
TOUCH’N’DOCUMENT
A Nutrition Management System on an NFC-tagged TFT-display
Philip Koene
1
, Felix Köbler
1
1
Technische Universität München, Boltzmannstr. 3, 85748 Garching bei Müchen, Germany
Jan Marco Leimeister
2
, Helmut Krcmar
1
2
Kassel University, Nora-Platiel-Str. 4, 34127 Kassel, Germany
Keywords: Telemedicine, Near field communication, Electronic data capture, Nutrition management.
Abstract: Self-reporting of patient data is a valuable tool for data capture in clinical trial studies and to support
ailment treatment. However, traditional paper-based self-reporting is cost- and time-consuming and
consequently suffers from low patient compliance. NFC-based electronic data capture methods allow a
quick and easy self-reporting for patients and the real-time presentation of patient data enables direct
medical intervention by physicians. Malnutrition, for example can be attenuated by continuous medical
supervision of nutrition data. Consequently, we introduce an NFC-based prototype system called
Touch’n’Document (TnD) that supports automatic aggregation and measurement of self-reported nutrition
status. The hardware of TnD consists of a TFT-display that was outfitted with an array of NFC-tags on the
backside. These allow an NFC-enabled mobile phone to be used as an input device to any software system,
running on the TFT-display. The patients simply have to touch the display with their mobile device to log
into the system and report and analyze their current nutrition. This ensures an adequate usability of the
nutrition management system, especially for non tech-savvy or physically impaired patients, consequently
increasing patient compliance. The technical feasibility, benefits, limitations and future research prospects
of the prototype system are discussed in this manuscript.
1 INTRODUCTION
Patients suffering from chronic diseases, e.g.,
dementia, Parkinson´s disease, motor neuron
diseases, such as amyotrophic lateral sclerosis (ALS)
and Multiple Sclerosis or spinal and bulbar muscular
atrophy (SBMA), often have to cope with limitations
and a reduced quality of life. In particular, patients
diagnosed with a motor neuron disease suffer from
progressive paralysis. Therefore patients are
seriously affected by an insufficient dietary intake
which in the long run leads to an (unnoticed)
reduction of weight due to malnutrition or cachexia
(Cleveland and Rothstein, 2001). The loss of weight
is affiliated with high morbidity and mortality, and
negatively affects the quality of life (Desport, Preux,
Truong, J. M. Vallat, Sautereau et al., 1999) of
patients and family members. Due to medical
complications and social consequences, malnutrition
and cachexia are of significant socio-economic
importance (Ludolph, 2006). In many cases,
supplementary nutrition by increased calories or the
use of percutaneous endoscopic gastrostomy (PEG)
tubes for enteral nutrition becomes inevitable in the
course of most motor neuron diseases. This
intervention not only causes a dramatic decrease in
patients’ quality of life (Löser, Lübbers, Mahlke and
Lankisch, 2007) but significantly affects personal,
logistical and financial expenditures for service
providers, as well as insurance and funding agencies.
The total financial impact on the German public
health and welfare system caused by malnutrition is
estimated to 17 billion Euros while the annual costs
for enteral nutrition amount to a total of
approximately 15,000 Euros (Löser et al., 2007) per
patient and year. This estimation excludes additional
costs of complex care expenses which result to total
expenditures of 50,000 Euros per patient and year
(Schauder, 2006).
In order to guarantee highly qualitative treatment
329
Koene P., Köbler F., Leimeister J. and Krcmar H..
TOUCH’N’DOCUMENT - A Nutrition Management System on an NFC-tagged TFT-display.
DOI: 10.5220/0003172803290336
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2011), pages 329-336
ISBN: 978-989-8425-34-8
Copyright
c
2011 SCITEPRESS (Science and Technology Publications, Lda.)

procedures, attending physicians need to be
adequately supplied with information regarding their
patients’ actual state and well-being. The differing
logistic challenges of capturing, archiving, analyzing
and interpreting health status information in routine
clinical practice are well recognized (Wolfe and
Pincus, 1995). For patients with impaired motor
control, resulting from chronic or motor neuron
diseases, this implies an even greater challenge, as
patients are usually living at home and relevant
contemporaneous information supporting the
therapeutic decision-making is not available in real
time.
