
TOWARDS AN ARTIFICIAL THERAPY ASSISTANT
Measuring Excessive Stress from Speech
Frans van der Sluis, Egon L. van den Broek
Human-Media Interaction (HMI), University of Twente, P.O. Box 217, 7500 AE Enschede, The Netherlands
Ton Dijkstra
Donders Institute for Brain, Cognition, and Behavior, Radboud University
P.O. Box 9104, 6500 HE Nijmegen, The Netherlands
Keywords:
Stress, Psychiatry, Diagnosis, Speech, Agent, Model.
Abstract:
The measurement of (excessive) stress is still a challenging endeavor. Most tools rely on either introspection
or expert opinion and are, therefore, often less reliable or a burden on the patient. An objective method could
relieve these problems and, consequently, assist diagnostics. Speech was considered an excellent candidate
for an objective, unobtrusive measure of emotion. True stress was successfully induced, using two storytelling
sessions performed by 25 patients suffering from a stress disorder. When reading either a happy or a sad story,
different stress levels were reported using the Subjective Unit of Distress (SUD). A linear regression model
consisting of the high-frequency energy, pitch, and zero crossings of the speech signal was able to explain
70% of the variance in the subjectively reported stress. The results demonstrate the feasibility of an objective
measurement of stress in speech. As such, the foundation for an Artificial Therapeutic Agent is laid, capable
of assisting therapists through an objective measurement of experienced stress.
1 INTRODUCTION
In 1975, Malcolm Lader stated: “Psychiatric re-
search has been unsuccessful in developing scientific
methods of its own but has relied on a series of tech-
niques borrowed from other disciplines. Too often the
outside discipline has been chosen because of its rel-
evance, and the high hopes at the outset of such stud-
ies have lessened as concrete advances have failed to
materialise.” (Lader, 1975). Since these words were
published significant progress has been made in both
science and engineering. However, psychiatry is still
struggling in some sense. On the one hand, it is now
generally accepted that mind and body go hand in
hand. Consequently, for example, psychopharmacy
have gained in popularity since Lader’s words. On the
other hand, science is not even close to truly under-
standing the relation between mind and body, which
is illustrated by the lack of computational models.
Computational models have been proposed in the
shape of decision support systems and agents. In
some branches of industry these models have been
successfully employed but not in psychiatry. Various
reasons for this lack of success can be opted; for ex-
ample, overly complex models, unjustified simplifi-
cations, a lack of validation procedures, and simply a
lack of domain knowledge. To prevent from suffering
the same pitfalls, this study limits its aims. The core
concept under investigation will be: stress.
The usage of the term stress has been liberal, leav-
ing it as a poorly defined term with many defini-
tions. However, as a common denominator, the differ-
ent views build upon some form of a process model,
in which “environmental demands tax or exceed the
adaptive capacity of an organism, resulting in psycho-
logical and biological changes that may place per-
sons at risk for disease” (Cohen and Oviatt, 2002).
Several traditions have emphasized different aspects
of this process: environmental, psychological, and
biological aspects. These can be roughly translated
to, respectively, the stressor (Kessler, 1997), the ap-
praisal (Lazarus, 1993), and their (often physiologi-
cal) responses (Cohen and Oviatt, 2002).
Table 1 gives an overview of a few prevalent
357
van der Sluis F., L. van den Broek E. and Dijkstra T..
TOWARDS AN ARTIFICIAL THERAPY ASSISTANT - Measuring Excessive Stress from Speech.
DOI: 10.5220/0003175203570363
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2011), pages 357-363
ISBN: 978-989-8425-34-8
Copyright
c
2011 SCITEPRESS (Science and Technology Publications, Lda.)

Table 1: Some Stress-Related Psychiatric Disorders.
Post-Traumatic Stress Disorder (PTSD) is caused by a severe trauma, originating from a range of situations;
e.g., warfare, natural disasters, inter-personal violence such as sexual, physical, and emotional abuse, intimate
partner violence, and collective violence. Key characteristics of PTSD are a persistent reexperience of the
stressor, and persistent symptoms of increased arousal (American Psychiatric Association, 2000).
