
Pedobarographic Profile of Gait in Patients
with Ankylosing Spondylitis
Igor Gruić
1
, Frane Grubišić
2
, Simeon Grazio
2
and Vladimir Medved
1
1
Faculty of Kinesiology, University of Zagreb, Horvaćanski zavoj 15, 10 000 Zagreb, Croatia
2
Department of Rheumatology, Physical Medicine and Rehabilitation, University Hospital Centre Sisters of Mercy,
Vinogradska 29, 10 000 Zagreb, Croatia
Keywords: Ankylosing Spondylitis, Pedobarography, Forward Stepwise Regression Analyses.
Abstract: Ankylosing spondylitis (AS) is chronic inflammatory rheumatic disease which predominantly affects
sacroiliac joints and spine and, during course of time, may also alter posture, movement patterns and
regulation and quality of life. Clinical diagnostic tools for assessment of AS internalizations complement
different qualitative and quantitative methods. Externalisations of axial skeleton alterations, followed by hip,
knee, ankle and foot joints posture and movement adjustments, are quantified by conservative biomechanical
approach. Items representing functional status and disease activity in AS patients correlated to
pedobarographic status were anchored to previous research, i.e. Doward et al, 2003, Grazio et al, 2009, Aydina
et al., 2015, Giacomozzi, 2010, Gruic et al, 2015, Gruic et al, 2016. Contrary to previous findings, multiple
correlation between clinical scores and dynamic pedobarographic measurements was established.
1 INTRODUCTION AND
OBJECTIVES
Ankylosing spondylitis (AS) is chronic inflammatory
rheumatic disease which predominantly affects
sacroiliac joints and spine and, during course of time,
may also alter posture, movement patterns and
regulation and quality of life. Clinical diagnostic tools
for assessment of AS internalizations complement
different qualitative and quantitative methods.
Externalisations of axial skeleton alterations,
followed by hip, knee, ankle and foot joints posture
and movement adjustments, are quantified by
conservative biomechanical approach.
Grazio et al., 2009, determined the reliability and
validity of Croatian version of the Bath Ankylosing
Spondylitis Functional Index (BASFI) and Bath
Ankylosing Spondylitis Disease Activity Index
(BASDAI) in patients with ankylosing spondylitis.
Findings were affirmative, therefore appropriate for
clinical trials, research and practice. In Aydina et al.,
2015, plantar pressure distribution in patients with
ankylosing spondylitis was measured. Findings
revealed that no clinically significant correlation
between clinical scores and static pedobarographic
measurements have been found. Gruic et al., 2015,
measured pedobarographic features of gait (by
FDM1.5 PMD), and Gruić et al., 2016, compared
pedobarographic profiles in young males with left and
right scoliotic posture. Main objective was to
determine feasibility and clinical standards for
pedobarographic assessment of gait features. It was in
line with conclusions of Giacomozzi (2010) that
“PMD measurements are increasingly used – alone or
in conjunction with other kinetic/kinematic
parameters – to deeply investigate clinical outcomes
of surgical interventions, rehabilitation treatments,
preventive actions, disease evolution, as well as to
implement new biomechanical models or validate
novel methodological approaches”.
Main objective of this research was to determine
both contribution and influence of pedobarographic
features of gait in results of clinical diagnostics
procedures quantifying status and development of
ankylosing spondylitis, i.e. to test appropriateness of
usage of pedobarographic measure protocol as an
extension of regular AS diagnostic tests/tools.
GruiÄ
˘
G I., GrubiÅ ˛aiÄ
˘
G F., Grazio S. and Medved V.
Pedobarographic Profile of Gait in Patients with Ankylosing Spondylitis.
DOI: 10.5220/0006516001210125
In Proceedings of the 5th International Congress on Spor t Sciences Research and Technology Support (icSPORTS 2017), pages 121-125
ISBN: 978-989-758-269-1
Copyright
c
2017 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

2 METHODS
Sample consists of 10 male patients diagnosed with
AS, age range between 18 and 65 years, regularly
participating in rehabilitation program. Exclusion
criteria were: lower extremity injuries (e.g. ankle
distortion, knee trauma, etc.), postoperative
procedures within 6 months (e.g. anterior cruciate
ligament surgery, hip surgery, etc.), neurological
diseases (e.g. neuropathy, cerebral palsy, etc.),
vascular diseases (e.g. intermittent claudication),
metabolic diseases (e.g. diabetic foot, obesity).
