
HEALTH INFORMATION RETRIEVAL AND USAGE
AMONG THE ELDERLY
Potential use of the Internet and Personal Health Records in Health
Awareness and Accountability
Dennis Cheung
Department of Health Policy and Management, Faculty of Medicine, University of Toronto
155 College Street, Suite 425, M5T 3M6, Toronto, Ontario, Canada
Keywords: ICT, Aging and Disability, Cognitive Informatics, & e-Health for Public Health.
Abstract: As North America anticipates an increase in the number of individuals expected to retire and fall into the
group of “older adults,” questions are raised regarding Canada’s healthcare system and its ability to deal
with this surge in consumption of resources. As the population ages, so too will the demands placed on the
current medical work force thus creating a shortage of medical practitioners available. By utilizing
information technologies such as personal health records (PHRs) and the internet, it is believed that this can
leverage some of the burden away from Canada’s healthcare system. By creating awareness and
accountability among this aging population through the use of ICT (information communication
technologies), cultural and behavioural changes in how this population consumes healthcare resources may
be altered. Not only are behaviours being changed due to ICT, but the way in which consumers are utilizing
resources and knowledge are also shifting. As the medical community is shifting away from the illness
model to that of a more patient centered one, it is important to understand the value of ICT solutions in the
prevention and continued well being of a patient in an economy where resources are scarce.
1 INTRODUCTION
With the change in Canada’s demographics, more
and more individuals are expected to retire and fall
under the group of “older adults” or the “elderly”.
Yet, contrary to popular belief, the increase in the
“older adult” population need not necessarily
translate into a greater strain on Canada’s Healthcare
system. With the common view that aging is directly
correlated to increased healthcare expenditures, it
was observed by Bevand (2010) that only one-third
to half of these expenditures will happen in the final
years of an individual’s life. In other words, it was
noted by Lee (2007) that the increased consumption
of resources is not entirely due to the population
aging (the cost of living of an aging individual), but
rather because of higher rates of mortality as the
population gets older (cost of dying). Nonetheless,
one significant problem does arise from the aging
population, namely, the lower number of available
healthcare practitioners as the population retires and
begins to work less hours (National Center for
Health Workforce Analysis, 2006).
One solution to this would involve the
integration of technology; in particular the Internet
and personal health records (PHRs), in helping to
leverage the shortage of available healthcare
practitioners providing information and guidance.
Coupled with this generation of older adults having
healthier lifestyles than their predecessors (Wiser,
2005), these individuals may not necessary utilize
public healthcare resources in the traditional sense,
of a patient, but rather as consumers wanting to
improve and be accountable for their own health. By
examining some of the current barriers and issues in
how the elderly access and retrieve information on
the Internet, this paper will strive to identify how the
Internet can be used as a health awareness and
information gathering tool. Together with the
introduction of PHRs, this paper will depict how
greater consumer awareness and accountability can
improve the time required with healthcare
practitioners in gathering health information.
205
Cheung D..
HEALTH INFORMATION RETRIEVAL AND USAGE AMONG THE ELDERLY - Potential use of the Internet and Personal Health Records in Health
Awareness and Accountability.
DOI: 10.5220/0003144702050212
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2011), pages 205-212
ISBN: 978-989-8425-34-8
Copyright
c
2011 SCITEPRESS (Science and Technology Publications, Lda.)

2 BACKGROUND
In a report conducted by the National Center for
Health Workforce Analysis, Bureau of Health
Professions, Health Resources and Services
Administration, five main problems were identified
in relation to future healthcare practitioners and an
aging population:
1) Many health profession are aging rapidly
2) Most healthcare professionals receive limited
training on how to care for the elderly
3) Many health professionals lack diversity
4) Future shortages of health workers to serve
the elderly
5) Future demand for health care professionals
to serve the elderly will be affected by many
factors including health insurance
reimbursement policies, emerging
technologies, new models of care, and
changes in profession-specific scope of
practice (National Center for Health
Workforce Analysis, 2006, p.3).