Therefore, the objective of our work is to provide
a simple, effective and efficient electronic data
capture (EDC) system, which can be used by
patients with impaired fine motor skills by using a
mobile phone implementing Near Field
Communication (NFC) technology. NFC is an
extension of the ISO/IEC 14443 (ISO/IEC, 2000)
proximity-card standard (such as contactless card,
RFID, etc.) that allows data exchange between
devices that are about four inches apart.
The motivation for the underlying prototype
derives from the unobtrusive integration of
applications following ambient assistant living
(AAL) concepts into everyday life environments-
enabled by radio frequency identification (RFID) -
for the purpose of real time and accurate data
collection. RFID technology features seamless and
non-intrusive integration of novel applications and
services into everyday life environments (Köbler,
Koene, Goswami, Leimeister and Krcmar, 2010,
Köbler, Koene, Krcmar, Altmann and Leimeister,
2010, Leimeister, Knebel and Krcmar, 2007,
Resatsch, Sandner, Leimeister and Krcmar, 2008,
Uhrich, Sandner, Resatsch, Leimeister and Krcmar,
2008) and thus supporting AAL environments. In
addition, mobile networks allow a flexible, location-
independent monitoring of the patients in real time.
An intelligent EDC system thus can improve
productivity of medical processes not only by being
more cost efficient, but also by accounting for
improved standards of medical care as well as
quality of life.
In the subsequent chapters we will first give an
overview of related research on NFC technology and
EDC methods, used in clinical trials, patient care
and AAL scenarios. We then elaborate on the
Touch’n’Document (TnD) prototype system, its
functionalities, application environment and
technical implementation, along with a potential use
case scenario. The benefits of the proposed system
for patient self-reporting and EDC in ailment
treatment are presented. We close with a discussion
of the contributions from this research, its
implications and the derived recommendations for
future research on contactless electronic capture of
self-reported patient data for different use cases
(e.g., fitness and dietary programs).
2 RELATED WORK ON EDC IN
HEALTH CARE
A vast number of literature elaborates on various
occurrences of EDC for the acquisition of
quantitative and qualitative data in surveys
(Bischoff-Ferrari, Vondechend, Bellamy and
Theiler, 2005, Blake H., 2008, Dale and Hagen,
2007, Palmblad and Tiplady, 2004, Richter, Nixdorf,
Koch, Schneider, Becker et al., 2006). A number of
studies (El Emam, Jonker, Sampson, Krleza-Jerić
and Neisa, 2009, Hyde, 1998) document the basic
advantages of EDC in panel surveys and trial
studies, which are the decrease in costs and increase
in data quality due to the digital form of data
collection.
Another set of advantages of EDC are brought to
bear within the domain of clinical and population
sciences, including medicine, health-care, health
services, epidemiology and demography. These
areas of research often “depend on self-reported
states, characteristics and behaviours” (Stone,
Shiffman, Atienz and Nebeling, 2007) of patients in
order to understand, e.g., disease progression,
treatment outcomes or gerontological requirements.
Self-reporting is described as “the only window on
the inner states” (Schwarz, 2007) of patients. In
comparison to traditional, paper-based
questionnaires, the application of EDC for the self-
reporting of patient data is shown to increase the
patient´s compliance, since it “has the potential to
dramatically reduce the time taken to acquire (…)
data” (Nyholm, Kowalski and Aquilonius, 2004).
Electronically captured, self-reported patient data
can furthermore be compiled in real-time and thus
provide cues for possible medical interventions
(Velikova, Wright, Smith, Cull, Gould et al., 1999).
Clinical trial studies, an area of widespread EDC
application, currently see a noticeable trend going
from remote, web-based data entry by the patients or
care-personnel to a direct capture of the data using
barcode scanning, or most recently, NFC or RFID
tags. This allows further improvement of generated
data quality and enables cost-reduction (Hyde, 1998,
Morak, Hayn, Kastner, Drobics and Schreier, 2009,
Smith and Offodile, 2002) . The application of RFID
HEALTHINF 2011 - International Conference on Health Informatics
330

technology for data capture in retail business
processes, solving complex tracking and tracing
problems of objects within the supply chain, is well
documented (Fleisch and Thiesse, 2007, Knebel,
Leimeister and Krcmar, 2007, Loebbecke and
Palmer, 2006, Murphy-Hoye, Lee and Rice, 2005).
