
Pervasive secure electronic healthcare records
management
Petros Belsis
1
, Apostolos Malatras
2
Stefanos Gritzalis
1
Christos Skourlas
3
, Ioannis
Chalaris
3
1
Department of Information and Comnmunication Systems Engineering, University of the
Aegean, Karlovasi, Samos, Greece
2
Department of Electronic Engineering, Centre for Communications Systems Research,
University of Surrey, UK
3
Department of Informatics, Technological Education Institute, Athens, Greece
Abstract. Pervasive environments introduce a technological paradigm shift,
giving a new impetus to the functionality of applications, overcoming
applicability barriers of legacy applications. Electronic healthcare records
management can clearly benefit from the new challenges brought by this
emerging technology, due to its low cost and high percentage of user adoption.
Still, the sensitivity of medical data, poses new requirements in the design of a
secure infrastructure based on the ad-hoc networking schema, which underlies
pervasive environments. User authorization and controlled access to
information is of outmost importance. This paper proposes a management
system for electronic healthcare records satisfying the aforementioned security
requirements.
1 Introduction
The rapid establishment of wireless technologies and their applicability to a wide
range and of various requirements environments, enables – among others – medical
domains with extended functionalities, providing their users with information
accessible at any time and independently of location within their range. The
continuous growth in the use of mobile devices and their relatively low cost causes a
shift from traditional applications and stable networking infrastructures, to the one
based in Mobile ad-hoc networks and other ubiquitous communications enablers.
These networks, pose new security challenges to electronic healthcare records
domain, due to the sensitivity of the data transmitted over insecure, wireless links; as
well as due to the instability of the infrastructure, which consists of several temporary
participating nodes. A major concern is brought by the mere notion of access to
everyone, everywhere that pervasive systems employ, as this contradicts every well-
known security principle.
Pervasive infrastructures are relying upon the concept of mobile ad-hoc networks
(MANETs) [1]. This can be considered as a serious drawback due to the versatility of
nodes. Therefore, MANETs should not be adopted as a universally acceptable
Belsis P., Malatras A., Gritzalis S., Skourlas C. and Chalaris I. (2005).
Pervasive secure electronic healthcare records management.
In Proceedings of the 2nd International Workshop on Ubiquitous Computing, pages 101-110
DOI: 10.5220/0002572801010110
Copyright
c
SciTePress

solution for every networking problem. Node mobility can lead to network instability,
and requires the adoption of pioneering solutions and innovative design in both the
underlying protocols as well as the supporting infrastructure.
IT enabled healthcare support on the other hand, raises constant demands for the
establishment of high quality services, accessible anywhere within a medical
department, leading thus to a utilization of mobile infrastructures. Though many
enterprise solutions exist for wireless applications they confront to conventional
security mechanisms [2], which fail to meet the extensive requirements of ubiquitous
environments. This dynamic environment imposes several additional security
requirements mainly related to the access control mechanisms for the sensitive,
private healthcare records information.
We are addressing the problem of providing transparent access to patient’s records
within a distributed coalition among medical domains. We discuss the notions
encompassing issues relative to the secure provision of transparent access to text
resources (medical files), according to a policy based management framework. In
order to prove the validity of our assumptions, we argue about a set of implementation
choices incorporated through our prototype, the functionality of which and scalability
potential is continuously rising.
The rest of this paper is organized as follows: Section 2 discusses related work and
motivations for our work. Section 3 provides our requirements analysis for the
proposed system design architecture; section 4 discusses our policy based
management framework, while section 5 provides implementation details and an
evaluation framework. Section 6 concludes the paper, providing directions for future
and ongoing work.