From this, it can be expected that as the
population ages, future trends in healthcare workers
will also change. With a lack of interest in the field
of geriatrics from new graduates in the medical
profession, the numbers of individuals replacing
those retiring are few (Häkkinen, 2009). Couple this
with the fact that the aging population will grow
exponentially over next couple of years, this
shortage of available healthcare practitioners is a
huge problem that must be addressed (Robson,
2001). Not only is a shortage of health professionals
an issue, but given the behavioral change in the
elderly today and those entering retirement, a shift in
consumer and patient needs is occurring
simultaneously. With the aging population today
having more access to information (i.e. the Internet),
and being more health conscious, the elderly may
seek out particular services due to their “higher level
of sophistication (National Center for Health
Workforce Analysis, 2006, p.5).” In a study
conducted by Maynard (1991), it was observed that
as individuals aged, favorable health habits
increased within these individuals, and that they
believed that certain diseases could be prevented
with proper-self management.
With technology being so prevalent today, a
transformation is taking place in the way many
individuals process and access information. From
the complexity of online banking to the simplicity of
using parking machines in paying for parking
tickets, technology has shifted many cultural and
behavioural standards assumed in the past.
Healthcare is of course no different. The Internet has
provided a vast array of information at ones
fingertips, the days of healthcare providers being the
sole vessels of healthcare knowledge have long
dissipated (Campbell, 2005). A paradigm shift is
now taking place within many healthcare systems
across the world whereby the medical model is seen
as outdated, and the days of a physician telling the
patient what to do, are long over (Eysenbach &
Jadad, 2001). Instead, a patient centered model has
emerged whereby the patient and physician are
working together for overall patient well-being.
Consequently many new technologies and web-
based applications were developed around this
patient centered model of care; the most promising,
PHRs and consumer portals. PHRs can be described
as information reservoirs where one completes
medical information is stored and accessible by the
patient 24/7 (Shortliffe, & Cimino, 2006). Even
though there are many challenges associated in
properly developing and using a PHR, the potential
of having a complete record of one’s medical
information in the hands of the patient can have
immense benefits (Kim et al., 2007). Accompanied
with the use of consumer health applications such as
patient portals and online health communities,
individuals can share, collaborate, and exchange
information regarding various health concerns and
issues. By utilizing such tools, elderly individuals
can become more proactive in the involvement of
their own health and take into consideration the
various options prior to accessing public health
resources subsequently reducing the frequency of
physician consultation and, in optimal situations,
eliminating utilization of public health resources for
minor concerns completely.
3 THE INTERNET AND PHRs
AS A CONSUMER AWARENESS
AND ACCOUNTABILITY TOOL
In light of the behavioral changes outlined above,
the Internet, together with PHRs can become tools
for individuals to gain greater knowledge and
accountability in understanding and managing their
own health. However, before examining how
technology can improve consumer awareness and
accountability, it is vital that we have a clear
understanding of how elderly individuals seek
information. In a literature review conducted by
Escamilla (2006), it was found that seniors first tend
HEALTHINF 2011 - International Conference on Health Informatics
206

to turn to their doctors as their primary source of
medical information, and then if all else fails; turn to
the Internet for medical information. Given that on
average, a physician spends only fifteen minutes per
patient, this may not be enough time for seniors to
gather the necessary medical information to make
decisions about their health (Belzer, 1999). Coupled
with findings from the Gladden (2000) study which
reveals that communication between patients and
doctors are often problematic, in that patients often
express dissatisfaction for being labelled as “nosy”
when asking for information.
The Internet can become a great tool in helping
elderly individuals retrieve medical information at a
comfortable pace. Not only does the Internet provide
a timeless space for individuals to retrieve
information, it also provides individuals a place
where they do not feel judged, isolated, or
disempowered (Escamilla, 2006). By empowering
individuals prior to visiting a physician’s office to
ask questions, discuss treatment options, express
opinions, and state preferences during this time, it
has been shown that these individuals have better
health outcomes than those who do not (Campbell &
Nolfi, 2005). In addition, it was noted by Wicks
(2004) that reading was the medium of choice for
many elderly individuals, and that a majority of
individuals use the library to rent books, audio,
videos and participate in library programs. In light of
this, library staff and administrators may be
considered as resources to encourage these same
individuals to try and access information through the
Internet. In a study conducted by Campbell (2005)
on the use of the Internet to gather healthcare
information by the elderly (n = 52), it was found that
86.5% of individuals used the Internet to look up
information. Of this 86.5%, it was further found that
63.5% of these participants who used the Internet for
health information were influenced to change their
current healthcare behaviors (Campbell, 2005). In
another study conducted by Campbell (2003) one
such behavioral change was when individuals were
going to see the doctor, individuals were quoted as
asking “…why I am seeing him in the first place?”
