
SEMANTIC PROCESS MINING FOR THE VERIFICATION OF
MEDICAL RECOMMENDATIONS
M. A. Grando
School of Informatics, Edinburgh University, 10 Crichton street, Edinburgh, U.K.
M. H. Schonenberg, W. van der Aalst
Department of Mathematics and Computer Science, Technische Universiteit Eindhoven, Eindhoven, Netherlands
Keywords:
Medical guidelines, Computer interpretable guidelines, Workflow languages, Process mining, Semantic con-
formance checking, Declarative specification.
Abstract:
The dissemination of best medical practices should contribute to a higher quality of care. Because natural
language specifications can be ambiguous, their miss interpretation can lead to all kinds of errors. Here we
propose a declarative approach for precisely defining medical recommendations. We also propose an approach
based on semantic process mining to verify that an arbitrary Computer Interpretable Guideline (CIG) complies
with the medical recommendations. Taking into account that some medical recommendations are critical, our
work can be seen as a contribution to the design of safer CIGs.
Moreover, we introduce some novel strategies to take full advantage of the information provided by the se-
mantic conformance checker in order to: 1) suggest scenarios than could lead to violations of the medical
constraints in the CIG and, 2) estimate how flexible is the CIG with respect to the medical recommendations
used as starting point.
1 INTRODUCTION
Medical guidelines are used to disseminate the con-
sensus reached on best medical practices. They are
paper-based and expressed in natural language, there-
fore they can be ambiguously interpreted if the med-
ical evidence provided in the guideline is not care-
fully considered. Some medical guidelines are de-
tailed enough to suggest possible care paths. For
such guidelines a general practice is to provide work-
flow diagrams that model the care paths explained in
the natural language description. The provided work-
flows are generally specified as networks of tasks and
states connected by relational constraints of succes-
sion. In (Mulyar et al., 2007) the declarative language
CIGDec has been proposed to precisely specify medi-
cal recommendations. The CIGDec specification lan-
guage is supported by DECLARE, a constraint-based
Workflow Management System. DECLARE (Pesic
and van der Aalst, 2006; van der Aalst and Pesic,
2006) offers a graphical notation for its constraints
that have precise semantics in Linear Temporal Logic
(LTL). This provides a platform for the verifica-
tion of constraint-based models. Furthermore, DE-
CLARE supports the execution of constraint-based
models. Constraint-based models do not explicitly
define the possible execution paths, but rather spec-
ify the boundaries of execution, i.e. any executionthat
does not violate the constraints is allowed. The advan-
tages of using the CIGDdec language for specifying
medical recommendations (Mulyar et al., 2007) are
(1) its flexibility, i.e. many care paths can be specified
with relative few constraints, and (2) its extendabil-
ity, i.e. it is possible to define additional constraints
specified in LTL to the default language to express
situation specific constraints.
Unfortunately, the translation of medical recom-
mendations into Computer Interpretable Guidelines
(CIGs) is not automatic and therefore not necessarily
error free. However, some languages for the specifi-
cation of CIGs, like Asbru (Shahar et al., 1998), have
been provided with formal techniques based on theo-
rem proving for verifying the satisfaction of proper-
ties (Teije et al., 2006) (Gendt et al., 2005). More-
over, the area of business process mining has con-
tributed with techniques to analyze processes based
on their execution history (event logs). Process min-
ing can amongst others be applied to automatically
5
A. Grando M., H. Schonenberg M. and van der Aalst W..
SEMANTIC PROCESS MINING FOR THE VERIFICATION OF MEDICAL RECOMMENDATIONS.
DOI: 10.5220/0003112600050016
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2011), pages 5-16
ISBN: 978-989-8425-34-8
Copyright
c
2011 SCITEPRESS (Science and Technology Publications, Lda.)

derive process models from the event logs, to check
the conformance of the actual execution with a pre-
sumed model of the process and to check properties
on the execution traces in the log.
More recently more accurate and robust process
mining techniques, known as semantic conformance
checking, were introduced in (Casati and Shan, 2002)
(Kharbili and Stein, 2008) to analyze processes by
adding semantics to the event logs. Here our aim is to
explore the use of semantic conformance checking for
verifying if a CIG satisfies/violates the recommenda-
tions from the medical guideline on which it is based.
We propose a novel strategy for a further analysis
and interpretation of the results generated during se-
mantic conformance checking. The strategy is based
on 1) generating the classes of unexplored scenarios
that could expose untested cases of violation of med-
ical recommendations with the DECLARE model of
medical recommendations, and 2) reusing the scenar-
ios from (1) exposing modeling decisions that reduce
the flexibility of the CIG with respect to the medical
recommendations on which it is based.
In Section 2 we take as starting point two natural
language recommendations from the chronic cough
guideline from (Irwin et al., 1998) and we disam-
biguate them by considering the medical evidence
provided in the guideline. Then in Section 3 we ex-
plain how to specify the chosen recommendationsas a
set of declarativeconstraints in the DECLARE frame-
work. While the analysis presented in sections 2 and
3 can not be automatized, the methodology presented
in sections 4 and 5 has been implemented in the DE-
CLARE tool and the ProM framework. In Section 4
we explain how to use the ProM framework(vanDon-
gen et al., 2005) for checking semantic conformance
of a CIG with respect to the DECLARE constraints
from Section 3. The CIG used in Section 4 is speci-
fied using the PROforma (Fox et al., 1997) language
and it has been taken from the Open Clinical reposi-
tory (http://www.openclinical.org) where other CIGs
for the same medical recommendations are available.
Every CIG from the repository is specified in a dif-
ferent language: Asbru (Shahar et al., 1998), EON,
GLIF and GUIDE. The PROforma CIG has been se-
lected for pragmatic reasons and the explained tech-
nique is generic and independent of the language and
decision-support system used for the specification of
the CIG. In Section 5 we explain some techniques
for allowing further analysis of the results obtained
from the DECLARE tool and the ProM framework
after performing the semantic conformance checking.
After mentioning related approaches in Section 6 we
finish the conclusions in Section 7.
2 CHRONIC COUGH GUIDELINE
RECOMMENDATIONs
In the chronic cough guideline (Irwin et al., 1998)
the eligibility criterion is that a patient has a cough
that lasts at least 3 weeks. Here we only consider the
case of immunocompetentadult patients. The chronic
cough guideline combines a strategy of diagnosis with
empirical treatment, it guides the physician to make
an assumption regarding the most likely cause of
cough and start treating it with the intention of con-
firming the diagnosis by resolving the cough. There-
fore, the guideline’s main goal is diagnosing chronic
cough for inmunocompetent patients and stopping it
by treating the most likely cause of cough.
Through out this paper we will consider the fol-
lowing medical recommendations from the chronic
cough guideline for inmunocompetent adult patients:
R1) ”chest radiographs should be ordered before any
therapy is prescribed in nearly all patients with
chronic cough. Chest radiographs do not have to
be routinely obtained before beginning treatment
for presumed PNDS [post nasal drip syndrome]
in young nonsmoker, or in pregnant women, or
before observing the result of discontinuation
of an ACEI [angiotensin-converting enzyme in-
hibitor].”
R2) ”When the chest X-ray is normal, PNDS, Asthma,
and GERD [Gastroesophageal reflux disease] are
the likely causes of chronic cough.”