2 Related work
2.1 Health records management
Electronic health records management attracts significant international interest [3] and
sets the scenery for the establishment of a distributed, coalition-based, security policy
enhanced records exchange framework among different medical domains. Several
European projects have proposed candidate solutions for secure inter-operations
between medical domains [4]. In the HARP project, security profiles related with
access rights are dynamically downloaded to the client side. The MEDITRAV EU-
project attempts to overcome national or linguistic barriers by adopting the solution of
a multilingual portable personal record. Security implications of medical records
treatment are discussed in [5] [6]. These approaches, pose mainly their research effort
on the security requirements for effective electronic health record management, still
they confront mainly to stable infrastructures; on the other hand, requirements
necessary for the dynamic nature and diverse characteristics of versatile mobile ad-
hoc networks are totally neglected. In [2] pervasive patient record management is
discussed, yet authentication schemes are based on a totally different model, this of
decentralized trust management [7]
102

2.2 Wireless healthcare applications
Wireless mediCenter [8], is a system for management of electronic medical records
and delivery through secure LANs or high-speed wireless connections. It provides
different portals for doctors and patients in order to achieve classification of access
permissions. It does not provide a flexible secure management framework for
cooperating medical domains, while its scalability potential is considerably low. The
m-Care project [9], aims at providing secure access through a WAP based
architecture. Users and access rights related information is kept in an MS-SQL Server
database. As its security model is based on simple access control lists its flexibility
and efficiency concerning to maintaining access rights related information is seriously
questioned.
3 Design choices
3.1 Requirements analysis
Effective design and implementation of pervasive health care applications should be
driven by a number of requirements, related mainly with the sensitive nature of
patient’s medical records data content. These requirements are mostly dictated by the
mere nature of the communications paradigm we have adopted, that of pervasive
technologies. In order to handle these issues from both a technical perspective as well
as for compliance purposes with the legislative principles enforced by EU directives
relative to sensitive data protection, we adopted a number of implementation choices
in our project, covering various issues, not treated so far by other similar approaches.
Such issues are:
• Policy driven approach. We argue that policy driven approach is more
suitable for medical environments, since the trust based model maps
unknown roles to users and therefore assigns privileges to them accordingly
to the reputation collected for them for other models. We believe that this
model is suitable for environments characterized by total adhocracy and
absence of well stated organizational policy, still it cannot be applied to well
policy configured, medical environments.
• Concern about the limited resources in terms of processing power, memory
or energy supplies. The presence of devices with sufficient resources should
not be considered the rule, but rather the exception.
• Agent based discovery and authentication. In order to perform a patient’s
related record identification among a number of domains in a distributed
environment, we utilize software agents, which through the means of a
predefined ontology they communicate and collect information on the user’s
behalf.
103
3.2 System Architecture
The need to create a pervasive environment based on transparent and secure
dissemination of health records among authorized users is the driving force behind
our framework. In a traditional stable networking infrastructure, access to medical
records -presuming a policy based approach- can be materialized through a single
policy interpretation and decision point, where a user performs a request to log on to a
certain service and security considerations are handled within the service’s
framework, providing therefore access only to users having the necessary level of
clearance. This centralized policy interpretation approach is totally inapplicable to our
environment, where instability is a main characteristic. Furthermore, providing a
similar architecture based on nodes with reduced reliability can direct to the provision
of a single point of failure. Due to the absence of stable links, there is a wireless
interconnection of all the devices, therefore providing access to all edges of the virtual
network. Our approach builds upon utilizing a hybrid set of both stable devices and
mobile devices. The focal points of the system, where role and policy repositories
reside and authentication occurs are supported by redundant identical entities to
ensure continuous and uninterrupted operation. In addition, the selection of the
devices to host these services occurs not in a random manner, rather by taking into
account the device relative stability in the volatile network topology.
Through the provision of user agents, implemented in the JADE platform [11], and by
means of a predefined ontology developed on Protégé [12] ontology editing tool, we
automate the medical records identification procedure. The usage of ontology is a
prerequisite in order to standardize the terminology concepts exchanged between the
agents. Table 1a provides a sample of an Agent Communication Language (ACL)
message exchange based on our role hierarchy ontology for the medical domain.
Table 1b defines an ACL message according to the FIPA-query protocol [13],
expressing the validity of the previous role assignment hierarchy.
Table 1a (left). Expression of an SL type definition of role hierarchy presenting that Doctor
and nurse in oncologist clinic have different hierarchy –and therefore permissions
classification. Table 1b (right). Example of ACL message based on the previous ontology
according to the FIPA-query- agent interaction protocol.