This statement in itself is significant as it points
towards a cultural and behavioral change in how
individuals access healthcare resources. Moreover, it
was further noticed that because participants have
more knowledge and awareness of specific medical
conditions and treatment options, these individuals
had measurably better health outcomes than those
who did not use the Internet (Mahler & Kulik,
1990). In being able to ask specific questions,
treatment options, and having an overall higher
understanding of the different illness and their
ramifications, individuals today play a more
collaborative role with their doctor and allied health
professionals in making important decisions
regarding treatment options (Campbell, 2003). With
75% of respondents from Campbell’s study
(Consumer Informatics: Elderly persons and the
Internet, 2005) reporting playing a collaborative role
in decision making with their physicians. It is hard
to deny that the Internet has significant influence in
creating greater consumer awareness and
accountability with regards to their own health
(Campbell, 2005). As health wellness and other
related material are becoming increasingly
accessible and available on the Internet, older adults
will also become more familiar with using this
medium to retrieve information in self-diagnosis and
remote consultation. In a study conducted by Chou
& Wister (2005), it was observed that lay
information-seeking behaviour could positively
influence health promotion activities for the elderly
population. It was found that elderly participants
(n = 827, age 50+) within this study who would
retrieve and look up information regarding chronic
illness, seek assistance from health professionals,
gain knowledge of community services, and consult
with friends about their own illnesses were more
likely to take action in self-care activities (Chou &
Wister, 2005). Findings from such studies
(Campbell, 2005; Mahler & Kulik, 1990; Campbell,
2003; & Chou & Wister, 2005) help to build on the
empirical evidence that information retrieval can
translate into significant self-care action by those
exposed to ICT. In addition, not only do health
promotion activities increase with the individual,
health outcomes can also improve as elderly patients
remind medical practitioners regarding best practices
and proper treatment methods (Campbell & Nolfi,
2005).
Another popular tool emerging in healthcare
today is the idea and concept of a PHR. PHRs may
be defined as a person’s entire medical history at his
or her access 24/7. PHRs can house different
elements which can include doctor visits, notes,
laboratory results, pharmacy information, diagnostic
images, and other medical information (Sprague,
2006). In an online survey conducted in 2003 by the
Markle Foundation’s Connecting for Health Project,
it was found that those with chronic illnesses
(usually those in the higher age groups) and those
caring for elderly parents reported the highest and
most urgent interest in PHRs. Given such existing
interest in PHRs, the shift in the way individuals
manage and account for their health is already in the
HEALTH INFORMATION RETRIEVAL AND USAGE AMONG THE ELDERLY - Potential use of the Internet and
Personal Health Records in Health Awareness and Accountability
207
midst of a paradigm shift. In a study conducted by
Kim et al. (2007), it was observed that participants
who used PHRs regularly filled in information in the
following elements: 1) medication, 2) health
problems, 3) surgeries, 4) lab tests, 5) allergies, & 6)
immunizations. Of these elements, the most
frequently updated was medication (updated 96% of
the time), which suggests that elderly individuals
recognize the value in recording their medication in
preventing adverse effects. Moreover, the active
updating and use of filling in medication history also
suggests that the elderly know their medication
information reasonably well (Kim et al., 2007).