Figure 1 shows the graphical representation of the
recommendations R1) and R2) explained above. This
simplified diagram has been extracted from a more
extended diagram that provides a workflow-like ex-
planation of the main medical recommendations in
the chronic cough medical guideline (Irwin et al.,
1998).
The analysis and interpretation of natural lan-
guage medical recommendations constitutes a time-
consuming, non-error free task that requires in most
of the cases medical expertise in order to disam-
biguate statements and to make explicit implicit
knowledge hidden in the guidelines. So far this pro-
cess has to be manually performed. In the rest of
this section we summarize our conclusions during the
disambiguation of the natural language medical rec-
ommendations from the chronic cough guideline after
analyzing in detail the provided medical evidence. In
the case of the chronic cough guideline the follow-
ing evidence grading scale has been provided with
the guideline’s specification, ordered from high to low
quality:
HEALTHINF 2011 - International Conference on Health Informatics
6
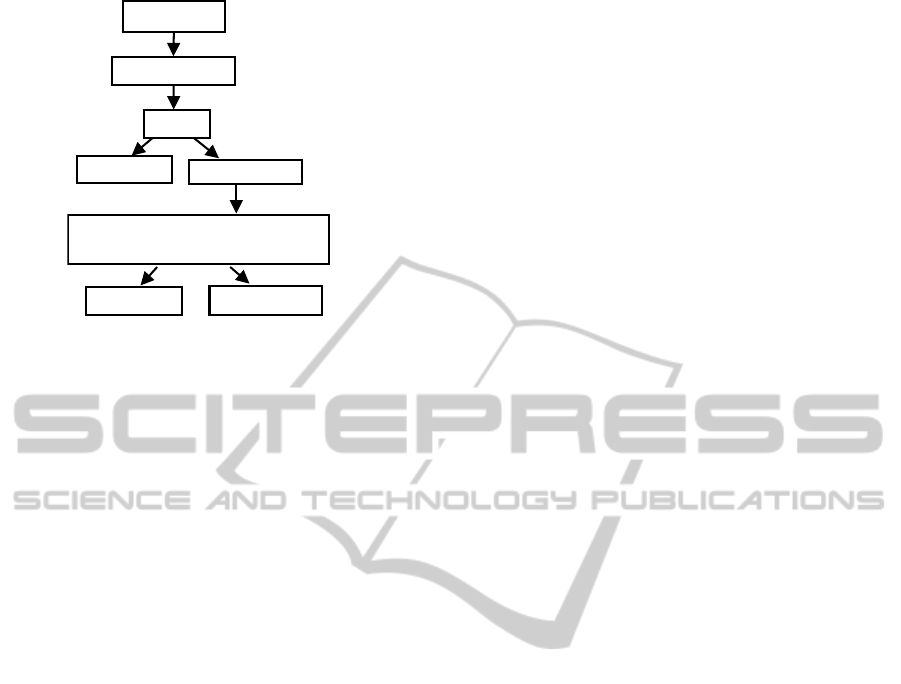
Cough persists
chest radiograph
Evaluate for three most common conditions
simply in the following order, or in
combination: 1. PNDS 2. Asthma 3. GERD
Cough gone
Cough persists
Cough gone
Cough persists
normal
Figure 1: Diagram providing a workflow-based view of
the recommendations R1) and R2) from the chronic cough
guideline for immunocompetent adult patients (Irwin et al.,
1998).
I: Evidence obtained from at least one properly
randomized controlled trial.
II: Evidence obtained from well-designed con-
trolled trials without randomization.
II-2: Evidence obtained from well-designed co-
hort or case-control analytic studies, preferably from
more than one center or research group.
II-3: Evidence obtained from multiple time series
with or without the intervention.
III: Opinions of respected authorities, based on
clinical experience.
We start by explaining our interpretation of rec-
ommendations R1) and R2):
R1)(a) Pregnant Patient or Young Non Smoker
with Presumed PNDS: behind the recommendation
of not routinely obtaining chest radiographs for preg-
nant women there is the implicit knowledge that the
X-ray exposes the embryo to radiation. It is known
that this desirability criterion (value) is intrinsic to
any X-ray based plan, although this is not explic-
itly explained in the chronic cough guideline. There-
fore for pregnant women this is a critical recom-
mendation supported by evidence of grade II-2. Be-
hind the recommendation of not routinely obtaining
chest radiographs before beginning treatment for pre-
sumed PNDS in young nonsmoker, or before observ-
ing the result of discontinuation of an ACEI there is
medical evidence also of grade II-2 which promotes
the value of maximizing the likelihood of diagnosis.
Behind this recommendation there is also the medi-
cal evidence of grade II-2 that for young nonsmok-
ers the probability of PNDS/Asthma/GERD is higher
than the average population, therefore it is more cost-
effective and less time consuming to skip Chest X-ray.
R1) (b) Patients forwhom Recommendation R1)(a)
does Not Apply (Not Pregnant and Not Young Non
Smokers with Presumed PNDS): therefore for this
class of patients obtaining a Chest X-ray is strongly
recommended based on evidence of grade II-2, pro-
moting the values of maximizing likelihood of diag-
nosis and maximizing cost-effectiveness because the
X-ray may contain results that can aid in making a
correct diagnosis.
R2) For the same reasons the opposite
recommendations apply to the treatment of
PNDS/Asthma/GERD with the same grade II-2.
This plan is recommended without necessarily doing
a Chest X-ray first, for pregnant women and for young
non-smokers with presumed PNDS. Quoting (Irwin
et al., 1998) ” PNDS either singly or in combination
with other conditions, is the most common cause
of chronic cough, followed by asthma and GERD”
(grade II-2), therefore the multi-treatment is recom-
mended to any patient to maximize the likelihood of
diagnosis. The treatment of PNDS/Asthma/GERD
should consider the following generic candidate
plans:
1) Sequentially treating PNDS, followed by treat-
ing asthma and finally treating GERD;
2) Sequentially treating two conditions while con-
currently treating the third condition (6 possible com-
binations);
3) Concurrently treating PNDS, asthma and
GERD: quoting (Irwin et al., 1998) ”Properly chosen
empiric therapy for PNDS should start to yield a fa-
vorable response within 1 week; for asthma within
1 week; for GERD within 1 week to 3 months”
(grade III). From this and the previous quote from the
chronic cough guideline that indicates that PNDS is
the most common cause of chronic cough we can de-
duce that to minimize the cost of the treatment PNDS
should not be preceded by the other treatments. The
reason is that if it is discovered that the chronic cough
is related to PNDS then all the other treatments can
be dropped.
Some of the benefits that can be obtained by incor-
porating value-based decision making in healthcare
have been considered in (McCartney, 2005) (Black
et al., 2009). Here we suggest simple questions that
can help to determine the level of compliance of a
medical recommendation based on its attached val-
ues:
• Which properties are related to the patient’s safe-
ness and therefore are critical to verify?
For the case of pregnant women the recommenda-
SEMANTIC PROCESS MINING FOR THE VERIFICATION OF MEDICAL RECOMMENDATIONS
7

tion R1)(a) of not performinga chest X-ray has as-
sociated the value of minimizing the risk of dam-
aging the embryo. This value is critical and there-
fore this property should be satisfied in every CIG
that models the chronic cough guideline from (Ir-
win et al., 1998).
• Which properties are not critical but are provided
with a high medical evidence and therefore should
be mandatorily enforced?
