
A Collaborative Learning Environment of the Medical Diagnosis on
the Basis of the Clinical Reasoning Theory
Mohamed Abderraouf Ferradji and Abdelmadjid Zidani
LaSTIC laboratory,
Department of Computing, Batna University, Batna, Algeria
Keywords: Clinical Reasoning, Medical Education, Medical Pedagogy, Collaborative Learning, Social Knowledge
Building, Synchronous Interaction, Group Awareness.
Abstract: In collaborative clinical learning field, several recent pertinent studies showed that gathering learners with
their tutor still insufficient to improve students' learning quality and knowledge acquisition. Consequently,
focusing attention on professional skills within a collaboration environment seems to be the most
appropriate way to reach the wished learning objectives, particularly in a complex specialty such as medical
diagnosis learning. In this paper, we firstly introduce the concept of medical diagnosis from cognitive
studies view that have been performed in the field of medical education. Then, we will discuss our shared
web environment designed to support distance diagnosis learning, which aims to promote knowledge co-
construction and collaboration between learners.
1 INTRODUCTION
In the medical field, the competencies of making a
diagnosis are refined through the good structuring of
an important mass of medical knowledge in the
doctor’s memory, and the mastery of relevant
reasoning process (Bordage, 2005; Eva, 2005;
Nendaz et al., 2005). However, the observation of
learning strategies in the medicine faculties of
Algeria, showed that the classical objective-based
pedagogy represent the most used learning method.
Indeed, we led an investigation mainly based on
observations and interviews with a medical staff
within a gynaecology and obstetrics emergency unit
in Algeria.
In fact the typical used approach is based on the
direct transmission of knowledge and considers
learner as an inactive entity with a great capacity of
theoretical knowledge memorization. Even in the
internships occurring at hospitals and before the
patient’s bed, we have noticed that the clinician
teacher has not always time and pedagogic strategy
that allow him to explain the approach of the used
reasoning and the mobilized knowledge to achieve
the stated diagnosis ( Nendaz et al., 2005).
Moreover, the quality of the acquired knowledge
depends on the richness of the met cases during the
internship cycle. To overcome these challenges,
many medicine faculties across the world have
introduced the collaborative learning methods
(Quénu-Joiron, 2002).
The integration of these learning methods in the
medicine faculties of Algeria requires radical
changes in terms of educative systems and even on
the faculties’ infrastructures. Moreover, this
pedagogic activity is based on learning in small
groups of learners and its organization in classroom
mode is not always easy (Ortega, 2005). Especially
in Algeria with the area of (2 381 741 Km
2
) and that
doesn’t allow the very limited number of
experimented doctors to contribute to the
pedagogical activities in all medicine faculties. This
fact limits significantly the learners’ opportunities,
in far southern areas of benefiting from their
experiences in a fair way. This observation ensues
directly from our study about the imbalance in terms
of specialized doctors’ availability compared to the
north of the country. The direction into the distant
collaborative learning support tools may bring more
flexibility and fluency in time and in space of
diagnosis learning (Quénu-Joiron, 2002).
Besides that, the fact of gathering learners with a
tutor in a team, either in classroom or distance mode,
is not enough to improve the learning quality and
knowledge acquisition, as supplementary factors
related to the professional skills, on one hand, and to
the collaboration, on the other hand, must be
80
Ferradji, M. and Zidani, A.
A Collaborative Learning Environment of the Medical Diagnosis on the Basis of the Clinical Reasoning Theory.
In Proceedings of the International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2016), pages 80-87
ISBN: 978-989-758-180-9
Copyright
c
2016 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

considered.
In this paper, we propose a web-based learning
environment supporting the collaboration, the
coordination and the communication between a
group of learners who are geographically distant,
and share a common task of elaborating a medical
diagnosis in synchronous mode. Finally, to increase
our environment efficiency, we have considered the
most pertinent cognitive studies achieved in the field
of medical education, as well as the researches
dedicated to the clinical reasoning process modeling.
