
Temporal Detection of Guideline Interactions
Luca Piovesan
1
, Luca Anselma
1
and Paolo Terenziani
2
1
Dipartimento di Informatica, Università degli Studi di Torino, Torino, Italy
2
DISIT, Università del Piemonte Orientale “Amedeo Avogadro”, Alessandria, Italy
Keywords: Computer-interpretable Clinical Guidelines, Comorbidity Treatment, Guideline Interaction Detection,
Ontology of Time and Interactions, Temporal Reasoning.
Abstract: Clinical practice guidelines are widely used to support physicians, but only on individual pathologies. On
the other hand, the treatment of patients affected by multiple diseases is one of the main challenges for the
modern healthcare. This requires the development of new methodologies, supporting physicians in the
detection of interactions between guidelines. In a previous work, we proposed a flexible and user-driven
approach, helping physicians in the detection of possible interactions between guidelines, supporting
focusing and analysis at multiple levels of abstractions. However, it did not cope with the fact that
interactions occur in time. For instance, the effects of two actions may potentially conflict, but practical
conflicts happen only if such effects overlap in time. In this paper, we extend the ontological model to deal
with the temporal aspects, and the detection algorithms to cope with them. Different types of facilities are
provided to physicians, supporting the analysis of interactions between both guidelines “per se”, and the
concrete application of guidelines to specific patients. In both cases, different temporal facilities are
provided to user physicians, based on Artificial Intelligence temporal reasoning techniques.
1 INTRODUCTION
The research about computer-interpretable clinical
guidelines (henceforth CIGs) has gained a relevant
role within the Medical Informatics community. In
the last twenty years, several different approaches
and projects have been developed to create domain-
independent computer-assisted tools for managing,
acquiring, representing and executing CIGs
(consider, e.g., the collections (Gordon and
Christensen 1995; Fridsma 2001; Ten Teije et al.
2008; Peleg 2013)).
By definition, clinical guidelines address
specific clinical circumstances (i.e., specific
diseases). However, unfortunately, specific patients
may be affected by more than one disease. The
treatment of comorbid patients (i.e., patients affected
by multiple diseases) is one of the main challenges
for the modern health care, also due to the aging of
population, and the consequent increase of chronic
diseases. This sets up the urgent need of developing
ways of merging multiple single-disease
interventions to provide professionals’ assistance to
comorbid patients (Riaño and Collado 2013).
However, though some CIGs covering
frequently occurring comorbidities might be
devised, the approach of considering all the possible
combinations of pathologies does not scale up. Thus,
there is a need for formal methodologies to support
physicians in the detection and resolution of
interactions between guidelines, and, ultimately, in
the process of merging two or more guidelines. This
is an increasingly “hot topic” within the Medical
Informatics community, and several approaches
have been proposed in the last years (see Section 5).
In a recent work in this context, we faced a
central issue in the management of multiple CIGs,
namely the interaction detection. In (Piovesan et al.
2014), we identified three different knowledge levels
at which interactions might occur: (i) level of the
intentions of the CIG actions, (ii) level of the goals
of the drug categories (recommended by the
pharmaceutical actions in the CIGs), and (iii) level
of drugs. We have also pointed out that, in turn,
levels (i) and (ii) may be structured at different
levels of detail. In (Piovesan et al. 2014), we have
also proposed an ontological representation for the
interactions at the different levels, as well as support
for interactive physician-driven analysis of the
interactions, at the different levels.
Nonetheless, to the best of our knowledge, until
now no CIG approach in the literature has focused
40
Piovesan L., Anselma L. and Terenziani P..
Temporal Detection of Guideline Interactions.
DOI: 10.5220/0005186300400050
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2015), pages 40-50
ISBN: 978-989-758-068-0
Copyright
c
2015 SCITEPRESS (Science and Technology Publications, Lda.)

on the temporal aspects of interactions. Indeed, a
non-temporal analysis can detect a possible
interaction between two actions in different CIGs,
identifying, e.g., a potential conflict between their
intentions (or effects). However, as long as no
temporal analysis is performed, such an interaction
is only “hypothetical”: actual interactions occur (and
the user physician should consider it) only in the
case that the conflicting intentions or effects overlap
in time. The approach in this paper is, to the best of
our knowledge, the first one starting to face such a
challenging problem. Indeed, we aim at supporting
physicians in the temporal analysis of interactions in
both “abstract” analysis of CIGs (not considering
patient data) and in the analysis during the execution
on specific patients.
In this paper, we consider time information
about action execution, effects and goals. After
introducing some preliminaries (Section 2), we
propose a representation formalism to model such
information (Section 3). Unfortunately, the only
representation of such knowledge is not enough to
support interaction detection: to this purpose, we
propose correct and complete temporal constraint
propagation techniques (Section 4). In particular, on
top of the temporal reasoning engine, we provide
users with different temporal facilities, to support
different forms of interaction detection. Finally,
Section 5 contains related works and conclusions.
2 PRELIMINARIES
Though the methodology we propose in this paper is
mostly system-independent, we based our approach
on GLARE (Subsection 2.1). In this preliminary
section, we also briefly describe our previous work
about comorbidity detection. In Subsection 2.2 we
summarize an ontology for interactions, and in
Subsection 2.3 we mention a (non-temporal)
detection algorithm.
2.1 Glare
GLARE (Guideline Acquisition, Representation and
Execution) has been built starting from 1997 in a
long-term cooperation between the Department of
Computer Science of the University of Piemonte
Orientale, Alessandria, Italy, and the Azienda
Ospedaliera San Giovanni Battista in Turin (one of
the largest hospitals in Italy).
GLARE supports the use of advanced artificial
intelligence techniques and decision support
techniques to assist physicians in merging two or
more guidelines developed for the treatment of
individual diseases.