A good example of this type of criterion are the
following recommendations supported by medi-
cal evidence of grade II-2:
1) performing multi-treatment for pregnant
women in recommendation R1) (a); 2) per-
forming a chest X-ray and a multi-treatment for
asthma/GERD/PNDS for the case of young non
smoker with presumed PNDS in recommendation
R1) (a) and 3) performing a chest X-ray and
a multi-treatment to patients for whom the
recommendation R1) (a) does not apply.
• Which properties are related to the efficient use
of resources (time, money, medical staff, etcetera)
and can mainly suggest optional improvements in
the quality of medical treatment?
This is the case of the recommendation R2) sup-
ported with medical evidence of grade III that sug-
gests that the treatment of PNDS should not be
preceded by the treatment of Asthma and GERD
in order to minimize the cost of the treatment.
3 DECLARE MODEL
In this section we present the medical cough guide-
line (cf. Section 2) expressed in CIGDec (Mul-
yar et al., 2007) constraints. CIGDec is one of the
languages offered by the constraint-based Workflow
Management System DECLARE (van der Aalst and
Pesic, 2006; Pesic and van der Aalst, 2006) that can
be used to define constraint-based models. A lan-
guage in DECLARE is defined by a set of constraint
templates, each template having a name, a graphical
representation and an LTL expression. This allows
users to interpret DECLARE models without requir-
ing LTL knowledge while having precise semantics at
the same time.
Table 1 summarizes the CIGDec constraint tem-
plates used in the rest of this paper. From now on
we write DECLARE model when we refer to a DE-
CLARE CIGDec model. The state formulas of the
LTL expressions are tuples (A, t) where A is the task
parameter and t refers to the state of the task, i.e.
started (t
s
), executed (t
x
) or completed (t
c
). A con-
straint between tasks in the model is expressed by as-
sociating the parameters of the template for that con-
straint to the tasks in the model. For example, con-
sider the fifth template from the table. The response
constraint is used to express that every time activity
A executes, activity B has to be executed after it. B
does not have to execute straight after A, and another
A can be executed between the first A and the sub-
sequent B. To specify that task multitreatment is a
response to task xray, parameters A and B of the re-
sponse constraint are associated to the tasks xray and
multitreatment respectively. To avoid task xray to be
enacted more than once before task multitreatment is
enacted additional conditional mandatory constraints
exactly1 and absence2 are specified for task xray,
each applying to different conditions. The graphical
representation of the constraint contains the associ-
ated task instead of the parameters as can be seen in
Figure 2.
Verification of models is essential to detect mod-
eling errors. DECLARE offers verification to check
constraint-models for (1) conflicts, i.e. constraints
that can never be satisfied and (2) dead activities, i.e.
activities that can never be executed. An error mes-
sage about the problem and the cause helps the mod-
eler to understand and to resolvethe cause of the error.
The data perspective of DECLARE specifies how
data is handled throughout the executionof the model.
Data attributes can be specified and associated to rel-
evant tasks, e.g. the X-ray task reads the pregnancy
status of a patient. While executing a task, its data
attributes can be read or written, as specified for
that task at design-time. DECLARE also offers a
resource-perspective that specifies which tasks should
be executed by whom. An organization of roles and
people can be specified and associated with tasks.
Constraints that should only hold under some con-
dition can be specified as conditional constraints. A
condition is a boolean expression that can involvedata
attributes from the model. At any point during execu-
tion the condition evaluates to true of false, depending
on current the value of data attributes. When the con-
dition evaluates to true, the constraint is active, other-
wise the constraint is inactive. For instance, the preg-
nancy status of a patient can be used as condition for
constraints that should only be active for this group of
patients. In the graphical representation of a condi-
tional constraint the condition is displayed next to the
constraint.
By default constraints are mandatory (hard) con-
straints and DECLARE does not allow the execution
of tasks that violate one or more active constraint in
the model. In DECLARE it is also possible to specify
HEALTHINF 2011 - International Conference on Health Informatics
8
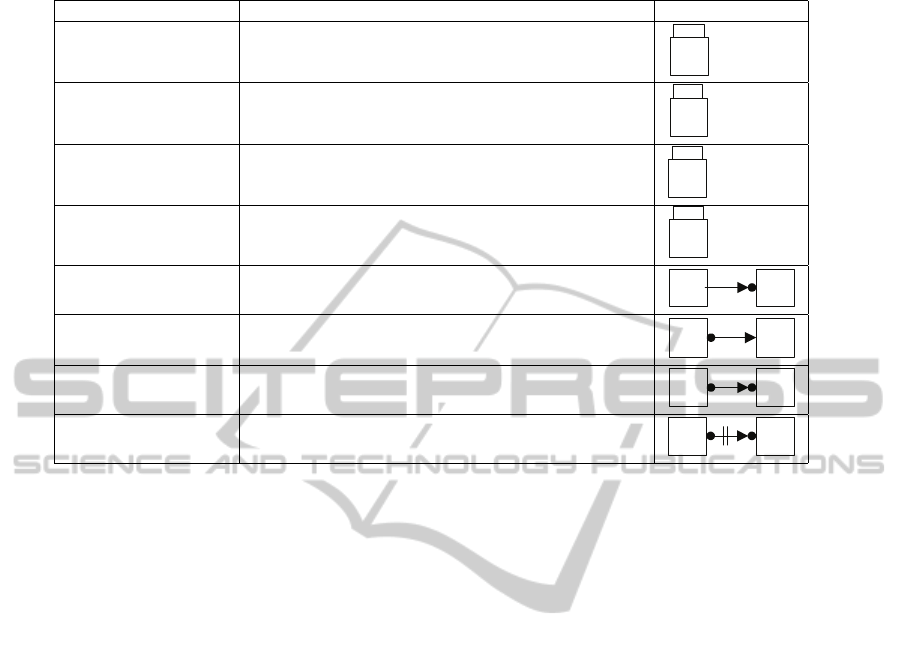
Table 1: Relevant CIGDec constraints.
Name LTL expression Graphical
init(A) ((A, t
s
) ∨ (A, t
x
))W (A, t
c
)
A
init
existence(A) ♦(A, t
c
)
A
1..*
exactly1(A) existence(c, A)∧!(♦((A, t
c
) ∧ °(existence(A))))
exactly1(A)
A
1
absence2(A) !(♦((A, t
c
) ∧ °(existence(A))))
absence2(A)
A
0..1
precedence(A,B) (!((B, t
s
) ∨ (B, t
c
) ∨ (B, t
x
)))W (A, t
c
)
A B
response(A,B) ¤((A, t
c
) ⇒ ♦(B, t
c
))
A B
succession(A,B) response(A, B) ∧ precedence(A, B)
A B
not succession(A,B) not response(A, B) ∧ not precedence(A, B)
A B
optional (soft) constraints that can be violated. Vio-
lations of mandatory constraints trigger warnings that
are specified for the violation of that constraint, ex-
plaining the violation and the consequence of the vi-
olation. Graphically, mandatory constraints are de-
picted as solid lines and optional constraint as dashed
lines.
