
Caregivers’ Perspectives on Ambient Assisted Living Technologies in
Professional Care Contexts
Julia van Heek, Martina Ziefle and Simon Himmel
Human-Computer Interaction Center, RWTH Aachen, Campus-Boulevard 57, 52064 Aachen, Germany
Keywords: Ambient Assisted Living Technologies, Technology Acceptance, Professional Caregivers, Data Gathering
and Storage, User Diversity.
Abstract: An increasing proportion of older people in need of care presents one of the major challenges within demo-
graphic change. The development of Ambient Assisted Living (AAL) technologies is one option to face the
challenges of rising care needs. Beyond technical and economic aspects, the acceptance of diverse stake-
holders plays a major role for a successful implementation and rollout of those technologies. In particular, it
is questionable whether and to which extent the use of assisting technologies is accepted in professional care
contexts, in particular with respect to gathering and storage of data. Thus, the current study aimed for an in-
vestigation of professional caregivers’ perspectives on the acceptance of AAL technologies in professional
care contexts. In a scenario-based online questionnaire, n = 287 professional caregivers evaluated perceived
benefits, barriers, and acceptance of AAL technologies. Also, they indicated which data can be gathered and
which specific technologies should be used to gather data. Further, data access and data storage were also
under study. The results showed a reserved and critical attitude of professional caregivers towards using
AAL technologies in their everyday working life and allow to analyze trade-offs between permitted gath-
ered data and specific requested technologies in depth.
1 INTRODUCTION
Demographic change entails the development of
more and more older people and people in need of
care representing enormous challenges for today’s
society and especially high burdens for the care
sector (Pickard, 2015; Walker & Maltby, 2012;
Bloom & Canning, 2004). In particular, geriatric and
nursing care institutions suffer badly from a lack of
specialists in combination with higher proportions of
old and diseased people who have to be cared
(Siewert et al., 2010; Shaw et al., 2010; Wild et al.,
2004; Roger et al., 2011). At the same time, there is
a first generation of “old disabled” people due to
medical and technical developments in healthcare
and otherwise also due to the specific historical
background of euthanasia offenses (in particular in
Europe), in which disabled people were systemati-
cally deported or even murdered (Poore, 2007).
Thus, similar to the challenges for geriatric and
nursing care, the sector of care and support of disa-
bled people is also confronted with higher propor-
tions of people in need of care and a simultaneous
lack of care staff (WHO, 2012).
Summarizing, all these care areas face essentially
the same challenges and questions arise how those
challenges can be addressed. Technical innovations
and ideas are increasingly developed in order to
relieve care staff, to enable a longer opportunity to
stay at home for older people, or to enhance safety in
emergencies. Among those technical innovations
and ideas, technical single-case solutions as well as
more complex ambient assisted living systems
(AAL) (Memon et al., 2014; Frank & Labonnote,
2015) exist that detect falls and emergencies, moni-
tor vital parameters, or enable living longer at home
using smart home technology elements (Cheng et al.,
2013; Baig & Gholamhosseini, 2013; Kleinberger et
al., 2007; Rashidi & Mihailidis, 2013).
Besides technical functionality and possibilities,
current research reveals that those systems are rarely
used in real life and especially in professional envi-
ronments (Wichert et al., 2012). The users’ ac-
ceptance is decisive for a sustainable implementa-
tion and usage of innovative technologies and sys-
tems. Hence, diverse stakeholders of AAL technolo-
gies should be addressed and their perceptions, opin-
ions, and ideas should be investigated. Previous
van Heek, J., Ziefle, M. and Himmel, S.
Caregivers’ Perspectives on Ambient Assisted Living Technologies in Professional Care Contexts.
DOI: 10.5220/0006691400370048
In Proceedings of the 4th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2018), pages 37-48
ISBN: 978-989-758-299-8
Copyright
c
2019 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
37

studies indicate differences in AAL acceptance be-
tween disabled people or people in need of care and
the perspective of professional caregivers. Addition-
ally, the caregivers’ acceptance of assistive technol-
ogies is a prerequisite for a successful implementa-
tion of AAL technologies in professional care con-
texts. Therefore, the current study especially focuses
on professional caregivers’ perspectives on specific
AAL technologies, on gathering of data, data access,
storage duration as well as perceived benefits and
barriers. Based on this investigation, it is possible to
integrate the caregivers’ professional perspective
into the design of AAL technologies. This way,
specific technologies can be adapted to the needs
and wishes of professional caregivers and the usage
of AAL technologies in professional care contexts
could potentially be increased.
2 ACCEPTANCE OF AAL
TECHNOLOGIES IN CARE
This section presents the theoretical background of
the current study starting with a short overview of
current AAL technologies and systems. Afterwards,
prestigious and well-known acceptance models as
well as results previous acceptance studies in the
context of AAL technologies for usage in profes-
sional care contexts are introduced.
2.1 Ambient Assisted Living
The term Ambient Assisted Living (AAL) summa-
rizes assisting technologies or systems that contrib-
ute to maintenance of autonomy in everyday life and
are especially applied in care for prevention and
rehabilitation (Kleinberger et al., 2007; Georgieff,
2008). Those technologies cover a broad range of
applications reaching from monitoring and detection
to reminders and smart home functionalities. Here, a
short overview of prototypical examples is given.
In the context of (outdoor) tracking and detection
of positions, Radio Frequency Identification (RFID)
tags are frequently used (Dohr et al., 2010). Further,
different types of monitoring are made possible by
integrating common Information and Communica-
tion Technologies (ICT) (e.g., microphones, move-
ment sensors, or (infra-red) cameras) into people’s
living environments. In particular, it is aimed for
enhancing safety by detection falls and emergencies
in private home environments (Stone & Skubic,
2015) as well as in professional care contexts, e.g.,
hospitals or care institutions (Ni et al., 2012). Be-
sides those safety-relevant functions, other types of
AAL technologies aim for facilitating everyday life
by using automated technologies, e.g. memory aids
or home automation (Costa et al., 2009; Hristova et
al., 2008). Further, also supporting communication
with families, friends, and caregivers by integrating
ICT in home environments is an aim of AAL
(Kleinberger et al., 2007). A further area of AAL
technologies are wearable technologies (e.g., emer-
gency arm strap) worn on the body or integrated in
clothes that are able to communicate with intelligent
AAL systems or smart home environments (Patel et
al., 2012; Memon et al., 2014). Although numerous
systems and technologies are available on the market
(e.g., Essence, 2017; Tunstall, 2017) or focused in
current research projects (e.g., Gövercin et al.,
2016), resounding success of those systems has not
occurred so far, as they are only rarely used in real
life (Wichert et al., 2012) and especially in profes-
sional care contexts (Isern et al., 2010).
On this basis, the question arises for what rea-
sons those existing, assisting, and facilitating tech-
nologies are not widely used in professional
healthcare contexts although they have the potential
to facilitate the professional everyday life? Future
users’ acceptance as well as their perception of us-
age benefits and especially barriers are decisive for a
successful integration of AAL systems in everyday
life. To understand the barriers of AAL usage in
professional contexts, we therefore focused on pro-
fessional caregivers as potential users of these sys-
tems, their perceptions, ideas, wishes, and willing-
ness to adopt home-integrated ICT in this study.