More recent publications also describe the
employment of RFID-based EDC for marketing
purposes, either from a consumer and retail
perspective (Resatsch, Karpischek, Sandner and
Hamacher, 2007) or focusing on the generation of
media usage data, vital to for publishers and
advertisers (Koene, Köbler, Burgner, Resatsch,
Sandner et al., 2010).
Employing NFC technology for the capture of
self-reported patient data in disease and ailment
treatment is an emerging practice without
widespread application. Fikry (2006) and Morak
(2009) employ NFC technology for the collection of
medical data in hospitals. Their systems envision
hospital personnel touching medical devices with
NFC-enabled mobile phones for the purpose of data
capture. The prototype system, described by Lahtela
(2008) is an NFC-based solution for the control and
distribution of medication in hospitals. The data
acquisition with the mobile device is conducted in
these systems exclusively by health-care personnel
and only within medical facilities, limiting their
suitability for long term disease and ailment
treatment that commonly involves patients, residing
at home. However, Iglesias (2009) describe a NFC-
based health monitoring system for elderly patients,
that can be conducted as a self-management process,
using mobile communication technology at home.
The authors concentrate however, on the capture of
vital signs and parameters like weight or blood
pressure with their proposed system solution and
exclude self-reported, subjective patient data. A
similar concept with similar limitations is developed
by Morak (2007) for the monitoring of heart failure
patients.
Few research projects focus on the support of
ailment treatment through electronic capture of self-
reported patient data on disease progression
(Nyholm et al., 2004), quality of life (Velikova et
al., 1999) or nutrition management (Denning,
Andrew, Chaudhri, Hartung, Lester et al., 2009,
Jarvinen, Jarvinen, Lahteenmaki and Sodergard,
2008, Siek, Connelly, Rogers, Rohwer, Lambert et
al., 2006). Nyholm et al. (2004) and Siek et al.
(2006) implement EDC systems by employing
mobile communication technology, highlighting the
increased patient compliance, when compared to
paper-based self-reporting, and the convenient, real
time access to patient data for medical personnel.
However, none of those research projects tap into
beneficial effects of NFC technology on the usability
of mobile applications.
Therefore this research paper presents the
Touch’n’Document (TnD) nutrition tracking
prototype application for patient self-reporting via
NFC technology. The TnD prototype is designed to
enable easy and highly usable electronic self-
reporting of patients´ nutritional data with the goal
of providing cues to physicians for possible medical
interventions in between practice appointments.
3 THE TOUCH’N’DOCUMENT
PROTOTYPE SYSTEM
Before we outline the technical solution of the
nutrition management prototype system, we will
describe the application environment, use case, basic
features and functionality of the prototype.
The application environment for the conceptual
prototype builds on GSM cellular phones equipped
with NFC antennas, mobile internet broadband
connectivity enabled through EDGE or UMTS
technologies and sufficient display measurements.
These mobile telephones interact with NFC-tags
(e.g., Mifare Ultralight, Standard 1k and DESfire)
attached to the backside of the screen of a standard
TFT-display in combination with a personal
computer equipped with Internet connection. The
personal computer is connected to a web server,
running the nutrition management system.
3.1 Use Case Scenario
In the following a use case scenario for a possible
employment of the presented TnD prototype or
similar applications is outlined:
Several months ago, John was diagnosed with spinal
and bulbar muscular atrophy (SBMA), which started
with a hypotension and atrophy of his musculature
in his upper legs and hip area. In addition to the
diagnosis, John has shown a tendency to be
overweight since his adolescence. His attending
physician, Dave, advises him to reduce his weight by
a long-term adjustment of nourishment to
cholesterol-low whole food. Dave knows that in
some cases of SBMA, patients tend to resort to
extreme measures to control their body weight, e.g.,
starvation diets and fasting cures, which can be
potentially dangerous for the patient and should be
avoided. In a therapy session, Dave reports to John
TOUCH'N'DOCUMENT - A Nutrition Management System on an NFC-tagged TFT-display
331

about a new nutritional management system (TnD),
featuring the simple and uncomplicated possibility
of recording and analyzing daily nourishment. The
physician devises a nutrition plan, setting and
documenting daily lower and upper limits of calorie
and cholesterol intake within the TnD system.