Sample of variables was comprised of three
criterion variables assessing AS – BASMI, BASFI
(Grazio et al, 2009) and ASQoL (a quality of life
instrument specific to ankylosing spondylitis -
Doward et al, 2003), and standard set of 63
quantitative variables and graphics assessing
pedobarographic features of gait within protocol
standardized for descriptive and inferential statistical
methods (Gruić et al, 2015). Normality of
distributions of results was tested with K-S test.
Contributions of pedobarographic variables to results
in dependent variables were tested by simple
correlation and forward stepwise regression analysis.
3 RESULTS
Different pedobarographic variables have different
power to explain AS status due to different
measurement protocols, measuring devices and
univariate and multivariate statistical tools used in
analysis.
Descriptive statistics of subjects’ basic
morphology, AS and pedobarographic status, is
presented in Table 1., along with regression analyses
summary and partial contributions within forward
stepwise regression analysis of contributions of
pedobarographic variables to results in dependent
variables: BASFI, BASDAI and ASQoL.
Simple relation trough inferential statistics reveal
that results in BASFI were found to be in positive
correlation with results in time to achieve maximal
force with right heel (FTMF1R: r=0,69; p=0,03), time
to change load from left heel to forefoot (LTPL:
r=0,76; p=0,01), maximum force in left midfoot
(MML: r=0,68; p=0,03), absolute difference in
average time in the gait cycle, at which the maximum
forces were measured for left and right forefoot zones
(TMAXF_D: r=0,69; p=0,03), in the average time in
the gait cycle, at which the maximum force was
measured for left midfoot zone (TMAXML: r=0,66;
p=0,04), and contact time for left heel (CHL: r=0,76;
p=0,01), and in negative correlation with results in
left leg step length (GSLL: r=-0,78; p=0,01), right leg
step length (GSLR: r=-0,77; p=0,01), and stride
length (GSL: r=-0,80; p=0,01). Results in BASDAI
were found not to be in simple correlation with results
in pedobarographical variables. Results in ASQoL
were found to be in positive correlation with results
in the average time in the gait cycle, at which the
maximum force was measured for left midfoot zone
(TMAXML: r=0,64; p=0,05), in the average time in
the gait cycle, at which the maximum force was
measured for left heel zone (TMAXHL: r=0,64;
p=0,05), and contact time with left midfoot (CML:
r=0,76; p=0,01), and in negative correlation with
results in absolute difference in maximum pressures
of left and right forefoot (MAXPF_D: r=-0,75;
p=0,01), and absolute difference in left and right step
length (GSL_D: r=-0,69; p=0,03).
4 DISCUSSION & CONCLUSION
Appropriateness of usage of pedobarographic
measure protocol as an extension of regular AS
diagnostic tests/tools was tested.
Contrary to findings of Aydina et al., 2015, i.e.
there is no clinically significant correlation between
clinical scores and static pedobarographic
measurements, and of Gruić, et al. 2016., i.e. plantar
pressure and force gait parameters seem to have no
diagnostic value in determining scoliosis-specific
gait, initial findings in this research, within forward
stepwise regression analysis, found clear statistical
multiple correlation between clinical scores and
dynamic pedobarographic measurements.
Sample size calculations, however, do not allow
immediate and final conclusions about effects and
applicability of final results. Also, additional static
and dynamic tests should complement the diagnostics
that assesses a complex phenomenon such as AS
Partial contribution of individual
pedobarographic variable and limitations to statistical
reasoning of this relation lay within many statistical
tools which are found to be uncommon in research
covering AS and plantar pressure measurements.