2 CLINICAL REASONING
In the medical education field, the major of the
definitions related to the clinical reasoning process
that have been proposed agree on a common point. It
is about the perception of such process as a set of
mental activities that allow the clinician to make the
right decision while dealing with a specific clinical
situation (Barrows, 1980; Higgs, 2008).
Furthermore, studies that have been achieved in this
area have revealed that doctors use diverse methods
of reasoning. These methods are mainly based on
two classes of reasoning: analytical and non-
analytical processes as mentioned by Pelaccia
(2011), as well as the study achieved by Croskerry
(2005).
According to the analytical reasoning approach,
a physician can explicitly draw his own reasoning
process (Duquerroux, 2009; Evans, 2008). Through
such drawing he may then establish a relationship
between the patient’s signs or symptoms and the
identification of the categories of diseases associated
with them ((Eva, 2005). Such kind of reasoning is
generally used by doctors who have very little
experience and which must always follow a set of
steps that allow them to confirm a diagnosis. It is
even used in complex clinical or soon encountered
cases, where the doctor can not directly establish a
diagnosis and will have to resort to reasoning efforts
to reach the final diagnosis (Edwards et al., 2004).
However, according to the non-analytic
approach, the physician cannot explain the used
reasoning process (Duquerroux, 2009; Evans, 2008).
So the non-analytical reasoning can be used in
typical cases where the physician can make a
diagnosis without deploying reasoning efforts,
especially when the considered case is characterized
by its similarity with a specific disease prototype.
Such reasoning way is mainly used by experienced
doctors who can systematically make diagnoses
while mobilizing a minimum of their conscience
through a direct projection of the current processed
case on a similar well known one (Croskerry, 2005;
Eva, 2005;Nendaz et al., 2005; Pottier & Planchon,
2011).
In this paper we mainly focus our work on the
complex process of hypothetical-deductive
reasoning (Figure 1). Such process may be
considered as a part of the analytical process and,
remains as the most used method in the clinical
training field (Coderre et al., 2003). According to the
analytical approach, the physician proposes a set of
early hypotheses, based on the preliminary
interaction with the patient, which seem to be the
most pertinent.
Figure 1: Hypothetical-deductive process of clinical
reasoning (Nendaz et al., 2005).
The number of those hypotheses is, generally,
comprised between 4 and 5 suggestions. After
additional clinical information gathering step, based
on the hypotheses proposed before, an interpretation
of these data must be carried out to check the
compatibility between the additional data and the
proposed hypotheses. Such verification allows for an
evaluation of the hypotheses that determines if it
should be accepted, rejected or reevaluated. It should
be noted here that it is quite possible that new
hypotheses may be generated and evaluated during
the next iterations. Thus the iterative process can
proceed through a cycle that will continue while the
final diagnosis still not reached (Nendaz et al., 2005;
Vanpee, Gillet, & Godin, 2002).
We must understand well that the efficiency of
the reasoning process is highly dependent on the
A Collaborative Learning Environment of the Medical Diagnosis on the Basis of the Clinical Reasoning Theory
81

way under which knowledge is structured in the
clinician long term memory (Steward et al., 1991).
Indeed, the most significant cognitive studies in
this area showed that the clinical cases encountered
during clinical experience provide physicians and
students with the ability to better structure their
knowledge and build pertinent inference networks,
which can be unconsciously activated every time
they are faced to a new clinical situation (Bordage,
2005; Harasym, Tsai, & Hemmati, 2008).
Consequently, the quality of memory knowledge
structuring is effectively a key factor that directly
impacts on clinicians ’skills and abilities,
particularly for students.
Therefore, one notices that a learning method of
the medical diagnosis becomes relevant since it
allows learners to easily overcome the challenges
related to the reasoning process, to effectively
structure their knowledge (Chamberland, 2007).