In this paper, we extend GLARE to cope with
comorbidities. Our goal is twofold: on a side, we
aim to build a system able to, during the merging
process, draw “intelligent” conclusions starting from
the knowledge about CIGs; on the other, the system
must be “collaborative”. This last desideratum is due
to the stance that, when facing decision making in
medical informatics, black-box tools that take
decisions for her/him could be not very useful for
the user physician. Instead, a tool that guides
her/him in the decision-making process, helping
her/him to integrate also the knowledge that is not
modelled in the system but that (s)he owns, is more
useful and could improve the quality of the decisions
obtained. This is also the underlying philosophy of
the mixed initiative approach in artificial intelligence
and human-computer interaction. In fact, Horvitz
(1999) defines mixed initiative as “methods that
explicitly support an efficient, natural interleaving of
contributions by users and automated services
aimed at converging on solutions to problems”.
In GLARE, a CIG can be represented as a
hierarchical graph, where nodes are the actions to be
executed, and arcs are the control relations linking
them. GLARE distinguishes between atomic and
composite actions (plans), where atomic actions
represent simple steps in a CIG, and plans represent
actions that can be defined in terms of their
components via the has-part relation.
GLARE adopts five types of atomic actions:
work actions, i.e. actions that describe a
procedure which must be executed at a given
point of the CIG,
pharmaceutical actions, specifying a drug (or
drug category) to be administered to the
patient, and the dosage,
decision actions, used to model the selection
among different alternatives,
query actions, i.e. requests of information
(typically of patient’s parameters),
conclusions, which explicitly identify the
output of a decision action.
In this paper, we focus on composite actions, and
work and pharmaceutical atomic actions.
Actions in a CIG are connected through control
relations. Control relations establish which actions
can be executed next and in what order. In
particular, the sequence relation explicitly
establishes what the following action to be executed
is; the alternative relation describes which
alternative paths stem from a decision action, and
the repetition relation states that an action has to be
TemporalDetectionofGuidelineInteractions
41
repeated several times. The constrained relation is
used in order to express more complex temporal
relations between actions. In GLARE it is possible
to express precise and imprecise dates, durations,
delays, and complex forms of repetitions (Anselma
et al. 2006). For the sake of simplicity, in this paper
we adopt an easier approach for repetitions: we
suppose that the exact number of repetitions of
repeated actions is known, and explicitly express the
constraints between repetitions using the above
language.
2.2 Ontology of Interactions
In a recent work (Piovesan et al. 2014) we detailed
our preliminary semantic model for the description
of CIG actions and for the non-temporal interactions
occurring between them. For the sake of brevity, in
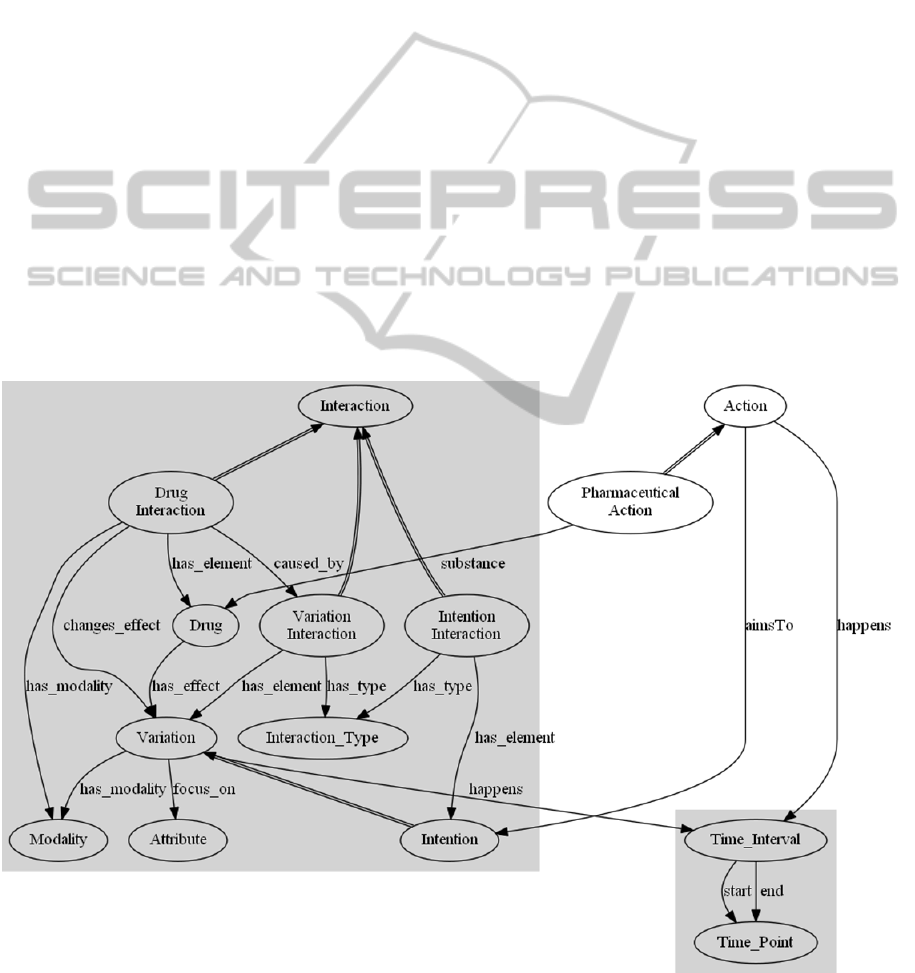
the left part of Figure 1we show a fragment of such
an ontology relevant to this paper. In our ontological
model, we focused on the goals of the actions and
the drugs administered by the pharmaceutical
actions, which are important sources of interactions
between CIGs.
In the ontology, a work, pharmaceutical or
composite action is described according to one or
more relations aimsTo with its goals, called
intentions, which are represented as variations of the
patient status. Each variation relates to exactly one
attribute (describing the patient status) and exactly
to one modality (of the variation). For instance, the
intention “Decrease Blood Pressure” is modelled by
the variation of the attribute “Blood Pressure” with
modality “Decreasing”.
