
INTCARE
Multi-agent Approach for Real-time Intelligent Decision Support
in Intensive Medicine
Manuel Filipe Santos, Filipe Portela and Marta Vilas-Boas
Departamento de Sistemas de Informação, Universidade do Minho, Guimarães, Portugal
Keywords: Artificial intelligence, Multi-agent systems, Agent intelligent Decision support systems, Intensive care.
Abstract: For an Intelligent Decision Support System to work in real-time, it is of great value the use of intelligent
agents that cooperate with each other to accomplish their tasks. In a critical environment like an Intensive
Care Unit, doctors should have the right information, at the right time, to better assist their patients. In this
paper we present an architecture for a Multi-Agents System that will support doctors’ decision by in real-
time, guaranteeing that all required clinical data is available and capable of predicting the patients’
condition for the next hour.
1 INTRODUCTION
There is a need to develop an Intelligent Decision
Support System (IDSS) for intensive care to help
doctors decide about the best care to provide their
patients. Such system is expected to reduce medical
errors, to fasten clinical interventions and, overall, to
provide better care by having the required
information at the right place, at the right time. The
INTCare system has this vision and its goals are
towards an IDSS as a Multi-Agents System (MAS).
“Intelligent agents with their properties of
autonomy, reactivity, and proactivity are well suited
for dynamic, ill-structured, and complex
environments (Gao and Xu 2009), such as an
Intensive Care Unit (ICU). This paper presents the
INTCare system as a MAS for intelligent decision
support, an innovative agent-based architecture, and
the prototype system.
Intelligent agent technology is at an appealing
point in its advance. “Intelligence with Interaction”
applications are progressively more being developed
in domains such as meteorology, manufacturing,
war gaming and capability assessment (Tweedale et
al. 2007).
More useful than a system acting intelligently, is
the ability for a system to cooperate in an
environment with other intelligent agents, whether
they are humans or machines (Guerlain et al. 2000).
Furthermore, “it is necessary for a system to be able
to communicate with others, detect and correct
mistakes, and take advantage of others’ abilities.”.
The key is to use distributed artificial intelligence
for decision support (Cortes et al. 2000).
2 BACKGROUND
MAS are computational systems in which several
artificial agents interact to perform predefined tasks
to satisfy some set of goals (Lesser 2003).
INTCare is an IDSS for intensive medicine that
makes use of intelligent agents based on a MAS. For
supporting clinical decision, it makes predictions of
organ failure and outcome and, according to the
predictions, it suggest therapies, treatments and
procedures, by means of DM (Data Mining)
techniques. In order to accomplish its goals, the
system is divided in four subsystems composed by
intelligent agents that cooperate amongst the
system’s modules, as shown in Figure 1.
Subsystems:
Data acquisition;
Knowledge Management;
Inference;
Interface.
364
Santos M., Portela F. and Vilas-Boas M..
INTCARE - Multi-agent Approach for Real-time Intelligent Decision Support in Intensive Medicine .
DOI: 10.5220/0003182603640369
In Proceedings of the 3rd International Conference on Agents and Artificial Intelligence (ICAART-2011), pages 364-369
