
DIASTOLIC TIMED VIBRATIONS FOR PRE-HOSPITALIZATION
TREATMENT OF MYOCARDIAL INFARCTION
Marcin Marzencki, Farzad Khosrow-Khavar, Syed Ammar Zaidi, Carlo Menon and Bozena Kaminska
Department of Engineering Science, Simon Fraser University, 8888 University Drive, Burnaby, BC, Canada
Keywords:
Heart attack, MI pre-hospitalization treatment, Coronary thrombosis.
Abstract:
Heart attack or myocardial infraction is the leading cause of deaths in the modern world. In order to increase
survival chance of patients, action should be taken during the first hour from the onset of symptoms, which
is most often impossible with the current technology. To this end, we propose a method of heart attack
treatment based on low frequency diastolic timed vibrations. This method can be used in ambulatory setting
by unspecialized personnel as it is noninvasive and safe for the patient. It is based on applying low frequency
mechanical vibrations synchronized with the heart cycle of the subject along with application of thrombus
dissolving drugs. We present an analysis of the proposed methodology and provide experimental results
obtained with a prototype device.
1 INTRODUCTION
In the developed world, heart diseases are the leading
cause of death, presenting higher mortality rate than
cancer (American Heart Association Statistics, 2010).
In the United States alone, over 7 million men and
6 million women are living with some form of coro-
nary heart disease and over a million people suffer a
(new or recurrent) coronary attack every year. About
40% of heart attacks result in death (American Heart
Association Statistics, 2010). Myocardial Infarction
(MI) or heart attack is most often caused by forma-
tion of a blood clot (thrombus) blocking the arterial
vasculature surrounding the heart. MI refers to my-
ocardial cell death and occurs due to a complete coro-
nary obstruction which results in a profound blood
flow impairment causing inadequate oxygen delivery
to the heart muscle. Once such an obstruction begins,
cell death can occur in as little as 20 minutes. Com-
plete death of all myocardial cells at risk can occur
in, at the earliest, 2 to 4 hours (Kostuk, 2008). Var-
ious methods have been developed to dissolve or re-
move thrombus before MI occurs. Preferred invasive
methods such as angioplasty require significant setup
time and resources in order to be successful. Inci-
dentally, the most effective treatment occurs during
the first 60 minutes of the symptoms known as the
golden hour. However, by the time an average pa-
tient reaches a hospital most deaths have already oc-
curred (Turner and Rosin, 2008). This is worsened
by the fact that those who manage to reach a hospital
spend additional time undergoing examinations or be-
ing transported to a cardiac cathlab before the actual
treatment can begin. As a result, speed of interven-
tion is the biggest factor in saving a patient’s life and
is the key to effective heart attack treatment. Thus, if
treatment could begin during transportation to a hos-
pital, it would play a key role in ensuring the survival
of patients.
To this end, we propose a method of treatment that
could be safely applied by unspecialized personnel
on-site or during patient transportation to the hospital.
We believe that this method could drastically improve
the survival rate of heart attack patients.
2 PROPOSED METHOD
We present a safe non-invasive method suitable for
treatment of heart attack and other states of low coro-
nary blood flow. It is based on applying low level
mechanical vibrations in the chest area along with
application of clot dissolving drugs. By performing
vibrations during the diastolic period of the cardiac
cycle (the relaxation of the heart) it is expected that
coronary flow is increased and thrombus dissolution
is achieved. In this study, we first aim at developing a
vibrating system that is independently controlled by a
real-time ECG signal. The triggering of the vibrating
405
Marzencki M., Khosrow-Khavar F., Ammar Zaidi S., Menon C. and Kaminska B..
DIASTOLIC TIMED VIBRATIONS FOR PRE-HOSPITALIZATION TREATMENT OF MYOCARDIAL INFARCTION.
DOI: 10.5220/0003130604050408
In Proceedings of the International Conference on Bio-inspired Systems and Signal Processing (BIOSIGNALS-2011), pages 405-408
ISBN: 978-989-8425-35-5
Copyright
c
2011 SCITEPRESS (Science and Technology Publications, Lda.)

system should be synchronized with the ECG signal
in such a way so as to remain vibrating in the dias-
tole and cease all vibrations in the systole of the ECG
signal.
