
Platform to Support the Development of Information Services
for Informal and Formal Care
Carlos Cardoso
1
, Yosvany Llerena Rodriguez
2
, Miguel Grade
1
, Filipe Augusto
1
, Alexandra Queirós
3
,
João Quintas
4
and Nelson Pacheco Rocha
5
1
Maisis, Rua D. Manuel B. Vasconcelos, Aveiro, Portugal
2
Instituto de Engenharia Electrónica e Telemática de Aveiro, University of Aveiro,
Campo Universitário de Santiago, Aveiro, Portugal
3
Health Sciences School, Instituto de Engenharia Electrónica e Telemática de Aveiro, University of Aveiro,
Campo Universitário de Santiago, Aveiro, Portugal
4
Instituto Pedro Nunes, Rua Pedro Nunes, Coimbra, Portugal
5
Health Sciences Department, Instituto de Engenharia Electrónica e Telemática de Aveiro, University of Aveiro,
Campo Universitário de Santiago, Aveiro, Portugal
Keywords: Integrated Care, eHealth, Electronic Health Record, Personal Health Record, Social Health Record, Services
Oriented Architecture.
Abstract: This paper presents a platform to support the development of services and applications for informal and
formal care, which is based on the principles of the Services Oriented Architecture. In particular, the paper
presents the mechanisms that allow the developers a significant freedom to implement and use new types of
information objects.
1 INTRODUCTION
Due to the ageing population and the inherent shift
in the burden of illness from acute to chronic
conditions, there is a generation of people living
with long term illness and disability and,
consequently, a substantial increase of the health
costs. Therefore, significant organizational changes
of the care away from medical institutions are
required, which means the urgency for the
consolidation of new practices that can contribute to
increase efficiency and, consequently, to decrease
costs.
As a consequence of major structural changes of
the contemporary society, particularly in terms of
structure and size of the families, there are a
considerable number of elderly people living alone.
Thus, the interventions should not be exclusively
focused on medical needs, but also in maintaining
the autonomy and independence of the individuals
(Santana et al., 2007) by supporting a set of
activities that are normal for every citizen, such as
home activities, mobility, recreation or safety, and
also social participation.
Significantly, the ageing population coincides
with the technological revolution of the last decades,
which is redefining how people work, communicate
and relate to each other and that should contribute
both to effectiveness and efficiency of the healthcare
and social care systems. In this respect, the ehealth
(Eysenbach, 2001) paradigm is essential.
One of the objectives of the TICE.Healthy
project, which integrates diverse Portuguese
academic and industrial partners, is to answer to
some of the identified needs by providing a
platform, the We.Can platform, supporting
applications in the health and quality of life
domains.
In this paper, we present some features of the
We.Can platform, based on the principles of the
Services Oriented Architecture (SOA). This
platform intends to complement the existing clinical
communication networks. Its main requirement is
the support of informal and formal care providers,
outside the hospitals wards, that, nowadays, do not
have access to services providing structured
information related with their clients.
417
Cardoso C., Llerena Rodriguez Y., Grade M., Augusto F., Queirós A., Quintas J. and Pacheco Rocha N..
Platform to Support the Development of Information Services for Informal and Formal Care.
DOI: 10.5220/0004903304170421
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2014), pages 417-421
ISBN: 978-989-758-010-9
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)

The paper is composed by this section
(Introduction) and three more sections: Related
Work, Architecture, Services and Conclusion.
2 RELATED WORK
Health Care Networks (HCN) (Katehakis et al.,
2006) are used for the integration and sharing of
distributed clinical information. Most HCN in
Europe are typically regional, although some
national solutions also exist. The implementation of
these networks requires the solution of a broad range
of technical and non-technical issues, such as user’s
identification, security, privacy, governance and
financial support for common operations.
The sharing of clinical information requires, in
addition to the communication infrastructure, the
existence of interoperable Electronic Health Records
(EHR). This interoperability can contribute to a
more effective and efficient care, facilitating the
transfer of information and knowledge between
different entities.
For that several standards (e.g. Reference
Information Model - RIM - or Clinical Document
Architecture - CDA) are being developed by the
Health Level Seven (HL7) organization, part of the
American National Standard Institution and founded
in 1987, while the European Committee for
Standardization - Technical Committee 251
(CEN/TC 251) is being defining the EHRcom whose
overall goal is to provide a rigorous and stable
information architecture for communicating part or
all of the EHR information of a patient.
However, despite all the advances in systems
interconnection and interoperability protocols,
semantic heterogeneity of information remains a
difficult problem to solve. This interoperability is
still more difficult knowing that health conditions
are influenced by the individual's medical history
and other factors, including behavioural, social and
environmental factors (Glass &. McAtee, 2006).