Intentions are organized along a hierarchy of
ISA and PART-OF relations (not shown in Figure
1): high-level intentions can be broken up into
lower-level intentions, and alternative
decompositions are possible. For instance, the
intention “Decrease Blood Pressure” can be
decomposed into the alternatives “Decrease Blood
Volume”, “Inhibition of Angiotensin Converting
Enzyme (ACE)”, “Block of Calcium Channels” and
so on.
In addition, pharmaceutical actions are described
by the relation substance with the drug (or drug
category) they recommend. Drug categories and
drugs (the bottom level) are hierarchically organized
and each level of the hierarchy is related(has_effect)
to its effects, which are defined as variations of the
patient status. For the drug taxonomy, the ATC
Figure 1: Preliminary semantic model. Double-line arcs represent is-a relations.
HEALTHINF2015-InternationalConferenceonHealthInformatics
42

classification (http://www.whocc.no/atc/) is used;
however, our approach is independent of the
classification adopted. A distinguishing feature of
our approach is that it copes with interactions at
three different levels of abstraction: between the
intentions of actions, between drug categories and
between specific drugs (see concrete examples in
(Piovesan et al. 2014)).
Intention interactions are described by the
relation has_element, with the two intentions they
involve and by an interaction type, whose basic
values are concordance, discordance and
independence. However, further refinements are
possible, such as opposite for interactions focusing
on the same attribute, but discording in the modality.
Drug interactions, besides the two drugs or drug
categories they involve, are related to an effect (of
one of the two drugs) and to the variation the
interaction causes in such effect. Often, an
interaction between two drugs is caused by an
interaction between two of their effects. In order to
model such information, the property caused by
(optional) relates a drug interaction to a variation
interaction (described by the two variations it
involves and by a type). For instance, a drug
interaction between the drugs nalidixic acid and
calcium carbonate is caused by the variation
interaction between “absorption of nalidixic acid”
(of the first drug) and “urine alkalinization” (of the
second), and its result is a decrease of the antibiotic
absorption. Such example is detailed further in
Sections 3 and 4.
It is worth stressing that drug interactions are
independent of a specific guideline and of a specific
action because they do not involve actions. When a
new CIG is introduced in the knowledge base,
introducing the specifications of all the interactions
between its actions and the CIGs already stored is
not needed. Only the relations between the actions of
the new CIG and their intentions in the ontology and
(in the case of pharmaceutical actions) the drugs
they recommend must be pointed out.
Such ontological representation of intentions and
effects allows the adoption of algorithms that,
navigating the ontology, automatically infer the
types of many interactions between intentions or
drugs. More precisely, we implemented our
ontology using OWL DL (http://www.w3.org/TR/
owl2-overview/) and we expressed such a kind of
basic medical knowledge about interaction
recognition using Semantic Web Rules
(http://www.w3.org/Submission/SWRL/). However,
since not all the interactions can be inferred
(especially for drug interactions) from the model,
they can also be imported from external data
sources.
Interactions may occur at all the levels of detail
adopted in CIGs. At a high level of detail, usually
actions are composite, thus intention interactions
may occur. On the other hand, going towards lower
levels of detail, pharmaceutical actions prescribe the
administration of drugs (usually drug categories,
from which the physician can choose, depending on
the specific patient conditions) and, at this level,
drug interaction occurs. Thus, in our opinion, a
“black box” system pointing out all the possible
interactions between two CIGs (considering all the
possible levels of detail) would be not practically
useful for physicians, since, in general, it would
return too many interactions. In our previous work
(Piovesan et al. 2014), we have devised a system
that, collaborating with the physician to focus only
on relevant parts of CIGs at the desired level of
detail, helps her/him in the detection of relevant
interactions (see Section 2.3), but we have neglected
the temporal dimension. Modelling time, and
extending the detection interaction system to cope
with the temporal dimension, are the goal of this
paper.
2.3 Non-temporal Interaction Detection
In the approach previously described, we have also
proposed a flexible and interactive detection tool
allowing physicians to navigate through the different
abstraction levels. For instance, at the highest level,
a physician may want to start to consider only the
interactions between the intentions of the “top-level”
actions of the guidelines. Then, focusing on a
specific part of the guideline, (s)he may want to
move down to a more detailed analysis, considering
the decomposition of the composite actions into their
parts, and/or the specific drugs category considered
in order to reach the high-level intentions. In
general, such approach provides physicians with the
possibility of moving in both directions, i.e.,
focusing down from a general to a more specific
analysis, or moving up, from a specific analysis to a
higher level of abstraction. Additionally, the
interaction detection algorithm maintains organized
in a tree data structure (the navigation tree) the
history of the focusing process, supporting both the
addition of new CIG focuses, and the rollback to
upper focuses. Each node of the tree consists of
three main components: two pairs <CIG
1
, focus
1
>,
<CIG
2
,focus
2
> determining the desired level of
abstraction and the focused actions, and an
interaction component, in which, for each pair
TemporalDetectionofGuidelineInteractions
43
<A
i
,A
j
> of actions (A
i
focus
1
, A
j
focus
2
), the
interactions between their intentions (or of the drugs
they administer, in the case of pharmaceutical
actions) are pointed out.
For the sake of brevity and simplicity, with no
loss of generality, in the following we suppose that
just two actions (one in the first CIG and one in the
second CIG) are focused on by the user-physician, at
the chosen level of detail.
3 TEMPORAL
REPRESENTATION
3.1 Temporal Ontology
Coping with time in the interaction detection is of
fundamental importance. Indeed, many of the
entities involved in such a task are characterized by
time, and physicians must consider such information
when they execute more than one CIG.
In particular, actions are characterized by the
time when they occur (or should occur), intentions
are characterized by the time the physician expects
they will be accomplished and effects (of drugs) are
characterized by the time when they should happen.
On the right side of Figure 1,we show how we relate
such temporal information to the previous model. In
particular, we introduce the relation happens, which
relates an action or a variation to the time interval in
which it takes place. A time interval is itself
described by two time points, which represent the
time when the interval starts and ends.