From this, it can be deduced that individuals, when
given the opportunity will try and manage their own
care, thus displaying accountability in regards to
personal well being. As individuals are becoming
more active in managing their own care, it is no
surprise that these same individuals will also start to
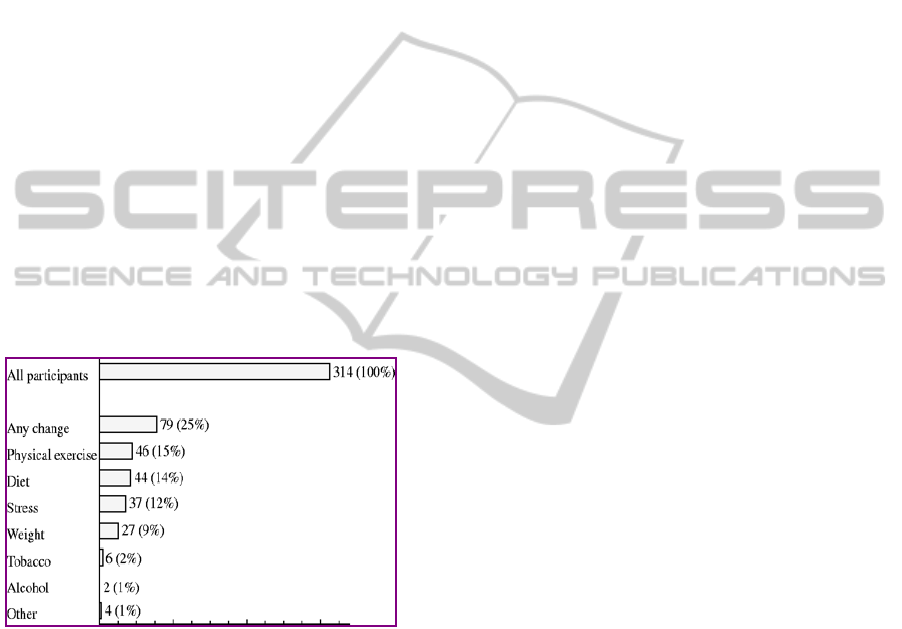
become more aware of their own health condition. In
a study conducted by Jerden & Weinehall (2004), it
was reported that individuals who had access to
patient-held health records did change their
behaviours. Highlighted below in Figure 1 are the
findings from this study.
Figure 1: Percentage and Type of Change in Health
Behaviour (Jerden & Weinehall, 2004).
As seen in Figure 1, there were significant
changes after the implementation of individuals
using patient-held health records. However, due to
the limitations of the study, the most significant
portion, being “any change” could not be further
explored. Overall, physical exercise and diet were
the most common of the health behaviour changes
with fifteen and fourteen percent of participants
reporting a change in their health behaviour. As an
enabling technology, PHRs can aid individuals to
become more actively involved in their own health.
In a national survey conducted by The California
Healthcare Foundation, it was found that 90 percent
of individuals in the United States wanted to be
active partners with physicians, 52 percent wanted to
make final treatment decisions for themselves and
family members, and 38 percent wanted to make
decisions together with their physician (Ball, Smith,
& Bakalar, 2007). Given these statistics, a shift in
consumer behavior has begun as consumers are
taking a more accountable and active role in their
own health. In two studies conducted in the fall of
2005 (McInturff; & Markle Foundation), it was
found that 60 percent of Americans favored the
creation of PHRs and believed that PHRs could
improve safety and convenience. Of this same
group, 69 percent of respondents said that they
would “use it to check for mistakes” in their medical
records and medical prescriptions. Additionally,
another 58 percent said that they would use PHRs to
get lab results over the Internet with 57 percent
stating that they would turn to PHRs to contact and
communicate with their family physicians. As such,
a new trend is emerging in the way people,
especially elderly individuals, manage their own
health. As stated above, with 90 percent of
individuals wanting to be active partners with their
medical practitioners and only 9 percent wanting
physicians to manage their health for them (Ball,
Smith, & Bakalar, 2007). Technologies, in particular
PHRs, have enabled individuals to take affirmative
action in the delivery of care. With the economy as it
is today, the ability for older adults to manage their
own health can translate into savings of hundreds of
dollars on prescription drugs and other health related
expenses through access to information in guiding
them in making healthier lifestyle changes.
Through the use of the two technologies as
highlighted in this section. Elderly individuals today
now have the tools that past generations have long
sought after in assisting to make informed healthcare
decisions. Through awareness and accountability of
their own health conditions and treatment options,
elderly individuals can change their health behaviors
accordingly in order to live longer, and healthier.