(ANCESTOROF
:source (ROLE
:name oncologist
:definedBy (DOMAIN
:name OncologyDept))
:target (ROLE
:name nurse
:definedBy (DOMAIN
:name OncologyDept))
(inform
:sender (agent-identifier :name agentA)
:receiver (set (agent-identifier :name agentB))
:ontology auth-ontology
:language fipa-sl0
:protocol fipa-query
:content
“(ANCESTOROF
:source (ROLE
:name doctor
:definedBy (DOMAIN :name OncologyDept))
:target (ROLE :name nurse
:definedBy (DOMAIN :name OncologyDept))”))
104

Several considerations needed to be taken due to the instability of the wireless
connections. Mainly we confront to security concerns, ensuring there will be no
breach in confidentiality of medical records. In order to retain the scalability potential
and support for large number of roles, we confront to the Role Based Access Control
(RBAC) [18] framework. The storage of access control information especially on
distributed environments where the number of assets to be managed grows
progressively - as well as the number of users- and cannot be efficiently managed
through the usage of contemporary authentication and access control schemes, such as
Access Control Lists (ACL’s). The usage of policies and policy languages can
simplify the management of distributed systems, which contain of large number of
objects which often span across organizational boundaries [19]. We adopted in our
approach the eXtensible Access Control Markup Language (XACML) [10], through
which we achieve platform independency and support interoperability characteristics
of the system in its entity; XACML can be codified in eXtensible Markup Language
(XML) which is specially designed to perform as interoperable data codification
format, suitable for integration to several platforms, such as Web Services and other
Web based environments.
4 Access control decisions on distributed health environment
Due to the dynamic nature and the presence of different roles from several medical
domains (i.e. hospitals) we have to ensure prior to a record distribution that the proper
access rights are maintained by a specific role requesting access to a resource. A
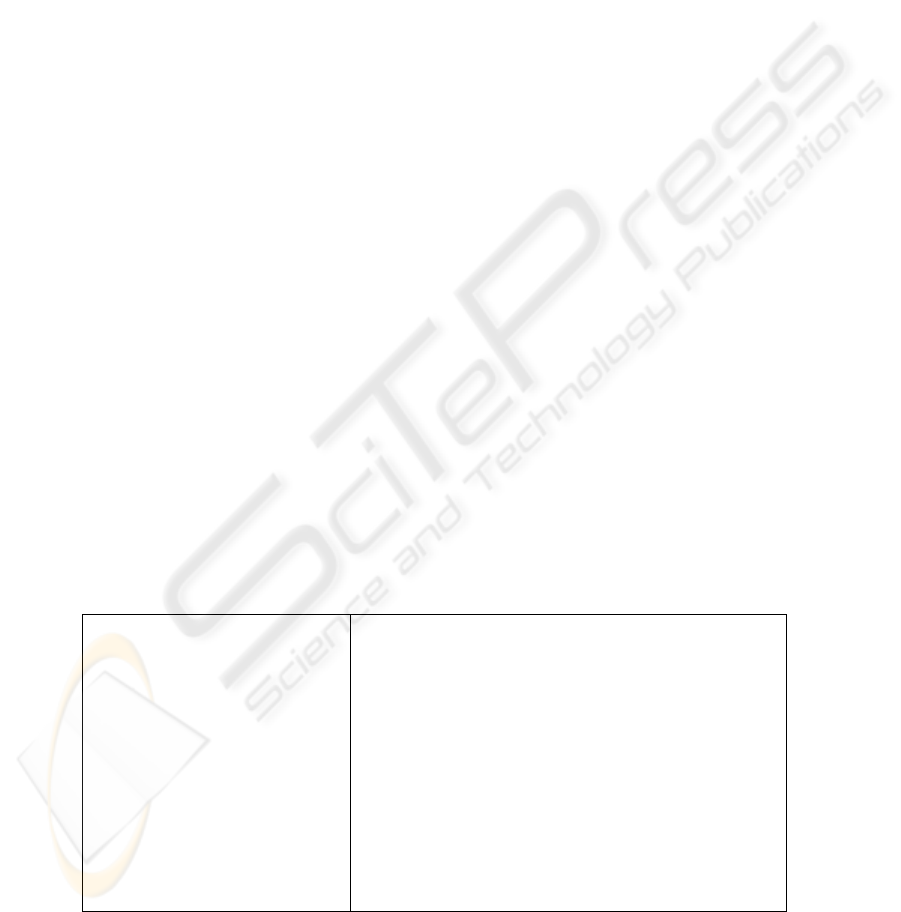
suitable management framework is that of the XML based XACML access control
language. This model in general operates as depicted in Fig 1.