2.2 User-specific Acceptance of AAL
Previous research results revealed that AAL tech-
nologies were mostly evaluated positively and the
necessity and usefulness of technical support were
acknowledged by diverse groups of potential users
(van Heek et al., 2017; Himmel & Ziefle, 2016;
Beringer et al., 2011; Gövercin et al., 2016). Ena-
bling an independent and more autonomous life as
well as a longer staying at the own home for older,
diseased and/or disabled people are strong drivers to
use AAL technologies. In contrast, feelings of isola-
tion (e.g., van Heek et al., 2017a; Sun et al., 2010),
feelings of surveillance, and invasion of privacy
(e.g., Wilkowska & Ziefle, 2012; Wilkowska et al.,
2015; van Heek et al., 2017b) represent the most
frequently mentioned barriers if people were asked
to think about an integration of AAL technologies in
their living environment. In more detail, numerous
focus group (e.g., Demiris et al., 2004; Ziefle et al.,
ICT4AWE 2018 - 4th International Conference on Information and Communication Technologies for Ageing Well and e-Health
38

2011) and interview studies (e.g., Beringer et al.,
2011) with people aged above 60 were conducted in
order to examine the elderly’s perceptions of AAL
technologies: Similar to the mentioned general posi-
tive perception, the older participants acknowledged
the benefits of staying at home longer, understood
the problematic lack of care staff as well as the
chances and potential of AAL technologies. On the
other side, they expressed fears concerning a de-
pendency on technologies they are not able to con-
trol, a lack of personal contact referring to the con-
cern that care staff will might be substituted by tech-
nologies, and privacy concerns. These mostly quali-
tative gained results have been confirmed by numer-
ous quantitative surveys over the last years (e.g.,
Himmel & Ziefle, 2016).
The perspectives of professional care givers on
integrating AAL technologies in professional care
contexts have rarely been considered in acceptance
research so far, although their perspectives are man-
datory in order to do justice to needs of care and care
itself in professional care contexts. Single studies
focused on caregivers as potential users and on their
perceived concerns regarding in-home monitoring
technologies (Larizza et al., 2014). Other studies
concentrated on requirements and perception of
AAL technology usage as well as the effectiveness
of different technologies, and deriving of guidelines
for design and implementation in the context of
professional care environments (López et al., 2015;
Mortenson et al., 2013).
Although those previous results showed a gen-
eral positive attitude towards AAL technologies,
another comparative study revealed a more critical
and restraint attitude of professional caregivers to-
wards AAL technologies compared to disabled par-
ticipants, relatives of disabled persons, and “not”-
experienced (in terms of professional expertise or in
terms of personal affliction) participants (van Heek
et al., 2017a). This might serve as a starting point
and explanation why AAL technologies are not
widely used in professional care contexts. Hence, it
is of great importance to investigate the perceptions,
wishes, and needs of this specific user group in
depth. To understand the emerging negative attitude
of professional caregivers and the trade-off between
acknowledged benefits and existing perceived barri-
ers, it is necessary to investigate the acceptance of
AAL technologies with a specific and detailed focus
on these users and their usage environments.
For investigating the acceptance of assisting ICT,
well-known and widely spread acceptance models
such as TAM, UTAUT, and their adapted versions
were urgently used in the past years. Against the
background of increasing usage requirements in the
context of care, the existing models of technology
acceptance are not sufficient among others due to
the sensible usage context of care, the models’ view
of acceptance as static technology assessment, and
leaving apart user factors as well as trade-offs be-
tween simultaneously existing benefits and barriers
(Ziefle & Jakobs, 2010).
Therefore, we used interviews specifically tai-
lored to professional caregivers in a first step in
order to identify challenges in care and focus on
perceived benefits as well as perceived barriers of
AAL technology usage. Further, we aimed for an
identification of what technology is exactly allowed
to do and not to do by professional caregivers. On
this basis, we conceptualized an online questionnaire
tailored to professional caregivers needs and wishes
and ensured that all relevant aspects (for this specific
user group) can be quantified.
3 METHOD
In this section, the research design is presented start-
ing with the research questions and aims of the cur-
rent study. Afterwards, the empirical design of the
quantitative study and the sample’s characteristics
are detailed. Our study aimed for an investigation of
professional caregivers’ acceptance of AAL tech-
nologies in professional care contexts including the
following research questions:
1. How do professional caregivers evaluate AAL
technologies and potential benefits as well as
barriers? (RQ 1)
2. Which data can be gathered, which technologies
can be used to gather data, and how is data ac-
cess and storage duration evaluated? (RQ 2)
3. Do user diversity characteristics impact the
acceptance and AAL technology evaluation di-
mensions (benefits, barriers, technologies, data,
data access, storage duration)? (RQ 3)
3.1 Empirical Design
The questionnaire items were developed based on
the findings of previous interview studies. The first
part of the questionnaire addressed demographic
characteristics such as age, gender, education, dura-
tion of professional experience, and care sector (i.e.
geriatric care, nursing care, care/support of disabled
people). In the next part, the participants were asked
to evaluate their technical self-efficacy (using four
items,
= .884; Beier, 1999), their needs for privacy
(using six items,
= .833; Xu et al., 2008; Morton,
Caregivers’ Perspectives on Ambient Assisted Living Technologies in Professional Care Contexts
39

2013), and their interpersonal trust (using three
items,
= .793; McKnight et al., 2002).
For ensuring that all participants pertain to the
same baseline referred to the evaluation of AAL
technology, a scenario was designed as a very per-
sonal everyday working situation wherein the partic-
ipants should imagine that an AAL system was inte-
grated in their professional working environment. As
technologies of the system, room sensors, ultrasonic
sensors, microphones, and video cameras were in-
troduced and their range of functions and possibili-
ties within the AAL system were explained (e.g.,
alarms (emergencies, falls), automatic opening and
closing of doors and windows, reminders, etc.).
Afterwards, the participants were asked to evalu-
ated potential benefits of the described AAL sys-
tem’s usage within their professional working envi-
ronment (using 14 items,
= .923; based on previ-
ous interview studies’ results). Further, the partici-
pants also assessed potential barriers (using 17
items;
= .861; also based on previous interview
studies’ results). In a next part, the participants
should indicate whether they agreed with gathering
different types of data (using 14 items (data types),
= .856; based on necessary information to realize
technical functions).
Then, the participants were asked to evaluate dif-
ferent technologies to gather data (using 12 items,
= .892; based on technical configurations of AAL
systems). To evaluate the acceptance of the AAL
system, the participants evaluated six different
statements (
= .932; e.g., “I find the described AAL
system useful”). All described items had to be eval-
uated on six-point Likert scales (1 = min: ”I strongly
disagree”; 6 = max: “I strongly agree”) and are pre-
sented in section 4.
Finally, the participants were given opportunity
to reason their opinions on an optional basis and to
provide their feedback concerning the study. Com-
pleting the questionnaire took, on average, 20
minutes. Data was collected online in Germany.
Participants were recruited in online networks as
well as by personal and project contact to care insti-
tutions. Overall, the questionnaire was made availa-
ble for 3 months in spring and summer 2017.
3.2 Sample Description
A total of 287 participants volunteered to participate
in our questionnaire study, which was partly ac-
quired by personal and by direct contact to profes-
sional care institutions. Since only complete data
sets could be used for statistical analyses, a sample
of n=174 remained. The participants were, on aver-
age, 36.3 years old (SD = 11.2; min = 19; max = 68)
and predominantly female (74.7%) (25.3% male).
