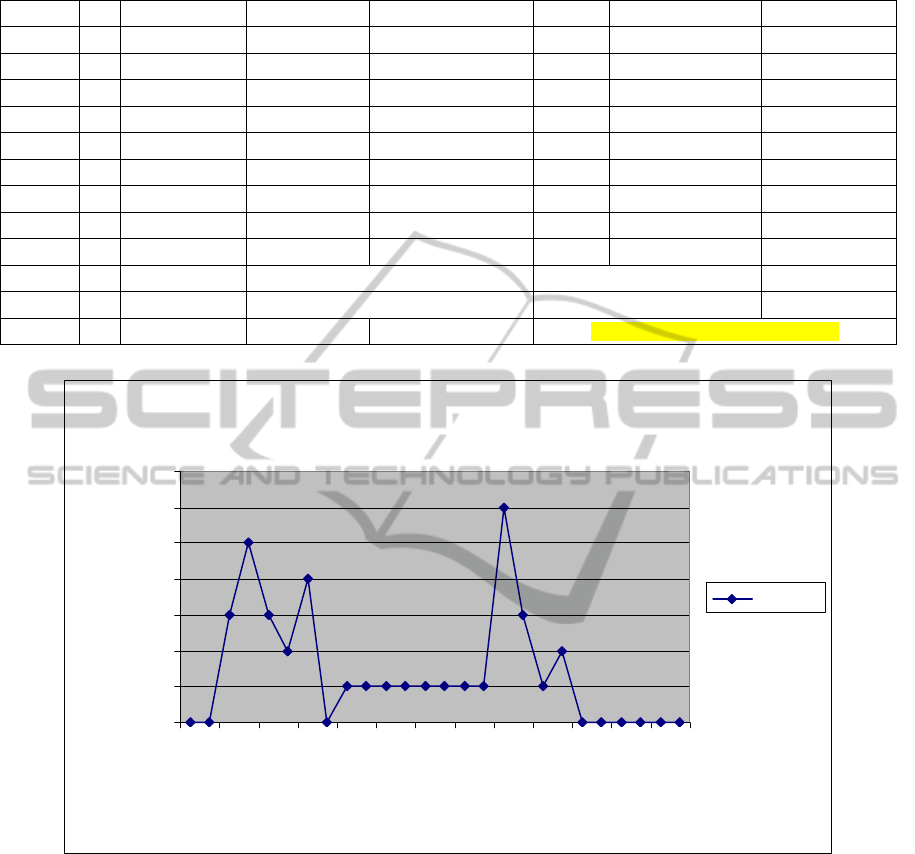
Table 3
Job band wte job band x wte salary paid £'s mid point salary £'s
new wte new skill amount salary total £'s
band 6 1 6 28000 28000 1 6 28000
band 6 1 6 28000 28000 1 6 28000
band 5 2.4 12 56040 23350 0 0 0
band 4 1 4 19500 19500 1 1 19500
band 3 1 3 17000 17000 1 1 17000
band 2 1 1 14360 14360 2 2 28720
totals 6.4
32
162900 5
16
121220
cost reduction 41680
wte= whole time equivalent skill reduction = 50%
BC = business case BC =£35k reduction
Additional benefit over BC = 16%
Errors ( green line = robot installed Sept 2009)
0
1
2
3
4
5
6
7
Ju
n
-08
Au
g-08
O
c
t-
08
Dec-08
F
eb
-
09
Apr-0
9
Jun-09
Au
g-09
O
c
t-
09
Dec-09
F
eb
-
10
Apr-1
0
Jun-
1
0
month
errors
Series1
Figure 2: Dispensing errors in in-patient pharmacy per month. Green line marks use of robot with EP.
put this in community pharmacy terms, a community
pharmacy needs around 7,000 items a month to be
solvent, and a very busy pharmacy might do around
20,000 items per month. The capacity of the in-
patient pharmacy is about 3 times that rate.
3 CONCLUSIONS
There are clear benefits in using electronic
prescribing and robotic dispensing, and these will be
realised so long as the following conditions are met:
• The EP system used is integrated with all
the other hospital software systems
• The robotic dispenser is integrated to the
EP system
• There are automated labellers for those
items robotically dispensed.
When the above conditions are applied several
advantages become apparent:
• For items in the robot, there is no scope to
make a dispensing error, improving patient
safety.
HEALTHINF 2011 - International Conference on Health Informatics
380

• The process is much more efficient, and the
skill mix of staff can be adjusted within the
dispensary
• The speed of the prescription process
increases dramatically.
The consequences of the above are that the
purchasing of medicines needs to be given
consideration so that items with appropriate bar
codes are purchased. There is also a change in the
professional model, as the dispensary pharmacist is
no longer in complete control of the dispensing
going on in the dispensary. The implications of this
are not within the scope of this paper.
REFERENCES
Beard J., Wood D., 2010. Pharmaceutical Journal vol 284
(17
th
April 2010) p369-371
Beard R. J., 2009. Professional Masters Thesis, University
of Sunderland
Donaldson L., 2001. An Organisation with a Memory
www.doh.gov.uk
Kelley D. Lynn, 1999. How to Use Control Charts for
Healthcare ASQ Quality Press. ISBN 0-87389-452-9
www.asq.org
Smith J.M., 2005. Building a safer NHS for patients.
Improving medication safety. . www.doh.gov.uk
Whittlesea C., Phillips C., Roberts D., Burfield R., Savage
J., Way C.. 2004. Automated dispensing- how to
evaluate its impact. Hospital Pharmacist 11 p283-285
INTEGRATED ELECTRONIC PRESCRIBING AND ROBOTIC PHARMACY DISPENSING - Are there Any Benefits?
381