Depression cannot always be related to a specific cause, though several contributing factors have been identi-
fied: e.g., genetic vulnerability and unavoidability of stress. More specific, certain stressful life events (e.g.,
job loss, widowhood) can lead to a state of depression. Furthermore, chronic role-related stress is significantly
associated with chronically depressed mood (Kessler, 1997). Important to note is that the experience of stress
is associated with the onset of depression, and not with the symptoms of depression (American Psychiatric
Association, 2000).
Insomnia often has a fairly sudden onset caused by psychological, social, or medical stress. Though, in some
cases, it may develop gradually and without a clear stressor. Insomnia is characterized by sleep deprivation,
and associated with increased physiological, cognitive, or emotional arousal in combination with negative
conditioning for sleep (American Psychiatric Association, 2000).
stress-related psychiatric disorders. Although not an
exhaustive list, this overview illustrates how differ-
ent aspects of stress can explain different disorders.
For example, depression and insomnia have a strong
appraisal component, whereas PTSD is mainly ex-
plained by a severe stressor. Moreover, Table 1 high-
lights the temporal course of the stressor as well as
the stress response. Although the actual stressor can
be both acute and chronic, there is a chronic stress
response for all diseases; either at the onset (e.g., de-
pression) or as a symptom (e.g., PTSD).
In general, the diagnosis of stress-related psychi-
atric disorders is, amongst other methods, performed
with a careful interview (American Psychiatric Asso-
ciation, 2000). During this interview, the clinician
has to determine if the patient suffers from exces-
sive stress. Moreover, the clinician has to identify the
possible stressor causing an excessive stress response.
Hence, a key diagnostic task is to determine whether
or not the patient suffers from excessive stress in re-
lation to specific stressors.
The diagnosis of excessive stress is repeated dur-
ing treatment as well, in order to indicate the progress
of the treatment. Depending on the treatment type,
this diagnostic repetition can even be part of the
treatment itself. (Everly, Jr. and Lating, 2002)
differentiate between three therapeutic genres: 1)
avoid/minimize/modify stressors; 2) reduce excessive
arousal and organ dysfunction; and 3) ventilate or
express the stress response. The latter incorporates
a repeated expression of the stress response and re-
quires a repeated measurement of it; for example, as
is done with the treatment of PTSD. Technology is
beginning to play a more significant role in the treat-
ment of stress disorders, evidenced by a new treat-
ment method of self-help and minimal contact thera-
pies which has proven to be succesful for certain types
of patients (Newman et al., 2010).
Currently, the measurement of excessive stress
is problematic. A clinician uses diagnostic criteria
based on a range of questionnaires to support this aim.
Introspection and the expert opinion of the clinician
are at the basis of these tools. Inherently, subjective
measures can be unreliable. Moreover, these ques-
tionnaires can be a burden for the patient.
The aim of the study is to lay the foundation for
an Artificial Therapy Assistant (ATA), capable of as-
sisting therapists through an objective measurement
of stress. Moreover, such a system can be useful
for minimal-contact or self-help interventions as well
(Newman et al., 2010). The next section will identify
the prerequisites that had to be taken into account for
this system. After that, in Section 3, a clinical study of
objective stress measurement will be introduced. This
study involved the participation of patients suffering
from a PTSD, which enabled the salient determina-
tion of stress characteristics and, with that, an indica-
tor of stress. Section 4 presents the results obtained
through this study and defines a model that can serve
as the foundation for an ATA. Finally, in Section 5 we
discuss the contribution of this work to the diagnosis
and treatment of stress disorders.
HEALTHINF 2011 - International Conference on Health Informatics
358

2 CONSIDERATIONS
AND SPECIFICATIONS
The aim of the study was an agent that is able to sup-
port psychiatrists and psychologists in their diagnosis
of excessive stress. Key to this system is the mea-
surement of signals indicative of emotions, in partic-
ular of stress, and the determination of intensity. It is
the intensity that can help the therapist in determining
whether or not the patient is suffering from an exces-
sive stress response. As such, the agent aims to sup-
port the decision of the clinician, contrary to giving a
decision itself.