Learners collaborate also with others and it seems
that it still the most practical used way in their real
contextual work as reported by numerous pertinent
studies related to such issue (Aarnio et al., 2010;
Lerner, Magrane, & Friedman, 2009; Zwarenstein,
Goldman, & Reeves, 2009).
Concerning our environment design, we have
adopted the analytical approach because it seems to
be the most suitable for learners’ training while it
favors interaction and negotiation between them and
thus promotes collaboration to enable social
knowledge construction. Indeed, such approach
provides for students the opportunity to deal
naturally with the reasoning process used by
experienced clinicians, while they work together on
a common clinical case and manage both
construction and structuring of their knowledge. The
method may even generate situations of socio-
cognitive conflicts that extend the learning process
towards social activities as they arise in real clinical
settings.
3 ENVIRONMENT
PRESENTATION
Our research approach reflects, the socio-
constructivist theory point of view, which considers
learning as an activity that overcomes the individual
scale, and projects it in a larger framework. It is
about the social process of knowledge construction,
which favors interaction and communication
between learners.
As we mentioned it previously, our environment
is based on the Hypothetical-deductive process,
which is considered as the most effective method in
the field of the medical education. Indeed, though
this process allows clinical reasoning to be modelled
according to a way that is individually used by
experienced doctors, we tried in our work to adapt it
for distant collaborative learning situations that are
based on synchronous interaction. Our approach is
intended to favour the social aspect within the
learning environments through a set of appropriate
tools supporting interaction and negotiation
activities as well as learners’ points of view
confrontation. Our main objective here is to enhance
the collaborative reasoning and knowledge co-
construction, as well as providing to learners the
suitable opportunities to master the most utilized
reasoning process in the clinical background.
Access to a remote collaborative learning
environment, should be considered across
heterogeneous platforms machines. This makes
interoperability a fundamental factor in the
assessment of the system quality and effectiveness.
The web 2.0 concept seems to be the most adequate
technical solution to effectively overcome machines
incompatibility problems. Taking into account also
the excessive keen interest of the current generation
of learners for any web technology, it would be
injudicious to provide learning assistance models
while ignoring such fact. Thus, the technological
solution we propose here is designed through a web-
based approach. Through such way, we expect to
have learners’ full commitment while taking part to
distance learning sessions and lead them to
effectively interact with their peers. Finally, a key
factor that also affects learners interactions, concerns
the environment external presentation.
Therefore, our preoccupation was obviously to
provide a learning environment with an ergonomic
easy to use web interface for learners in order to
significantly reduce their cognitive loads, and then
enable them to focus more on the clinical reasoning
and the common case solving.
Through a typical collaborative learning
scenario, a clinical problem must be presented to
learners as a spontaneous complaint announced by a
patient. This complaint is elaborated by the tutor
who will supervise the whole problem solving
process. We must notice here that the case
elaboration should be done by taking into account
the tutor’s learning objectives that he plans to
achieve with learners. Another key factor concerns
the problem’s complexity degree which must be
adapted to learners’ skills and work session duration.
Consequently, the suggested environment
consists of three workspaces (Figure 2). The first
ICT4AWE 2016 - 2nd International Conference on Information and Communication Technologies for Ageing Well and e-Health
82

workspace is intended for the preparation of the
clinical case by the tutor, the second one is designed
to support collaborative learning sessions and the
third one allows learners to review any previous
learning session, by replaying different scenarios of
the associated clinical solved problems.
Figure 2: Environment workspaces.