Next, we explain how to model the recommenda-
tions from the chronic cough guideline (cf. Section
2) in DECLARE. The model contains the following
tasks that correspond to the activities from the cough
guideline depicted in Figure 1:
(1) choice has no equivalent in Figure 1 because
the case of pregnant patient or young non smoker with
presumed PNDS has not been modeled in (Irwin et al.,
1998) in order to simplify the diagram; we have added
it into the DECLARE model to differentiate between
the care path recommended for patients with the men-
tioned medical conditions (R1) (a)) and other patients
(R1)(b));
(2) xray that corresponds to acquiring an chest X-
ray;
(3) multitreatment that corresponds to the evalua-
tion of Asthma, GERD and PNDS;
(4) asthma that corresponds to the treatment of
Asthma;
(5) pnds that corresponds to the treatment of
PNDS;
(6) gerd that corresponds to the treatment of
GERD.
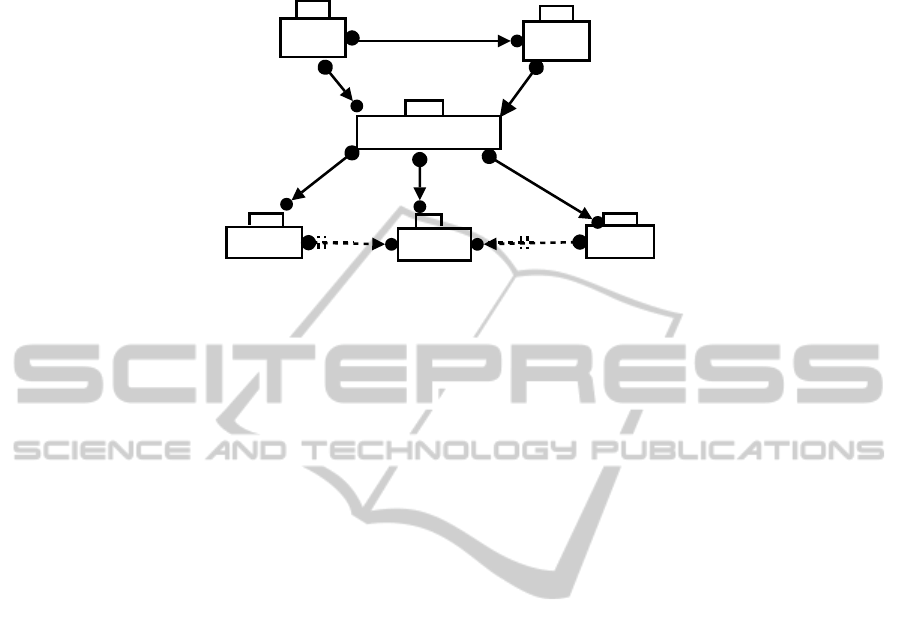
For clarification, constraints in Figure 2 are an-
notated with the corresponding guideline fragments.
The following general recommendations should al-
ways be satisfied:
RG1) The choice of ordering a chest X-ray is
made once (constraint exactly1 over task choice);
RG2) Performing the treatment of asthma, GERD
or PNDS more than once will not change the diagno-
sis therefore the constraint exactly1 is associated to
the tasks multitreatment, asthma, GERD and PNDS.
This restriction is related to the value of maximizing
the likelihood of diagnosis.
The general constraints are independent of the
patient’s medical condition, so these constraints do
not have conditions. The following boolean data at-
tributes (in italics) have been introduced to capture
the different conditions in the guideline. (1) cough is
true if the cough is persistent, (2) normalXray is true
if the result of the X-ray is normal, (3) pregnant is
true if the patient is pregnant, (4) young is true if the
patient is less than 18 years old, (5) smoking is true
if the patient is a smoker, (6) pnds is true if PNDS is
presumed. These six boolean data attributes are used
in the conditions of the next constraints.
The recommendation concerning the X-ray (R1)
is captured using mandatory conditional constraints.
For the case of pregnant patient or young non smoker
with presumed PNDS (R1 (a)) we consider condition
c which returns true when the patient belongs to the
mentioned class. When we consider recommendation
R1) (b) we use the negation of c denoted as !(c).
R1) (a) Pregnant Patient or Young Smoker with
SEMANTIC PROCESS MINING FOR THE VERIFICATION OF MEDICAL RECOMMENDATIONS
9
pnds
gerd
succession
cough
not succession
R2)ii.
R2)i.
asthma
succession
cough
succession
cough
R2)iii.
not succession
choice
xray
multitreatment
init
response
cough &&
normalXray
succession
c && cough
succession
!(c) && cough
absecen2 c&& cough
exactly1 !(c)&& cough
R1)(a)iv.
R1)(a)i.
R1)(a)ii.
R1)(b)ii.
R1)(a)iii.
R1)(b)iii.
R1)(b)i.
Figure 2: DECLARE model for the considered recommendations from the chronic cough guideline.
Presumed PNDS: according to the recommendation
R1 the care path for this class of patients corresponds
to first optionally performing a chest X-ray and then
if the cough persists treat for PNDS/Asthma/GERD.
Therefore, for patients who are pregnant or are young
smokers with presumed PNDS and have chronic
cough (c && cough) the following care path is rec-
ommended:
i. first the decision of performing a X-ray has to be
taken (init constraint over task choice);
ii. performing a X-ray is optional (conditional ab-
sence2 constraint in task xray);
iii. in the case that after the X-ray the patient has
persistent cough and the result of the X-ray is
normal (cough && normalXray) then eventually
the treatment for PNDS/Asthma/GERD has to
be started (conditional response relation between
tasks xray and multitreatment);
iv. it is possible to decide not to perform the Chest
X-ray and to immediately start the treatment
of PNDS/Asthma/GERD (conditional succession
between tasks choice and multitreatment). In this
case the enactment of xray task is not possible
anymore because it would violate the precedence
constraint between tasks choice and xray.
R1)(b) Patients for whom Recommendation R1)(a)
does Not Apply: according to the recommendation
R1 if cough persists the correct decision is to perform
the Chest X-ray and then in case of normal X-ray
avoid irritants. If after avoiding irritants the cough
persist then treat for PNDS/Asthma/GERD. There-
fore for patients with chronic cough who are not preg-
nant or are not young smokers with presumed PNDS
(!(c) && cough):
i. the result of the choice is to perform a chest X-ray
(conditional succession constraint between tasks
choice and xray).
ii. exactly one chest X-ray has to be done (condi-
tional exactly1 constraint on task xray);
iii. similarly to R1) (a) iii. if the result of the
X-ray is normal and the patient still has a
cough (cough && normalXray) then the multi-
treatment of PNDS/Asthma/GERD has to be
started (conditional response constraint between
tasks xray and multitreatment).
R2) Instead of specifying all possible combina-
tions of treatments, for PNDS, asthma and GERD
where the treatment of PNDS should not preceded by
the other treatments, it is enough to define the pre-
ferred scenarios by conditional constraints, that hold
in case condition cough is true:
i. a mandatory relation of conditional succession
between the task multitreatment and each of the
treatments, where the condition is that the patient
still has a cough (cough). This constraint has as-
sociated the value of maximizing the likelihood of
diagnosis;
ii. an optional negativerelationship of succession be-
tween asthma treatment and PNDS treatment, so
before treating PNDS the patient cannot be treated
for asthma and after treating for asthma the pa-
tient cannot be treated for PNDS. This constraint
has associated the value of minimizing the cost of
treatment;
iii. similarly to R2)ii. define an optional negativesuc-
cession constraint between GERD and PNDS.
Note that the translation of the preferred treatment
plan from recommendation (R2) to a declarative lan-
guage is straightforward.