It is known from literature that multiple physi-
cal sources can be applied as stress indicator (Lader,
1975; van den Broek et al., 2010). This research
elaborates on speech, which has a number of advan-
tages: i) In therapy sessions, speech is often already
recorded. Hence, using speech requires no additional
effort for the therapists; ii) Speech processing is fully
unobstrusive; and iii) There is fairly little noise in the
speech signal, as therapy sessions are generally held
in a controlled environment.
2.1 Feature Extraction
For the following features there is a fair amount of
support for their affective information: pitch, energy,
high-frequency energy, and to a lesser extent zero-
crossings rate (Kedem, 1986; Scherer, 2003; El Ayadi
et al., xxxx). Although there is no general concen-
sus on the best features for stress detection, there is
substantial evidence for these. Hence, they extracted
from the audio signal.
For a domain [0,T ], consisting of N number of
samples, the energy of the speech signal is defined as:
20 log
10
1
P
0
s
1
N
N−1
∑
n=0
x
2
(n), (1)
where the amplitude or sound pressure of the signal
is denoted in Pascals (Pa) as x(n) and the auditory
threshold P
0
is 2 ·10
−5
Pa (Boersma and Weenink,
2006). The energy of the speech signal is also de-
scribed as the Sound Pressure Level (SPL). It is
expressed in decibels (dB) relative to the auditory
threshold P
0
; i.e., in dB (SPL).
To extract speech’s high-frequency energy (i.e.,
the energy for the domain [1000,∞] in Hz), the sig-
nal first has to be transformed to the frequency do-
main (Banse and Scherer, 1996). This is done by a
fast Fourier implementation of the discrete Fourier
transform. The discrete Fourier transform (Lyons,
2004):
X(m) =
1
N
N−1
∑
n=0
x(n)e
−j2πnm/N
, (2)
with j representing the
√
−1 operator and where m
relates to frequency by f (m) = m f
s
/N. Here, f
s
is
the sample frequency and N is the number of bins.
The number of bins typically amounts to the next
power of 2 for the number of samples being ana-
lyzed; e.g., 2048 for a window of 40 msec. sampled
at 44100 Hz. The energy for the domain [M
1
,M
2
],
where f (M
1
) = 1000Hz and f (M
2
) = f
s
/2 (i.e., the
Nyquist frequency), is defined by:
20 log
10
1
P
0
v
u
u
t
1
M
2
−M
1
M
2
∑
m=M
1
|X|
2
(m). (3)
The F0 or pitch is extracted using the autocor-
relation method. The autocorrelation is the cross-
correlation of the signal with itself, where the cross-
correlation denotes the similarity between two signals
as a function of a time-lag between them. The auto-
correlation R of signal x at time lag m is defined as:
R
x
(m) =
N−m−1
∑
n=0
x(n +m)x(n) (4)
where N is the length of the signal. The autocorrela-
tion is then computed for each time lag m over the do-
main M
1
= 0 and M
2
= N −1. The global maximum
of this method is at lag 0. The local maximum beyond
0, lag m
max
, represents the fundamental frequency, if
its normalized local maximum R
x
(m
max
)/R
x
(0) (its
harmonic strength) is large enough (e.g., above .45).
The fundamental frequency is derived by 1/m
max
. We
refer to (Boersma, 1993) for a detailed description of
the (implementation of) the F0 extraction.
The zero crossings rate of the speech signal is also
computed. This is defined as:
1
N
N−1
∑
n=1
I
{
x(n)x(n −1) < 0
}
, (5)
where N is the number of samples of the signal ampli-
tude x. The I
{
α
}
serves as a logical function (Kedem,
1986).
3 CLINICAL STUDY
The exact relation between the identified features of
speech and stress is as yet unclear. Two problems
make it hard to compare most previous studies and
methods on stress detection. First, many studies use
mimicked emotions instead of true emotions as the
TOWARDS AN ARTIFICIAL THERAPY ASSISTANT - Measuring Excessive Stress from Speech
359
basis of their model of stress (i.e., acted vs. expe-
rienced emotions). Second, since there is often no
ground truth, it is unclear if the measured vocal pa-
rameters represent an (induced) affective state. For
more information on these problems, see (Scherer,
2003). To arrive at an acoustic stress indicator, this
section presents a study of stress in speech, dealing
with the two identified problems.