3.1 Clinical Case Elaboration
The first environment’s workspace is private and is
accessible only to the tutor where he (she) elaborates
the clinical case content that will be collaboratively
solved by learners under a synchronous mode. We
have to remind that learners work on the same case
at the same time through a WYSIWIS way (What
You See Is What I See), which is a synchronous way
of sharing the same view, so the actions performed
by one of them are immediately made visible to the
others. The case elaboration includes the clinical
case presentation, collecting patient's personal
information, anamnesis or clinical history, patient’s
clinical and paraclinical exams related to the case as
well as the pertinent related documentation required
when solving the problem. We should note that
efficiency of the collaborative session depends
greatly on the clinical case elaboration. In addition,
the tutor has the possibility of adapting or enriching
more the studied case as the learning session
evolves. The prepared content will be progressively
displayed depending on the session’s phase and
learners’ needs. Once a case elaboration is fully
completed, the collaborative learning session of the
clinical problem solving may be achieved within the
second shared workspace, which represents the
environment’s core and the most significant step of
the clinical reasoning training process. Learners can
access it through a simple authentication protocol
based on the user’s login and password. To allow
group awareness, each learner’s action in the shared
workspace is colored by his specific associated
color. Such way allows his peers to intuitively
identify him (her) within the shared workspace via
his contributions. The patient’s role is assigned to
the tutor, who is considered as the session’s
facilitator and the main source of the patient’s
information.
3.2 Medical Diagnosis Collaborative
Learning Session
The collaborative learning session comprises three
work phases according to the clinical reasoning
Hypothetical-deductive process (Figure 1, Sec. 2). In
the following paragraphs of this section, we will
discuss each phase and bring more details through
our environment interface views.
3.2.1 Clinical Problem Representation
The first phase of the session (Figure 3) takes into
account the representation of the clinical problem,
which constitutes a key step of the whole process.
We should note that for the medical community, the
direct exploration of the patient’s complaint in the
clinical problem solving has a negative effect on the
reasoning approach as well as on the quality of the
suggested diagnosis. It is rather highly required first
to look for the most appropriate medical meaning
that should be associated to such complaint and then
generate what we call semantic axes (man/woman,
unilateral/bilateral, acute/chronic) whose medical
data are compared and contracted (Bordage, 1999,
2005; Steward et al., 1991).
The resulting semantic transformation called also
mental representation of the problem enables
optimising the research of pertinent hypotheses in
the clinician’s memory. Compared to experienced
doctors, novices ones generally encounter
difficulties when building their mental
representation of the met case, this may lead to a
random generation of hypotheses and to an uncertain
research on clinical data. Consequently, it seems
very important to fix the problem’s representation as
one of the key learning objectives in the clinical
background (Bowen, 2006).
In this phase of the session, learners elaborate
their own representations of the clinical problem.
A Collaborative Learning Environment of the Medical Diagnosis on the Basis of the Clinical Reasoning Theory
83

Figure 3: Interface view of the first step of the learning session.
Each learner can visualize the others’
representations and leave them comments which will
be displayed as notifications. According to these
remarks, learners can adjust or correct their
representations, and the most agreed one will be
selected as the relevant collaborative representation.
Regarding to the patient’s medical history,
learners can explore a fictive medical patient record
to collect any required information for their medical
representation. Our shared workspace embeds
diverse assistance tools that learners may use. To
support communications within the shared
workspace, we provided a conversational tool with
the patient, and another for collaborative discussions
among the group’s members. Learners can also
access at any time to the documentation
recommended and seek assistance from tutors to
remove ambiguities or seek clarifications. Finally, to
support learners’ notes and remarks editing, we have
integrated within the shared workspace a shared text
editor.
As we have previously indicated, the problem’s
representation quality has a great impact on the
pertinence of the clinical reasoning approach and the
correctness of the proposed diagnosis. In our
environment, we have provided to learners the
opportunity to compare and confront their different
representations in order to favour brainstorming
activity during clinical reasoning and enable them to
significantly improve their skills.
3.2.2 Hypotheses Generation, Filtering and
Structuring
The first generation of hypotheses, allows learners to
start collecting as much information as possible on
the considered case. The following step will be
achieved through interactions among learners and
lead them to structure the clinical problem and
reduce the number of its associated suggestions.