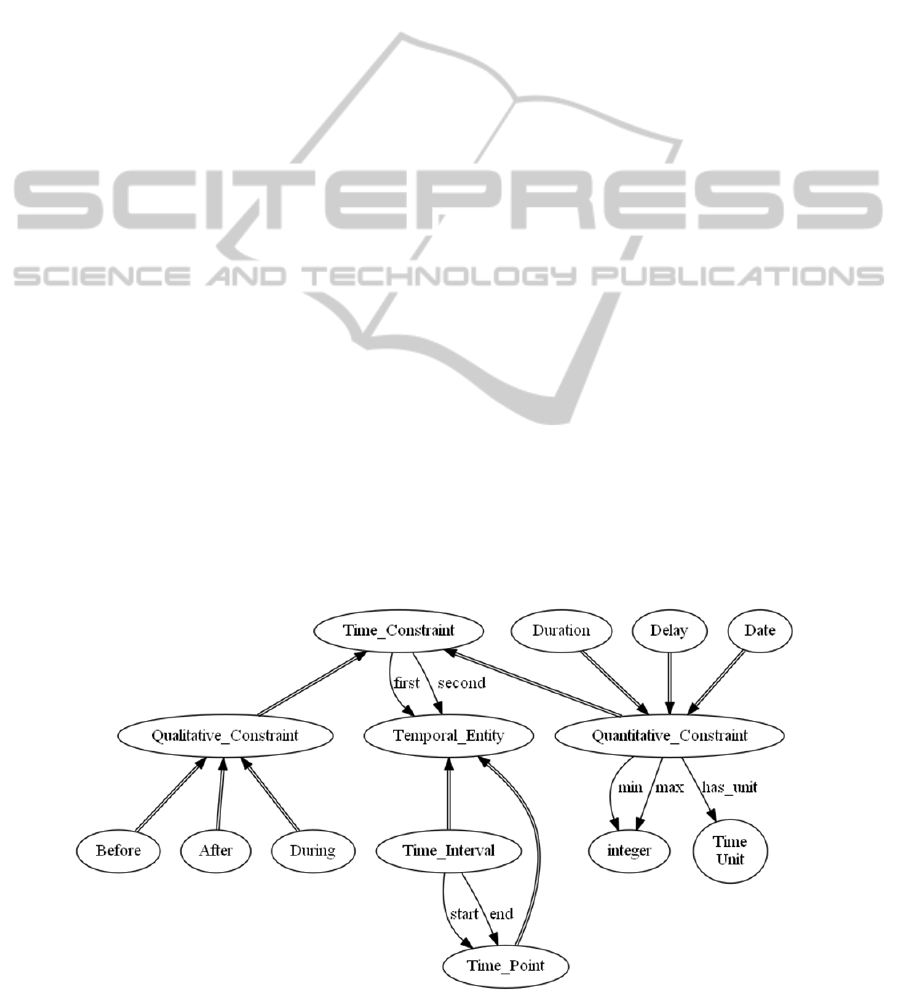
Obviously, the various times are strictly related
to each other (i.e., the time of the effect of a drug
depends on the time of administering such drug). In
order to represent such relations, we detailed in our
model two types of constraints: qualitative (such as,
e.g., before, after, during (Allen 1983; Vilain et al.
1990)) and quantitative ones (such as, e.g., duration,
delay and date). Notice that we support also
imprecise quantitative constraints: for example, if
the exact duration is not known, it is possible to
express a minimum and a maximum duration (see
Figure 2).
3.2 Temporal Constraint
Representation
As discussed in the introduction, to deal with CIG
interactions, three different sources of temporal
constraints must be taken into account. In this
section, we show how they can be represented in our
model.
(1) Knowledge about (i) the delay (with respect to
the action execution/drug administration) and (ii)
the duration of effects (or intentions). In many
cases, such data can be approximately predicted. In
our model, they are represented with two
quantitative constraints: (i) is a delay between the
ending (or, in some cases, the starting) point of the
action and the starting point of the effect (or
intention); (ii) is a duration between the starting and
ending point of the effect (or intention). In our
approach, such knowledge is directly expressed at
the ontological level.
Example 1. Calcium carbonate is a gastric
antacid and it is often prescribed in order to alleviate
the symptoms of gastroesophageal reflux after
meals, when needed. One of its effects is the urine
Figure 2: Temporal constraint ontology.