Most of the participants indicated a completed ap-
prenticeship (42.5%) as their highest educational
level. Further, each 23.0% reported to hold a univer-
sity degree and a university entrance diploma. 7.5%
indicated to hold a secondary school certificate,
while 4.0% reported other certificates.
All participants worked or have worked as pro-
fessional caregivers: 25.9% (n = 45) in geriatric
care, 21.3% (n = 37) in nursing care, and 52.9% (n =
92) in care and support of disabled people. On aver-
age, the caregivers have long-term professional
experience: 43.5% (n = 74) more than 10 years,
41.8% (n = 71) between 3 and 10 years, and only
14.7% (n = 25) have less than 3 years professional
experience.
Referring to attitudinal variables, the participants
reported to have on average a middle technical self-
efficacy (M = 3.4; SD = 0.7; min = 1; max = 6) and
also a middle interpersonal trust (M = 3.5; SD = 0.8;
min = 1; max = 6). The participants’ needs for priva-
cy and data security were on average positive (M =
4.2; SD = 0.9; min = 1; max = 6).
4 RESULTS
Prior to descriptive and inference analyses, item
analyses were calculated to ensure measurement
quality, while a Cronbach’s alpha > 0.7 indicated a
satisfying internal consistency of the scales. Data
was analyzed descriptively, by linear regression
analyses and, with respect to user diversity effects,
by correlation and linear regression analysis. The
level of significance was set at 5%.
First, the results were presented descriptively for
the perception of benefits and barriers as well as the
participants’ evaluation of different technologies,
gathered data, data access, and data storage. In a
second step, the results of a linear regression analy-
sis are presented to analyse which aspect affects the
professional caregivers’ acceptance of AAL tech-
nologies most. Afterwards, the results are analysed
regarding influences of user diversity characteristics.
4.1 General Perception of AAL
This section presents the results concerning per-
ceived benefits and barriers of AAL system usage,
desired applied technologies and data that could be
gathered as well as acceptance of different AAL
technology systems. Thereby, the results initially
ICT4AWE 2018 - 4th International Conference on Information and Communication Technologies for Ageing Well and e-Health
40
refer to the whole sample of caregivers investigating
RQ 1 and RQ 2.
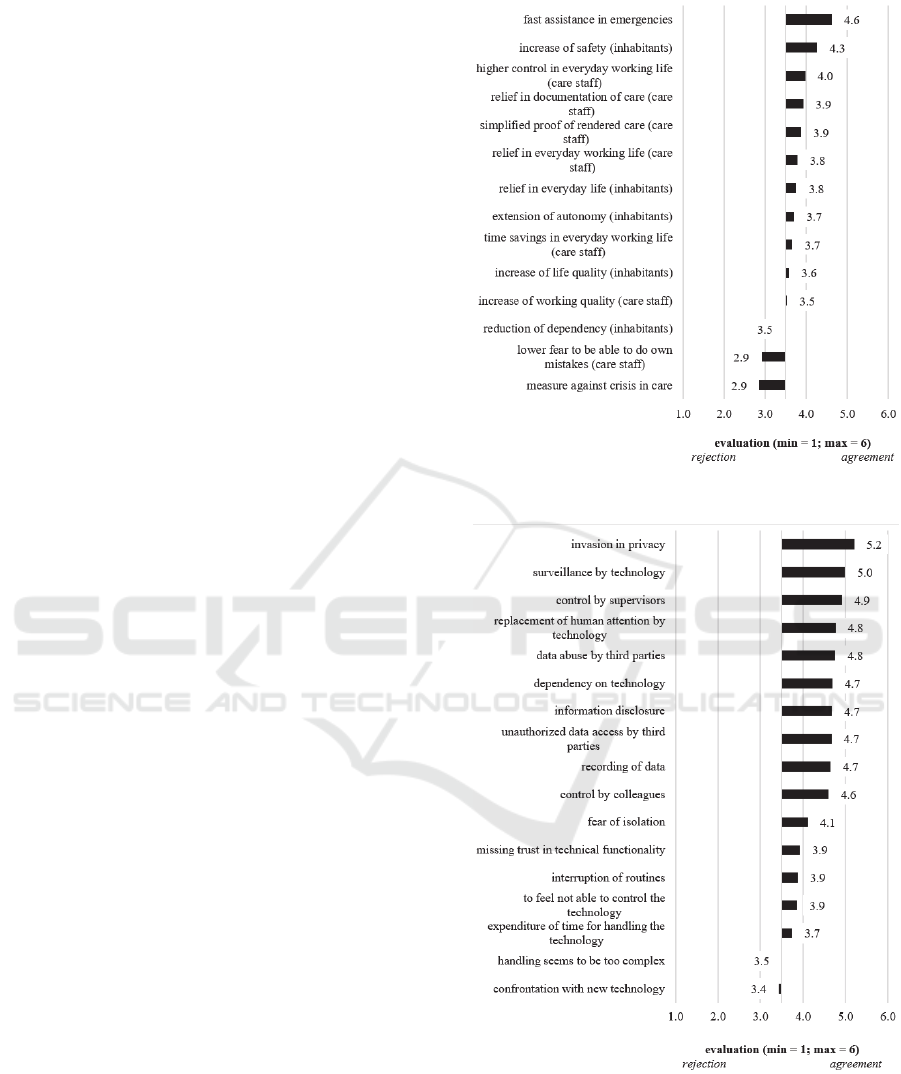
4.1.1 Perceived Benefits and Barriers (RQ 1)
Figure 1 presents the evaluation of perceived bene-
fits of an AAL system’s usage. Fast Assistance in
emergencies (M = 4.6; SD = 1.2) was perceived as
the most important benefit, followed by increase in
safety for inhabitants (M = 4.3; SD = 1.2). Potential
benefits with regard to care staff (higher control in
everyday working life (M = 4.0; SD = 1.5), relief in
documentation of care (M = 3.9; SD = 1.4), simpli-
fied proof of rendered care (M = 3.9; SD = 1.4),
relief in everyday working life (M = 3.8; SD = 1.4))
were rated only slightly positively. Other potential
benefits such as relief in everyday life (M = 3.8 SD =
1.3), extension of autonomy (M = 3.7; SD = 1.4), or
reduction of dependency (M = 3.5; SD = 1.4) for
inhabitants were also rated only slightly positive or
almost neutrally. The two rather care staff-related
aspects lower fear to be able to do own mistakes (M
= 2.9; SD = 1.5) and measure against crisis in care
(M = 2.9; SD = 1.6) were rated slightly negatively
and were thus not perceived as benefits of AAL
technologies in professional care contexts.
In contrast to the diverse evaluation of benefits
(with accepted and rejected potential benefits), none
of the potential barriers was rejected (see Figure 2).
Therefore, almost all aspects were perceived as solid
barriers of AAL technology usage in professional
care contexts. In detail, items related with privacy
and data security (e.g., invasion in privacy (M = 5.2;
SD = 1.0), data abuse by third parties (M = 4.8; SD
= 1.2), recording of data (M = 4.7; SD = 1.3)) or
with a perceived surveillance (i.e. surveillance by
technology (M = 5.0; SD = 1.1), control by supervi-
sors (M = 4.9; SD = 1.2), control by colleagues (M =
4.6; SD = 1.3)) were rated highest and represent
relevant barriers. Further, other aspects such as fear
of isolation (M = 4.1; SD = 1.4), missing trust in
technical functionality (M = 3.9; SD = 1.4), or inter-
ruption of routines (M = 3.9; SD = 1.3) were evalu-
ated slightly positively. In contrast, handling seems
to be too complex (M = 3.5; SD = 1.3) and confron-
tation with new technology (M = 3.4; SD = 1.4) were
rated neutrally and thus, those aspects were not per-
ceived as notably relevant barriers of AAL technol-
ogy usage.