Our goal is to create a device for field use - a Dias-
tolic Timed Vibrator (DTV) to be employed by med-
ical emergency personnel to remediate acute states of
low coronary blood flow, such as those exhibited in
angina pectoris (chest discomfort secondary to coro-
nary artery narrowing) or heart attack (an acute block-
age of a coronary artery, usually by a blood clot). The
DTV will impose mechanical vibrations to the chest
of the patient in order to improve coronary blood flow.
We aim at creating an inexpensive and portable sys-
tem requiring minimal intervention of specialized per-
sonnel.
2.1 Mechanical Vibrations
There is strong experimental evidence that diastolic
mechanical vibrations on the chest wall increase coro-
nary blood flow (CBF). In past studies, diastolic vi-
brations performed on patients with coronary arte-
rial disease (CAD) and on normal subjects resulted in
an immediate increase of CBF as measured by both
transesophageal doppler and coronary flow wire. The
CBF increase in CAD patients was significantly larger
than those of normal subjects (Taihei et al., 1994). In
addition, clinical studies performed on humans and
canines (Koiwa et al., 1997) have shown that exter-
nal diastolic vibrations can release incomplete relax-
ation (IR) and improve the systolic function of the
heart. Similar studies (Koiwa et al., 1997) consisting
of external vibrations applied on human patients with
aortic regurgitation (AR) and ischemic heart disease
(IHD) resulted in a decrease of left ventricle systole
pressure; proving that vibration induced depression
does occur in humans. Clinical studies have shown
that diastolic timed mechanical vibrations around 50
Hz improve coronary blood flow and left ventricu-
lar (heart muscle) performance in human volunteers,
with and without coronary artery disease (Taihei et al.,
1994). Low frequency vibration is a known potent va-
sodilator, especially for arteries with a degree of ac-
tive tension or spasm, which is often the case in heart
attack (Oliva and Breckinridge, 1977), and it has fur-
ther been shown to significantly enhance clot disso-
lution with or without a thrombolytic agent both in-
vitro and in commercially available catheter systems
(Evans et al., 2003).
2.2 ECG Synchronization
Our method provides a new technique for disrupting
and clearing the thrombus present in a patient’s ar-
terial vasculature surrounding the heart. During sys-
tole the heart is contracting and pressure needed for
driving the blood is being generated within the cham-
bers of the heart. As a result, vibrations should only
be applied in the diastole (Koiwa et al., 1997). Fur-
thermore, it has been demonstrated in clinical stud-
ies that vibrations timed exclusively to the diastole of
the cardiac cycle advantageously facilitate heart mus-
cle relaxation and paradoxically improve the strength
of the heart contractions and hence can be utilized
safely (Koiwa et al., 1994). In order to be able to
synchronize mechanical vibration with the heart cy-
cle, the ECG signal has to be analyzed and QRS com-
plexes indicating the onset of systole have to be iden-
tified. Automatic detection of QRS complexes has
been a subject of intensive research in the last several
decades. Proposed algorithms range from simple fil-
ters to very calculation intensive machine learning al-
gorithms (Kohler et al., 2002). Currently, most algo-
rithms use a discrete or continuous wavelet transform
which gives both the time and frequency characteris-
tics of the signal. Machine learning algorithms such
as Hidden Markov Model, Neural Networks and/or
Support Vector Machine (SVM) are used to classify
different parts of the ECG signal. The extensive
amount of training that is required prior to use is a
serious limitation of these methods in certain cases.
We decided to use the widely employed ”Tompkins”
algorithm due to its implementation simplicity and ro-
bustness in finding abnormal QRS complexes.