HEALTHINF 2011 - International Conference on Health Informatics
10
4 SEMANTIC MODEL
CHECKING
The analysis and interpretation of natural language
medical recommendations can not be automated and
therefore can be error prone. In Section 2 we disam-
biguated the recommendations R1) and R2) from the
chronic cough guideline based on our interpretation
of the medical evidence provided in the guideline. In
this section we explain that once the medical recom-
mendations are modeled in a formalism that provides
a precise semantic, as CIGDec, it is possible to use the
formal model to automatically check if an arbitrary
CIG complies with the medical recommendations.
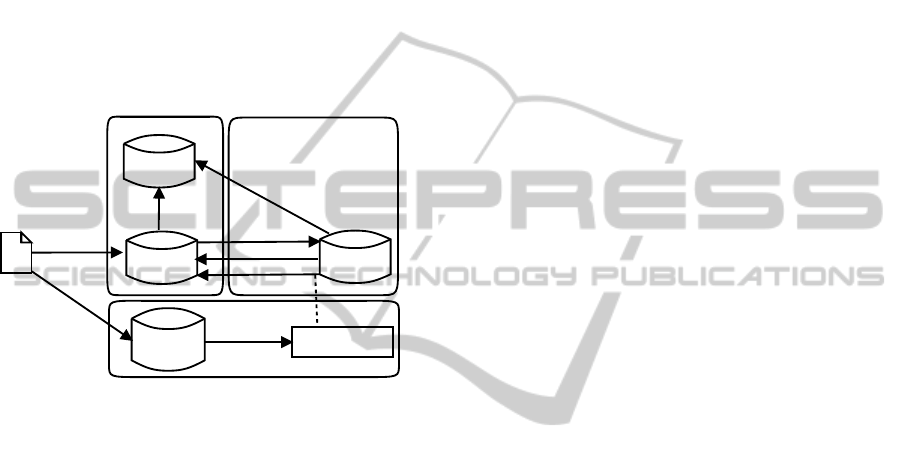
ontologies
CIGs
LTL constraints
Event logs
Declarative
constraints
medical
guidelines
DECLARE
ProMTallis
link to
3) link to
2) generate
4) discover
5) check
conformance
1) generate
Specified
by
Implemented
by
Figure 3: Steps required by the methodology proposed here:
1) Generate LTL constraints from the DECLARE model,
2) Generate logs by enacting the CIG in the Tallis engine,
3) Link ontologies, 4) Discover the model mined from the
event logs using ProM, 5) Check conformance using ProM.
The methodology proposed here to check the con-
formance in a CIG of the DECLARE specification of
medical recommendations is illustrated by Figure 3
and explained in detail below:
1) Generate LTL properties from the DECLARE
model: the DECLARE tool automatically generates
the LTL properties from the constraint model of the
medical recommendations explained in Section 3.
2) Enact the CIG to generate event logs: in Mor
Peleg et al. work (Peleg et al., 2003) the develop-
ers of Asbru (Shahar et al., 1998), GLIF, GUIDE,
EON and PROforma (Fox et al., 1997) languages
were asked to specify CIGs for similar recommenda-
tions to the ones we explained in Section 3. But the
developers of the CIGs did not have any access to the
chronic cough medical guideline from (Irwin et al.,
1998). The recommendations on which the study (Pe-
leg et al., 2003) was based on and the repository of
the resulting CIGs is available at the Open Clinical
repository (http://www.openclinical.org). None of the
CIGs from the repository have been used in any real
medical environment. Therefore, we decided to ex-
plain the methodology with the PROforma CIG from
the Open Clinical repository which has been enacted
using the Tallis engine (http://www.cossac.org/tallis).
But the strategy explained here requires the execution
history (event logs) of the CIG and therefore it is in-
dependent of the language used for the specification
of the CIG. An event log contains the executions of
one or more processes. To construct such log is the
required that each event in the log (e.g. an X-ray)
can be mapped to a single case or process instance
(e.g. a patient treated for cough) and that each pro-
cess instance can be mapped to a single process (e.g.
the process for treating chronical cough). The more
information is available in the log, the better the qual-
ity of the results and the larger the number of ques-
tions that can be answered. For instance, event time
stamps can be used to do performance analysis. Simi-
larly, every process instance has zero or more tasks.
Every task or audit trail entry must have at least a
name and an event type. The event type determines
the state of the tasks. Timestamps can be used for
capturing timing information and to analyze perfor-
mance related aspect. The originator element records
the person/system that performs the task. Because the
Tallis CIG specified for the chronic cough recommen-
dations has not been used in a real medical environ-
ment, the event logs have to be generated considering
generic patient cases. According to the DECLARE
constraints from Section 3 six different patient medi-
cal conditions are significant: (1) if the cough is per-
sistent, (2) if the result of the X-ray is normal, (3) if
the patient is pregnant, (4) if the patient is less than
18 years old, (5) if the patient is a smoker, (6) if
PNDS is presumed. But the enactment of the Tallis
CIG showed that the developers of the CIG also con-
sidered two additional medical conditions: (7) if the
patient has ACE-related cough and (8) if the cough
is productive. Therefore firstly generic patient cases
were created based on all the possible combinations
of the eight mentioned medical conditions. Secondly
the generic patient cases were used to enact the Tallis
CIG. This is a standard practice in software engineer-
ing when system’s correctness needs to be tested be-
fore the system’s release. Finally the events generated
during the CIG enactment were recorded as event logs
using the MXML (Mining eXtensible Markup Lan-
guage) format. The schema for the MXML format
is available at www.processmining.org. If the con-
sidered Tallis CIG would have be running in a real
medical context then so-called Process-Aware Infor-
mation Systems (PAISs) (Dumas et al., 2005) could
have been used to automatically generate the corre-
sponding event logs from anonymized real patient’s
data.
SEMANTIC PROCESS MINING FOR THE VERIFICATION OF MEDICAL RECOMMENDATIONS
11
file:///C:/Documents%20and%20Settings/Adela/Desktop/CoughActivities#
xray
task
pndsnonspecifictreatmentmultitreatmentgerddiscontinueaceichoiceasthma
CoughActivities
Cxr_reportPNDS_evaluationNon_specific_initial_treatmentInvestigationsGERD_evaluationDiscontinue_ACEIScheduling_decisionAsthma_evaluation
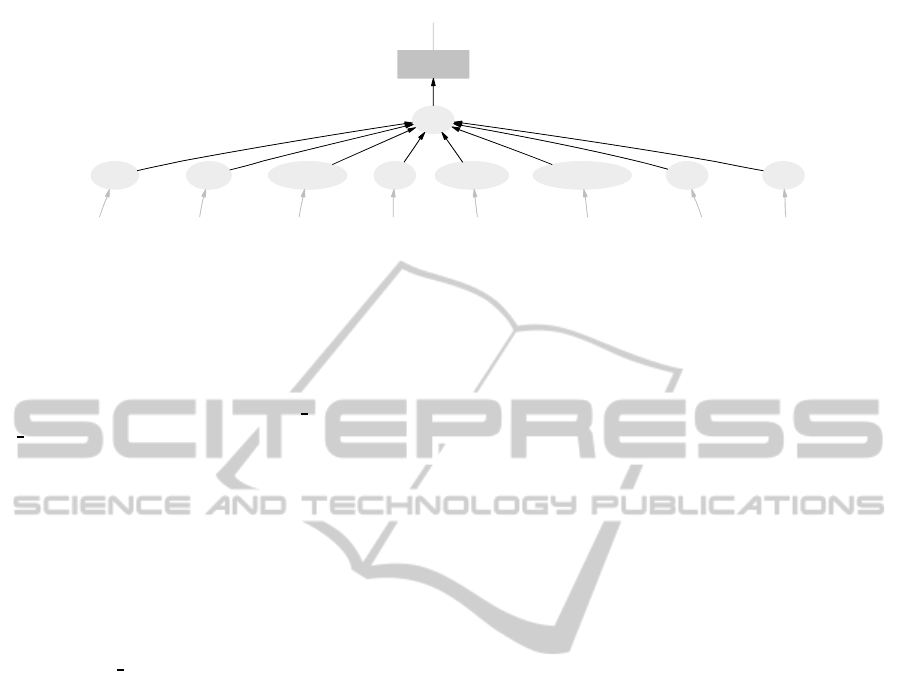
Figure 4: Ontology of activities, where the leafs are the annotated Tallis activities.