ISBN: 978-989-8425-40-9
Copyright
c
2011 SCITEPRESS (Science and Technology Publications, Lda.)
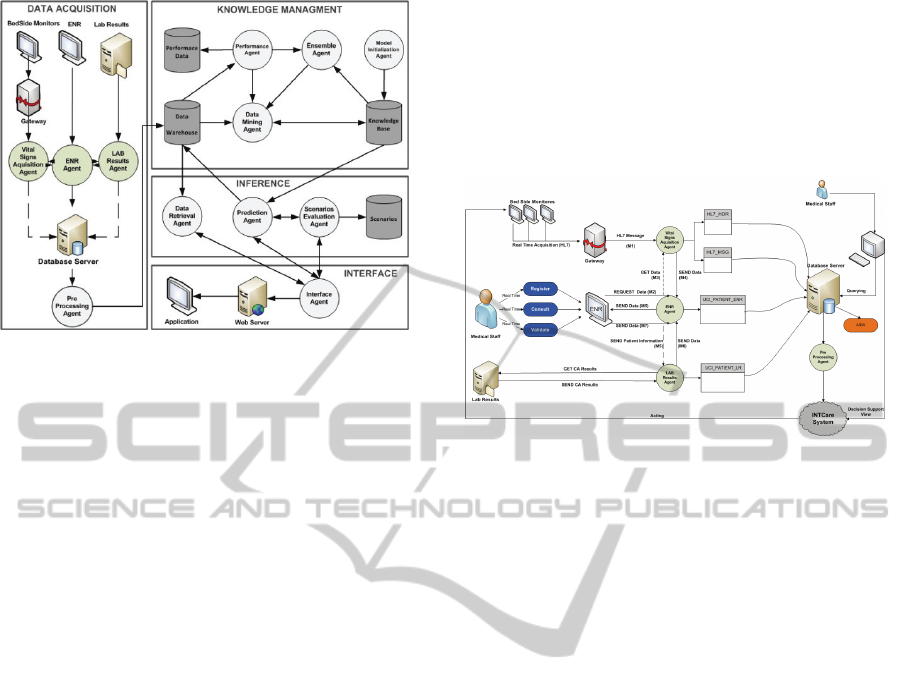
Figure 1: INTCare system and its four subsystems.
The data required for the DM models is gathered
in the ICU and relates to the patients’ clinical
condition (monitored data, nursing records, lab
results) and derived variables like Sequential Organ
Failure Assessment (SOFA) scores, critical events
(Silva et al. 2008), ratios (Vilas-Boas 2010) and
Modified Early Warning Scores (MEWS) (Subbe et
al. 2001). These data origins in distributed
heterogeneous data sources and, to guarantee the
system’s viability in real-time, it relies on intelligent
agents. In this paper, we focus on latest
developments of the data acquisition subsystem in
order to achieve INTCare’s goals. They go beyond
retrieving, collecting and integrating relevant
information; they encompass discovering previously
unknown, implicit and valuable knowledge (Klusch
et al. 2003). Even though the previous system had a
data acquisition subsystem, it lacked some important
features and functionalities, mainly related to the
information it was able to acquire. This subsystem
was able to gather and store data from the vital signs
monitoring. However, with our advances in the
research related to the prediction of organ failure,
there is the need for more data other than the
previously gathered, mainly data from lab results
and drugs systems. Also, previously, data was
collected and post processed, which was not suited
for a real-time system.
The system is currently being tested in the ICU
of Hospital Geral de Santo António (HGSA), Porto,
Portugal.
3 DATA ACQUISITION SYSTEM
- REDESIGN
With the new requirements of INTCare, i.e. data
collected in real-time and available online, it was
necessary to redesign the data acquisition system
and its architecture. The new model allows all data
to be collected and stored in electronic mode and the
extinction of paper-based information throughout the
ICU. The existing agents were preserved and added
new tasks.
Figure 2: Data acquisition subsystem.
The tables contained in the database are defined
in terms of their attributes, as follows:
HL7_HDR {MSG DATA}
HL7_MSG {Vital Signs)
UCI_PATIENT_FEE {PaO
2
, FiO
2
, Glasgow,
Urine Output, Amines,
Patient Outcome, Drugs, …}
UCI_PATIENT_LR {Creatinine, Billirubin,
Blood Platelets, PaO
2
, FiO
2
,
SOFA, …}
UCI_DATABAE {HL7_MSG,UC
I_PATIENT_FEE,
UCI_PATIENT_LR}
Figure 2 presents the link to other subsystems,
which is a consequence of the work of Data
Acquisition System.
4 INTCARE SYSTEM’S AGENTS
The tasks of the intelligent agents support some
system modules: Data Acquisition, Management of
Knowledge, Inference and Interface. The flexibility
and effectiveness of such systems depend on the
agents and the interactions between them.
4.1 Data Acquisition Agents
These agents will be in charge of the tasks
associated to the data acquisition.