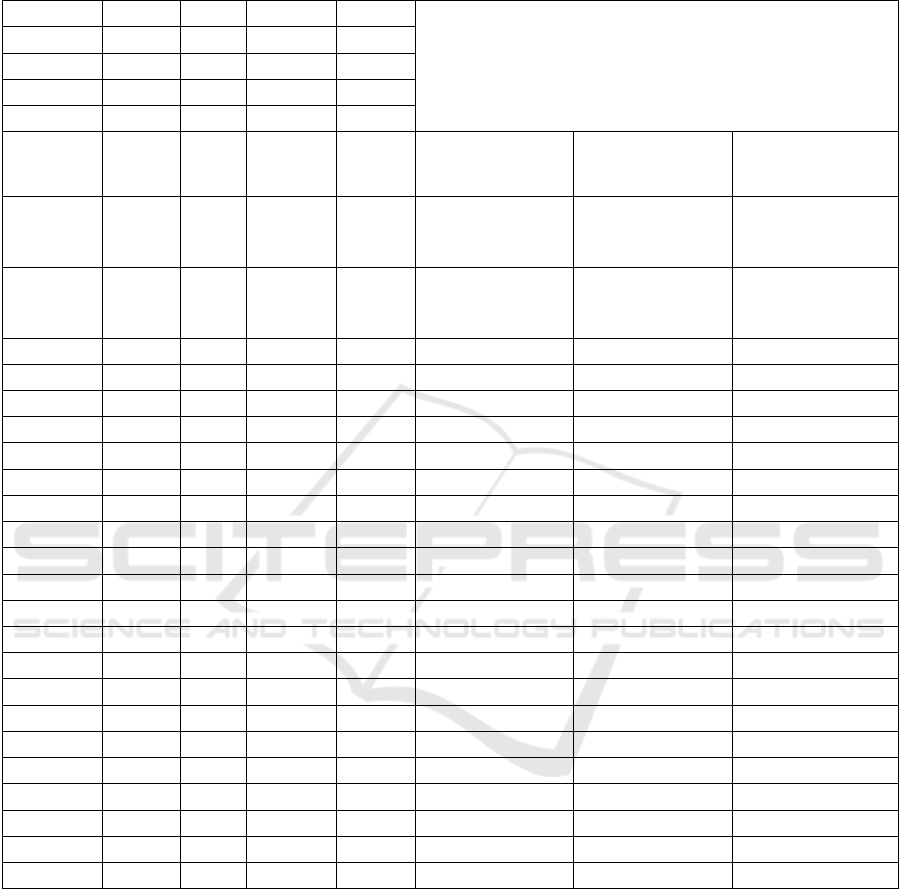
Table 1: Descriptive statistics - subjects’ info, AS status, pedobarographic variables; Regression summary and partial
contributions within forward stepwise regression analysis of contributions of pedobarographic variables to results in
dependent variables: BASFI, BASDAI and ASQoL.
N=10
Mean
SD
max D
K-S
Regression Summary (forward stepwise)
/
b* (standardized beta regression coefficients/weights); p-value (t)
Age
41,60
8,76
0,1920
p > .20
BM
76,70
18,29
0,2388
p > .20
BH
174,80
9,74
0,1056
p > .20
BMI
24,91
4,37
0,1755
p > .20
ASQoL
5,40
3,50
0,0955
p > .20
Adj.R2=,99*;
F(8,1)=1453E5
p<0,00006
BASDAI
1,82
1,04
0,2498
p > .20
Adj.R2=1,00;
F(8,1)=160E10
p<0,00000
BASFI
3,98
1,75
0,2203
p > .20
Adj.R2= ,99*;
F(8,1)=1007E5
p<0,00008
BSL
129,52
12,48
0,2294
p > .20
0,01; 0,04
CH_D
6,22
6,25
0,3648
p < ,15
0,12; 0,00
0,14; 0,00
CHR
57,41
11,13
0,2196
p > .20
0,00; 0,01
CML
72,04
4,01
0,1662
p > .20
0,29; 0,00
CMR
71,94
5,59
0,1611
p > .20
-0,02; 0,00
-0,02; 0,00
FTMF1L
16,30
3,33
0,1831
p > .20
-0,24; 0,00
FTMF2L
48,10
2,73
0,1567
p > .20
0,50; 0,00
GFRR
16,07
4,67
0,2060
p > .20
-0,92; 0,00
GSL
123,80
17,64
0,1374
p > .20
-1,11; 0,00
GSL_D
3,20
2,70
0,2717
p > .20
-0,69; 0,00
LT_D
0,04
0,05
0,3807
p < ,10
-0,57; 0,00
LTP_D
5,56
5,76
0,2593
p > .20
0,42; 0,00
MAXPFL
43,48
13,69
0,2609
p > .20
0,29; 0,00
MAXPFR
46,05
12,54
0,1881
p > .20
0,31; 0,00
MAXPHR
29,87
8,77
0,1307
p > .20
0,15; 0,00
MFL
736,36
144,48
0,1645
p > .20
0,20; 0,00
0,23; 0,00
MHL
518,80
89,90
0,2406
p > .20
0,00; 0,02
TMAXFL
76,36
2,27
0,2280
p > .20
0,50; 0,00
TMAXML
52,09
13,05
0,2148
p > .20
0,07; 0,00
TST_D
0,02
0,02
0,3334
p < ,20
-0,41; 0,00
TSTR
0,54
0,05
0,1326
p > .20
0,96; 0,00
CODE - description, unit, (L/R foot): BSL - Single support line, mm L; CH_D - Contact time H, % L/R, CHR - Contact time H, % R; CML
- Contact time MF, %L*; CMR - Contact time MF% R *; FTMF1L - Time maximal force1, % L; FTMF2L - Time maximal force2, % L;
GFRR - Foot rotation, degree R; GSL - Stride length, cm; GSL_D - Step length, cm L/R; LT_D - Time to change heel to FF, sec L/R;
LTPR - Time to change heel to FF, % R; MAXPFL - Max pressure FF, N/cm2 L; MAXPFR - Max pressure FF, N/cm2 R; MAXPHR -
Max pressure H, N/cm2 R; MFL - Maximum force FF, N L; MHL - Maximum force H, N L; TMAXFL - Time max force FF, %L*;
TMAXML - Time max force MF, %L*; TST_D - Step time, sec L/R; TSTR - Step time, sec R; (*% of stance time; FF-Forefoot, MF-
Midfoot, H-Heel); ( ‘_D ‘ in name of variable means absolute difference between left and right - L/R)
ACKNOWLEDGEMENTS
Research was conducted by Research Group of