3) Link ontologies by semantically annotating the
event logs generated by the CIG: this requires map-
ping the concepts used in the CIG with the concepts
from the DECLARE specification. For instance as
Figure 4 shows the tasks Scheduling decision and
Cxr report from the Tallis implementation presented
here can be mapped into the semantically equiva-
lent concepts choice, xray from the DECLARE model
from Section 3.
Only after mapping concepts it is possible to ver-
ify if the DECLARE constraints are satisfied in the
mined model. For example the DECLARE constraint
that specifies that task choice has to be enacted ex-
actly once is verified in the model mined from the
Tallis implementation as the constraint that the Tallis
task Scheduling decision has to be enacted exactly
once.
The same DECLARE model used to perform the
conformance checking of the Tallis implementation
can be reused to check the conformance of any other
implementation from the Open Clinical repository on
which Mor Peleg et al. work (Peleg et al., 2003) is
based on. The only requirement is that previously
the corresponding mapping between the DECLARE
model and the new implementation has been done.
In particular from the DECLARE model from
Section 3 we can create ontologies for data, activities,
event types, process instances and originators (actors
who enact activities). We have called the ontologies
of data and activities CoughData and CoughActivi-
ties respectively. Figure 4 shows the graphical repre-
sentation of the ontology CoughActivites, where the
leafs correspond to the annotated activity instances
from the Tallis CIG. To perform the ontology link-
ing the MXML file generated in 2) is annotated with
concepts from these created ontologies. The resulting
semantic annotation is expressed in the SA-MXML
(Semantically Annotated MXML) format used by the
ProM framework. The SA-MXML format is avail-
able at www.processmining.org and it is an extension
of the MXML formant where all elements (except for
audit trail entries and time stamps) have an optional
extra attribute that links to a list of concepts in the on-
tologies. For instance in the SA-MXML log shown
in Figure 5 for the process instance with identifier
”Case0100a” the variables young and old from the
DECLARE ontology CoughData are linked by an at-
tribute to the variables younger and older from the
data ontology in the Tallis CIG.
4) Discover the PROforma model from the seman-
tically annotated event logs: using the alpha ++ algo-
rithm that is provided as a plug-in of the ProM frame-
work it is possible to extract (mine) the PROforma
model based on the dependency relations that could
be inferred among the activities in the Tallis event
logs from the SA-MXML file generated in 3). Fig-
ure 6 shows the resulting mined PROforma process
for generated event logs for the 64 combinations of
medical conditions.
5) Perform semantic conformance checking of the
discovered PROforma model: using the semantic LTL
checker plug-in from the ProM framework it is possi-
ble to perform semantic conformance checking of the
PROforma semantically annotated model discovered
in 4) and the DECLARE model from Section 3.
In Section 3 we explained that it is possible to dif-
ferentiate in DECLARE between medical recommen-
dations that are mandatory or optional.
Only if a DECLARE constraint is mandatory and
it is not satisfied in all the event logs generated from
the CIG, a warning should be given during confor-
mance checking. Otherwise if the DECLARE con-
straint is optional and not satisfied in all the generated
event logs it is considered that the CIG complies with
the recommendation though it is not optimal. The
level of satisfaction of a property can be seen as the
percentage of eventlogs that satisfy the property. This
information is provided by the semantic LTL checker
as two lists: the first list corresponds to the event logs
that satisfy the property and the second list contains
the event logs that do not satisfy that property.
In Table 2 we show the results of performing se-
HEALTHINF 2011 - International Conference on Health Informatics
12
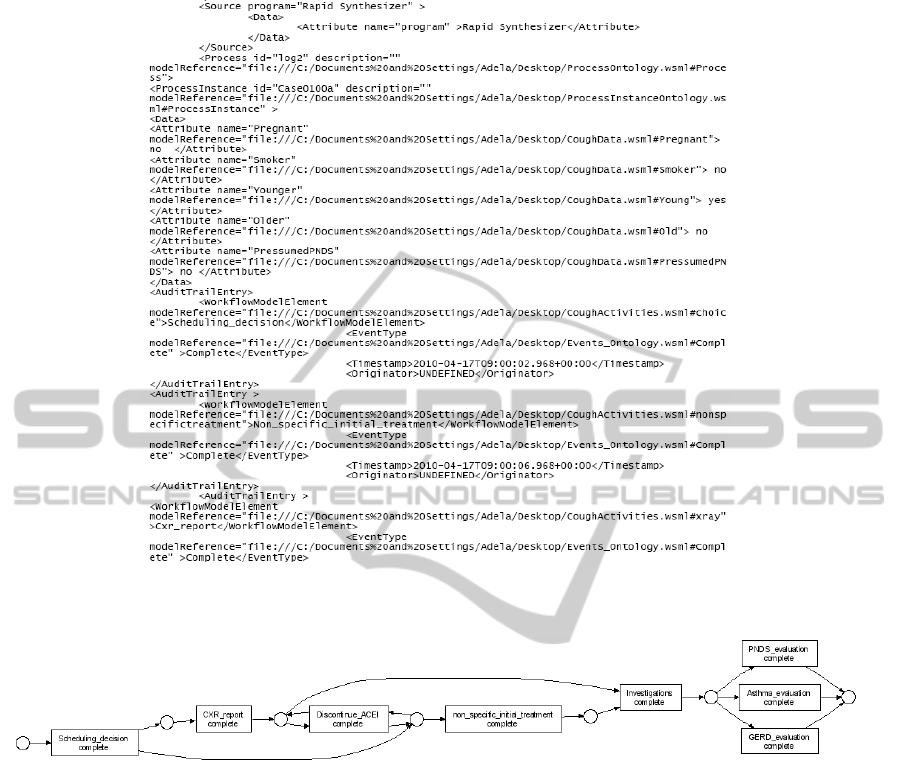
Figure 5: SA-MXML file of annotated event logs from the Tallis CIG for chronic cough.
Figure 6: Model of the PROforma CIG discovered by the ProM framework from the Tallis event logs.
mantic conformance checking as explained in Section
4 over the Tallis CIG.
For instance the recommendations R1)(a)ii. and
R1)(a)vi. for the case of pregnant women are re-
lated to the decision of performing a chest X-ray and
they have associated the value of minimizing the risk
of damaging the embryo. This value is critical and
therefore was modeled in Section 4 as mandatory DE-
CLARE constraints. We have shown that all the event
logs that we generated with the Tallis CIG satisfy
these properties.