INTCARE - Multi-agent Approach for Real-time Intelligent Decision Support in Intensive Medicine
365

Gateway (a
gat
)
is responsible for capturing the vital
signs data from bedside monitors and operates in
real-time. These data are packed into HL7 messages
and sent to the Vital Signs Acquisition Agent. It
collects information, in average, once per minute
and restarts at each hour to ensure that no
communications failures compromise the system;
Vital Signs Acquisition (a
vsa
)
was reformulated. It
is an AIDA process that parses the HL7 messages in
real-time, extracts information blocks, splits the
information and stores them in the database tables.
The table HL7_Message contains the values and
results from vital signs monitoring (id_category,
value, patient_id, msg_date).
ENR Agent (a
enr
) is new and was created with the
Electronic Nursing Record (ENR) (Portela et al.
2010, M.F. Santos et al. 2009b) and replaces the
Clinical Data Entry Agent. It was developed to allow
some information in electronic mode.
This agent works in two forms: automatic (can
save the data in minutes) and manual, when it’s the
user who saves the information. It is responsible to
capture the clinical data from the medical and
nursing staff (Gago et al. 2006). When it receives the
data, it splits the information, clears the information
displayed in the table for that patient in that day and
stores the new data.
LR (a
lr
) is new and it’s an evolution of Clinical
Analysis Data Entry Agent that was responsible for
capturing the clinical data from the lab results.
This agent works in association with the ENR
because it only gets information from a certain
patient when it is required by the ENR. The process
is easy and smooth; The ENR agent requests to (a
lr
),
every five minutes, new results of lab results. This
agent verifies if there are new results from a patient
and, if so, it stores them in UCI_PATIENT_LR and
sends the new information to ENR.
All information collected and stored by data is
available by AIDA (Abelha et al. 2003).
AIDA (a
ada
) is an agency to archive and to
disseminate medical exams and results, implemented
at the hospital. It supplies the lab results and nursing
records through the clinical analysis data entry agent
and clinical data entry agents (Abelha et al. 2004).
Pre-processing (a
pp
) agent is responsible for the
correct linking of all the values in order to create a
valid medical record for the patient (Gago et al.
2006). It is in charge of solving some data
acquisition problems (M.F. Santos et al. 2009a).
Before data is consolidated in the data
warehouse, the agent verifies the data in order to
remove null values and correct the values that are
out of range (M. F. Santos et al. 2009). It proceeds
with the copy of the values received from the three
data sources: bedside monitors, electronic nursing
records and lab results that were stored in the tables.
At the moment, we are studying another method
to optimize results using the MEWS.
4.2 Knowledge Management Agents
This subsystem is composed by three agents: Data
Mining, Performance and Ensemble.
Data Mining (a
dm
) agent is responsible for the
retrieval of the relevant data in order to make
possible the application of AI algorithms for the
predictions and to train new models, whenever
requested by the Performance Agent (apf). After the
training, the models are stored in the the Knowledge
Base, applying the Predictive Markup Model
Language (PMML), which is a XML based model
description language (Guazzelli et al. 2009) (Gago et
al. 2006).
This agent converts the data stored in the data
warehouse in Knowledge, creating models in real-
time using online data.
Performance (a
pf
) agent is responsible for
continually consulting the data warehouse to collect
statistics, as a base to calculate a set of assessment
parameters maintained in the Performance Database
(Gago et al. 2006). It analyzes the new data that was
stored in data warehouse and verifies the
performance of the prevision models through DM.
If the collected statistics show that the performance
has fallen below a predefined parameter, a new
model is requested to replace the poor performing
one (Gago et al. 2006).
Ensemble (a
ens
) agent was created to enhance
predictive performance by combining several
models in order to produce models with better
results (Dietterich 2000); It is possible to combine
techniques like decision trees and artificial neuronal
networks.
4.3 Inference Agents
The inference subsystem didn’t have any
adjustments and its agents are the same presented
with the INTCare System (Gago et al. 2006).
Prediction (apd) agent answers user questions by
applying the adequate models contained in the
ICAART 2011 - 3rd International Conference on Agents and Artificial Intelligence
366

Knowledge Base to the data stored in the data
warehouse (Gago et al. 2006);
Data Retrieval (adr) agent’s task is to retrieve, from
the data warehouse, the information requested by the
interface agent (Gago et al. 2006);
Scenario Evaluation (asc) agent makes possible for
doctors to create and evaluate what-if scenarios.