Such selection of hypotheses allows learners to
optimize their work memory efficiency while
useless details don’t have to be memorized and
overload it, which may have great impact on
learners’ focusing ability (Nendaz et al., 2005). We
note here that the work memory enables keeping
short term information in mind, some seconds or
minutes, to mentally realize the associated
operations.
At the second step of the session, learners can
suggest early hypotheses (Figure 4). Each one is
displayed with the specific learner’s color that has
suggested it. It follows then interactions between
learners through explicit comments related to these
hypotheses which may be added to naturally express
learners’ diverse points of view.
We notice that with the collaborative learning
approach, it is strongly possible that among the
generated hypothesises we find many of them that
are not suitable for the current case. Consequently,
learners should filter them at the beginning before
the following steps. Such situation that seems to be
ICT4AWE 2016 - 2nd International Conference on Information and Communication Technologies for Ageing Well and e-Health
84
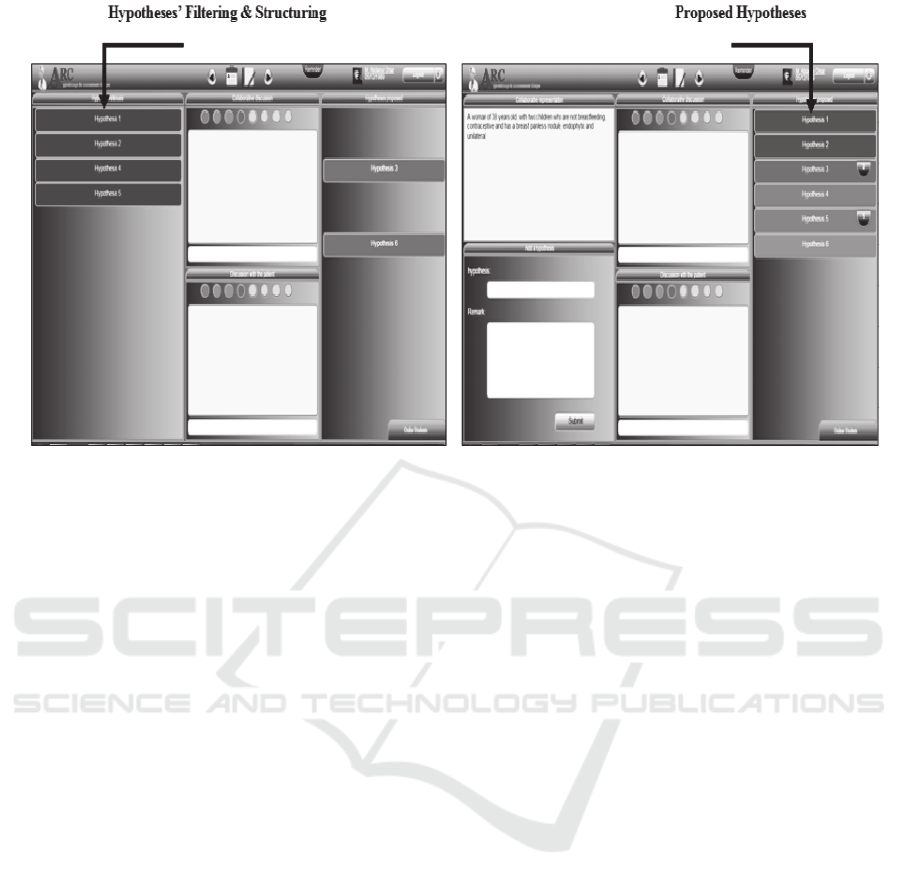
Figure 4: Hypotheses generating, filtering and structuring.
as a constraint is pedagogically interesting. Indeed
learners reported that they found it very useful while
it generates strong wish for interactions and
exchanges between them and enables them by the
way to better structure their knowledge.
Furthermore, the next step will be easier while
learners have only to focus their attention on the
most probable hypothesis, which can improve the
quality of the problem solving approach.