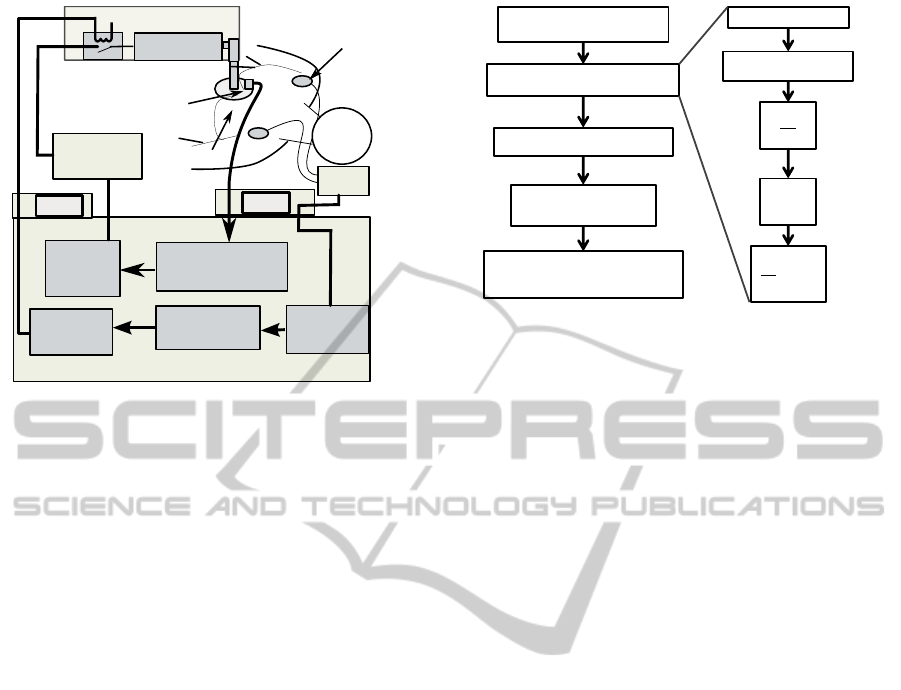
2.3 System Architecture
The proposed system is composed of four main parts:
vibrator, accelerometer, ECG system, DC power sup-
ply, and a LabView VI containing signal processing
and control. Figure 1 schematizes the system archi-
tecture.
The mechanical vibrations were generated using
a commercially available massager device (Human
Touch HT-1280) driven by a DC voltage source inter-
faced with LabView. This setup generates the linear
movement of the plate attached to a patient. An active
damping stage is added to adjust the amplitude of gen-
erated vibrations and allow for rapid stopping of the
motor. In order to be able to generate vibrations only
in the desired periods of the heart cycle, an electro-
magnetic relay is introduced on the power line of the
motor. This setup allows for efficient control of on-off
time of the motor along with its rotational frequency.
Furthermore, a MEMS accelerometer (LIS3L02AL)
has been integrated into the vibrating plate to provide
a feedback on the generated vibration amplitude and
BIOSIGNALS 2011 - International Conference on Bio-inspired Systems and Signal Processing
406
DC motor
massager
ECG electrodes
feedback
accelerometer
patient's
chest
ECG
DC power
supply
acceleration data
processing
ECG data
filtering
pulse
generator
QRS complex
detection
LabView VI
DAQ
motor
voltage
control
DAQ
Figure 1: Block diagram of the proposed diastolic vibration
system.
frequency.
An ECG acquisition system Burdick EK10 is em-
ployed to amplify and filter the ECG signal. The re-
sulting signal is digitalized by a DAQ at 14bit and
200Hz and further processed in LabView.
An algorithm has been developed to detect the
systole and diastole in a real time ECG signal in order
to allow diastolic timed vibration. We created a vir-
tual instrument using National Instruments LabView.
The VI software implements the real-time Hamilton
and Tompkins QRS complex detection algorithms.
Figure 2 presents the stages of the algorithm. The
ECG signal is band-pass filtered with a combination
of low and high pass filters to separate the high energy
QRS complex from the rest of the ECG signal. The
resulting signal is differentiated to extract the onset of
R-wave. Next, the signal is squared to make it posi-
tive prior to integration. The integrator sums the area
of the positive wave form. The width of the integra-
tor is chosen carefully to be long enough to consider
abnormally long QRS complexes and short enough so
that it does not overlap with the T-wave. The operator
can pick the window size and the detection threshold
in the software.