HEALTHINF2015-InternationalConferenceonHealthInformatics
44
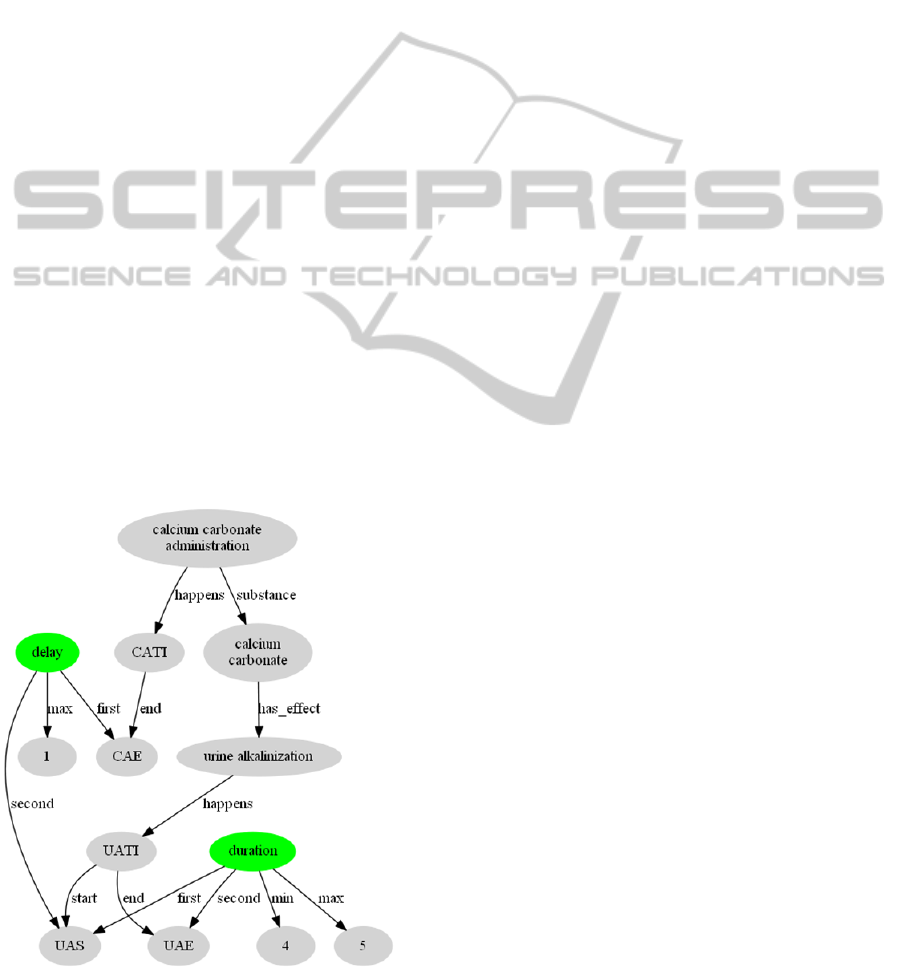
alkalinization (variation, modelled as an increase of
urine pH), which starts at most one hour after the
assumption and lasts 4-5 hours. In Figure 3, we
show how we express temporal constraints between
the calcium carbonate administration, which
happens in a time interval (CATI) of which only the
end (CAE) is relevant for the example, and the urine
alkalinisation, which is characterized by a time
interval (UATI) with a start (UAS) and an end
(UAE) time points. For the sake of clarity, we do not
represent the time unit of hours.
(2) Temporal constraints between actions in the
CIGs: different types of constraints between CIG
actions can be expressed in GLARE. All of them can
be expressed through the model presented in this
paper. In particular, the duration of an action can be
expressed as a possibly imprecise quantitative
constraint between its starting and ending points.
Temporal constraints between two actions can be
represented both through qualitative and quantitative
constraints. Such constraints are directly represented
in the CIG, as described in (Anselma et al. 2006). In
particular, the constraint formalism has been
designed in such a way that only the qualitative
constraints that can be mapped to conjunctions of
STP constraints (Dechter et al. 1991) can be
expressed (see Section 4.2).
(3) Information about the time of execution of
previous CIG actions on the specific patient: such
information are modelled as absolute dates
(expressed as distances from the start of the
Figure 3: Representation of temporal constraints for the
effect "urine alkalinization".
calendar). Also imprecise starting times and ending
times are supported. Obviously, no execution time is
provided in case an “abstract” (i.e., patient-
independent) analysis of the interactions between
CIGs must be performed.
Additionally, for the sake of generality, we also
allow the possibility of expressing any constraint in
the above language (constraints between CIG
actions) also between action execution times.
4 TEMPORAL REASONING
The goal of this work is to provide user-physicians
with a general set of facilities in order to enable
them to look for temporal interactions between
CIGs. In this section, we introduce such facilities,
the constraint propagations techniques we propose
and how the facilities are grounded on the constraint
propagation techniques.
4.1 Facilities
We provide the following facilities, where the user-
physician is enabled to:
1. (Interaction?) check whether two actions in
two different CIGs may interact, certainly
interact or certainly do not interact;
2. (Interaction (what-if)?) assume a hypothetical
execution time for some future actions and
check whether – given such an assumption –
two actions in two different CIGs may interact,
certainly interact or certainly do not interact;
3. (Time of future actions to have (or to avoid) an
interaction?) determine the execution times of
some future actions in order to have or to avoid
some interactions;
4. (Time of future actions to have (or to avoid) an
interaction (what-if)?), as (3), but assuming
some temporal constraints concerning the
execution of future actions.
Notice that the answers may be not crisp, in the
sense that an interaction between two actions can be
temporally necessary, temporally possible or
temporally impossible.
Taking into account the different contexts in which
we support the temporal analysis of interactions (i.e.,
either considering the guidelines with no reference
to specific patients or considering the actual
execution of two CIGs on specific patients) and the
specific temporal assumptions that we can have on
the temporal data of the executions, we singled out
three scenarios. In fact, different scenarios can
induce different types of facilities available to
TemporalDetectionofGuidelineInteractions
45
physicians. The first scenario is the “no temporal
log” scenario, where no temporal information on the
execution of the CIGs is available. This could
happen because either the CIGs have not been
executed yet or no time has been recorded. The
second scenario is the “temporally exact log”, where
the times when the actions of the CIGs have been
executed are known with the precision allowed by
the granularity chosen for the log (e.g., hour or
minute). In this scenario, for example, we assume
that personnel records the exact time (e.g., hour or
minute) of the start and of the end of the executed
actions. The last scenario is the “temporally
imprecise log”, where, because of imprecision in
time measurement or because of lack of information,
the log does not contain the exact start/end time of
the clinical actions but, e.g., a range of time when
the action has started and a range of time when the
action has ended.
In Table 1 we report the facilities available in
each scenario, as detailed below.
4.2 Temporal Reasoning
Our treatment of temporal constraints is grounded on
the STP framework (Dechter et al. 1991). In short, in
STP a set of constraints is modelled as a conjunction
of bounds on differences of the form –
, which have an intuitive temporal interpretation,
namely that the temporal distance between the time
points x and y is between c (minimum distance) and
d (maximum distance). Also strict inequalities are
possible (i.e., <), and – and + can be used to
denote infinite lower and upper bounds respectively.
Temporal reasoning on STP can be
performed/computed by an “all-pairs shortest paths”
algorithm such as the Floyd-Warshall’s one. Such an
algorithm provides as output the minimal network of
the constraints, i.e., the minimum and maximum
distance between each pair of points. A draft version
of Floyd-Warshall’s algorithm is shown below,
where 1, … , denote the time points (e.g.,
starting/ending points of actions), D[i,j] represents
the distance (difference) between i and j, and Min is
the function which provides the minimum between
the two arguments.