4 BARRIERS TO THE INTERNET
AND PHR USE AMONG
THE ELDERLY
Given that the Internet and PHRs have just arrived in
the healthcare field during the last decade or so,
there are of course challenges associated with its
adoption and usage among the elderly. Some
barriers include, though not exclusively: 1) access to
HEALTHINF 2011 - International Conference on Health Informatics
208

a computer and the Internet, 2) computer literacy, 3)
individuals that have the ability to understand and
interpret health information, and 4) that users have
the ability to assess the health information available
to them (Donahue, personal communications, June
07, 2010). In another article by Tang et al. (2006),
two wider range of barriers were discussed which
were characterized as “environmental” and
“individual-level” barriers. Environmental barriers
included organizational, economic, legal, and
privacy concerns while “individual-level” barriers
included items such as workflow models, challenges
to provider autonomy, recognition of value by the
patient, and behavioural changes.
Moreover, from the literature, it was found that
cognitive functionality and physical limitations
among the elderly also played a big part in the
adoption of information technology (IT) and
information communication technology (ICT). In a
study by Lober et al. (2006), it was observed that for
many individuals over the age of 65, cognitive
barriers were prevalent. With 11% of women and
15% of men over the age of 65 having moderate to
severe memory impairment, the ability to navigate
and keep track of what information was inputted and
retrieved would prove to be daunting (Federal
Interagency Forum on Aging Related Statistics,
2008). Furthermore in Lober’s study, it was
observed that as the population ages, physical
limitations begin to limit certain activities. With
21% of the elderly population having visual
impairment, 24% (ages 64-74) and 40% (age 75)
with hearing impairments, and 60% having arthritis
and other rheumatic conditions; this portrays a pretty
clear image in how physical limitations can create
barriers to IT and ICT adoption when individuals
cannot see, hear, or navigate a computer properly
(Lober et al., 2006).
Lastly, another common theme found among the
literature with regards to barriers to the Internet and
PHR adoption, were the terms digital and social
divide. The digital divide being defined as the gap
between individuals owing or knowing how to use
technology, i.e., ICT infrastructure, hardware, and
software, has always been a barrier to adoption (Kim
et al, 2009). Given that low income families or
elderly individuals may not necessarily have the
resources to purchase a computer or accessories to
optimize these online tools, many individuals are left
in the dark. Moreover, accompanied with this notion
of low income, is the idea of a social divide whereby
the skills required to manipulate and utilize these
technical tools are split between the low and high
income individuals (Kim et al., 2009). Provided that
those with higher incomes usually have higher levels
of education and continued access and training on
up-to-date technologies, those on the lower income
spectrum are usually the opposite. That is, low
income earning individuals on average will never
have a chance to learn the skills to use such
technologies, and in many instances, may not even
be exposed to them.
From listing the number of barriers associated
with the adoption and usage of the Internet and
PHR, it is hard to believe that these technologies can
be used to increase health awareness and
accountability. However, given the speed to which
technology has advanced, and is continuing to
advance, many barriers related to technology and its
usage among the elderly are slowly dissipating. As
the population ages and technology (computers and
the Internet) becomes more common and prevalent
in daily lives, the number of elderly individuals who
don’t have access or don’t know how to use a
computer will also decrease, thus increasing
adoption and usage of the Internet and PHR as a
health awareness and accountability tool.
5 DISCUSSION
In light of the number of barriers associated with the
implementation, adoption, and usage of the Internet
and PHR among the elderly; how then, can such
tools be used in the creation of greater consumer
awareness and accountability in overcoming the
shortage of healthcare professionals in the foreseen
future? As it was discussed above, the Internet and
PHRs have the capabilities to change not only an
individual’s health behavior, but it can also place
greater emphasis on the individual themselves to be
more aware and responsible for the type of treatment
they are to receive (Campbell, 2005). Provided that
this generation of elderly individuals thrived and
worked during the age of the computer, many
elderly individuals today are at least aware of the
Internet and computer as information gathering
tools. Knowing this, the concept of using the
Internet or a computer to retrieve or document
information is not a new idea. However, even with
familiarity and awareness of the computer and the
Internet, many websites and computer applications
are not user friendly. Due to the fact that not enough
consideration has been given to the usability of
many of these websites and PHR applications, the
implications of usability features can play a big role
in the adoption of these technologies (Squire &
Preece, 1996). In the article by Lober et al., one of
HEALTH INFORMATION RETRIEVAL AND USAGE AMONG THE ELDERLY - Potential use of the Internet and
Personal Health Records in Health Awareness and Accountability
209

the main reasons provided to account for the poor
adoption rates of elderly individuals with computers
was that “they were scared.” Given that most
websites today and applications are jumbled with
many features and options, it is no wonder this is the
case. One solution to this would be to gather
stakeholder input prior to launching a site or
application (or the proper term, usability testing), to
ensure it matches the needs of those using it. In
addition, another problem with this idea of
technology as a social awareness and accountability
tool, is the fact that physical ability plays a role in
the success of such a strategy. As mentioned earlier,
with old age being accompanied usually with some
form of physical deterioration, the ability to use
tools that are tailored towards able bodied
individuals may not be adoptable to this older age
group. Even though some tools and/ or applications
are geared specifically towards the elderly, the costs
associated to these pieces of technology are usually
higher. With the knowledge that elderly individuals
may not have high incomes, this can become an
issue in terms of accessibility.