The administrator is editing the policy and makes it available to the Policy
Decision Point (PDP). When a request is made, it is directed to the Policy
Enforcement Point (PEP). Now the PEP directs the request to the PDP which prior to
inspecting the request’s compliance with the predefined policy, requests additional
context information from the Context Handler. Accordingly the PDP authorizes or not
the requester and provides access to the service. Several security considerations arise
when it comes to the applicability of this scheme to our framework. First, in a single
domain environment there is a well-defined role and associations upon them,
hierarchy. This is inapplicable here, where several participating domains with
different role hierarchies, different roles and permissions are involving. In order to
enable this cooperation scheme therefore we adopted the following solution. Each
domain has its well-defined policy based on the grounds of the policy language. We
create a global role hierarchy scheme, and prior to different domain participation, the
administrators have to pre-establish a role mapping of the joining organization to the
global hierarchy scheme. Administrators are aware of the ethical and legal
implications of an incorrect role assignment, as well as they are aware of the policy
language specifications in order to perform role assignment.
105
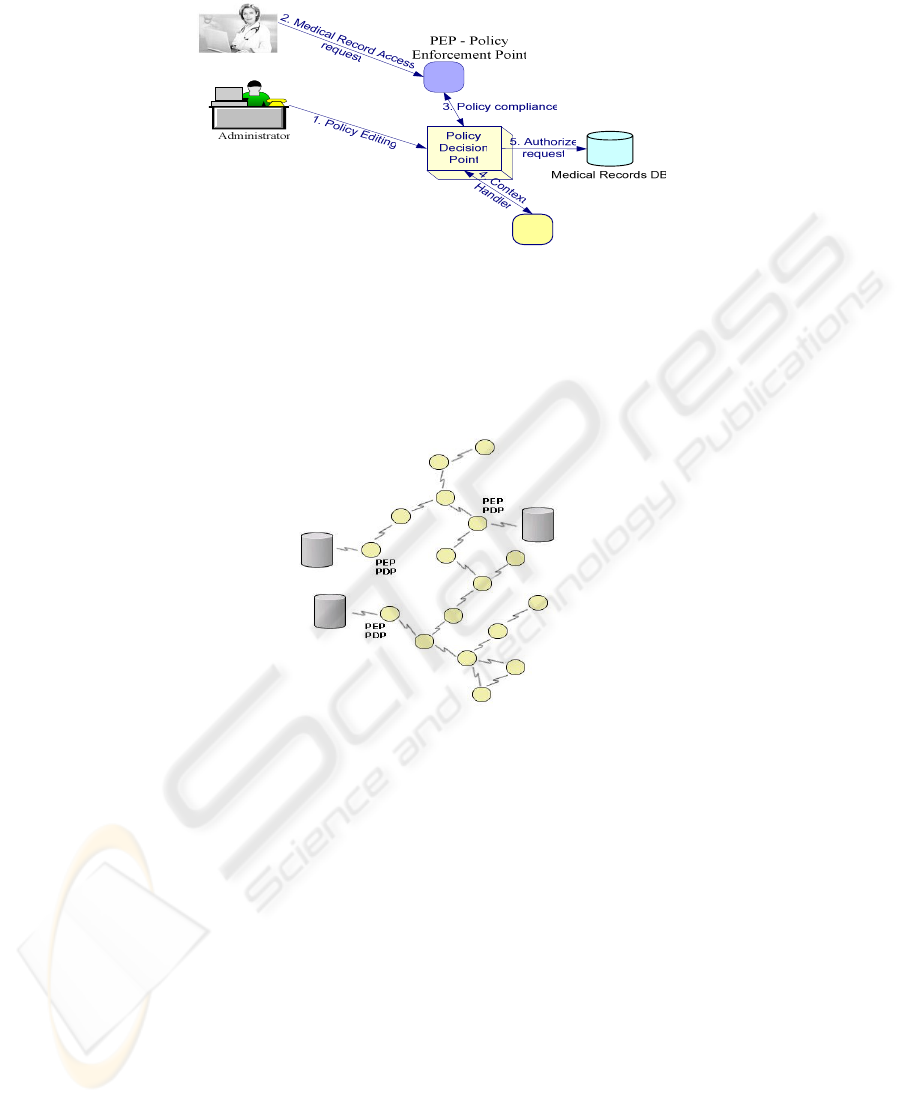
Fig. 1. XACML access control framework overview
This mapping is not enough though, due to the topology of the network, which cannot
be based on a single policy enforcement and decision point. Therefore, we consider
several nodes to play the role of PEPs and PDPs employing well established and
documented techniques of redundancy proposed for the unstable pervasive
environment. Each node that provides direct access to medical records has to be able
to enforce policy decisions [Fig 2] to control access to this information.