3.2.3 Additional Information Research and
Hypotheses Evaluation
The third step of the session concerns additional
information requesting in order to confirm or reject
the suggested hypotheses (Figure 5). Such
information may be collected through the patient’s
questioning, signs confirmation and complementary
examinations. The requested information will
automatically be sent as soon as it is available in the
data base. For more pedagogic clarifications, the
tutor can ask any requesting learner to motivate his
request in order to increase the debate around the
question if he deems it relevant. For example, in the
case of an imaging diagnostic examination request
(scanner, ECG, radio ...) the image will be displayed
in a shared window where learners can insert
graphic marks or textual comments.
During the hypotheses evaluation step and in
case of conflictual situations, learners may use a
voting embedded tool to complete filtering them.
Any learner has the opportunity to express and
motivate his point of view. Through the negotiation
process that is fully coordinated within the
environment, learners’ ideas may dynamically
evolve. This is especially intended to enhance
learners’ skills while providing them with the
opportunity to interact within a shared workspace.
Furthermore through awareness features, each
hypothesis is displayed with one of these specific
colours that explicitly shows its state according to
the learners’ voting process. Thus, the green color
means that most of the learners have agreed the
hypothesis; the orange one that few learners among
the group have rejected it; and the red one is
displayed when it has been rejected by most of them.
The collaborative reasoning process progress
may be simultaneously edited by learners through a
graphical structure. Such structure is visualized by
learners and dynamically evolves during a work
session. It allows each learner to evaluate his
contributions with regard to the others and adjust
them according to the diagnosis evolution. The main
goal of the reasoning process graphical structure is
to provide as much as possible assistance to learners
and enable them to better organize knowledge in
their long-term memory. Therefore, they will be
predisposed to reuse the acquired knowledge during
work session. We notice that at the current state of
our research we used a simple graphical structure to
facilitate learners’ task. However, we plan in the
short term to recourse to concept mapping
representation which is more suitable while it
illustrates the relationships between symptoms and
disease related to the treated case.
A Collaborative Learning Environment of the Medical Diagnosis on the Basis of the Clinical Reasoning Theory
85
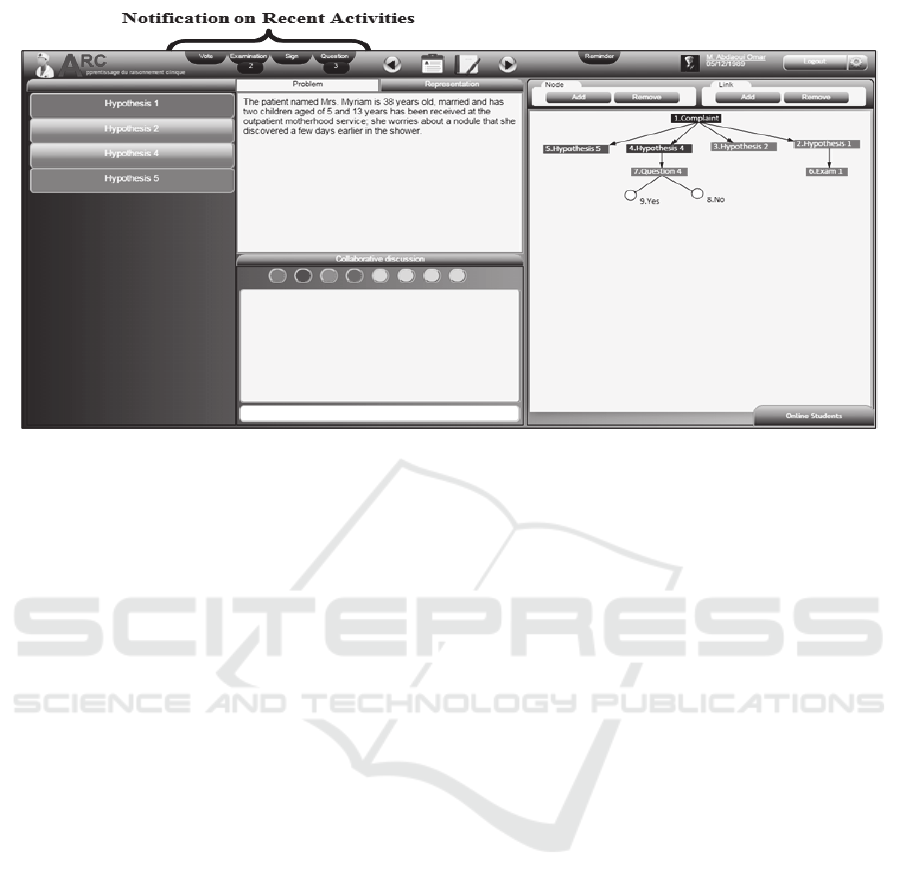
Figure 5: Interface view of the third step of the learning session.