4.1.2 Data and Specific Technologies (RQ 2)
Besides perceived benefits and barriers of AAL
technology usage in professional care contexts, the
participants were also asked for which data should
Figure 1: Perceived benefits of AAL technology usage.
Figure 2: Perceived barriers of AAL technology usage.
be allowed to be gathered (Figure 3) and which
specific technology should be used to gather data
(Figure 4) to answer RQ 2.
Caregivers’ Perspectives on Ambient Assisted Living Technologies in Professional Care Contexts
41

Figure 3: Evaluation of type of gathered data.
To gather data related with emergency situa-
tions (emergencies (falls epileptic seizures) (M =
5.3; SD = 0.9), actuation of emergency buttons (care
staff: M = 5.2; SD = 1.0; inhabitants: M = 5.2; SD =
1.0), and cries for help/support M = 5.2; SD = 1.0)
was clearly accepted. Data about fixations (M = 4.1;
SD = 1.6) and rooms (opening windows, doors, …)
(M = 4.0; SD = 1.6) were also allowed to be gath-
ered. Further, gathering the position of inhabitants
(M = 3.6; SD = 1.4) was evaluated neutrally, while
the position of care staff (M = 2.8; SD = 1.5) was
rather rejected. Data about sleeping (M = 3.3; SD =
1.5), care duration (M = 3.0; SD = 1.6), whole care
situations (M = 2.9; SD = 1.6), and times (rooms are
entered or left) (M = 2.9; SD = 1.5) should also not
be gathered due to rather negative values. In con-
trast, to gather data concerning a 24h observation (M
= 2.6; SD = 1.6) and regarding talks during care
(M
= 2.1; SD = 1.4) was clearly rated negatively and
was thus not accepted.
Like the diverse evaluation of the type of gath-
ered data, the specific technologies that should be
used to gather data were also assessed quite differ-
ently (Figure 4). The use of emergency buttons (in-
habitants: M = 5.1; SD = 1.1; care staff: M = 5.1; SD
= 1.2) and fall sensors into the floor (M = 4.8; SD =
1.4) were clearly accepted. Further, fall sensors in
clothes on body of inhabitants (M = 4.3; SD = 1.5)
and room sensors (M = 4.1; SD = 1.6) were rated
positively. To use motion detectors (in rooms: M =
3.4; SD = 1.6; in clothes of inhabitants: M = 3.3; SD
= 1.6) as well as ultrasonic sensors (M = 3.3; SD =
1.5) was marginally rejected. In contrast, infra-red
Figure 4: Evaluation of technologies used to gather data.
cameras (M = 2.5; SD = 1.4), motion detectors in
clothes of care staff (M = 2.5; SD = 1.5), micro-
phones (M = 2.4; SD = 1.4), and cameras (M = 2.2;
SD = 1.3) were evaluated clearly negatively. There-
fore, those technologies were not accepted as tech-
nologies to gather data in professional care contexts.
As a further aspect, the participants assessed the
storage duration and data access after data was gath-
ered (Figure 5). Here, only the most striking descrip-
tive results are reported.
Concerning data access, room data was the own
data type that received slightly positive values and
data access for all supervisors (M = 3.7; SD = 1.7),
direct supervisors (M = 3.9; SD = 1.6), and col-
leagues (M = 4.0; SD = 1.6) was at least tolerated. In
contrast, the negative evaluations showed that posi-
tion data, audio data, and video data should neither
be accessible for all supervisors, direct supervisors,
nor colleagues. Regarding storage duration, the
comparatively positive values showed that all data
types should only be allowed to be evaluated for the
moment (video: M = 3.8; SD = 1.7; audio: M = 3.8;
SD = 1.8; position: M = 4.0; SD = 1.6; room: M =
4.1; SD = 1.5). Storage on a daily basis (video: M =
2.6; SD = 1.5; audio: M = 2.6; SD = 1.6; position: M
= 2.8; SD
= 1.5) and in particular long-term storage
(video: M = 1.9; SD = 1.2; audio: M = 1.8; SD = 1.1;
position: M = 2.1; SD = 1.3) were rejected for all
data types except of room data that received only
almost neutral values for storage on a daily basis (M
= 3.7; SD = 1.7) as well as long-term storage (M =
3.4; SD = 1.8). Thus, storage was most likely toler-
ated with regard to room data.
ICT4AWE 2018 - 4th International Conference on Information and Communication Technologies for Ageing Well and e-Health
42
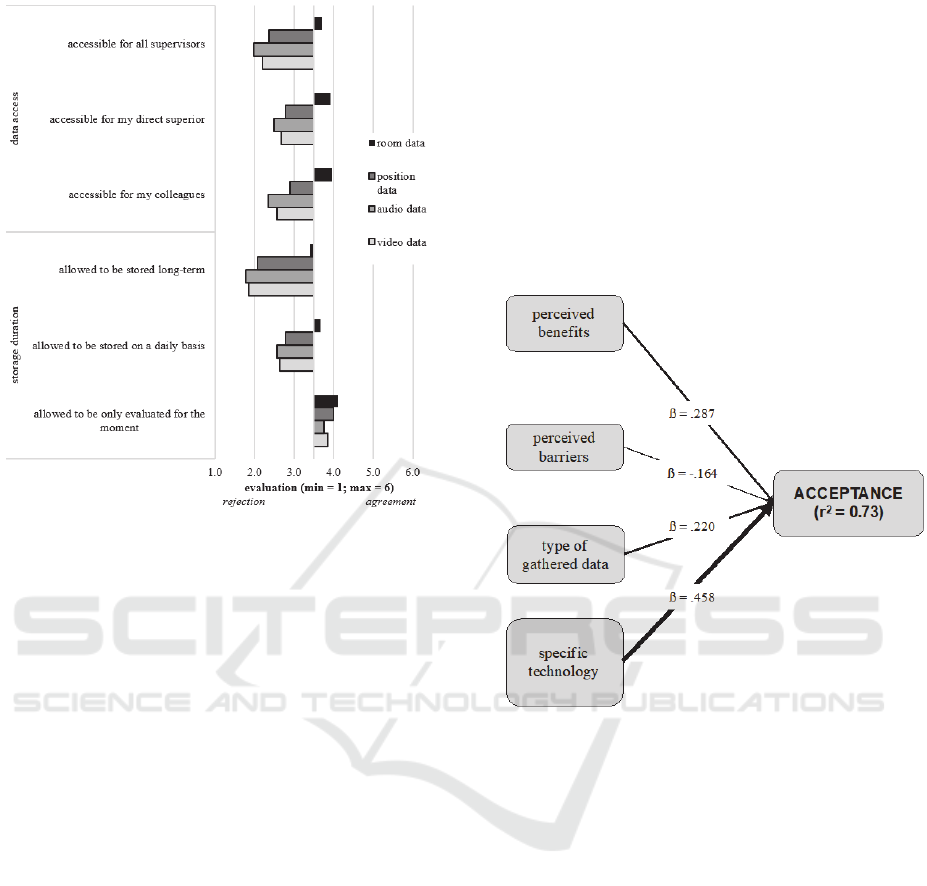
Figure 5: Evaluation of storage duration and data access
for different data types.