Fig. 2. Adjustment of XACML model to pervasive infrastructures
5 Implementation details
In order to test the validity of our framework, we experimented with a set of 4 laptops
(INTEL Centrino’s and Mobile Celeron’s) containing wireless cards, which played
the role of the mobile nodes. We implemented different role hierarchies for three
medical domains, edited on Protégé ontology development kit. We used as an
example an oncology clinic, a cardiology clinic and a general clinic. For each clinic
we implemented the WardManager role, the doctor role (oncologist, cardiologist) a
nurse role and a patients role. We presume that the general clinic role hierarchy
functions as the federal role hierarchy, to which the other domains have to confront.
For patients we created a simple historic record, consisting of their name and lab test
results, recorded in XML format (Fig. 4).
106

Patients and nurses were defined to view only personal details; doctors and wards
were authorized to view lab tests also. We considered all nodes to contain several
medical records. XACML enables context-based authorization, based on the domain.
By forming an appropriate XACML request message, the PDP was able to define
whether the specific user was authorized or not, by identifying his role and the
domain he belongs to (defined as part of his personal data). Our framework is dealing
with high-level security considerations in pervasive environments. We used standard
encryption schemes (WEP) for the lower communication levels, in order to avoid
eavesdropping or identity tampering.
The Java platform, J2SE 1.4, was the basis of our implementation due to the need
for interoperability amongst the variety of platforms that can be found in pervasive
environments. Another reason was the immediate integration with the JADE agent
platform that forms the basis of our proposed approach. We understand that the
Standard Edition of the Java Runtime that we used is processing demanding for small
mobile devices, but we consider switching to J2ME when testing with such devices in
the future. The Apache Xerces2 XML Parser handles XML processing, since it
widely adopted and viewed as the baseline solution to Java-based XML parsing.
Moreover and in accordance to the previous statement, lightweight XML processing
in the future will be handled by the kXML2 Parser, which is targeted to small devices
with limited resources and is J2ME compliant.
Fig. 3. Overview of pervasive health records management framework.
6 Conclusions
Security is a major issue in medical environments. Electronic patient record’s
management poses new challenges when it comes to its applicability to pervasive
environments. Such a framework can prove to be beneficial to all roles related with
such an environment, including doctors, nurses, and patients. In a real life scenario,
the doctor can acquire at anytime and any place within the range of a hospital,
information relative to patient’s medical history, previous treatments or medication,
by simply using his mobile device (Fig. 3) (enabled with 802.11b, Infrared, or
Bluetooth communication capability).
107

Pervasive environments are built upon mobile ad-hoc networks. Adaptations and
extensions [14] of classical topology-based routing protocols known from static
networks are coping with the problem of permanent link failures due to device
mobility. Furthermore, except form this adaptation to network protocols design, due
to their unstable architecture, they demand a totally innovative design of their security
management scheme. The large number of users and roles coming from different
domains requires further considerations concerning the deployment and enforcement
of security decisions. Our approach is policy-based, confronting with the RBAC
access control model. Additively, we provided a flexible solution for the multi-
domain role equipollence problem and we redesigned the XACML policy
enforcement scheme in order to become applicable to pervasive environments. We
adjusted the standardized XACML based authorization scheme to a distributed
architecture, suitable for the instability issues that characterize MANET’s
infrastructures.