The study consisted of two phases, triggering ei-
ther a happy or an anxious state in the patients. Hence,
anxiety was the stressful emotion chosen to induce
stress. The order of sessions was counterbalanced
over the participants. 25 Female PTSD patients (mean
age: 38) participated voluntarily. An informed con-
sent was signed by all participants. Having PTSD pa-
tients as participants had several advantages. First,
PTSD patients are relatively sensitive to stress and,
thus, to stressors. Hence, they were expected to react
more intensively to the emotion elicitation. Second,
within the context of this study, the use of real pa-
tients increases the ecological validity.
The patients had to read two stories aloud, one of
an anxious and one of a happy situation. To prevent
any interfering factors the stories were kept similar on
their syntactic structure and their complexity. More-
over, the order of the stories was counterbalanced over
all participants. Before the patients started with the
emotion inducing stories, they read a sample story to
familiarize themselves with the task.
The stories served as emotional Stroop tasks
(Williams et al., 1996), since they included words
that induced either anxiety or a happy emotional state.
Emotional Stroop tasks are frequently used in clinical
psychology and psychiatry research and are accepted
as a reliable method for eliciting emotions. Emo-
tional Stroop tasks can be defined as the presentation
of stimuli that are expected to evoke emotions, due to
an attentional bias of the participants. In this research,
the Stroop effect was achieved through anxiety trig-
gering words incorporated in one of the stories.
To be able to derive stress from speech, several
steps had to be performed. First, the signal was
recorded. This was done using a standard PC, a
microphone preamplifier, and a microphone. The
recording’s sample rate was 44.1 kHz, mono chan-
nel, and a resolution of 16 bits. The recordings were
divided into samples of approximately one minute of
speech. This resulted in a one-on-one mapping be-
tween the ground truth (explained furtheron) and the
speech features. Second, other voices and speckle
noise were removed from the recorded signal.
Several features were extracted from the clean sig-
nal; see also Section 2.1. From each of these fea-
tures, a number of statistical parameters were de-
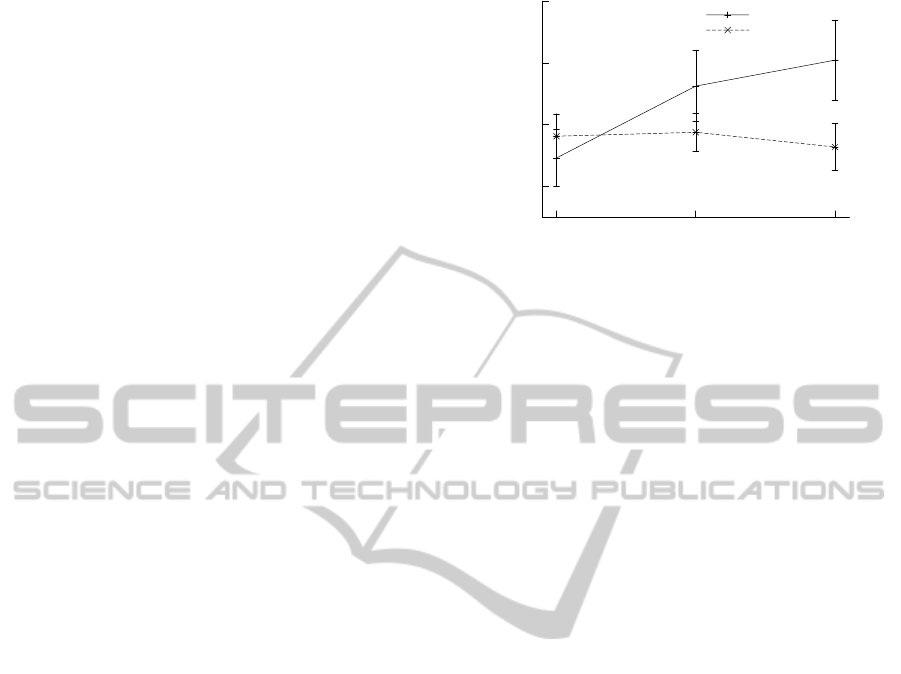
2
3
4
5
1 2 3
SUD
Time (minutes)
Anxiety
Happy
Figure 1: Reported stress per group and time.
rived: mean, median, standard deviation (std), vari-
ance (var), minimum value (min), maximum value
(max), range (max −min), the quantiles at 10%(q10),
90%(q90), 25%(q25), and 75%(q75), the inter-
quantile-range 10%−90% (iqr10, q90 −q10), and the
inter-quantile-range 25% −75% (iqr25,q75 − q25).