4.1.3 Acceptance of AAL technologies
Overall, the acceptance of the mentioned AAL tech-
nologies was evaluated rather neutrally (M = 3.6; SD
= 1.3). Comparatively, a system consisting only of
room sensors (M = 4.0; SD = 1.5) received the high-
est evaluation, while a system consisting of all men-
tioned technologies except of a camera was assessed
worst (M = 2.9; SD = 1.4).
In order to analyze, which of the descriptively
presented factors influences the acceptance of AAL
technologies most, a step-wise linear regression
analysis was conducted: here, the acceptance of
AAL technology usage was calculated as dependent
variable, while perceived benefits, perceived barri-
ers, data that is allowed to be gathered, specific type
of technology, data access, and storage duration
represented the independent variables. The calcula-
tion revealed four significant models. The first mod-
el predicted 59.1% (adj. r
2
= .591) variance of AAL
technology acceptance and was based on the specific
technology that is used to gather data. Thus, the
acceptance of AAL technology usage depends clear-
ly on the specific technologies that are used and
integrated in the system. The second model addi-
tionally contained perceived benefits and explained
+8.5% (adj. r
2
= .676) variance of AAL technology
acceptance. The third model explained +3.2% (adj.
r
2
= .708) variance and was based on the specific
technology, perceived benefits, and additionally on
the type of gathered data. The fourth and final mod-
el explained +2.2% (adj. r
2
= .730) variance of AAL
technology acceptance and contained besides per-
ceived benefits, specific technology, type of gath-
ered data, also perceived barriers. The other two
integrated dimensions data access and storage dura-
tion were not part of the regression models and did
not influence the acceptance of AAL technologies
significantly. Figure 6 illustrates the final regression
model and displays the regression coefficient
for
all independent variables.
Figure 6: Final regression model based on significantly
influencing variables.
4.2 Impact of Individual
Characteristics (RQ 3)
So far, the results referring to the whole sample of
caregivers have been presented. As user diversity
plays an important role in the acceptance of medical
and assistive technologies (see section 2.2), the re-
sults are further analyzed concerning impacts of
demographic and attitudinal characteristics of the
participants to answer RQ 3.
First, correlation analyses were conducted in or-
der to find out which demographic and attitudinal
characteristics are relevant for the acceptance of
AAL technologies (Figure 7). Starting with demo-
graphic characteristics, the results revealed only
single correlations with the dimensions of AAL
technology usage: Age was not related at all with
one of the other dimensions. Gender correlated only
slightly with perceived barriers of AAL technology
usage (
= -.156; p < .05) and women showed a
Caregivers’ Perspectives on Ambient Assisted Living Technologies in Professional Care Contexts
43
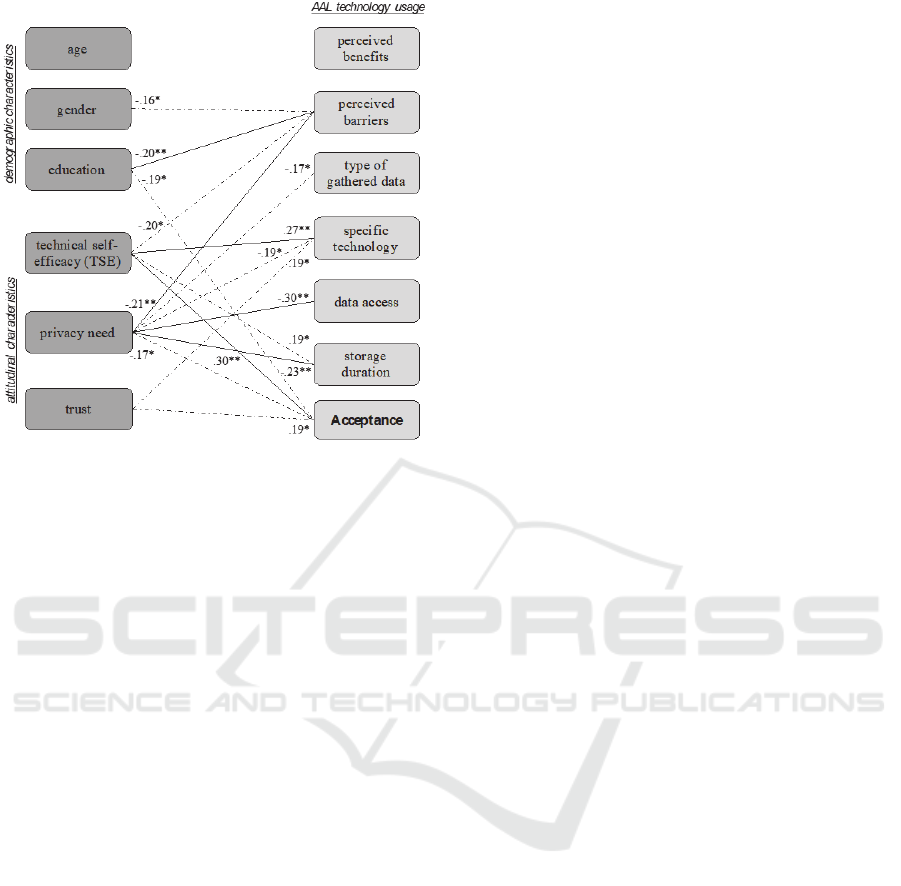
Figure 7: Results of correlation analysis: user diversity
impacts (dotted line: p<.05; solid line: p<.01).
slightly higher evaluation of perceived barriers than
men. Education was slightly related with perceived
barriers (
= -.202; p < .01) and acceptance of AAL
technologies (
= .196; p < .05). Subsequently con-
ducted multivariate variance analyses, revealed no
significant impact of the demographic characteristics
on the AAL technology usage dimensions.
Referring to attitudinal characteristics, the re-
sults revealed more striking relationships. For inter-
personal trust, there were indeed only single, slight
correlations with the evaluation of specific technol-
ogies (
= .189; p < .05) and acceptance of AAL
technologies (
= .186; p < .05). In contrast, the
results showed numerous and partly also stronger
correlations for the two attitudinal variables privacy
need and technical self-efficacy (TSE). The strongest
correlations of privacy need referred to perceived
barriers (
= .209; p < .01), data access (
= -.301; p
< .01), and storage duration (
= -.228; p < .01)
indicating that participants with higher needs for
privacy showed higher evaluations of perceived
barriers and a more negative attitude towards data
access for other people and a long-term data storage.
Concerning technical self-efficacy, the strongest
relationships referred to the evaluation of specific
technologies (
= .274; p < .01) and acceptance of
AAL technology usage (
= .299; p < .01) indicating
that participants with a higher technical self-efficacy
showed a more positive attitude towards specific
technologies and a higher acceptance of AAL tech-
nologies.
To investigate the impact of user diversity fac-
tors in depth, the attitudinal variables were also
analyzed in multivariate variance analyses. For trust,
the results revealed no significant impact on the
AAL technology usage dimensions. Concerning two
groups with different privacy needs, the analysis
confirmed that data access (F(1,158)=7.076; p < .01)
and storage duration (F(1,158)=6.359; p < .05) are
considered as significantly more critical by people
with high privacy needs (M
access
= 2.7, SD
access
= 0.9;
M
storage
= 2.9, SD
storage
= 0.9) compared to people with
lower privacy needs (M
access
= 3.2, SD
access
= 1.1;
M
storage
= 3.3; SD
storage
= 0.7).