For k:=1 to N do
For i:=1 to N do
For j:=1 to N do
D[i,j]=Min(D[i,j],D[i,k]+D[k,j])
Property. Floyd-Warshall’s algorithm operates
in a time cubic in the number of time points, and is
correct and complete on STP (meaning that it
performs all and only the correct inferences while
propagating the STP constraints) (Dechter et al.
1991).
As mentioned above, we have chosen to design
our high-level language for temporal information
in such a way that all the temporal constraints can be
mapped onto the STP framework. In particular, our
temporal constraint language allows one to express
both quantitative constraints such as (i) exact or
imprecise (min/max) dates, (ii) exact or imprecise
durations, (iii) exact or imprecise delays; and
qualitative constraints between time points (e.g., P1
before P2) and/or time intervals (e.g., I1 during I2)
(restricting the language to qualitative constraints
mappable onto STP; see (Brusoni et al. 1997)). In
our approach, such a high-level language is
homogeneously adopted to represent (1) temporal
constraints between actions in the CIGs; (2) exact
dates of actions in the log, or temporal constraints
between them; (3) temporal constraints in the
ontology, and (4) temporal constraints on the
hypothesized actions, if any.
The translation of the constraints of our high-
level language into STP is easy: dates are mapped
Table 1: Facilities for temporal interaction detection and reasoning.
Query
Interaction?
Interaction
(what-if)?
Time of future actions
to have (or to avoid)
an interaction?
Time of future actions
to have (or to avoid) an
interaction (what-if)?
Scenario
No temporal
log
N/A
HYP_TR(O,
G1,G2,Var1,
Var2,Hyp)
TR(O,G1,G2,
Var1,Var2)
HYP_TR(O,G1,G2,
Var1,Var2,Hyp)
Temporally
exact log
TR(O,G1,G2,
Var1,Var2,Log)
HYP_TR(O,
G1,G2,Log,
Var1,Var2,Hyp)
TR(O,G1,G2,
Var1,Var2,Log)
HYP_TR(O,G1,G2,
Var1,Var2,Log,Hyp)
Temporally
imprecise log
TR(O,G1,G2,
Var1,Var2,Log)
?
TR(O,G1,G2,
Var1,Var2,Log)
?
HEALTHINF2015-InternationalConferenceonHealthInformatics
46

into distances with respect to a fixed Reference
Time (e.g., the start time of the calendar), durations
into distances between ending and starting points,
delays into distances between points. Also the
translation of qualitative constraints is easy: just as
an example, I1 during I2 corresponds to the set of
STP constraints 0 1 2
∞, 0 2 1 ∞.
Property. The translation of each constraint in
our high-level temporal language into STP can be
performed in constant time.
In order to provide the temporal facilities in
Table 1, the first step is the collection of (relevant)
constraints from the log (if present), from the CIGs
and from the ontology. In the case of exact temporal
log, each executed action is timestamped with its
starting and ending time (which are exact dates); in
the case of temporally imprecise log, the log
explicitly contains temporal constraints between the
executed actions. In both cases, temporal constraints
are simply collected by inspecting the log. The
collection of constraints from the CIGs involves the
navigation of the CIGs (expressed in GLARE) from
the starting action A
s
to the focused action A
f
, and
the collection of the constraints on the arc in the path
connecting them. In case multiple alternative paths
are present, each one of the paths must be
considered independently of the others (in the rest of
the discussion, for the sake of simplicity, we assume
that only one path is considered). Additionally, in
case composite actions are present in the path, also
the constraint that the temporal extent of a
composite action contains the extents of its
components must be considered. Finally, the
ontology can be easily navigated in order to retrieve
the temporal constraints between the focused actions
and their focused effects. Different types of arcs in
the ontology have to be navigated, depending on the
types of the focused action. Figure 3 shows the case
of pharmacological prescriptions (calcium carbonate
administration in the example). The happens and
end (or start) arcs connect actions with the ending
(starting) point of the time when they occur (e.g.,
CAE in Figure 3). The substance arc connects
pharmacological actions to the drug they prescribe,
and the has_effect arc points out the effect
(variation) caused by such a drug. In turn, happens
and start/end arcs relate effects to their
starting/ending times (e.g., UAS, UAE in Figure 3).
Temporal constraints between such endpoints (e.g.,
the delay between CAE and UAS) can then finally be
retrieved.
After the collection of constraints (from log,
CIGs and ontology) is performed, and all constraints
are translated onto STP constraints, temporal
reasoning can be performed, to offer the above
facilities to user-physicians.
To provide the different facilities shown in Table
1 we rely on two basic algorithms that propagate the
temporal constraints: TR, which performs temporal
reasoning, i.e., it checks for consistency and
evaluates the minimal network using Floyd
Warshall’s algorithm, and HYP_TR, which performs
temporal reasoning assuming some hypothetical
temporal information. The parameters O, G1, G2,
Var1, Var2, Log, Hyp in the table represent the
ontology, the two CIGs, the two interacting
variations to be examined, the log and the
hypothetical temporal constraints, respectively.
Now we discuss how the different types of log
(log with no temporal information, with exact times,
and with imprecise temporal information) affect the
facilities.
When no information is available on the
execution of the CIGs (“no log”, first row of the
table), all relative temporal relations between the
two CIGs are possible. Therefore, in order to infer
any meaningful conclusion on the interactions, it is
necessary to anchor a CIG to the other, otherwise
the query cannot be answered (N/A in the table).
Such anchoring can be made in two ways in the “no
log” scenario: by devising an interaction between the
two CIGs (in Time of future actions to have (or to
avoid) an interaction?) or by assuming some
temporal relations between the two CIGs in the
facilities that contemplate hypothetical temporal
constraints.