Although John has never been interested in technical
equipment in his life, he is fascinated by the non-
intrusive integration of this new system: all
functionalities are operated from his mobile phone
by touching an NFC-tag equipped TFT displaying
food icons. Touching the screen twice is sufficient to
send nutrition data to the system, which is then
processed for the attending physician and patient.
Dave has set a minimum and maximum limit for
calories within the system. This enables the system
to warn the physician, patient and care giver of a
possible malnutrition or supernutrition of the
patient. Through the constant supervision and
guidance from his physician, enabled by the TnD
self-reporting, John was able to continuously reduce
his weight over the last months.
A potential prototype system and its implemented
functionalities that support the described health care
environment are described in the following chapters.
3.2 Prototype Functionality
The current prototype system provides a simple set
of features:
Figure 1: Interaction Process of the TnD prototype system.
1. The user can log into the nutrition management
system and can operate it through a simple touch-
based interface. She uses his cell phone to touch the
specific area on the TFT-display and her cell phone
gives a short haptic and visual feedback that the
control-input was successful.
2. The nutrition management interface allows her to
select different kinds of food and amounts in order
to specify and log her food intake. For the sake of an
intuitive user interface and a quick interaction, the
selection of food will be example-based. A
comparative study will be necessary to confirm,
whether the results of an example-based input of
nutrition data coincides with the real nutrition intake
within an acceptable margin of error. In this step, the
system could also provide the user with specific
information on food characteristics (e.g., calories
and ingredient information) of his example-based
input of nutritional data.
3. Both user and physician/nutrition manager can
access the nutrition data in the form of reports and
statistics on a web-browser.
From a technical point of view, the data input
component of the prototype is implemented as a
J2ME midlet and Grails web server (see technical
description for details).
3.3 Technical Description
The hardware prototype we constructed for the
nutrition management system consists of a regular
17-inch TFT display that was equipped with NFC-
tags. The display was dismantled and the tags were
attached directly to the back of the Perspex sheet
that distributes the backlighting for the display. The
Perspex layer and the liquid crystal layer of the
display are together approximately half an inch thick
and high quality NFC-tags can be read through
them. The electronics of the TFT-display had to be
moved about one inch away from the back of the
screen to allow operation of the NFC-tags.
The interaction process description in Figure 1
outlines the communication routine of the hard- and
software components of the conceptual nutrition
management system prototype.
The mobile component of the prototype system
is implemented as a J2ME midlet that can facilitate
the communication with the NFC reader of the
mobile device on the one hand and on the other hand
gain access to functions and data of the web server
component through a RESTful API (representational
state transfer application programming interface).
The web server component is implemented as a
HEALTHINF 2011 - International Conference on Health Informatics
332
Grails web server with a Flash graphical user
interface (GUI) (see
Figure 2 and Figure 3). The basic
communication routine of the prototype consists of
four steps (see also
Figure 1). The NFC-tagged
display is connected to a personal computer with a
browser opened and connected to the nutrition
management web server:
1. The user touches the login button or another GUI
element of the nutrition management system
displayed on the TFT-screen with her NFC-enabled
mobile device.
2. The NFC-enabled mobile device reads the
corresponding NFC-tag on the backside of the
display and the J2ME midlet component of the
nutrition management software is started (if not
running already). The midlet sends the ID of the tag
and the ID of the user (stored on the mobile device)
to the nutrition management web server through a
mobile internet connection, using the RESTful API.
3. The web server component looks up the tag ID
and the user ID in its database to determine what
button was pressed and by whom. The GUI (or
login) command is then processed and the GUI is
updated for that specific instance of the nutrition
management system interface.
4. Physicians, nutrition consultants or users with an
affinity to technology can also access the nutrition
management system through a web interface that is
not meant for easy data entry, but for data analysis.