Biomechanics Laboratory, Institute of Kinesiology,
Faculty of Kinesiology, as a continuation of
cooperation with Department of Rheumatology,
Physical Medicine and Rehabilitation, University
Hospital Centre Sisters of Mercy based on outcomes
of UniZg project “Pedobarographic features of

human locomotion in sports and medicine”. Authors
declare that there is no conflict of interest.
REFERENCES
Aydina E., Turana Y., Tastabana E., Omurlub I. K., and
Sendura O.F. (2015) Plantar pressure distribution in
patients with ankylosing spondylitis. Clinical
Biomechanics, Vol. 30, Issue 3, March 2015, pp238-
242,https://doi.org/10.1016/j.clinbiomech.2015.02.003
Doward L. C., Spoorenberg A., Cook S. A., Whalley D.,
Helliwell P. S., Kay L. J., McKenna S. P., Tennant A.,
van der Heijde D. and Chamberlain M. A. (2003)
Development of the ASQoL: a quality of life instrument
specific to ankylosing spondylitis, Ann Rheum Dis.
2003;62:20–26.
Giacomozzi, C. (2011). Potentialities and Criticalities of
Plantar Pressure Measurements in the Study of Foot
Biomechanics: Devices, Methodologies and
Applications, Biomechanics in Applications, Dr Vaclav
Klika (Ed.), ISBN: 978-953-307-969-1.
Grazio S., Grubišić F., Nemčić T., Matijević V., Skala H.
(2009). Pouzdanost i valjanost hrvatske inačice Bath
funkcijskog indeksa za ankilozantni spondilitis
(BASFI) i Bath indeksa aktivnosti bolesti za
ankilozantni spondilitis (BASDAI) u bolesnika s
ankilozantnim spondilitisom (The reliability and
validity of Croatian version of the Bath Ankylosing
Spondylitis Functional Index (BASFI) and Bath
Ankylosing Spondylitis Disease Activity Index
(BASDAI) in patients with ankylosing spondylitis),
Reumatizam (0374-1338) 56 (2009), 2; 63-76.
Gruic I., Cebovic K., Radas J., Bolcevic F. and Medved V.
(2015). Pedobarographic Features of Gait Measured by
FDM1.5 PMD.In Proceedings of the 3rd International
Congress on Sport Sciences Research and Technology
Support - Volume 1: icSPORTS, ISBN 978-989-758-
159-5, pages 66-71. DOI: 10.5220/0005662800660071.
Gruić I., Cebović K. and Medved V. (2016). Comparison of
Pedobarographic Profile in Young Males with Left and
Right Scoliotic Posture.In Proceedings of the 4th
International Congress on Sport Sciences Research and
Technology Support - Volume 1: icSPORTS, ISBN 978-
989-758-205-9, pages 89-95. DOI:
10.5220/0006085400890095.
Specifications and operating instructions/software User
manual, zebris Medical, Gmbh.
APPENDIX
A) Questionnaire: BASFI (Croatian version of the Bath
Ankylosing Spondylitis Functional Index) (answers on a
scale from ‘Easy’ to ‘Impossible’)
1. Putting on your socks or tights without help or
aids (e.g. sock aid).