We did not find any property that is fully unsatis-
fied by the generated event logs. For fully unsatisfied
properties the semantic LTL model checker returns an
empty list of event logs satisfying the property.
For the rest of the properties we showed that they
are partially satisfied by the Tallis CIG, it means that
some of the generated traces of the event logs are in
the first list generated by the semantic LTL checker
(traces satisfying the property) and some others are in
the second list (traces not satisfying the property). For
example this was the case of the non critical manda-
tory chronic cough medical recommendations R2)i.
which specifies that the diagnosis by multi-treatment
consists on evaluating for Asthma, GERD and PNDS.
Therefore a notification should be given in order to
inform that this recommendation has been violated
though it was mandatory. From the partial satisfaction
of this property and from the observation of the event
logs contained in each list computed by the semantic
LTL model checker we can infer that the PROforma
CIG was designed to ask the user to choose to evaluate
only one of the mentioned possible causes of chronic
cough.
SEMANTIC PROCESS MINING FOR THE VERIFICATION OF MEDICAL RECOMMENDATIONS
13

Table 2: Results of the semantic conformance checking of the medical constraints from the chronic cough guideline in the
Tallis CIG. A property can be unsatisfied (-), fully satisfied (+) or partially satisfied (+/-).
Medical DECLARE Natural Language Semantic
recommendation constraint checking
RG1) Non critical Only once it is possible to decide +
exactly1(choice) mandatory if a X-ray is performed
RG2) Non critical The diagnosis of asthma as cause of cough +/-
exactly1(asthma) mandatory is evaluated only once
RG2) Non critical The diagnosis of gerd as cause of cough +/-
exactly1(GERD) mandatory is evaluated only once
RG2) Non critical The diagnosis of PNDS as cause of cough +/-
exactly1(PNDS) mandatory is evaluated only once
RG2) Non critical The diagnosis by multi-treatment +
exactly1(multitreatment) mandatory is evaluated only once
R1)(a)i. Non critical Initially for any patient +
init(choice) mandatory decide if X-ray should be made
R1) (a)ii. Critical For pregnant women or young non smoker +
absence2(xray) mandatory with presumed PNDS X-ray is optional
R1) (a)iii. Non critical After X-ray multi-treatment should +
response(xray, multitreatment) mandatory be started
R1) (a)iv. Non critical For pregnant women or young non smoker +
response(xray, multitreatment) mandatory X-ray can be skipped
R 2)i. Non critical The muti-treatment consists on the +/-
succession(mutitreatment, asthma) mandatory treatment of asthma, GERD
succession(mutitreatment, PNDS) and PNDS
succession(mutitreatment, GERD)
R 2) ii. Non critical PNDS can not be preceded by +
not succession(asthma, PNDS) optional Asthma or GERD
not succession(GERD, PNDS)
5 SCENARIO-BASED ANALYSIS
Semantic conformance checking allows to automati-
cally show that certain properties are not satisfied by
a CIG. Here we propose a novel methodology to al-
low further automatic analysis over a CIG once the
semantic conformance checking was performedas ex-
plained in Section 4. Our methodology takes advan-
tage of: 1) the DECLARE specification of the medical
recommendation on which the semantic conformance
checking is based on, and 2) results computed by the
semantic LTL checker enacted in the ProM frame-
work.
The methodology is based on the scenarios gener-
ated by the DECLARE model which can be used to 1)
suggest event logs corresponding to unexplored criti-
cal behaviors of the CIGs, and 2) analyze if the CIG
is more or less restricted than the medical recommen-
dations that were used as starting point.
DECLARE models can be used to suggest signifi-
cant testing scenarios because they are provided with
algorithms to generate: the finite automata that cor-
responds to the scenarios that do not violate any con-
straint, and the finite automata that represents all the
possible scenarios that violate same of the model con-
straints (see (Pesic, 2008)).
The information provided by the automaton could
be used to:
1. Suggest classes of scenarios that comply
with/violate the medical recommendations. For
instance these scenarios can be used to generate
test cases to verify properties that are satisfied
because no event log could be use to check its
satisfaction.
2. Provide classes of scenarios that are generated by
the DECLARE model and therefore comply with
the medical recommendations but can not be gen-
erated by the CIG. The generated scenarios can be
used to verify if the CIG is more restricted than the
medical recommendations on which it is based.
For instance we can construct the automata that
generates all the scenarios which do not vio-
late the constraints defined by the DECLARE
model from Figure 2. According to this automata
there is a direct transition between the activities
choice and multitreatment for the class of pa-
tients corresponding to pregnant women or non-
smokers with presumed PNDS. This means that
it is possible to chose to start the muti-treatment
of asthma/PNDS/GERD without need to perform
before a chest X-ray. So in the mined PROforma
HEALTHINF 2011 - International Conference on Health Informatics
14

model (Figure 6) there should be a direct transi-
tion between the semantically equivalent activi-
ties Scheduling decision and Investigations. But
this is not the case, the enactment of activity
Scheduling decision is only possible if the activ-
ity Cxr report has been enacted before. From
this analysis we deduce that the mined PROforma
model is more restricted that the medical recom-
mendations from the DECLARE model: for the
class of pregnant women or non-smokers with
presumed PNDS the mined PROforma model
obliges to perform a X-ray, instead of offering it
as an option.
6 RELATED WORK
In this paper, we focussed on the problem of check-
ing a posteriori whether a CIG satisfies a set of medi-
cal recommendations specified in a declarative formal
notation. While in (Mans et al., 2009) they have ad-
dressed this problem a priori by first specifying the
medical recommendations as a Coloured Petri Net
(CPN) and then mapping the CPN into CIGs speci-
fied in different workflow-based language. It seems
that using this mechanism it should be possible to ob-
tain CIGs that are closer to the behavior described by
the medical recommendations modeled by the CPN,
but there is no claim in (Mans et al., 2009) that the
obtained CIG preserves all the behavior from the CPN
used as starting point.
An approach close to ours has been proposed in
(Stegers et al., 2006) as a strategy to identify and for-
malize in the Asbru (Shahar et al., 1998) language
goals (intentions) identified in clinical guidelines de-
scribed in natural language. Once the intentions are
formalized in the Asbru language they are suscepti-
ble of verification. Verification by theorem proving
has been proposed in (Teije et al., 2006) (Gendt et al.,
2005) to prove that protocols defined in the Asbru lan-
guage satisfy a set of desirable properties (medical
goals and quality indicators) and to find out ambigui-
ties, incompleteness (gasp in the information or insuf-
ficient information), inconsistencies or redundancies.
By theorem proving it is possible to guaranty the ab-
sence of errors, though this strategy is highly costly
because it requires to provide a mapping of the lan-
guage on which the CIG is implement into a theorem
prover. So far from the available languages for spec-
ification of CIG only the Asbru language provides
a mapping to a theorem prover. In contrast an ad-
vantage of the semantic conformance checking based
approach presented here is that it only requires the
process history and therefore it can be applied over
any CIG independently of the language used for its
implementation. This feature is very important, con-
sidering that currently there are numerous incompat-
ible languages available for the specification of med-
ical guidelines (Peleg et al., 2003). Nevertheless, us-
ing the LTL constraints that can be generated by DE-
CLARE also conventional model checking could be
used without needing event logs.