Finally, to model the iterative approach of the
hypothetical-deductive method, our environment
allows learners to review previous steps of the
clinical reasoning process to make changes either on
the problem collaborative representation, or on the
proposed hypotheses, as new hypotheses can be
generated and guide the diagnosis to alternative
directions. Furthermore, in order to keep all the
participants attention and let them strongly focused,
the environment diffuses immediately notifications
when new actions are performed by learners. Thus
when one clicks a specific notification, a list of
shortcuts is displayed to allow direct access to the
associated activities areas. We think that through
such approach, each learner will have a complete
idea about others current activities. For more
transparency and coordination within the shared
workspace, we also explore reminding notifications
that appear when for example a learner proposes a
hypothesis or an examination already mentioned
before to recall him a redundancy case.
3.3 Individual and Collaborative
Review of Previous Learning
Sessions
In the classical methods of learning, it is widely
recognized that the majority of learners cannot
follow and understand the entire session’s content,
where each of them reaches some level of
comprehension and can only improve it during the
revision. Thereof, the third section of our
environment provides learners with the opportunity
of replaying any previous session scenario to fill the
gaps. The review session may happen through both
individual and collaborative mode and learners can
add questions or observations to the session’s
content.
4 CONCLUSIONS AND FUTURE
WORK
In this paper, we have discussed our collaborative
web-based environment designed to support medical
diagnosis learning and synchronous interaction
between learners. Its design aims to favour the
professional skills acquiring for medical diagnosis
learners, and to enhance collaboration between
them.
In order to model a better learning opportunities,
we have tried to explore the most pertinent cognitive
studies results achieved in the medical education
field, that have tackled the hard issue of the clinical
reasoning and highlighted the most relevant
impacting factors. Finally for the next step of our
research work, we plan to elaborate an experimental
protocol through our collaboration with our partners
at the faculty of medicine. This step will enable us to
draw the necessary lessons to improve our design
proposition.
ICT4AWE 2016 - 2nd International Conference on Information and Communication Technologies for Ageing Well and e-Health
86

ACKNOWLEDGEMENTS
This paper is the result of our collaboration with the
medical staff within a gynecology and obstetrics
emergency unit at Batna town, which we especially
like to thank all of them. We also extend our thanks
to the students of the service for their patience and
cooperation during this study, and for the fruitful
exchange of ideas.
REFERENCES
Aarnio, M., Nieminen, J., Pyörälä, E., & Lindblom-
Ylänne, S., 2010. Motivating medical students to learn
teamwork skills. Medical Teacher, 32(4), e199-e204.
Barrows, H. S., 1980. Problem-based learning: An
approach to medical education. Springer Publishing
Company.
Bordage, G., 1999. Why did I miss the diagnosis? Some
cognitive explanations and educational
implications. Academic Medicine, 74(10), S138-43.
Bordage, G., 2005. La prise de décision en médecine:
quelques mécanismes mentaux et des conseils
pratiques. La revue de médecine interne, 26, S14-S17.