Thus, we need to consider new requirements in
terms of distributed management, integration and
use of a whole range of information, such as those
related to Personal Health Records (PHR),
Electronic Social Records (ESR) and Ambient and
Assisted Living (AAL) generated information
(Queirós et al., 2013).
PHR include data and information related with
the individuals’ lifetime and the individuals’ care
maintain by themselves, namely patient-reported
outcomes (Bos, 2012).
ESR are composed by forms (e.g. nationally used
forms or local assessment forms), coded data
(mainly for management and statistical reporting
purposes) or unstructured information such as
letters, emails or notes of meetings (SCDH, 2004).
Finally, recent developments related with AAL
and the consolidation of standards such as the
ISO/IEEE 11073 for the interconnection and
interoperability of medical devices, have brought
new possibilities in terms of new services (Teixeira
et al., 2009; Teixeira et al., 2011) and automatic
collection of information about individuals and
environment. Sensory data are captured by sensors
embedded in the environment and can be used for
systems automation or to monitor chronic diseases
among other applications.
Considering this complex reality, there is the
need to develop innovative solutions to persist all
the required information, such as the We.Can
platform.
3 ARCHITECTURE
Although one of the main requirements of the
We.Can platform is the information persistence, its
architecture should not only provide the necessary
services for information persistence, but also other
services supporting applications such as: i) audit
services responsible for verifying all interactions
conducted among services and end users; ii)
authentication services to provide access to the
information only to authorized services or end users;
iii) encryption services to enable secure
communications of sensitive information (Hafner,
2009); iv) concepts and terminology services to
assist the processes of data codification, data
translation into formats easily understood by humans
or data indexing and inference, and to determine the
structure and meaning of some data; and v) users
identification services, enabling a unique identifier
information distributed across multiple entities and
systems.
To consolidate the We.Can architecture it was
necessary to consider a comprehensive set of
problems, namely the heterogeneity of potential end-
users and, consequently, the challenges in terms of
usability, the difficulty of ensuring a safe and
efficient access to different types of information and
ultimately, the capture and management of new
information types related with knowledge not
properly structured, and for which the platform must
ensure that its meaning is transversal (i.e. their
meanings must be the same, regardless the involved
actors and the future evolutions).
HEALTHINF2014-InternationalConferenceonHealthInformatics
418
Ideally, the architecture should allow the
integration of software components from different
sources. The SOA approach is a good solution to
ensure technological neutrality, namely because it
can encapsulate components developed in other
technologies. Furthermore, this paradigm allows
business processes to be responsive with a high
degree of flexibility and adaptability, namely
(Crawford et al., 2005): i) the development of new
services from the aggregation of components that
can be built on different systems, running different
operating systems, and build in different
programming languages; ii) consistency of the
infrastructure development and deployment; iii)
reduction of the design, development, testing, and
deployment time due to the reuse of existing
services and components; iv) reduction of the
development costs and the risk of introducing new
errors, and thus potential points of failure, through
the process of enhancing or creating new business
services; v) continuous business process
improvement, since the developers are allowed to
change process flows while monitoring the resulting
effects; and vi) user-configurable solutions.
The formal consistency of the information is the
responsibility of the persistence mechanisms. Those
mechanisms also ensure that the information
requirements of individual applications are met
through the evocation of standardized primitives.
The customization of the applications to specific
requirements of the application domain requires
substantial code modifications. To obviate this
difficulty there is the modelling at two levels
approach (i.e. knowledge and information models),
which has been considerably developed by the
openEHR promoters (Schloeffel, 2003).
The Archetypes and the respective constraint
rules domain constitute the knowledge model that is
used to adapt the underlying information technical
specifications.
The knowledge model considers that there is
contextual information that should always be
recorded and there is information that will vary
according to clients, events and service providers.
Therefore, it exist different types of Archetypes that
are part of the basic care process. A generalization
of base Archetypes was performed in order to
systematize the overall information that can be
considered essential.
An Archetype is a pre-defined structure which
organizes information facilitates the creation of
appropriate forms for data input and queries. The
basic structure of any Archetype consists of a
header, a body and data. The header contains
information such as the type, name, author and
header details, which, in turn, comprise several
attributes.