After receiving the data from the interface agent, this
agent requests a forecast from the prediction agent,
the scenario is then stored in the Scenarios Database.
and the result is sent back to the interface agent
(Gago et al. 2006).
4.4 Interface Agents
The Interface subsystem only has one agent, the
Interface Agent. This subsystem suffered some
alterations due the changes presented before. At the
moment we have the web-based ENR that collects
data from various data sources. ENR is also a
consulting platform for patients’ clinical data and,
furthermore, the prediction models created by DM
can also be consulted.
Interface (aint) agent makes possible web-based
interaction with the system by providing an easy
way for doctors to request prognostics and evaluate
scenarios (Gago et al. 2006). For the past days, the
actual SOFA score is shown, together with the value
predicted for the next day. It is also possible to
consult the confidence levels associated with the
prediction values (Gago et al. 2006). At the moment,
we can predict the results for the next hour (Vilas-
Boas 2010) and a holistic view of the patient to the
next hour will be supported by presenting, in the
same chart, the information regarding the organic
systems. Also, the values predicted for the next hour
are shown, providing information that may suggest
the need for immediate action.
5 MULTI-AGENT SYSTEM
INTCare is a MAS because it uses a conjunction of
several agents for preparation of data for prediction.
MAS consists of a set of agents that communicate
with each other and work together towards common
goals, with a degree of reactivity and / or reasoning
(Wooldridge, 1999).
5.1 First Multi-agent Process
All agents presented collect data in real-time and
online mode. They communicate among themselves
to obtain better results. The a
gat
agent processes the
monitored data. When the gateway receives the vital
signs from the monitors, it sends a HL7 message
(M1) to the vital signs acquisition agent and it parses
the information. Next, there is an example of a HL7
message:
MSH|^~\&|DHV |h2|h3|h4|||ORU^R01|h1|P|2.3.1
PID|1||d1||d2
PV1|1|U|v1
OBR|1|||DHV|||r1|
OBX|x2|NM|x3^x4^^^x5||x6|x7|||||R||||x1^ v1||
Table 1 explains the variables in the exchange of
messages between the agents a
gat
and a
vsa
.
Table 1: HL7 message variables (M. F. Santos, et al.,
2009).
h1 Version ID x1 Producer's ID
h2 Sending Facility x2 Value Type
h3
Receiving
Application
x3
Observation
Identifier (cod)
h4
Receiving
Facility
x4
Observation
Identifier (cod2)
d1
Patient ID
(Internal ID)
x5
Observation
Identifier (descp)
d2 Patient Name x6
Observation
Value
v1
Assigned Patient
Location
x7
Units
r1
Observation
Date/Time
x1
The information received by a
gat
is split by a
vsa
in
the form:
HL7_HDR = {h1, h2, h3, h4, d1, v1, x1 }
HL7_MSG = {v1,r1,x2,x3,x4,x5,x6,x7,x1^v1}
5.2 Second Multi-agent Process
The ENR agent communicates with two other agents
(a
vsa
and
a
lr
) and all tasks are triggered by the ENR.
The ENR comprises of two forms to register data
- manual and automatic. When the ENR requires
information to fill its fields, it sends requests to the
ENR Agent with the alert that data it required.
The a
enr
analyzes the request and, according the
needs, (M2) sends information to the other agents
(M3, M5).
The Vital Sign Agent works in real-time and has
new data all the time. In this case, it sends the new
data (M4) to a
enr
and it is sent to the ENR. If the
ENR need lab results, the ENR Agent sends the
Patient ID (PID) (M5) to Lab Results Agent and it
INTCARE - Multi-agent Approach for Real-time Intelligent Decision Support in Intensive Medicine
367

will verify if some new results are available in Lab
Results Server.
Finally, the a
lr
stores data in the DB table and
sends the newest data to the ENR Agent (M6)
which, in turn, sends to the ENR application.