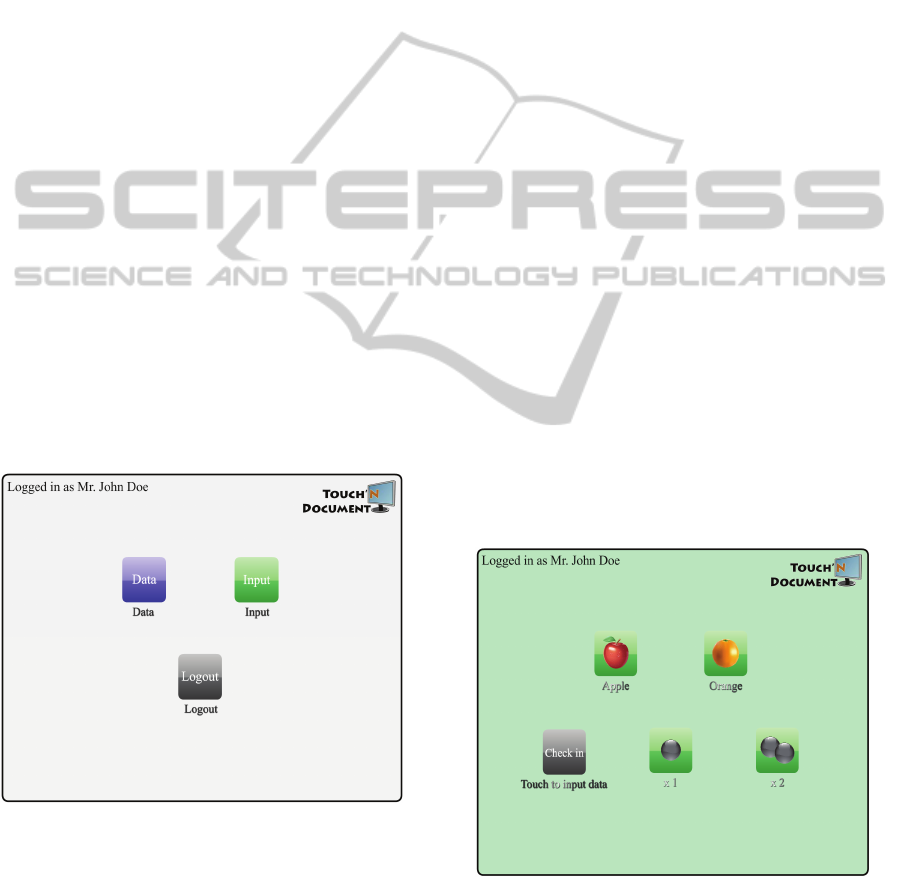
Figure 2: Login-Screen of TnD.
In a next step, we elaborate and discuss the benefits of the
proposed concept in the domain of telemedicine.
4 BENEFITS OF
THE PROPOSED CONCEPT
FOR TELEMEDICINE
The following gives an overview over the major
benefits of the integration of NFC technology,
mobile devices and a client-server-architecture for
telemedicine applications:
The TnD prototype system could be easily
expanded to capture patient data, different from
nutrition data, e.g., weight, heart rate, blood
pressure, quality of life measures, etc.
The utilization of NFC and mobile devices, as
well as the implementation of a client-server-
architecture lowers technological barriers of and
costs for integration in established hospital
information systems (HIS).
The presented prototype solution offers the
possibility for the easy integration of NFC equipped
medical devices such as blood pressure instruments,
for direct capture of medical data.
Novel mobile devices (e.g., smartphones) and
mobile computing devices similar to the Apple iPad
could be enhanced with NFC technology in the near
future and provide users (patients and medical
personnel) with an adequate user interface.
The utilization of mobile devices, in particular of
mobile phones, guarantees an absolute mobile and
ubiquitous data transmission but and additionally
enables a voice channel for real time support for
patients or medical personnel.
Figure 3: Main Menu of TnD.
The TnD prototype provides an intuitive and
secure solution for the user to (1) simple data
capture by touching, to (2) initiate data capturing
TOUCH'N'DOCUMENT - A Nutrition Management System on an NFC-tagged TFT-display
333

and transmitting processes and to (3) secure login
and authentication without entering login and
password information. The usability and
consequently the acceptance of the proposed system
need to be evaluated in further research, however.
In terms of usability, the utilization of mobile
devices and NFC for the capturing of data results in
a: (1) high usability, (2) minimal interaction with the
display and keypad of the mobile device and (3)
avoidance of erroneous data entries.