As elderly individuals become increasingly
engulfed in technology, the natural shift towards
using computers and the Internet for healthcare
needs will become ever apparent. With 5 million
adults aged 65 and over who use the Internet to
access and search for health related information, this
trend will surely continue to grow. Indeed as
technology advances, mankind becomes ever more
reliant upon it (Campbell & Nolfi, 2005). With
elderly individuals (or consumers) using these tools
in preparing themselves prior to seeing a family
physician, i.e., looking for health information,
individuals then can better maximize and utilize the
limited amount of time they have with their
physicians (Belzer, 1999). By changing the
relationship between physician and patient, in that
both parties arrive informed, patient outcomes can
also be improved as adverse events are more
noticeable, mistakes are flagged, and physicians are
kept up-to-date with current best practices.
However, as consumers are using the Internet to
look for health information, the lack of proper
training or level of knowledge required to interpret
this information, could also have potential harm for
individuals retrieving this information (Cline &
Haynes, 2001). Although the Internet can never
replace the information received and given from
physicians, it can, if used and interpreted correctly,
can provide useful insight into treatment options and
barriers against adverse events. In one survey
conducted by Neff (1999), it was found that 67% of
physicians reported having patients who discussed
internet retrieved information with them. Given that
this survey is a little outdated, one would expect the
number of individuals today who discuss
information with their physicians should be
increasing as more individuals use the Internet to
search for information.
In general, if the technologies used by the elderly
are tailored towards their individual needs, it is
believed that the adoption rates will greatly improve.
Due to the fact that old age hinders many physical
abilities that many others take for granted,
technology may not always be the best fit. However,
given the growing body of literature and
advancement in technology, the use of the Internet,
PHRs have shown to be quite useful in providing
individuals with health information which have
positively changed their health behaviours.
Consequently individuals are more likely to take a
greater interest in the control of their health
information by being more accountable for it.
However, many of these studies and findings are
based on able bodied elderly individuals. Thus, this
leads to the question those who cannot use these
technologies. Will the results be the same? Is this
really representative of the elderly population?
Nonetheless, as physicians and patients begin to
work side by side in sharing and exchanging
information, patients will in all likelihood live
healthier lifestyles because of this. Moreover, due to
the large amounts of health information available on
the internet 24/7 with personal health information
stored within PHRs, accessible 24/7, the utilization
and need to see healthcare practitioners (especially
physicians) should also decrease. Individuals will
search the internet for minor illnesses and utilize
information available from their PHR to share with
other health professionals in remote consultation.
This subsequently should help move some of the
burden away from the healthcare systems since
individuals will not need to see physicians as often
for minor items, allowing relief for the already small
number of health practitioners available.