5.3 Other Multi-agent Process
The knowledge management, inference and
interface subsystems needn’t modifications at the
moment, for they are working correctly and in
accordance to the MAS and INTCare’s goals. Their
communication is visible in the arrows presented in
the agents of each subsystem in figure 1.
Performance agents perform some actions to
Data Mining Agent and Ensemble Agent;
Assemble Agents perform some actions to data
Mining Agents;
Scenario Evaluation Agent works together with
Prediction Agent and Interface Agent;
Prediction Agent works with interface agent and
Scenario Evaluation Agent;
Data Retrieval Agent works with Interface Agent
and vice-versa;
Interface Agent works with Scenario Evaluation,
Prediction Agent and Data Retrieval Agent;
6 DISCUSSION
Table 2: Impact of the MAS system in intensive care.
Characteristics Impact
Robustness
The medical staff can work with the
guarantee that the information will
never lost.
Fault Tolerance
Lack of system failures in critical
environments and reduction of medical
error.
Scalability
Possibility to work with large
quantities of clinical information.
Speed up a system's
operation
less time spent with informatics issues.
Efficiency
Systems always running in real-time
and efficiently doing what users
require.
Interconnection and
interoperation of
multiple existing
legacy systems
Medical Staff can have information
about patients when required,
independently of the systems in which
they that are stored.
Table 2 summarizes a set of characteristics of the
MAS and their impact on a critical environment like
ICU, comparing to a single agent or centralized
approach.
By distributing computational resources and
capabilities across a network of interconnected
agents, performance bottlenecks or critical failures,
are not a problem (Gruer and Hilaire 2003).
Overall, with the MAS there is great gain in
system’s performance, efficiency, reliability,
scalability, robustness, maintainability,
responsiveness, flexibility, and reuse (Chira 2007).
These are a critical aspects in intensive care
where, most of the time, patients’ lives are at risk
and all valuable information should be available and
its correctness and ease of interpretation must be
guaranteed. Moreover, the MAS will also provide
the means for prediction and decision models in
real-time, with an hourly granularity.
In our approach, each of the intelligent agents is
able to deal with specific tasks that can be grouped
in data acquisition, knowledge management,
inference and interface in an independent way, so
that the system has a transparent behaviour for the
applications, as well as for the users. For a real-time
system like INTCare, a MAS presents advantages in
processing speed-up, automatic data validation,
access to data and availability of information
electronically.
All modifications were tested in the real
environment of the ICU, guaranteeing that they will
suit correctly the requirements and identifying
possible new requirements and/or refinements.
7 CONCLUSIONS
AND FURTHER WORK
For accomplishing INTCare’s goals, some redesign
regarding the agents was presented. Data acquisition
subsystems and its agents were reformulated and
new agents were created.
Agents can perform some previously manual
action in automatic mode, without human
intervention. This feature is of great importance in a
real-time IDSS. To achieve so, the Data Acquisition
Architecture was redesigned to allow data
acquisition in real time and online mode.
Regarding the interface, we are studying two
solutions for presenting the information originated
by the DM models – partially in the ENR and
wholly it INTCare platform.
ICAART 2011 - 3rd International Conference on Agents and Artificial Intelligence
368

ACKNOWLEDGEMENTS
The authors would like to thank FCT (Foundation of
Science and Technology, Portugal) for the financial
support through the contract PTDC/EIA/72819/
2006.
REFERENCES
Abelha, A., Machado, J., Alves, V. and Neves, J. (2004)
'Health data management in the medical arena',
WSEAS-Transactions-on-Computers.
Abelha, A., Machado, M., Santos, M., Sollari, A., Rua, F.,
Paiva, M. and Neves, J. (2003) 'Agency for Archive,
Integration and Diffusion of Medical Information',
Proceeding of AIA.
Balter, J., Labarre-Vila, A., Ziébelin, D. and Garbay, C.
(2002) 'A knowledge-driven agent-centred framework
for data mining in EMG', Comptes Rendus Biologies,
325(4), 375-382.
Chira, C. (2007) 'A Multi-Agent Approach to Distributed
Computing'.