5 NEXT STEPS AND FUTURE
RESEARCH IDEAS
From a technical point of view, both soft- and
hardware of the data input component of the
nutrition management prototype system demonstrate
the concept of using NFC-tagged TFT-displays in
conjunction with NFC-enabled mobile phones for
simple, efficient and usable data entry. The system is
currently in a refinement phase of the GUI design. In
a next step we plan to setup focus groups with
patients suffering from motor neuron diseases to
collect improvements for the usability and data
capture process. In this step, we additionally plan to
evaluate the degree of functionality that could be
implemented on the mobile device itself, in order to
make the system less dependent on a stationary
desktop personal computer and a fixed or mobile
Internet connection. A field test with a larger
number of participants is continuatively planned to
be conducted in a German hospital specializing on
motor neuron diseases. The evaluation will focus on
technology acceptance and usability of the proposed
prototype system.
Future versions of the hardware device could
serve different purposes, besides a nutrition
management system, for example to capture patient
data different from nutrition data, e.g., weight, heart
rate, blood pressure, quality of life measures.
The prototype system could also be applied in
environments uncoupled form medical use case
scenarios, e.g., supporting and expanding campus
management systems in universities.
We see the proposed prototype system as a first
step and proof of concept, to develop autonomous
and dynamic smart posters by utilizing NFC
technology and electronic ink foil (E-Ink) or organic
light emitting diode displays (OLED) (Payne and
Macdonald, 2004). In our vision, novel dynamic
smart posters are autonomous in the sense that
electronic ink foil in front of the NFC-tags of the
smart poster is charged by using power of the mobile
device through an adapter or induction and that the
data displayed on this electronic ink foil is requested
through the internet link of a mobile device from a
server. This technical setup allows a dynamic mode
of operation, in the sense that the poster can be used
for multiple and different sessions (in contrast to
paper based smart posters) by displaying different
information in front of NFC-Tags, thus changing the
data-input command that is activated by touching
them with an NFC-enabled mobile device.
6 LIMITATIONS
AND CONCLUSION
The TnD prototype system can enhance the
productivity of telemedicine processes by improving
the information logistics between the involved
stakeholders in nutrition management, thus fulfilling
the seamless healthcare paradigm, postulated by
Schweiger (2007). With TnD, an active participation
and integration of patients into ailment treatment
processes, a better documentation of disease
progression and therefore an improved
communication basis for treatment and nursing can
be achieved. Furthermore, we predict, that the
proactive participation of malnutrition patients,
while recording their nutrition status, can foster their
ability to cooperate in the treatment and consultation
processes by enabling a deeper understanding of the
disease and condition itself. Our results at present
and the prognosticated benefits of the TnD system
are, however, not yet verified in a real world setting.
Beyond this stage, studies are necessary to evaluate
the acceptance of the proposed system by patients,
family members, care personnel, physicians and
funding agencies. In addition, the effects of the
proposed system on patient compliance with
nutrition plans and in a second step the
consequences of an improved nutrition situation for
the progression of, e.g., motor neuron diseases need
to be assessed. For further iterations of the prototype
system, issues like data security and privacy,
robustness, stability and scalability will be subject to
close scrutiny.
ACKNOWLEDGEMENTS
The Touch’n’Document prototype was developed in
the context of the research project Mobile
HybriCare. Mobile HybriCare is funded by the
HEALTHINF 2011 - International Conference on Health Informatics
334

German Federal Ministry of Education and Research
(BMBF - FKZ: 01FG08001). It is a joint project of
the Technische Universität München and various
partners. For further information, see
www.mobilehybricare.de.
REFERENCES
Bischoff-Ferrari, H. A., Vondechend, M., Bellamy, N. and
Theiler, R. (2005). Validation and patient acceptance
of a computer touch screen version of the WOMAC
3.1 Osteoarthritis Index. Ann Rheum Dis., 64, 80-84.
Blake H. (2008). Innovation in practice: mobile phone
technology in patient care. Br J Community Nurs., 13,
160,162-616.
Cleveland, D. W. and Rothstein, J. D. (2001). From
Charcot to Lou Gehrig: deciphering selective motor
neuron death in ALS. Nature Reviews Neuroscience,
2, 806-819.
Dale, O. and Hagen, K. B. (2007). Despite technical
problems personal digital assistants outperform pen
and paper when collecting patient diary data. J Clin
Epidemiol, 60, 8-17.
Denning, T., Andrew, A., Chaudhri, R., Hartung, C.,
Lester, J., Borriello, G. and Duncan, G. (2009).
BALANCE: towards a usable pervasive wellness
application with accurate activity inference.
Proceedings of the 10th workshop on Mobile
Computing Systems and Applications, Santa Cruz,
California, ACM, 1-6.