6 CONCLUSIONS
Technology has grown leaps and bounds over the
last century. The internet has opened many new
doors for individuals to gather and share
information. This in itself is changing the ways
many individuals do things. Provided that humans
are becoming ever reliant on technologies to perform
daily activities, it is only a matter of time until
HEALTHINF 2011 - International Conference on Health Informatics
210

looking up information on the internet becomes
second nature (Givens, 2008). Of course, given the
vast amount of information available on the Internet,
perhaps having websites meet certain standards in
health information would be beneficial in preventing
harm (Cline & Haynes, 2001). One example of this
is HON which stands for Health On the Net
Foundation which aims to promote and guide the
deployment of useful and reliable online health
information and its appropriate and efficient use
(HON, 2010). Even though this accreditation and
standard is relatively new, it allows the individuals
searching for online health information instant
access and protection from inaccurate or false
information. By providing consumers or the elderly
the proper tools and information about health
information and their own personal health records,
many of these same individuals will change their
health behaviors to that of a more positive one, or a
health promotion and wellness model. Even though
there are barriers associated with using technology
in changing ones health behaviors as shown above;
by working with stakeholders and application/ web
developers, many of these hurdles can be overcome
(Squire & Preece, 1996). Moreover, with technology
advancing faster than anything else currently in
development, the costs of owning a personal
computer are decreasing while having access to the
internet is increasing rapidly. Through the use of
technology, particularly the Internet and PHRs, the
number of individuals going to visit family
physicians will decline. As more elderly individuals
become healthier and act healthier from changing
their lifestyles; many elderly individuals will think
twice (or check twice) prior to seeing a physician. In
doing so, this will ultimately decrease the number of
individuals having to see a physician for all their
information needs, thus allowing physicians more
time in seeing more severely injured or ill
individuals.
ACKNOWLEDGEMENTS
I would like to thank my friends and mentors, in
particular Kamran Ahmed and Jimmy Wang in
encouraging me to actualize my academic pursuits.
REFERENCES
Ball, M., Smith, C., & Bakalar, R. (2007). Personal health
records: Empowering consumers. Journal of
Healthcare Information Management, Vol.21(1).
Bevand, T. (2010). Canadian Health Care System:
Sustainable? An analytical exploration of current and
future trends in health care funding. Retrieved June 11,
2010, from
http://www.scribd.com/doc/30804821/Canadian-
Health-Care-System-Sustainable-An-Analytical-
Exploration-of-Current-and-Future-Trends-in-Health-
Care-Funding
Belzer, E. (1999). Improving Patient Communication in
No Time. American Academy of
Family Physicians. Retrieved June 15, 2010, from
http://www.aafp.org/fpm/990500fm/23.html
Campbell, R. (2003). The elderly and the Internet: A Case
study. The Internet Journal of Health, Vol. 3(1).
Campbell, R. (2005). Consumer Informatics: Elderly
persons and the Internet. Perspective Health
Information Management. Vol. 2(2).
Campbell, R., & Nolfi, D. (2005). Teaching elderly adults
to use the Internet to access health care information:
before-after study.” Journal of Medical Internet
Resources, Vol. 7(2).
Chou, P., & Wister, A. (2005). From cues to action:
Information seeking and exercise self-care among
older adults managing chronic illness. Canadian
Journal on Aging. Vol. 24(4), pp. 395-408.
Cline, R., & Haynes, K. (2001). Consumer health
information seeking on the Internet: the state of the art.
Health Education Research, Vol.16, No.6, 671-692.
Escamilla, M. (2006). Medical information seeking
behaviour of the elderly & Pathfinder. Journal of
Medical Internet Resources. Retrieved May 15, 2010,
from http://www.gseis.ucla.edu/faculty/
maack/Documents/SeekingPaperME.pdf
Eysenbach, G. & Jadad, A. (2001). Evidence-based patient
choice and consumer health informatics in the Internet
age. Journal of Medical Internet Research, 3(2):e19.
Federal Interagency Forum on Aging Related Statistics.
Older Americans 2008: Key Indicators of Well Being.
Retrieved June 15, 2010, from http://www.
agingstats.gov/agingstatsdotnet/Main_Site/Data/2008_
Documents/OA_2008.pdf
Gladden, J. (2000). Information exchange: critical
connections to older adult decision- making during
health care transitions. Geriatric Nursing 21, no. 4:
213-218.
Givens, J. (2008). The Increasing Human Dependence on
Computers. Associated Content. Retrieved June 17,
2010, from
http://www.associatedcontent.com/article/701085/the_
increasing_human_dependence_on.html?cat=9
Häkkinen, H. (2009). Health care challenges in regions
with declining and ageing population. Council of
European Municipalities and Regions, June 15-16.