When precise temporal information is available
on the execution of the CIGs (“temporally precise
log”, second row of the table), all types of queries
can be answered. Since we know the exact time
when the actions have been performed, it is possible
to check whether they interact in time. Notice that
temporal reasoning is required also in this case: in
fact, the time of “future” actions, i.e., the time of
actions in the CIGs not yet performed, is not exactly
known. Therefore, the temporal constraints in the
CIGs, along with the temporal constraints from the
logs, have to be propagated.
When temporal information on the execution of
the CIGs is available but it is imprecise (“temporally
imprecise log”, third row of the table), it is important
noting that hypothetical queries may have some
undesired side effect. In fact, in hypothetical queries,
where some hypothetical temporal constraints are
added to the known temporal information, the
propagation of such new temporal information could
cause a tightening of some imprecise log constraints.
TemporalDetectionofGuidelineInteractions
47

In this case, such constraints could take only some
of the possible values that make the hypothetical
query consistent. However, these constraints are not
“controllable”, in the sense that they represent
imprecision in the measurement of the time and it is
not possible for the user to choose a specific time
value. Treating this case is an open problem and it is
left as a future work.
For the sake of brevity, we illustrate in more
detail only the facility Hypothetical Interaction? in
the “temporally exact log” scenario (see Algorithm
1). After extracting the temporal constraints from the
CIGs, from the logs and from the ontology in a STP,
the hypothetical temporal constraints are
provisionally added to the STP. Then the constraints
are propagated and the resulting minimal network is
used to answer the query. Such minimal network, in
fact, contains the strictest inferred constraints
between the two variations under consideration.
Thus, by examining the inferred temporal difference
between the starting and ending points of variations
Var1 and Var2, we can determine whether their
overlap is certain, possible or it is certain that there
is no overlap.
As regards the evaluation of the algorithm, its
computational complexity is dominated by
HYP_TR, which operates in time cubic in the
number of (i) the actions considered in the two CIGs
plus (ii) the actions in the log plus (iii) the
hypothesized actions.
Example 2. We consider the case where a
patient suffering from gastroesophageal reflux
treated with calcium carbonate (see Example 1)
contracts a urinary tract infection and, thus, the two
pertaining CIGs have to be executed at the same
time on this patient. In particular, the urinary tract
infection is treated with nalidixic acid, which starts
its “absorption of nalidixic acid” effect (modelled as
an increase of nalidixic acid blood level) in at most
Hypothetical Interaction?(O, G1, G2,
Var1, Var2, Hyp)
Extract temporal constraints
HYP_TR on temporal constraints given
hypothesis Hyp
Given minimal network:
If there is necessarily an overlap
between variation Var1 and variation
Var2 then return YES
Else If variation Var1 necessarily
does not temporally overlap
variation Var2 then return NO
Else return MAYBE
Algorithm 1: Algorithm for detecting temporal interaction
assuming some temporal constraints.
one hour after the assumption and lasts 4 hours. We
consider the case where the physician wants to know
if the administration of nalidixic acid will interact
with the assumption of calcium carbonate. The
physician decides to focus in the CIGs on the
pharmaceutical actions of administration of the two
drugs. We assume that the patient takes the calcium
carbonate after each meal (say lunch at 1 pm and
dinner at 8 pm). The physician decides to perform a
“what-if” analysis of interaction and to explore the
consequences of administering the nalidixic acid at 3
pm and (s)he asks to the system if the two focused
actions interact. First, a non-temporal interaction is
extracted from the ontology between the two drugs,
caused by a variation interaction between the “urine
alkalinization” and the “absorption of nalidixic acid”
effects, with has_modality “decreasing” of the
“absorption of nalidixic acid” effect. Then, in order
to decide if the two actions temporally interact, the
facility Hypothetical Interaction is used, with
parameters the ontology, the two CIGs, the two
interacting variations “urine alkalinization” and
“absorption of nalidixic acid”, and the hypothesis of
administration of nalidixic acid at 3 pm. The
propagation of the temporal constraints allows the
physician to discover that the calcium carbonate has
effect surely between 2 pm and 5 pm and that the
temporal intervals of effect of the two interacting
drugs surely overlap at least from 4 pm to 5 pm.
Thus, the facility returns YES. Because of this
result, in order to avoid the interaction, the physician
can decide to change one of the two drugs or the
time of administration of the antibiotic, repeating the
focusing and detection process.
5 RELATED WORKS AND
CONCLUSIONS
The treatment of comorbid patients is one of the
main challenges for the modern healthcare. This is a
hot topic in Medical Informatics, too, and several
approaches are recently emerging.
The approach in (Michalowski et al. 2013) and
(Wilk et al. 2013) uses constraint logic programming
to identify and address adverse interactions. In this
solution, a constraint logic programming (CLP)
model is derived from the combination of logical
models that represent each CIG, then a mitigation
algorithm is applied to detect and mitigate
interactions. On the other hand, Sánchez-Garzón et
al. (Sánchez-Garzón et al. 2013) propose an agent-
based approach to guideline merging. Each guideline
HEALTHINF2015-InternationalConferenceonHealthInformatics
48

is considered as a physician expert in the treatment
of a single disease, and is represented by an agent
with hierarchical planning capabilities. The result is
obtained through the coordination of all the agents,
and respects the recommendations of each guideline.
Riaño et al. represent guidelines as sets of
clinical actions that are modelled into an ontology
(López-Vallverdú et al. 2013). To combine two
treatments, first they are unified in a unique
treatment and then a set of “combination rules” is
applied to detect and avoid possible interactions. A
model-based automatic merge of CIGs is then
purposed in (Riaño and Collado 2013), through the
definition of a combining operator. Jafarpour and
Abidi (Jafarpour and Abidi 2013) use semantic-web
rules and an ontology for the merging criteria. Given
these, an Execution Engine dynamically merges
several CIGs according to merge criteria. GLINDA
proposes a wide ontology of cross-guideline
interactions (http://glinda-project.stanford.edu/guide
lineinteractionontology.html). We recently proposed
an original approach, supporting user-driven and
interactive interaction detection over different levels
of abstractions (Piovesan et al. 2014).