Likewise, two groups with a different technical
self-efficacy (TSE) differed significantly regarding
perceived barriers (F(3,149)=7.708; p < .01), the
evaluation of specific technologies (F(1,149)=6.051;
p < .05), and acceptance of AAL technologies
(F(1,149)=6.564; p < .01). The results revealed that
people with a higher TSE (M = 4.1; SD = 0.7) evalu-
ated perceived barriers significantly lower than peo-
ple with a lower TSE (M = 4.5; SD = 0.7). Further,
the results confirmed that people with a higher TSE
(M
tech
= 3.8, SD
tech
= 1.1; M
accept
= 4.0; SD
accept
= 1.3)
had a more positive attitude towards the specific
technologies and showed also a higher acceptance of
AAL technologies than people with a lower TSE
(M
tech
= 3.4, SD
tech
= 0.9; M
accept
= 3.4; SD
accept
= 1.2).
These results show that user groups with different
needs for privacy and a different technical self-
efficacy differed with regard to the evaluation of
AAL technology usage dimensions. Thus, it was
important to find out, whether different dimensions
influence the acceptance of AAL technologies for
the TSE and privacy need groups.
For this purpose, we again conducted regression
analyses separately for the diverse groups. Here,
only the final regression models are reported (Table
1 & 2). Starting with privacy needs (Table 1), the
final model for participants with low privacy needs
explained 61.4% variance of AAL acceptance based
on the evaluation of specific technologies and per-
ceived benefits of AAL technology usage. In con-
trast, the final regression model for participants with
high needs for privacy explained 76.6% of the vari-
ance of AAL technology acceptance based on the
four dimensions: specific technologies, perceived
benefits, type of data, and perceived barriers.
A similar pattern occurred for the two technical
self-efficacy (TSE) groups (Table 2). Here, the re-
gression model for people with a high TSE ex-
plained 73.4% variance of AAL acceptance based on
the dimensions technology and perceived benefits.
ICT4AWE 2018 - 4th International Conference on Information and Communication Technologies for Ageing Well and e-Health
44

Table 1: Final regression model for participants with low
and high needs for privacy.
Privacy Dimension B SE B T
high needs technologies .640 .104 .458 6.145
benefits .319 .079 .236 4.019
type of data .448 .112 .282 4.013
barriers
-.279 .099 -.155 -2.836
low needs technology .603 .145 .504 4.148
benefits .364 .089 .269 3.988
However, the regression model for the low TSE
group explained 70.6% variance of AAL technology
acceptance and - similar to the high needs for priva-
cy group – based on the four dimensions: specific
technologies, perceived barriers, type of data, and
perceived benefits.
Table 2: Final regression model for participants with a low
and a high technical self-efficacy (TSE).
TSE Dimension B SE B T
low technologies .716 .131 .490 5.470
barriers -.333 .125 -.179 -2.660
type of data .389 .126 .247 3.087
benefits .251 .101 .197 2.494
high technology .780 .094 .651 8.274
benefits .606 .112 .425 5.400
5 DISCUSSION
This study revealed insights into caregivers’ per-
spectives on the acceptance of specific AAL tech-
nologies in professional care environments. As pro-
fessional caregivers play a decisive role for the ac-
ceptance of AAL technologies in professional care
contexts, we aimed for a detailed analysis of the
needs and wishes of this specific stakeholder group.
The results provide valuable insights into ac-
ceptance-decisive factors of AAL technologies in
professional care contexts and should be taken into
account for the development, design, and configura-
tion of AAL technologies.
5.1 AAL System Acceptance (RQ 1&2)
The caregivers’ evaluations of AAL technology
acceptance, perceived benefits, and barriers (see RQ
1) differ clearly from previous research results con-
cerning AAL technology acceptance. In contrast to a
general positive evaluation of AAL technologies
found in numerous past studies (e.g., Beringer et al.,
2011; Gövercin et al., 2016), this study’s profession-
al caregivers uncover a very restrained attitude to-
wards AAL technologies and show neutral ac-
ceptance evaluations, if at all. As implied in a pre-
ceding study (van Heek et al., 2017a), the present
study confirms that professional caregivers are much
more critical with regard to the integration of AAL
technologies in their (professional) everyday life
than other stakeholders.
On the one hand, this is expressed by low agree-
ments of potential benefits. Except of a faster assis-
tance in emergencies, all benefits are evaluated only
with rather positive or rather negative i.e. primarily
neutral values. Thus, potential benefits (e.g., meas-
ure against care crisis) are not perceived as real
benefits. This may be due to the applied methodolo-
gy of the scenario-based approach: as previous stud-
ies proved that hands-on experience with AAL tech-
nologies lead to more positive perceptions of usage
motives (Wilkowska et al., 2015), it can be assumed
that professional caregivers would also evaluated
AAL technologies differently if they would have the
chance trying to use those technologies in their pro-
fessional everyday life.
On the other hand, the more negative and critical
attitude of professional caregivers is expressed by
high agreements of barriers: none potential barrier is
rejected and thus, all potential barriers are perceived
as real barriers and severe drawbacks. This pattern
contrasts clearly to previous research results show-
ing a much lower reluctance to AAL systems and a
lower confirmation to the perceived barriers. (e.g.,
van Heek et al., 2017a,b). Within the perceived
barriers especially the aspects of a potential invasion
of privacy, data security concerns, and a feeling of
surveillance are of importance for professional care-
givers. It is a noteworthy finding that the nature of
the seen barriers in the professional caregivers’ per-
spective center around their own professional per-
son. The most severe concern is not to be tracked or
controlled. The patients, the caretakers, for which
caregivers are responsible and which could seriously
profit from AAL Systems are not taken into account.
Further, the study revealed detailed novel in-
sights into the perceptions of professional caregivers
respecting their perspective which data should be
allowed to be gathered and which technology should
be used to gather data, if at all (RQ 2). The results
show clearly that only emergency-related data is
allowed to be gathered. All other data types are
rejected or only just tolerated. This contrasts signifi-
cantly to the functions caregivers want AAL tech-
nologies to undertake (as reported in open comment
fields and interviews), for which gathering different
data types is factually necessary. The evaluation of
technologies that should be used for data collection,
shows similar results: the professional caregivers
only indicate to accept technologies that are partly
already existing (e.g., emergency buttons) or gather
only static, binary data (e.g., room sensors). More
Caregivers’ Perspectives on Ambient Assisted Living Technologies in Professional Care Contexts
45

complex technologies with a potential higher priva-
cy invasion (e.g., cameras, microphones) are reject-
ed. This is in line with previous research results
(e.g., Himmel et al., 2016) and illustrates the opposi-
tion between the desired technical functionality (that
could support them in caring) and the admitted data
and technology configurations. The evaluation of
data storage and data access confirms the negative
attitude and evaluation of perceived barriers, be-
cause nearly nobody is really allowed to access
gathered data and data should only be processed -
not stored.
As data is not needed to be stored long-term for
most of the functions AAL technologies could un-
dertake, targeted communication strategies focusing
on handling of data (e.g., only processing, not stor-
age) could may help to dismantle perceived barriers
and especially caveats concerning privacy and data
security.
5.2 Diversity of Users Matters (RQ 3)
The integration of user diversity factors into the
analysis of AAL technology acceptance shows that
demographic characteristics of the professional
caregivers are not decisive and did not influence the
caregivers’ acceptance of AAL technologies (see RQ
3). In contrast, the results illustrate that attitudinal
characteristics are more relevant and influence the
perception of AAL technologies.