HON. (2010). Health On the Net Foundation. Retrieved on
June 24, 2010, from http://www.hon.ch/
Kim, E., Stolyar, A., Lober, W., Herbaugh, L., Shinstrom,
S., Zierler, B., Soh, C., & Kim, Y. (2007). Usage
patterns of a personal health record by elderly and
disabled users. Annual Symposium Proceedings
Archive, 2007:409-413.
HEALTH INFORMATION RETRIEVAL AND USAGE AMONG THE ELDERLY - Potential use of the Internet and
Personal Health Records in Health Awareness and Accountability
211

Kim, E., Stolyar, A., Lober, W., Herbaugh, L., Shinstrom,
S., Zierler, B., Soh, C., & Kim, Y. (2009). Challenges
to using an electronic personal health record by a low-
income elderly population. Journal Medical Internet
Research, 2009;11(4):e44.
Lee, M. (2007). How sustainable is Medicare? A closer
look at aging, technology and other cost drivers in
Canada’s Healthcare system. Ottawa: Canadian
Centre for Policy Alternatives.
Lober, W., Zierler, B., Herbaugh, A., Shinstrom, S.,
Stolyar, A, Kim, E., & Kim, Y. (2006). Barriers to the
use of a Personal health record by an elderly
population. Annual Symposium Proceedings Archive,
2006: 514-518.
Mahler, H., & Kulik, J. (1990). Preferences for health care
involvement, perceived control and surgical recovery:
a prospective study. Soc Sci Med. Vol. 31(7):743-751.
Markle Foundation. (2003). Connecting for Health.
Personal Health Working Group Final Report.
Retrieved June 15, 2010 from http://www.
connectingforhealth.org/resources/phwg_final_report.
pdf
Markle Foundation. (2005). Attitudes of Americans
Regarding Personal Health Records and Nationwide
Electronic Health Information Exchange. Key
Findings from Two Surveys of Americans Conducted
by Public Opinion Strategies, Alexandria, Va.
Retrieved June 18, 2010 from www.phrconference.
org.
Maynard, M. (1991). Two groups of elderly residents’
health attitudes and behaviours: Implications for health
promotion. Physical & Occupational Therapy in
Geriatrics,Vol. 9(2), p.43-54.
McInturff, B. (2005). Public Opinions Strategies. Key
findings from focus groups and two national surveys
conducted on behalf of the Markle Foundation, the
Robert Wood Foundation and Connecting for Health.
Presented October 11, 2005 at the Personal Health
Records Conference in Washington, DC.
National Center for Health Workforce Analysis. (2006).
The impact of the aging population on the health
workforce in the United States: Summary of key
findings. National Center for Health Workforce
Analysis, Bureau of Health Professions, Health
Resources and Services Administration. Retrieved
June 11, 2010, from http://www.albany.edu/
news/pdf_files/impact_of_aging_excerpt.pdf
Neff, J. (1999) Internet could see more Web site
sponsorships. Advertising Age, 70(11), s6–7.
Robson, W. (2001). Will the Baby Boomers Bust the
Health Budget? Demographic Change and Health Care
Financing Reform. C. D. Howe Institute Commentary,
No. 148. Renouf Publishing, Toronto.
Shortliffe, E., Cimino, J. (2006). Biomedical informatics:
computer applications in health care and biomedicine
(3
rd
edition), New York: Springer.
Sprague, L. (2006). Personal Health Records: The
people’s choice? National Health Policy Forum,
No.820.
Squire, D., & Preece,J. (1996). Usability and Learning:
Evaluating the potential of educational software,
Computer & Education, Elsevier Science Ltd, Great
Britain, Vol. 27, N. 1, pp. 15-22.
Tang, P., Ash, J., Bates, D., Overhage, J., & Sands, D.
(2006). Personal health records: definitions, benefits,
and strategies for overcoming barriers to adoption. J
Am Med Inform Assoc. Mar–Apr; 13(2):121–6.
Wicks, D. “Older Adults and their information seeking.”
Behavioral and Social Sciences Librarian 22, no.
2(2004):1-26.
Wiser, A. (2005). Wister. Baby Boomer Health Dynamics:
How Are We Aging? Toronto, ON: University of
Toronto Press.
HEALTHINF 2011 - International Conference on Health Informatics
212