Bowen, J. L., 2006. Educational strategies to promote
clinical diagnostic reasoning. New England Journal of
Medicine, 355(21), 2217-2225.
Chamberland, M., 2007. Les séances d’apprentissage du
raisonnement clinique (ARC): description de la
méthode pédagogique. Université de SHERBROOKE.
Coderre, S., Mandin, H., Harasym, P. H., & Fick, G. H.,
2003. Diagnostic reasoning strategies and diagnostic
success. Medical education, 37(8), 695-703.
Croskerry, P., 2005. The theory and practice of clinical
decision-making.Canadian Journal of
Anesthesia/Journal canadien d'anesthésie, 52, R1-R8.
Duquerroux, V., 2009. Etude du raisonnement du clinicien
expérimenté et de l'étudiant: apports de la psychologie
cognitive (Doctoral dissertation).
Edwards, I., Jones, M., Carr, J., Braunack-Mayer, A., &
Jensen, G. M., 2004. Clinical reasoning strategies in
physical therapy. Physical therapy, 84(4), 312-330.
Eva, K. W., 2005. What every teacher needs to know
about clinical reasoning.Medical education, 39(1), 98-
106.
Evans, J. S. B., 2008. Dual-processing accounts of
reasoning, judgment, and social cognition. Annu. Rev.
Psychol., 59, 255-278.
Harasym, P. H., Tsai, T. C., & Hemmati, P., 2008. Current
trends in developing medical students' critical thinking
abilities. The Kaohsiung journal of medical
sciences, 24(7), 341-355.
Higgs, J., 2008. Clinical reasoning in the health
professions. Elsevier Health Sciences.
Lerner, S., Magrane, D., & Friedman, E., 2009. Teaching
teamwork in medical education. Mount Sinai Journal
of Medicine: A Journal of Translational and
Personalized Medicine, 76(4), 318-329.
Nendaz, M., Charlin, B., Leblanc, V., & Bordage, G.,
2005. Le raisonnement clinique: données issues de la
recherche et implications pour l’enseignement.
Pédagogie médicale, 6(4), 235-254.
Ortega, E. M., Lessard, Y., Burgun, A., & Le Beux, P.,
2005, September. Virtu@ I Consult@ tion: an
interactive and multimedia environment for remote
clinical reasoning learning in cardiology.
In Computers in Cardiology, 2005 (pp. 829-832).
IEEE.
Pelaccia, T., Tardif, J., Triby, E., & Charlin, B., 2011. An
analysis of clinical reasoning through a recent and
comprehensive approach: the dual-process
theory. Medical education online, 16.
Pottier, P., & Planchon, B., 2011. Description of the
mental processes occurring during clinical
reasoning. La Revue de médecine interne/fondée... par
la Société nationale francaise de médecine
interne, 32(6), 383-390.
Quénu-Joiron, C., 2002. Une contribution aux systèmes
supports de Formation Médicale Continue à distance
et d'apprentissage entre pairs: conception et
expérimentation du forum DIACOM (Discussions
Interactives à bAse de Cas pour la fOrmation
Médicale) (Doctoral dissertation, Université de
Picardie Jules Verne).
Steward, D., BORDAGE, G., & LEMIEUX, M., 1991.
Semantic structures and diagnostic thinking of experts
and novices. Academic Medicine, 66(9), S70-S72.
Vanpee, D., Gillet, J. B., & Godin, V., 2002. Séance
d'apprentissage au raisonnement clinique: Une
méthode potentiellement intéressante pour
l'enseignement de la médecine aiguë. Louvain
médical, 121(10), 425-429.
Zwarenstein, M., Goldman, J., & Reeves, S., 2009.
Interprofessional collaboration: effects of practice-
based interventions on professional practice and
healthcare outcomes. Cochrane Database Syst
Rev, 3(3).
A Collaborative Learning Environment of the Medical Diagnosis on the Basis of the Clinical Reasoning Theory
87