Cortes, U., Sanchez-Marre, M., Ceccaroni, L., R-Roda, I.
and Poch, M. (2000) 'Artificial intelligence and
environmental decision support systems', Applied
Intelligence, 13(1), 77-91.
Dietterich, T. (2000) 'Ensemble methods in machine
learning', Multiple classifier systems, 1-15.
Gago, P., Santos, M. F., Silva, Á., Cortez, P., Neves, J.
and Gomes, L. (2006) 'INTCare: a knowledge
discovery based intelligent decision support system for
intensive care medicine', Journal of Decision Systems.
Gao, S. and Xu, D. (2009) 'Conceptual modeling and
development of an intelligent agent-assisted decision
support system for anti-money laundering', Expert
Systems with Applications, 36(2), 1493-1504.
Gruer, P. and Hilaire, V. (2003) A multi-agent approach to
modeling and simulation of transport on demand
problem, translated by Springer, 119.
Guazzelli, A., Zeller, M., Lin, W. C. and Williams, G.
(2009) 'Pmml: An open standard for sharing models',
The R Journal, 1(1), 60-65.
Guerlain, S., Brown, D. E. and Mastrangelo, C. (2000)
Intelligent decision support systems, translated by
1934-1938.
Klusch, M., Lodi, S. and Moro, G. (2003) 'Agent-based
distributed data mining: The KDEC scheme',
Intelligent information agents, 104-122.
Lesser, V. R. (2003) Multi-agent systems, translated by
John Wiley and Sons Ltd., 1196.
Portela, F., Vilas-Boas, M., Santos, M. F. and Fernando,
R. (2010) 'Improvements in data quality for decision
support in Intensive Care', in eHealth 2010 - 3rd
International ICST Conference on Electronic
Healthcare for the 21st century, Casablanca, Morroco,
8.
Santos, M. F., Portela, F., Vilas-Boas, M., Machado, J.,
Abelha, A. and Neves, J. (2009a) 'Information
Architecture for Intelligent Decision Support in
Intensive Medicine', 8th WSEAS International
Conference on APPLIED COMPUTER &
APPLIED COMPUTATIONAL SCIENCE (ACACOS
'09), 8(5), 810-819.
Santos, M. F., Portela, F., Vilas-Boas, M., Machado, J.,
Abelha, A., Neves, J., Silva, A. and Rua, F. (2009)
'Information Modeling for Real-Time Decision
Support in Intensive Medicine' in Chen, S. Y. and Li,
Q., eds., Proceedings of the 8th Wseas International
Conference on Applied Computer and Applied
Computational Science - Applied Computer and
Applied Computational Science, Athens: World
Scientific and Engineering Acad and Soc, 360-365.
Santos, M. F., Portela, F., Vilas-Boas, M., Machado, J.,
Abelha, A., Neves, J., Silva, A., Rua, F., Salazar, M.,
Quintas, C. and Cabral, A. (2009b) 'Intelligent
Decision Support in Intensive Care Units - Nursing
Information Requirements' in Springer, ed. WSEAS
Transactions on INFORMATICS.
Silva, Á., Cortez, P., Santos, M. F., Gomes, L. and Neves,
J. (2008) 'Rating organ failure via adverse events using
data mining in the intensive care unit', Arificial
Intelligence in Medicine, 43(3), 179-193.
Subbe, C. P., Kruger, M., Rutherford, P. and Gemmel, L.
(2001) 'Validation of a modified Early Warning Score
in medical admissions', QJm, 94(10), 521.
Tweedale, J., Ichalkaranje, N., Sioutis, C., Jarvis, B.,
Consoli, A. and Phillips-Wren, G. (2007) 'Innovations
in multi-agent systems', Journal of Network and
Computer Applications, 30(3), 1089-1115.
Vilas-Boas, M., Santos, MF.,Portela, Filipe., Silva,
Álvaro., Rua, Fernando. (2010) Hourly prediction of
organ failure and outcome in intensive care based on
data mining techniques, translated by Funchal,
Madeira.
INTCARE - Multi-agent Approach for Real-time Intelligent Decision Support in Intensive Medicine
369