Technical self-efficacy as well as the caregivers’
need for privacy impact the acceptance and percep-
tions of AAL technologies significantly. Similar to
previous studies (e.g., Ziefle & Schaar, 2010), peo-
ple with a higher technical self-efficacy show a
higher acceptance of AAL technologies which is
influenced by the type of technology and perceived
benefits. In contrast, people with a lower technical
self-efficacy are more restrained concerning the
acceptance of AAL technology. A low technical
self-efficacy affects the evaluation of the type of
technology and perceived benefits but additionally
also the type of gathered data as well as perceived
barriers. A similar pattern was revealed for persons
with different needs for privacy: people with low
needs for privacy show a considerably higher AAL
technology acceptance, influenced by type of tech-
nology and perceived benefits. And vice versa: peo-
ple with high needs for privacy indicate a lower
acceptance influenced by the evaluation of type of
technology, perceived benefits, perceived barriers,
and type of data.
Summarizing, professional caregivers’ technical
expertise and need for privacy contribute to a differ-
ent emphasis referring to the perception of barriers
and caveats (i.e. data gathering, storage, access, and
privacy). This confirms that especially the way AAL
technologies handle data should be focused in future
studies and integrated in communication referring to
AAL technologies in professional environments.
5.3 Limitations and Future Research
Our empirical approach provided valuable insights
into AAL technology acceptance of professional
caregivers in professional care contexts as it focused
on evaluations of specific benefits and barriers as
well as concrete data and technology configurations.
Nevertheless, there are some limitations concerning
the applied method and sample that should be con-
sidered in future approaches.
The present study was a first scenario-based ap-
proach focusing on professional caregivers’ ac-
ceptance of AAL technologies, their perceptions of
benefits and barriers as well as specifically on their
evaluations of technologies and data configurations.
As already mentioned, the applied methodological
approach was based on a scenario and thus, on a
fictional and not on a real AAL system, what proba-
bly influences the evaluations and may lead to an
underestimation of potential benefits and an overes-
timation of potential barriers (Wilkowska et al.,
2015). Thus, we aim for hands-on evaluations of
AAL technologies in future studies focusing on
professional caregivers and respectively usage of
AAL technologies in professional care environ-
ments.
As a first aspect referring to the sample, the
sample size as well as balance of demographic char-
acteristics was sufficient - in particular, referred to
the condition that only professional caregivers were
acquired. The higher proportion of female partici-
pants in the sample represents and fits to the higher
proportion of women working in care institutions
(Simonazzi, 2008). An interesting aspect for future
studies is the investigation of potential care sector
influences (geriatric care, nursing care, care of disa-
bled people) on the acceptance and perception of
AAL technologies in professional contexts due to
different challenges and processes in the respective
sectors. Finally, this study focused German partici-
pants and thus, it represents the perspective of pro-
fessional caregivers of one specific country with a
specific health care system. We assume that the
acceptance of AAL technologies differs with regard
to different countries, their cultures and their specif-
ic healthcare systems. Therefore, we aim for con-
ducting our approach in other countries to be able to
directly compare AAL acceptance depending on
different countries and cultures.
ICT4AWE 2018 - 4th International Conference on Information and Communication Technologies for Ageing Well and e-Health
46

ACKNOWLEDGEMENTS
The authors thank all participants for their openness
to share opinions on innovative technologies. Fur-
thermore, the authors want to thank Hannah Fahnen-
stich for research assistance. This work was funded
by the German Federal Ministry of Education and
Research project Whistle (16SV7530).
REFERENCES
Baig, M. M., Gholamhosseini, H. (2013). Smart Health
Monitoring Systems: An Overview of Design and
Modeling. J Med Syst., 37(2), 1-14.
Beier, G., 1999. Kontrollüberzeugungen im Umgang mit
Technik, [Control beliefs in dealing with technology].
Rep Psychol 9, 684–693.
Beringer, R., Sixsmith, A., Campo, M., Brown, J.,
McCloskey, R. (2011). The “acceptance” of ambient
assisted living: Developing an alternate methodology
to this limited research lens. In Proceedings of the In-
ternational Conference on Smart Homes and Health
Telematics, Toward useful services for elderly and
people with disabilities. Springer, pp. 161–167.
Bloom, D. E., & Canning, D. (2004). Global Demograph-
ic Change: Dimensions and Economic Significance
National Bureau of Economic Research. Working Pa-
per No. 10817.
Cheng, J., Chen, X., Shen, M. (2013). A Framework for
Daily Activity Monitoring and Fall Detection Based
on Surface Electromyography and Accelerometer Sig-
nals. IEEE J Biomed Health Inform, 17(1), 38–45.
Costa, R., Novais, P., Costa, Â., & Neves, J. (2009).
Memory support in ambient assisted living. Leverag-
ing Knowledge for Innovation in Collaborative Net-
works, 745-752.
Demiris, G., Rantz, M., Aud, M., Marek, K., Tyrer, H.,
Skubic, M., & Hussam, A. (2004). Older adults’ atti-
tudes towards and perceptions of “smart home” tech-
nologies: a pilot study. Med Inform Internet, 29(2),
87–94.
Dohr, A., Modre-Opsrian, R., Drobics, M., Hayn, D., &
Schreier, G. (2010). The internet of things for ambient
assisted living. In 2010 Seventh International Confer-
ence on Information Technology: New Generations
(ITNG), IEEE, 804-809.
Essence. (2017). Homepage: Smart Care - Care@ Home
Product Suite. Retrieved from http://www.essence-
grp.com/smart-care/care-at-home-pers.
Frank, S., & Labonnote, N. (2015, November). Monitoring
technologies for buildings equipped with ambient as-
sisted living: Current status and where next. In SAI In-
telligent Systems Conference (IntelliSys), IEEE, 431-
438.
Georgieff, P. (2008). Ambient assisted living.
Marktpotenziale IT-unterstützter Pflege für ein
selbstbestimmtes Altern. [Market potential of IT-
supported care for self-determined aging]. FAZIT
Forschungsbericht, 17, 9-10.
Gövercin, M., Meyer, S., Schellenbach, M., Steinhagen-
Thiessen, E., Weiss, B., Haesner, M. (2016).
SmartSenior@home: Acceptance of an integrated am-
bient assisted living system. Results of a clinical field
trial in 35 households. Inform Health Soc Care, 1–18.
Himmel, S., Ziefle, M. (2016). Smart Home Medical
Technologies: Users’ Requirements for Conditional
Acceptance. I-Com, 15(1), 39-50.
Hristova, A., Bernardos, A. M., & Casar, J. R. (2008).
Context-aware services for ambient assisted living: A
case-study. IEEE Applied Sciences on Biomedical and
Communication Technologies, pp. 1-5.
Isern, D., Sánchez, D., & Moreno, A. (2010). Agents
applied in health care: A review.
Int J Med Inform,
79(3), 145-166.
Kleinberger, T., Becker, M., Ras, E., Holzinger, A.,
Müller, P. (2007). Ambient Intelligence in Assisted
Living: Enable Elderly People to Handle Future Inter-
faces. In Universal Access in Human-Computer Inter-
action. Ambient Interaction, Springer Berlin Heidel-
berg, pp. 103–112.