The frequency of QRS complexes is used to cal-
culate the heart beat rate and the period of the ECG
signal. Furthermore, lengths of two counters are cal-
culated which, in coordination with the R peak de-
tection, are time controlled to stop the vibrating sys-
tem during systole and enable it during diastole. Af-
ter detecting the R peak, systole counter is reset dis-
abling the vibrating system until the systole cycle is
complete. Once the systole counter reaches its limit
(which is derived from the period of ECG signal), the
vibrating system is enabled again for a duration deter-
1
32
n=32
X
n=1
Real-time ECG signal
acquistion
QRS complex detection
Heart rate calculation
Counter length
determination
Counter control and driving
pulse generation
Low pass filter
High pass filter
[]
2
d
dt
Figure 2: Block diagram of the ECG signal processing used
to generate driving signal for mechanical vibrations syn-
chronized with the diastole of a cardiac cycle.
mined by the diastole counter. The diastole counter is
accordingly set to reach its limit before the beginning
of the systole cycle. In case where the two counters
overlap due to arrhythmic operation of the heart, the
systole counter has priority over the diastole counter;
thus ensuring that any detection of an R peak would
immediately disable the vibrating system. The sys-
tole counter duration was approximated based on the
QT interval calculations performed during past clini-
cal studies of heart disease patients (Alexander et al.,
1951).
3 EXPERIMENTAL RESULTS
In order to verify the accuracy of our predictions con-
cerning the effectiveness of diastole timed vibrations,
we built a prototype system. We concentrated on
proper synchronization of the mechanical vibrations
with the ECG signal.
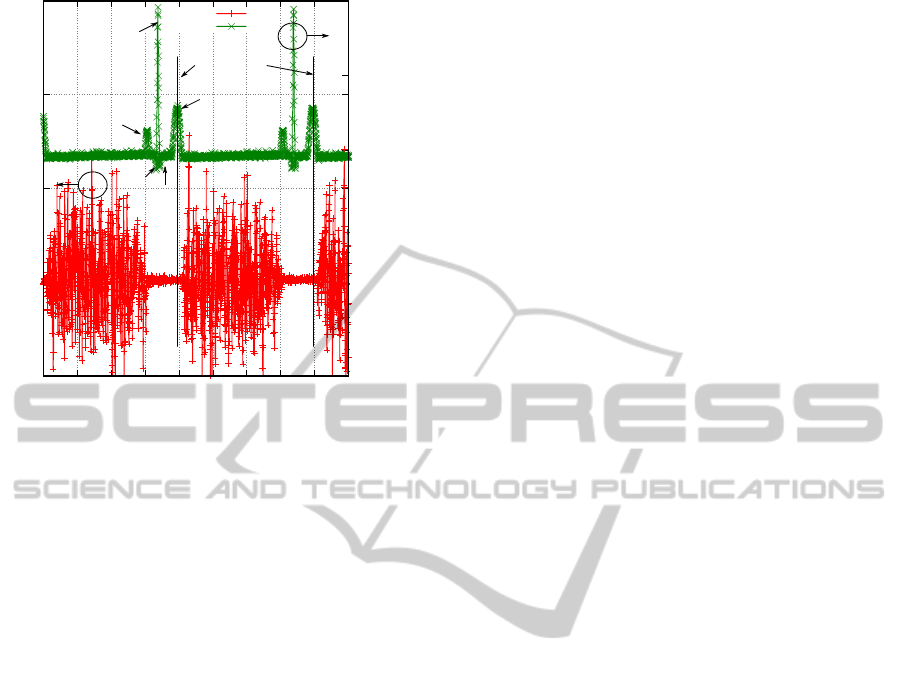
Figure 3 shows mechanical vibrations generated
with the massager synchronized with a real-time ECG
signal. The overall period of the heart beat is 2 sec-
onds in which the PQRST region of the ECG lasts
for 0.55± 0.05s. Although the systole (QRST region)
only lasts for 0.41 ± 0.04 seconds, the vibrating sys-
tem is turned off before the PQRST region begins in
order to ensure that vibrations occur only when the
heart is in its relaxation state. During the diastolic cy-
cle, the DC motor is allowed to vibrate for 1.40 ± 0.04
seconds. The massager device has high rotary inertia,
therefore a special damping stage was introduced in
order to allow more precise timing of the generated
vibrations. The delay between the end of the driv-
ing pulse and the actual termination of the mechanical
vibrations was measured to be approximately 17ms .