Desport, J., Preux, P., Truong, T., J. M. Vallat, Sautereau,
D. and Couratier, P. (1999). Nutritional status is a
prognostic factor for survival in ALS patients.
Neurology, 53, 1059-1063.
El Emam, K., Jonker, E., Sampson, M., Krleza-Jerić, K.
and Neisa, A. (2009). The use of electronic data
capture tools in clinical trials: Web-survey of 259
Canadian trials. Journal of Medical Internet Research,
11, e8.
Fikry, M., Karim, A. and Muhamad, R. (2006). Integration
of Near Field Communication (NFC) and Bluetooth
Technology for Medical Data Acquisition System
Computational Geometry & Artificial Vision, 147-
152.
Fleisch, E. and Thiesse, F. (2007). On the Management
Implications of Ubiquitous Computing: An IS
Perspective. In Österle, H., Schelp, J. & Winter, R.
(Eds.) 15th European Conference on Information
Systems (ECIS2007), St. Gallen, St. Gallen,
Switzerland, 1929-1940.
Hyde, A. W. (1998). The Changing Face of Electronic
Data Capture: From Remote Data Entry to Direct Data
Capture. Drug Information Journal, 32, 1089-1092.
Iglesias, R., Parra, J., Cruces, C. and Segura, N. G. d.
(2009). Experiencing NFC-based touch for home
healthcare. Proceedings of the 2nd International
Conference on PErvsive Technologies Related to
Assistive Environments, Corfu, Greece, ACM, 1-4.
ISO/IEC (2000). ISO/IEC 14443-1:2000.
Jarvinen, P., Jarvinen, T. H., Lahteenmaki, L. and
Sodergard, C. (2008). HyperFit: Hybrid media in
personal nutrition and exercise management.
Proceedings of the Second International Conference
on Pervasive Computing Technologies for Healthcare,
Tampere, Finland, 222-226.
Knebel, U., Leimeister, J. M. and Krcmar, H. (2007).
Potentials of Tracking and Tracing Technologies - The
Perspective of IT Decision Makers in Germany. In
Österle, H., Schelp, J. & Winter, R. (Eds.) Proceedings
of the 15th European Conference on Information
Systems, St. Gallen, Switzerland, 1766-1777.
Köbler, F., Koene, P., Goswami, S., Leimeister, J. M. and
Krcmar, H. (2010). NFriendConnector - Verbindung
zwischen virtueller und realer sozialer Interaktion. 5.
Konferenz Mobile und Ubiquitäre
Informationssysteme (MMS 2010), Göttingen,
Germany, 139-153.
Köbler, F., Koene, P., Krcmar, H., Altmann, M. and
Leimeister, J. M. (2010). LocaTag - An NFC-Based
System Enhancing Instant Messaging Tools with Real-
Time User Location. Near Field Communication
(NFC), 2010 Second International Workshop on, 57-
61.
Koene, P., Köbler, F., Burgner, P., Resatsch, F., Sandner,
U., Leimeister, J. M. and Krcmar, H. (2010). RFID-
based Media Usage Panels in Supportive
Environments. Proceedings of the 18th European
Conference on Information Systems, Praetoria, South
Africa.
Lahtela, A., Hassinen, M. and Jylha, V. (2008). RFID and
NFC in healthcare: Safety of hospitals medication
care. In Health, C. T. f. (Ed.) Proceedings of the
Second International Conference on Pervasive
Computing Technologies for Healthcare, Tampere,
Finland, 241-244.
Leimeister, J. M., Knebel, U. and Krcmar, H. (2007).
RFID as enabler for the boundless real-time
organisation: empirical insights from Germany.
International Journal of Networking and Virtual
Organsations, 4, 45-64.
Loebbecke, C. and Palmer, J. W. (2006). RFID in the
Fashion Industry: Kaufhof Department Stores AG and
Gerry Weber International AG Fashion Manufacturer.
MIS Quart. Exec., 5, 15-25.
Löser, C., Lübbers, H., Mahlke, R. and Lankisch, P. G.
(2007). Der ungewollte Gewichtsverlust des alten
Menschen. Dtsch Arztebl, 104, 3411.
Ludolph, A. (2006). 135th ENMC International
Workshop: Nutrition in Amyotrophic Lateral Sclerosis
18–20 of March 2005, Naarden, The Netherlands.