Semantic process mining techniques have been
successfully applied in the area of business process
managing (Casati and Shan, 2002) (Kharbili and
Stein, 2008) for all kinds of analysis of event logs,
like auditing, performance analysis, process discov-
ery, etc. In (Kharbili and Stein, 2008) a theoreti-
cal framework (not yet a detailed technical architec-
ture) has been proposed for verifying that a company
complies with with external and internal regulations
and policies. While more sophisticated than our ap-
proach, their work remains as a theoretical proposal.
The idea of using semantic process mining techniques
to analyze healthcare processes is not new. In (Mans
et al., 2008a) (Mans et al., 2008b) they extract rele-
vant event logs from real applications running in hos-
pitals’ information systems and they analyze these
logs using the ProM framework. Their results show
that process mining can be used to provide new in-
sights that facilitate the improvement of existing care-
flows. Their work differs from us on the fact that they
do not use semantic conformance checking to verify if
the medical recommendations on which the care pro-
cess is based are satisfied/violated.
7 CONCLUSIONS
In this paper we propose a technique for checking
the compliance of CIGs with respect to medical rec-
ommendations specified using a precise declarative
language. The technique is based on the execution
history of the CIGs and therefore can be applied at
post-execution time. Because the Tallis CIG that
we used as case study has not been used in a real
medical environmentwe have manually generated the
event logs by: 1) creating significant classes of patient
cases, 2) enacting the CIG with the classes from (1),
3) recording the resulting events as event logs. But
the event logs could be automatically generated from
real medical applications by using available PAISs
(Dumas et al., 2005). PAIs have been successfully
used before for analyzing non-trivial careflow pro-
cesses, where the patient’s real data has been pre-
viously anonymised. For instance in (Mans et al.,
2008b) they have analyzed a group of 267 gyneco-
logical oncology patients treated in 2005 and 2006 in
SEMANTIC PROCESS MINING FOR THE VERIFICATION OF MEDICAL RECOMMENDATIONS
15

the AMC hospital in Amsterdam, covering diagnostic
and treatment activities.
Taking in to account that existing medical recom-
mendations are periodically revised/updated and new
medical recommendations can be added, the run-time
prevention and detection of violations to medical rec-
ommendations and policies is an important problem
to consider. Some formal frameworks like (Grando
et al., 2010) are available in the field of health in-
formatics for specifying exception managers to de-
tect and recover from undesirable states happening
during the enactment of CIGs. But so far no strat-
egy has been proposed to automatically suggest the
scenarios or states that violate the medical policies
and recommendations. As we explained in Section
5, from DECLARE models it is possible to automat-
ically generate the automaton that describes all the
scenarios that violate the model constraints. In the
future we are interested on considering the incorpo-
ration of the scenario-based information provided by
the DECLARE models into exception manager sys-
tems like (Grando et al., 2010).
ACKNOWLEDGEMENTS
The authors would like to thank the LOIS initiative
at TU/e and the NWO project ”MinAdept” for their
support.
REFERENCES
Black, E., Glasspool, D., Grando, M. A., Patkar, V., and
Fox, J. (2009). Goal-based decisions for dynamic
planning. In AIME, pages 96–100.
Casati, F. and Shan, M. C. (2002). Semantic analysis of
business process executions. In EDBT, pages 287–
296.
Dumas, M., van der Aalst, W., and ter Hofstede, A. H.
(2005). Process-Aware Information systems: Bridg-
ing People and Software Through Process Technology.
Wiley.
Fox, J., Johns, N., Lyons, C., Rahmanzadeh, A., Thomson,
R., and Wilson, P. (1997). PROforma: a general tech-
nology for clinical decision support systems. Com-
puter Methods and Programs in Biomedicine, 54(1-
2):59–67.
Gendt, M. V., Teije, A. T., Serban, R., and Harmelen, F. V.
(2005). Formalising medical quality indicator to im-
prove guideline. In LNAI, editor, Proceedings AIME
conference, volume 3581, pages 201–220.
Grando, M. A., Peleg, M., and Glasspool, D. (2010). A
goal-oriented framework for specifying clinical guide-
lines and handling medical errors. J Biomed Inform,
43(2):287–299.
Irwin, R. S., Boulet, L. S., Cloutier, M. M., and et al (1998).
Managing cough as a defense mechanism and as a
symptom, a consensus panel report of the american
college of chest physicians. Chest, 114(2):133–181.
Kharbili, M. E. and Stein, S. (2008). Policy-based seman-
tic compliance checking for business process manage-
ment. In MobIS Workshops, pages 178–192.
Mans, R., Schonenberg, H., Leonardi, G., Panzarasa, S.,
Cavallini, A., Quaglini, S., and van der Aalst, W. M. P.
(2008a). Process mining techniques: an application to
stroke care. In MIE, pages 573–578.
Mans, R. S., Schonenberg, H., Song, M., van der Aalst, W.
M. P., and Bakker, P. J. M. (2008b). Application of
process mining in healthcare - a case study in a dutch
hospital. In BIOSTEC (Selected Papers), pages 425–
438.
Mans, R. S., van der Aalst, W. M. P., Russell, N. C., Bakker,
P. J. M., Moleman, A. J., and et al (2009). From re-
quirements via colored workflow nets to an implemen-
tation in several workflow systems. Transactions on
Petri Nets and Other Models of Concurrency, 3:25–
49.
McCartney, J. J. (2005). Values based decision making
in helathcare: Introduction. Journal HEC Forum,
17(1):1–5.
Mulyar, N., Pesic, M., van der Aalst, W., and Peleg, M.
(2007). Declarative and Procedural Approaches for
Modelling Clinical Guidelines: Addressing Flexibil-
ity Issues. In Informal Proceedings of the Interna-
tional Workshop ProHealth 2007, pages 17–28. QUT,
Brisbane, Australia.
Peleg, M., Tu, S. W., Bury, J.,Ciccarese, P., Fox, J., and et al
(2003). Comparing computer-interpretable guideline
models: A case-study approach. J Am Med Inform
Assoc, 10(1):52–68.
Pesic, M. (2008). Constraint-based workflow management
systems: Shifting controls to users. PhD thesis, Beta
Research School for Operations Management and Lo-
gistics, Eindhoven.
Pesic, M. and van der Aalst, W. M. P. (2006). A declarative
approach for flexible business processes management.
In Business Process Management Workshops, pages
169–180.
Shahar, Y., Miksch, S., and Johnson, P. (1998). The Asgaard
Project: A task-specific framework for the application
and critiquing of time-oriented clinical guidelines. Ar-
tificial Intelligence in Medicine, 14(1-2):29–51.
Stegers, R., Teije, A. T., and van Harmelen, F. (2006). From
natural language to formal proof goal, structured goal
formalisation applied to medical guidelines. In Proc
Int Conf on Knowledge Engineering and Knowledge
Management, volume 4248, pages 51–58. LNCS.
Teije, A. T., Marcos, M., Blaser, M., and et al (2006). Im-
proving medical protocols by formal methods. AI in
Medicine.
van der Aalst, W. and Pesic, M. (2006). DecSerFlow: To-
wards a truly declarative service flow language. In In-
ternational Conference on Web Services and Formal
Methods 2006, volume 4184 of LNCS, pages 1–23.
springer.
van Dongen, B. F., de Medeiros, A. K. A. A., Verbeek, H.
M. W., Weijters, A. J. M. M., and van der Aalst, W.
M. P. (2005). The ProM framework: a new era in
process mining tool support. volume 3536. LNCS.
HEALTHINF 2011 - International Conference on Health Informatics
16