All features were computed using a time window of
40 msec. and a step length of 10 msec.; i.e., every 10
msec. over the next 40 msec. of the signal. Next, the
statistical parameters were derived over time chunks
of 60 sec., allowing a one-on-one comparison with the
Subjective Unit of Distress (SUD) data.
To enable the validation of the speech parame-
ters they were compared to a subjective measurement:
the SUD. The SUD is a Likert scale indicative of the
(dis)stress a participant experiences at the moment of
measurement. For this study, a linear scale with range
0 to 10 was used on which the participants were in-
structed to place a cross or a dot. After (Wolpe, 1958)
introduced the SUD, it has proven itself to be a re-
liable measure of one’s emotional state. The partici-
pants used the SUD every minute, making it a routine
task. The SUD was used as ground truth for the de-
rived speech parameters (See Section 2.1).
4 RESULTS
If the manipulation of stress was successful, the re-
sults can be used as a stress indicator. Figure 1 il-
lustrates the mean values of both manipulations and
denotes the confidence intervals without the inter-
subject variance (Cousineau, 2005) through the ver-
tical bars. This figure shows that the manipulation
has been successful. Furthermore, when isolating the
anxiety condition, a trend was visible for time on
SUD scores (F(2,56) = 2.726; p = .07).
In order to create a generic stress indicator, the
most relevant of all features and accompanying pa-
HEALTHINF 2011 - International Conference on Health Informatics
360

rameters were selected. This selection process was
done with a linear regression model (M ). A M ex-
plains how p independent variables (predictors, x)
predict dependent variable y. In order to do so, p
optimal weighting factors Beta (B) over each of the
i = 1,...,n observations are determined:
y
i
= B
0
+ B
1
x
i1
+ ···+ B
p
x
ip
+ ε
i
, (6)
where ε
i
represents unobserved random noise. The
method used to determine the average optimal
weighting factors over all n observations is the ordinal
least squares method. To reduce the number of pre-
dictors, a backward selection algorithm was applied.
Through an iterative process, this algorithm removes
the non-significant predictors (p > .10) for subjective
stress. As the backward method uses the relative con-
tribution to the model as selection criterium, the in-
terdependency of the features is taken into account
as well (Harrell, Jr., 2001). This makes it a robust
method for feature and parameter selection.
The model was created using the SUD scores
of the anxiety and happy conditions (See Figure 1).
Here, a M containing all features and all parame-
ters (i.e., in total 40 predictors), explained 69.72% of
the variance: R
2
= .697 and R
2
= .575, F(40,99) =
5.70, p < .001. Applying the backward selection
method with 22 iterations, leaving 18 predictors, the
model still explained 67.37% of the variance: R
2
=
.674 and R
2
= .625, F(18,121) = 13.88, p < .001.
The model and the used features are described in more
detail in (van der Sluis et al., 2010).
5 DISCUSSION
25 Patients reported stress that had successfully been
caused by reading/telling a carefully created story.
By comparing speech features to a subjective report
of stress, this study defined and evaluated an acous-
tic profile of stress characteristics in speech. The
acoustic profile was shown to explain nearly 70% of
variance in the subjectively reported stress. Hence,
demonstrating the feasability of speech as an objec-
tive measure of experienced stress and, with that, as
an ATA.
Although it is only one of many ways to induce
emotions, storytelling was shown to be particularly
useful in creating an emotion-induced speech signal.
In particular, it is likely to create true emotions, this
contrary to many other commonly used methods. The
triangulation of the SUD and various speech charac-
teristics suggests that indeed true emotions were trig-
gered through the storytelling.