2. Bending from the waist to pick up a pen from the
floor without aid.
3. Reaching up to a high shelf without help or aids
(e.g. helping hand).
4. Easy
5. Getting up from an armless chair without your
hands or any other help.
6. Getting up off the floor without help from lying
on your back.
7. Standing unsupported for 10 minutes without
discomfort.
8. Climbing 12-15 steps without using a handrail or
walking aid.
9. Looking over your shoulder without turning your
body.
10. Doing physically demanding activities (e.g
physiotherapy exercises, gardening or sports).
11. Doing a full days activities whether it be at home
or at work.
B) Questionnaire: BASDAI (Croatian version of the
Bath Ankylosing Spondylitis Disease Activity
Index) (placing a mark on line below to indicate
answer to each question relating to the past week
on a scale from ‘None’ to ‘Very severe’, and for
q6: 0 hrs, ½, 1, 1½, 2 or more hours; add the sum
of answers 5. and 6., first divided by 2, to answers
1.-4., and then divide total sum by 5)
1. How would you describe the overall level of
fatigue/tiredness you have experienced?
2. How would you describe the overall level of AS
neck, back or hip pain you have had?
3. How would you describe the overall level of
pain/swelling in joints other than neck, back, hips
you have had?
4. How would you describe the overall level of
discomfort you have had from any areas tender to
touch or pressure?
5. How would you describe the overall level of
morning stiffness you have had from the time you
wake up?
6. How long does your morning stiffness last from
the time you wake up?
C) Questionnaire: ASQoL (Ankylosing Spondylitis
Quality of Life Questionnaire) (answers are ‘Yes’
or ‘No’; Each statement on the ASQoL is given a
score of “1” or “0”. A score of “1” is given where
the item is affirmed, indicating adverse QoL. All
item scores are summed to give a total score or
index. Scores can range from 0 (good QoL) to 18
(poor QoL). Cases with more than three missing
responses (ie more than 20%) cannot be allocated
a total score. For cases with between one and
three missing responses, the total score is
calculated as follows: T=18x/18-m where: T is
the total score, x is the total score for the items
affirmed and m is the number of missing items;
Doward et al, 2003)
1. My condition limits the places I can go
2. I sometimes feel like crying
3. I have difficulty dressing
4. I struggle to do jobs around the house
5. It’s impossible to sleep
6. I am unable to join in activities with my
friends/family
7. I am tired all the time
8. I have to keep stopping what I am doing to rest
9. I have unbearable pain
10. It takes a long time to get going in the morning
11. I am unable to do jobs around the house
12. I get tired easily
13. I often get frustrated
14. The pain is always there
15. I feel I miss out on a lot
16. I find it difficult to wash my hair
17. My condition gets me down
18. I worry about letting people down
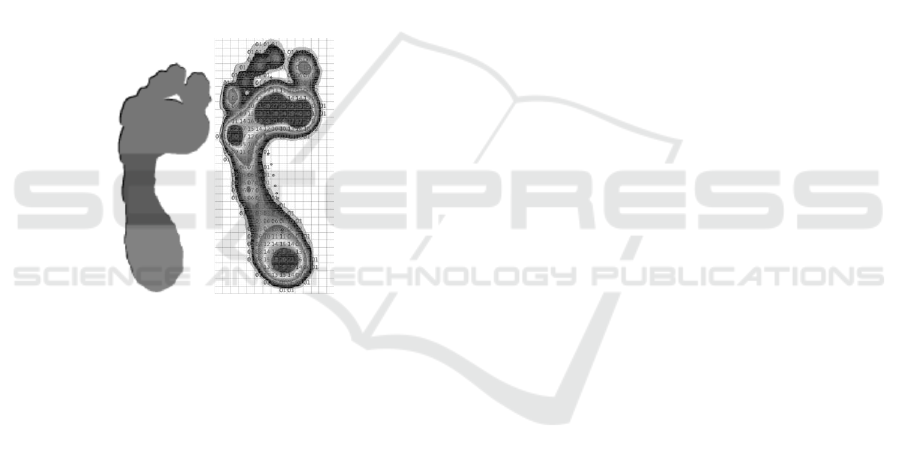
D) Kinetic models for foot analysis (3 zones-
forefoot, midfoot, heel
Figure 1: Kinetic models for foot analysis (Zebris: ref 7.).