Another characteristic of our approach is the transparency it provides, based on
the utilization of software agents. The agents were implemented in the JADE
platform, and were used for identification of medical records related to a specific
patient, as well as for performing authorization procedures transparently to the user,
by providing to the PDP the user’s credentials. This transparent identification and
authorization scheme, utilized concepts described in [15]. We plan to expand our
experimentation by utilizing protocols such as these described in [16] [17], and to
apply the scenario on a more complex hardware infrastructure.
Acknowledgments
The authors would like to thank John Varnas for providing assistance with the
drawings. We would also like to thank the anonymous reviewers for their insightful
comments.
This work was co-funded by 75% from E.E. and 25% from the Greek Government
under the framework of the Education and Initial Vocational Training Program –
Archimedes.
References
1. Perkins, C. E., Ad Hoc Networking, 2001 Addison Wesley Longman Inc.
2. A. Choudhri, L. Kagal, A. Joshi, T. Finin, and Y. Yesha, “PatientService : Electronic
Patient Record Redaction and Delivery in Pervasive Environments”, Fifth International
Workshop on Enterprise Networking and Computing in Healthcare Industry (Healthcom
2003), Santa Monica, June 2003
3. Scott R.E., Jennet P., Yeo M. Access and authorization in a Global e-Health Policy context.
International Journal of Medical Informatics (2004) 73, 259-266.
4. Ruotsalainen P. “A cross platform model for secure Electronic health record
communication”, International Journal of Medical Informatics, (2004) 73, 291-295
5. Kokolakis, S., Gritzalis, D. and Katsikas, S. (1998a). Generic security policies for
healthcare information systems. Health informatics journal, 4(4), 184-195.
108

6. Katsikas, S. and Gritzalis, D. (1996). High level security policy guidelines. In The
SEISMED Consortium (eds), Data security for health care. IOS Press, Amsterdam.
7. M. Blaze, J. Feigenbaum, J. Ioannidis, and A. Keromytis. The keynote trust management
system version. Internet RFC 2704, September 1999
8. Wireless Medicenter. http://www.wirelessmedicenter.com/mc/glance.cfm
9. David Brazier, Alpha Bravo Charlie Ltd. The m-care project. http://www.m-
care.co.uk/tech.html
10. Organization for the Advancement of Structured Information Standards (OASIS),
‘‘XACML Extensible access control markup language specification 2.0’’, OASIS Standard,
(available at http://www.oasis-open.org
11. The JADE agent development kit. Available at http://jade.tilab.com/
12. Protégé ontology development kit. http://protege.stanford.edu, (2004)
13. FIPA Standard Status Specifications. www.fipa.org/repository/standardspecs.html
14. Elizabeth M. Royer and Chai-Keong Toh. A review of current routing protocols for ad-hoc
mobile wireless networks. IEEE Personal Communications, pages 46.55, April 1999.
15. Belsis P., Gritzalis S., ‘‘Distributed autonomous Knowledge Acquisition and Dissemination
ontology based framework’’, Proceedings of “Interop” Workshop on Interoperability, H.
Kuehn ed., November 2004, Vienna, Austria, pp. 100-104
16. R. Friedman, M. Gradinariu and G. Simon, “Locating cache proxies in MANETs”, ACM
MobiHoc 2004
17. P.-J. Wan, K. M. Alzoubi and O. Frieder, “Distributed construction of connected
dominating set in wireless ad hoc networks”, IEEE Infocom 2002
18. Ravi Sandhu, David Ferraiolo, and Richard Kuhn. The NIST model for role-based access
control: towards a unified standard. In Proceedings of the Fifth ACM Workshop on Role-
Based Access Control (RBAC’00), pages 47–63, 2000.
19. Damianou, N., N. Dulay, E. Lupu and M. Sloman . Managing Security in Object-based
Distributed Systems using Ponder. In Proceedings of the 6th Open European Summer
School (Eunice 2000), Enchede, The Netherlands, 13-15 September 2000
109

110