A potential problem with the acoustic stress indi-
cator, as introduced, is described by the existing theo-
retical distinction of emotional and emotive commu-
nication (Caffi and Janney, 1994). Emotional com-
munication is a type of spontaneous, unintentional
leakage or bursting out of emotion in speech, while
emotive communication has no automatic or neces-
sary relation to “real” inner affective states. Emotive
communication is a strategic signaling of affective in-
formation in speaking to interaction partners that is
widespread in interactions; see also (Caffi and Janney,
1994). It uses signal patterns that differ strongly from
spontaneous, emotional expressions and can be both
intentionally and unintentionally accessed (Banse and
Scherer, 1996).
Another issue is the distinction between cognitive
and emotional stress, which is known as the problem
of emotion specificity (Zeelenberg et al., 2008). Emo-
tion specificity distinguishes cognitive stress, the in-
formation processing load placed on the human op-
erator while performing a particular task, and emo-
tional stress, the psychological and physiological ten-
sion due to emotions triggered before or during the
task.
In general, the subjectively reported stress was
somewhat dispersed. This is likely to be partly due
to inter-personal differences and, consequently, indi-
cates that the stories did have an influence. More-
over, a trend was shown for the anxiety inducing story
to create stress over time, supporting this influence.
These results suggest the value as well as the draw-
backs of storytelling. Two problems can be identified:
• inducing an affective state with stories is strongly
dependent on the temporal course; i.e., a story
needs a build-up; and
• there were substantial inter-personal differences
in the experience of the stories.
The latter problem may be useful for diagnostic goals.
Inter-personal differences are likely to be caused by
differences in appraisal. Hence, this can be used
to assess a patient’s appraisal patterns, which have
been identified as a major component for certain psy-
chiatric illnesses; for example, depression (Kessler,
1997).
The explained variance of 70% can be considered
as high, especially considering the number of partici-
pants. Moreover, since the model is not personalized,
some generic chacteristics of stress in speech seem to
be uncovered. However, some restrictions also apply:
• only PTSD patients participated, while other
patient groups might show different stress re-
sponses;
TOWARDS AN ARTIFICIAL THERAPY ASSISTANT - Measuring Excessive Stress from Speech
361

• many stressful emotions have been identified,
these may be different kinds of stress; and
• restrictions applying to storytelling for emotion
elicitation may have influenced the results.
These three restrictions can be seen as future research
challenges. Namely, to use other patient groups, emo-
tions, and emotion elicitation techniques.
Using the acoustic profile, one can arrive at an
ATA for the diagnosis and treatment of stress-related
psychiatric disorders. An ATA can help the clinical
setting in several ways, to:
1. support the measurement of stress responses;
2. give decision support on whether a patient suffers
from excessive stress;
3. aid the treatment of stress disorders; and
4. improve self-help and minimal-contact therapy
methods (Newman et al., 2010).
Through making the measurement objective, the mea-
surement of stress becomes more reliable; i.e., no
longer solely relying on introspection. Objective mea-
surement also increases inter- and intra-expert relia-
bility. Moreover, diagnosis, decision-making in gen-
eral, and treatment could become more fine-grained.
Concluding, an important and significant step to-
wards an ATA for stress-related psychiatric disorders
has been made. This study has shown that an objec-
tive measurement of stress through speech is feasible.
Par excellence, the feasibility of objective stress mea-
surement illustrates the possibility of more objective
measures for the generally subjective fields of psy-
chology and psychiatry.
ACKNOWLEDGEMENTS
We gratefully acknowledge the PTSD patients for vol-
untarily participating in this research. We thank Lynn
Packwood for proof reading this article.
REFERENCES
American Psychiatric Association (2000). DSM-IV-TR: Di-
agnostic and Statistical Manual of Mental Disorders.
Washington, DC, USA: American Psychiatric Pub-
lishing, Inc., 4 (Text Revision) edition.
Banse, R. and Scherer, K. R. (1996). Acoustic profiles in
vocal emotion expression. Journal of Personality and
Social Psychology, 70(3):614–636.