Larizza, M. F., Zukerman, I., Bohnert, F., Busija, L.,
Bentley, S. A., Russell, R. A., Rees, G. (2014). In-
home monitoring of older adults with vision impair-
ment: exploring patients’, caregivers’ and profession-
als’ views. J American Medical Informatics Associa-
tion, 21(1), 56–63.
López, S. A., Corno, F., Russis, L. D. (2015). Supporting
caregivers in assisted living facilities for persons with
disabilities: a user study. Universal Access in the In-
formation Society, 14(1), 133–144.
McKnight, D. H., Choudhury, V., & Kacmar, C. (2002).
Developing and validating trust measures for e-
commerce: An integrative typology. Information sys-
tems research, 13(3), 334-359.
Memon, M., Wagner, S. R., Pedersen, C. F., Beevi, F. H.
A., & Hansen, F. O. (2014). Ambient assisted living
healthcare frameworks, platforms, standards, and qual-
ity attributes. Sensors, 14(3), 4312-4341.
Mortenson, W. B., Demers, L., Fuhrer, M. J., Jutai, J. W.,
Lenker, J., DeRuyter, F. (2013). Effects of an assistive
technology intervention on older adults with disabili-
ties and their informal caregivers: an exploratory ran-
domized controlled trial. American J of Physical Med-
icine & Rehabilitation/Assoc of Academic Physiatrists,
92(4), 297–306.
Ni, B., Nguyen, C. D., & Moulin, P. (2012, March).
RGBD-camera based get-up event detection for hospi-
tal fall prevention. In International Conference on
Acoustics, Speech and Signal Processing (ICASSP),
IEEE, 1405-1408.
Pickard, L. (2015). A growing care gap? The supply of
unpaid care for older people by their adult children in
England to 2032. Ageing & Society, 35(1), 96-123.
Patel, S., Park, H., Bonato, P., Chan, L., & Rodgers, M.
(2012). A review of wearable sensors and systems
with application in rehabilitation. Journal of neuroen-
gineering and rehabilitation, 9(1), 21.
Caregivers’ Perspectives on Ambient Assisted Living Technologies in Professional Care Contexts
47

Poore, C. (2007). Disability in Twentieth-century German
Culture. University of Michigan Press.
Rashidi, P., Mihailidis, A. (2013). A Survey on Ambient-
Assisted Living Tools for Older Adults. IEEE J Bio-
med Health Inform, 17(3), 579–590.
Roger, V. L., Go, A. S., Lloyd-Jones, D. M., Adams, R. J.,
Berry, J. D., Brown, T. M., et al. (2011). American
Heart Association Statistics Committee and Stroke
Statistics Subcommittee. Heart disease and stroke sta-
tistics--2011 update: a report from the American Heart
Association. Circulation, 123(4), e18–e209.
Ruyter, B. de, & Pelgrim, E. (2007). Ambient Assisted-
living Research in Carelab. Interactions, 14(4), 30–33.
Shaw, J. E., Sicree, R. A. Zimmet, P. Z. (2010). Global
estimates of the prevalence of diabetes for 2010 and
2030. Diabetes Res Clin Pract, 87(1), 4–14.
Siewert, U., Fendrich, K., Doblhammer-Reiter, G., Scholz,
R. D., Schuff-Werner, P., & Hoffmann, W. (2010).
Health care consequences of demographic changes in
Mecklenburg–West Pomerania: projected case num-
bers for age-related diseases up to the year 2020, based
on the study of health in Pomerania (SHIP). Deutsches
Ärzteblatt International, 107(18), 328.
Simonazzi, A. (2008). Care regimes and national employ-
ment models. Cambridge Journal of Economics,
33(2), 211-232.
Stone, E. E., Skubic, M. (2015). Fall detection in homes of
older adults using the Microsoft Kinect. IEEE journal
of biomedical and health informatics, 19(1), 290-301
Sun, H., De Florio, V., Gui, N., Blondia, C. (2010). The
missing ones: Key ingredients towards effective ambi-
ent assisted living systems. J Ambient Intell Smart En-
viron, 2(2), 109–120.
Tunstall (2017). Homepage: Tunstall - Solutions for
Healthcare Professionals. Retrieved from
www.tunstall healthcare.com.au.
van Heek, J., Himmel, S., Ziefle, M. (2017a). Helpful but
Spooky? Acceptance of AAL-Systems Contrasting
User Groups with focus on Disabilities and Care
Needs'. Proceedings of the International Conference
on ICT for Aging well (ICT4AWE 2017),
SCITEPRESS – Science and Technology Publications,
78-90.
van Heek, J., Himmel, S., Ziefle, M. (2017b). Privacy,
Data Security, and the Acceptance of AAL-Systems –
a User-Specific Perspective. In: Zhou J., Salvendy G.
(eds) Human Aspects of IT for the Aged Population.
Aging, Design and User Experience. ITAP 2017. Lec-
ture Notes in Computer Science, vol 10297. Springer,
Cham, 38-56.
Walker, A., Maltby, T. (2012). Active ageing: A strategic
policy solution to demographic ageing in the European
Union. Int J Social Welfare, 21, 117–130.
Wichert, R., Furfari, F., Kung, A., & Tazari, M. R. (2012).
How to overcome the market entrance barrier and
achieve the market breakthrough in AAL. In Ambient
assisted living. Springer Berlin Heidelberg, pp. 349-
358.
Wild, S., Roglic, G., Green, A., Sicree, R., King, H.
(2004). Global prevalence of diabetes: estimates for
the year 2000 and projections for 2030. Diabetes
Care, 27(5), 1047–1053.
Wilkowska, W. & Ziefle, M. (2012). Privacy and Data
Security in E-health: Requirements from Users’ Per-
spective. Health Informatics Journal, 18(3) 191–201.
Wilkowska, W., Ziefle, M., & Himmel, S. (2015). Percep-
tions of Personal Privacy in Smart Home Technolo-
gies: Do User Assessments Vary Depending on the
Research Method? In Int Conference on Human As-
pects of Information Security, Privacy, Trust, Spring-
er, pp. 592–603.
World Health Organization (WHO) (2012). World Health
Day 2012: ageing and health: toolkit for event organ-
izers. Available online: http://apps.who.int/iris/bitstr
eam/10665/70840/1/WHO_DCO_WHD_2012.1_eng.
pdf
Xu, H., Dinev, T., Smith, H. J., & Hart, P. (2008). Exam-
ining the formation of individual's privacy concerns:
Toward an integrative view. ICIS 2008 proceedings, 6.
Ziefle, M., Himmel, S., Wilkowska, W. (2011). When
Your Living Space Knows What You Do: Acceptance
of Medical Home Monitoring by Different Technolo-
gies. In Information Quality in e-Health, Springer
Berlin Heidelberg, pp. 607–624.
Ziefle, M., & Jakobs, E. M. (2010). New challenges in
human computer interaction: Strategic directions and
interdisciplinary trends. Proceedings of the 4th Inter-
national Conference on Competitive Manufacturing
Technologies, COMA, 389-398.
Ziefle, M. & Schaar, A.K. (2010). Technical Expertise and
its Influence on the Acceptance of Future Medical
Technologies. What is influencing what to which ex-
tent? In G. Leitner, M. Hitz & Andreas Holzinger
(eds). HCI in Work & Learning, Life & Leisure, Lec-
ture Notes in Computer Science, 6389, Berlin, Heidel-
berg: Springer, pp. 82-100.
ICT4AWE 2018 - 4th International Conference on Information and Communication Technologies for Ageing Well and e-Health
48