Neuromuscular Disorders, 16, 530-538.
Morak, J., Hayn, D., Kastner, P., Drobics, M. and
Schreier, G. (2009). Near Field Communication
Technology as the Key for Data Acquisition in
Clinical Research. First International Workshop on
Near Field Communication, Hagenberg, Austria.
Morak, J., Kollmann, A., Hayn, D., Kastner, P., Humer, G.
and Schreier, G. (2007). Improving telemonitoring of
TOUCH'N'DOCUMENT - A Nutrition Management System on an NFC-tagged TFT-display
335

heart failure patients with NFC technology.
Proceedings of the fifth IASTED International
Conference: biomedical engineering, Innsbruck,
Austria, ACTA Press.
Murphy-Hoye, M., Lee, H. L. and Rice, J. B. J. (2005). A
Real-World Look at RFID. Supply Chain Management
Review, 2005, 18-26.
Nyholm, D., Kowalski, J. and Aquilonius, S.-M. (2004).
Wireless real-time electronic data capture for self-
assessment of motor function and quality of life in
Parkinson's disease. Movement Disorders, 19, 446-
451.
Palmblad, M. and Tiplady, B. (2004). Electronic diaries
and questionnaires: designing user interfaces that are
easy for all patients to use. Qual Life Res., 13, 1199-
1207.
Payne, R. and Macdonald, B. (2004). Ambient
Technology - Now You See It, Now You Don't. BT
Technology Journal, 2004, 119-129.
Resatsch, F., Karpischek, S., Sandner, U. and Hamacher,
S. (2007). Mobile sales assistant: NFC for retailers.
9th international conference on Human computer
interaction with mobile devices and services,
Singapore, ACM, 313-316.
Resatsch, F., Sandner, U., Leimeister, J. M. and Krcmar,
H. (2008). Do Point of Sale RFID-Based Information
Services Make a Difference? Analyzing Consumer
Perceptions for Designing Smart Product Information
Services in Retail Business. Electronic Markets, 18,
216-231.
Richter, J. G., Nixdorf, M., Koch, T., Schneider, M.,
Becker, A. and Monser, R. (2006). Mobile Computing
instead of paper based documentation in German
Rheumatology. Proceedings of the International
Conference on Mobile Business, IEEE Computer
Society, 28.
Schauder, P. (2006). Ernährungsmedizin Prävention und
Therapie. München; Jena: Elsevier, Urban und
Fischer.
Schwarz, N. (2007). Retrospective and concurrent self-
reports: The rationale for real-time data capture. The
science of real-time data capture: Self-reports in health
research, 11–26.
Schweiger, A., Sunyaev, A., Leimeister, J. M. and
Krcmar, H. (2007). Toward Seamless Healthcare with
Software Agents. Communications of the Association
for Information Systems, 19, 692-709.
Siek, K. A., Connelly, K. H., Rogers, Y., Rohwer, P.,
Lambert, D. and Welch, J. L. (2006). When Do We
Eat? An Evaluation of Food Items Input into an
Electronic Food Monitoring Application. Pervasive
Health Conference and Workshops, 2006, 1–10.
Smith, A. D. and Offodile, F. (2002). Information
management of automatic data capture: an overview of
technical developments. Information Management &
Computer Security, 10, 109-118.
Stone, A. A., Shiffman, S., Atienz, A. A. and Nebeling, L.
(2007). The science of real-time data capture: Self-
reports in health research. Oxford University Press,
USA.
Uhrich, F., Sandner, U., Resatsch, F., Leimeister, J. M.
and Krcmar, H. (2008). RFID in Retailing and
Customer Relationship Management. The
Communications of the Association for Information
Systems, 23, 219-234.
Velikova, G., Wright, E. P., Smith, A. B., Cull, A., Gould,
A., Forman, D., Perren, T., Stead, M., Brown, J. and
Selby, P. J. (1999). Automated Collection of Quality-
of-Life Data: A Comparison of Paper and Computer
Touch-Screen Questionnaires. J Clin Oncol, 17, 998-
998.
Wolfe, F. and Pincus, T. (1995). Data collection in the
clinic. Rheum Dis Clin North Am, 21, 321-358.
HEALTHINF 2011 - International Conference on Health Informatics
336