Boersma, P. (1993). Accurate short-term analysis of the fun-
damental frequency and the harmonics-to- noise ratio
of a sampled sound. In Proceedings of the Institute of
Phonetic Sciences, volume 17, pages 97–110. Univer-
sity of Amsterdam.
Boersma, P. P. G. and Weenink, D. J. M. (2006). Praat
4.0.4. http://www.praat.org (Last accessed on Octo-
ber 22, 2010).
Caffi, C. and Janney, R. W. (1994). Toward a pragmatics of
emotive communication. Journal of Pragmatics, 22(3–
4):325–373.
Cohen, P. R. and Oviatt, S. L. (2002). The role of voice
input for human-machine communication. Proceed-
ings of the National Academy of Sciences (PNAS),
92(22):9921–9927.
Cousineau, D. (2005). Confidence intervals in within-
subject designs: A simpler solution to Loftus and
Masson’s method. Tutorials in Quantitative Methods
for Psychology, 1(1):42–46.
El Ayadi, M., Kamel, M. S., and Karray, F. (xxxx). Survey
on speech emotion recognition: Features, classifica-
tion schemes, and databases. Pattern Recognition, [in
press].
Everly, Jr., G. S. and Lating, J. M. (2002). A clinical guide
to the treatment of the human stress response. The
Plenum series on stress and coping. New York, NY,
USA: Kluwer Academic / Plenum Publishers, 2nd edi-
tion.
Harrell, Jr., F. E. (2001). Regression modeling strategies
– with applications to linear models, logistic regres-
sion, and survival analysis. Springer Series in Statis-
tics. New York, NY, USA: Springer-Verlag New York,
Inc., 1st; 6th printing edition.
Kedem, B. (1986). Spectral analysis and discrimina-
tion by zero-crossings. Proceedings of the IEEE,
74(11):1477–1493.
Kessler, R. C. (1997). The effects of stressful life
events on depression. Annual Review of Psychology,
48(1):191–214.
Lader, M. (1975). The psychophysiology of mental illness.
London, Great Britain: Routledge & Kegan Paul Ltd.
Lazarus, R. S. (1993). From psychological stress to the
emotions: A history of changing outlooks. Annual
Review of Psychology, 44(1):1–22.
Lyons, R. G. (2004). Understanding Digital Signal Process-
ing. Upper Saddle River, NJ, USA: Prentice Hall PTR,
2nd edition.
Newman, M. G., Szkodny, L. E., Llera, S. J., and Prze-
worski, A. (2010). A review of technology-assisted
self-help and minimal contact therapies for anxiety
and depression: Is human contact necessary for ther-
apeutic efficacy? Clinical Psychology Review, [in
press].
Scherer, K. R. (2003). Vocal communication of emotion:
A review of research paradigms. Speech Communica-
tion, 40(1–2):227–256.
Van den Broek et al., E. L. (2009/2010). Prerequisites
for Affective Signal Processing (ASP) – Parts I–IV.
In Fred, A., Filipe, J., and Gamboa, H., editors,
BioSTEC 2009/2010: Proceedings of the Interna-
tional Joint Conference on Biomedical Engineering
HEALTHINF 2011 - International Conference on Health Informatics
362

Systems and Technologies, pages –, Porto, Portugal
/ Valencia, Spain. INSTICC Press.
Van der Sluis, F., van den Broek, E. L., and Dijkstra, T.
(2010). Towards semi-automated assistance for the
treatment of stress disorders. In HealthInf 2010: Pro-
ceedings of the Third International Conference on
Health Informatics, pages 446–449, Valencia, Spain.
INSTICC Press.
Williams, J. M. G., Mathews, A., and MacLeod, C. (1996).
The emotional Stroop task and psychopathology. Psy-
chological bulletin, 120(1):3–24.
Wolpe, J. (1958). Psychotherapy by reciprocal inhibition.
Stanford, CA, USA: Stanford University Press.
Zeelenberg, M., Nelissen, R. M. A., Breugelmans, S. M.,
and Pieters, R. (2008). On emotion specificity in deci-
sion making: Why feeling is for doing. Judgment and
Decision Making, 3(1):18–27.
TOWARDS AN ARTIFICIAL THERAPY ASSISTANT - Measuring Excessive Stress from Speech
363