However, although interactions can only occur in
time, to the best of our knowledge no previous
approach to the treatment of interactions (and
comorbidities) has already provided facilities to
address the temporal dimension. This is the goal of
the approach in this paper, in which we proposed a
general approach, suitable in different situations
(e.g., either in case a specific comorbid patient is
considered, or in case “abstract” possible
interactions between CIGs are taken into account),
and providing a wide range of facilities to user-
physicians.
Temporal issues are pervasive in the CIG context
and many previous approaches have faced some of
them (see, e.g., the survey in (Terenziani et al.
2008)). In particular, in the Asbru (Shahar et al.
1998) and in the GLARE (Anselma et al. 2006)
projects, rich representation formalisms have been
proposed to cope with temporal constraints in the
CIGs, and in GLARE correct and complete temporal
constraint propagation algorithms have been
proposed to reason with them and to merge them
with the time of execution of actions on specific
patients (Anselma et al. 2006). However, to the best
of our knowledge, no other approach to CIGs has
explicitly addressed the treatment of time and
temporal constraints for the detection of CIG
interactions. In this sense, we believe that our
approach, besides being innovative, is somehow
complementary with respect to several other
approaches in the literature, so that an integration
with them can be devised as a future work (e.g., with
Riaño’s methodology to merge CIGs (Riaño and
Collado 2013)).
We are currently developing a prototypical
implementation to demonstrate our approach, based
on GLARE. In our short-term future work, we aim at
extending our approach to cope also with cases not
covered in Table 1. In our long-term future work, we
will attempt to support physicians also in the
interaction solving, and, finally, in merging multiple
guidelines in the treatment of a specific patient.
ACKNOWLEDGEMENTS
The work described in paper was partially supported
by Compagnia di San Paolo, in the Ginseng project.
REFERENCES
Allen, J.F., 1983. Maintaining knowledge about temporal
intervals. Communications of the ACM, 26(11),
pp.832–843.
Anselma, L. et al., 2006. Towards a comprehensive
treatment of repetitions, periodicity and temporal
constraints in clinical guidelines. Artificial Intelligence
in Medicine, 38(2), pp.171–195.
Brusoni, V. et al., 1997. Later: managing temporal
information efficiently. IEEE Expert, 12(4), pp.56–64.
Dechter, R., Meiri, I. and Pearl, J., 1991. Temporal
Constraint Networks. Artif. Intell., 49(1-3), pp.61–95.
Fridsma, D.B., 2001. Special Issue on Workflow
Management and Clinical Guidelines. Journal of the
American Medical Informatics Association, 22(1).
Gordon, C. and Christensen, J.P. eds., 1995. Health
telematics for clinical guidelines and protocols,
Amsterdam, Netherlands: IOS Press.
Horvitz, E., 1999. Uncertainty, Action, and Interaction: In
Pursuit of Mixed-Initiative Computing. IEEE
Intelligent Systems, 14(5), pp.17–20.
Jafarpour, B. and Abidi, S.S.R., 2013. Merging Disease-
Specific Clinical Guidelines to Handle Comorbidities
in a Clinical Decision Support Setting. In AIME. pp.
28–32.
López-Vallverdú, J.A., Riaño, D. and Collado, A., 2013.
Rule-Based Combination of Comorbid Treatments for
Chronic Diseases Applied to Hypertension, Diabetes
Mellitus and Heart Failure. In R. Lenz et al., eds.
Process Support and Knowledge Representation in
Health Care. Lecture Notes in Computer Science.
Springer Berlin Heidelberg, pp. 30–41.
Michalowski, M. et al., 2013. Using Constraint Logic
Programming to Implement Iterative Actions and
Numerical Measures during Mitigation of
Concurrently Applied Clinical Practice Guidelines. In
TemporalDetectionofGuidelineInteractions
49

N. Peek, R. M. Morales, and M. Peleg, eds. Artificial
Intelligence in Medicine. Lecture Notes in Computer
Science. Springer Berlin Heidelberg, pp. 17–22.
Peleg, M., 2013. Computer-interpretable clinical
guidelines: A methodological review. Journal of
Biomedical Informatics, 46(4), pp.744–763.
Piovesan, L., Molino, G. and Terenziani, P., 2014. An
ontological knowledge and multiple abstraction level
decision support system in healthcare. Decision
Analytics, 1(1).
Riaño, D. and Collado, A., 2013. Model-Based
Combination of Treatments for the Management of
Chronic Comorbid Patients. In Artificial Intelligence
in Medicine. 14th Conference on Artificial Intelligence
in Medicine. Springer, pp. 11–16.
Sánchez-Garzón, I. et al., 2013. A Multi-agent Planning
Approach for the Generation of Personalized
Treatment Plans of Comorbid Patients. In AIME. pp.
23–27.
Shahar, Y., Miksch, S. and Johnson, P., 1998. The
Asgaard project: a task-specific framework for the
application and critiquing of time-oriented clinical
guidelines. Artificial Intelligence in Medicine, 14(1-2),
pp.29–51.
Ten Teije, A., Miksch, S. and Lucas, P. eds., 2008.
Computer-based medical guidelines and protocols: a
primer and current trends, Amsterdam, Netherlands:
IOS Press.
Terenziani, P., German, E. and Shahar, Y., 2008. The
temporal aspects of clinical guidelines. Studies in
Health Technology and Informatics, 139, pp.81–100.
Vilain, M., Kautz, H. and van Beek, P., 1990. Constraint
propagation algorithms for temporal reasoning: a
revised report. In D. S. Weld and J. de Kleer, eds.
Readings in Qualitative Reasoning About Physical
Systems. San Francisco, CA, USA: Morgan Kaufmann
Publishers Inc., pp. 373–381.
Wilk, S. et al., 2013. Mitigation of adverse interactions in
pairs of clinical practice guidelines using constraint
logic programming. Journal of biomedical
informatics, 46(2), pp.341–353.
HEALTHINF2015-InternationalConferenceonHealthInformatics
50