Therefore, the vibration spill defined as the amount
DIASTOLIC TIMED VIBRATIONS FOR PRE-HOSPITALIZATION TREATMENT OF MYOCARDIAL INFARCTION
407
-0.5
0
0.5
1
1.5
1 1.5 2 2.5 3 3.5 4 4.5 5 5.5
-1.5
-1
-0.5
0
0.5
1
Acceleration [g]
ECG [mV]
Time [s]
Acceleration
ECG
Vibration
trigger signals
P
Q
R
S
T
Figure 3: Experimental results for mechanical vibrations
(represented by acceleration amplitude) synchronized with
diastolic period of the cardiac cycle.
of vibrations present in the systole is minimal. For
the most part, the QT interval was free of vibrations
and with the predictive termination of vibration based
on a regression algorithm, it was possible to com-
pletely avoid vibration spill on the QRS complex in
most cases.
4 CONCLUSIONS
The proposed diastolic timed vibration system is a
safe and innovative method for rapid treatment of
heart strokes and other low blood flow cases. Clinical
studies have shown that mechanical vibrations help
increase the coronary blood flow and aid in the im-
provement of the systolic function of the heart. In
case of a heart attack, mechanical vibrations along
with application of thrombolytic agents can improve
clot dissolution and thus increase chances of patient’s
survival. We presented a prototype of a diastolic
timed vibrator controlled by a custom LabView VI
and synchronized with a commercial ECG system.
We demonstrated that mechanical vibrations gener-
ated by a massager device can be synchronized with a
real time ECG signal from a patient. We developed al-
gorithms used in the control Labview VI used to trig-
ger the vibrator only in the diastole. The presented
results show that we can accurately control the me-
chanical vibrations and thus avoid application of vi-
brations in the critical part of the QT interval.
ACKNOWLEDGEMENTS
This project was supported by Simon Fraser Univer-
sity in collaboration with Ahof Biophysical Systems
Inc. The authors would like to thank Andrew Hoff-
man for valuable inputs to the project.
REFERENCES
Alexander, J. K., Ferrer, M. I., Harvey, R. M., and Cour-
nand, A. (1951). The q-t interval in chronic cor pul-
monale. Circulation, 3(5):733–737.
American Heart Association Statistics (2010). Executive
summary: heart disease and stroke statistics–2010 up-
date: a report from the american heart association.
Circulation, 121(7):948–954.
Evans, M. A., Demarais, D. M., Eversull, C. S., and
Leeflang, S. A. (2003). Patent No. US 6,663,613 B1:
System and methods for clot dissolution.
Kohler, B.-U., Hennig, C., and Orglmeister, R. (2002). The
principles of software QRS detection. IEEE Eng. Med.
Biol., 21(1):42–57.
Koiwa, Y., Honda, H., Takagi, T., Kikuchi, J., Hoshi, N.,
and Takishima, T. (1997). Modification of human
left ventricular relaxation by small-amplitude, phase-
controlled mechanical vibration on the chest wall. Cir-
culation, 95(1):156–162.
Koiwa, Y., Naya, T., Takagi, T., Hond, H., Hoshi, N., Ka-
mada, H., Shirato, K., Kanai, H., and Cyubachi, N.
(1994). Diastolic mechanical vibration on the chest
wall increases human coronary blood flow. Japanese
Circulation Journal, 58(7):476.
Kostuk, W. J. (2008). Coronary artery disease - angina, un-
stable angina, myocardial infarction. Discussion pa-
per prepared for The Workplace Safety and Insurance
Appeals Tribunal.
Oliva, P. B. and Breckinridge, J. C. (1977). Arteriographic
evidence of coronary arterial spasm in acute myocar-
dial infarction. Circulation, 56(3):366–374.
Taihei, N., Yoshiro, X., Takehiko, T., Hideyuki, H.,
Nobuo, H., Hideichi, K., Kunio, S., Hiroshi, K., and
Noriyoshi, C. (1994). Diastolic mechanical vibra-
tion on the chest wall increases human coronary blood
flow. Japanese Circulation Journal, 58(7):476.
Turner, G. O. and Rosin, M. B. (2008). Recognizing and
Surviving Heart Attacks and Strokes: Lifesaving Ad-
vice You Need Now. University of Missouri Press.
BIOSIGNALS 2011 - International Conference on Bio-inspired Systems and Signal Processing
408