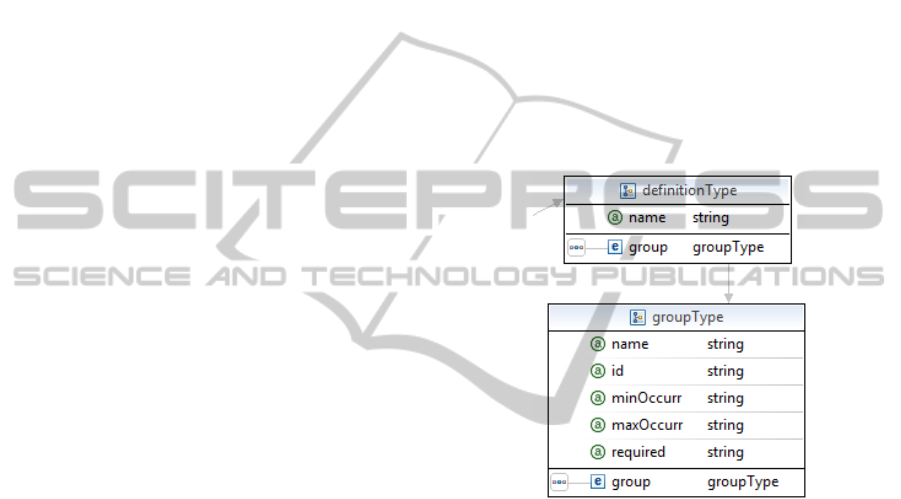
The body of the Archetype (Figure 1) is a
dynamically modelled component and contains three
main fields: participations (i.e. contextual
information), description (i.e. the elements that
compose the body) and definition. Definition is used
to specify one or more groups of information. Each
group has a name, an id, the minimum and
maximum number of occurrences, and if it is
mandatory. The data field is structured to support the
information groups specified by the aforementioned
body definition field. It comprises a group which can
be subdivided into collections and elements. In turn,
collections may contain elements or other
collections.
Figure 1: Structure of the Archetype body.
To guarantee the flexibility of the Archetypes and to
ensure the persistence of the information together
with the respective semantics there is the need of
robust information models. Therefore, the data
repository (i.e. the information model) was
implemented accordingly to HL7 RIM (ISO/HL7
21731, 2006).
4 SERVICES
The information persistence service, based on the
RIM implementation provides a simplified access to
the platform databases. In order to offer a high
abstraction level, the create, read and update
operations to access the relational databases that
support the implementation of the RIM container
allow the manipulation of objects and, therefore,
provide enough abstraction to the services that use
them. Since the deletion of previously persisted
PlatformtoSupporttheDevelopmentofInformationServicesforInformalandFormalCare
419

information is not allowed, the delete operation was
not implemented. This is one of the fundamental
rules that must not be violated in order to ensure
coherence and consistency of the stored information.
Queries are important features to bear for any
information system. This importance becomes even
more critical when the volume, complexity and
variability of the stored data increase.
Considering the Archetypes modelling approach
and the variability of the Archetypes structure
becomes critical the existence of specific search
syntax sufficiently flexible to answer the needs of
the final information consumers (i.e. applications).
Therefore, we propose a domain specific language
with adequate syntax to formalize flexible queries.
A search is formalized through a Search
operation that contains a Query or a Filter
mechanism.
The Query mechanism is prepared to be used
when searching free text fields, which is extremely
useful for research in fields with long text, or when
the result should be sorted by relevance. On the
other hand, it is recommended to use the Filter
operations in binary searches (i.e. searches that
return yes or no results), exact value searches (i.e.
filtering by a certain value) and recurrent searches
that need to be optimized by caching mechanisms.
The formalization of a Filter or a Query search
can be refined with additional criteria including
different types of operators (e.g. Boolean, exact,
range or fuzzy).
Archetypes are complex structures and,
therefore, the platform provides dedicated services
to create and edit them. Furthermore, the support
services provide search functions for the selection,
within the existing Archetypes, the one that must be
edited, and the required operations to manage the
information introduced by the application domain
experts and to manage the different Archetypes
versions.
The developed support services use the LiU
Archetype Editor of the openEHR framework, which
has been complemented by a parser able to adjust to
RIM.
The Archetypes processed by the parser can be
included in an Archetypes repository. This is an
application that allows all the required Archetypes
operations, namely, searching and publishing,
authentication, versioning and ownership
management.
Once the applications that can be supported by
the platform We.Can necessarily have a broad range
of requirements in terms of user interfaces and that
these interfaces must evolve over time with the help
of domain experts and the end users themselves, it is
important to have a support development services
based on the Archetypes formulations for the
extension of the presentation features.
The presentation service provides a generic
interface to create, access, modify and delete records
based on existing Archetypes without the need to
change the persistence layer. The selected
development environment was the Play Framework,
which is a web framework based in Java and the
configurations of generic entities are stored in
JSON.
The created custom fields are dynamic so that
they can be modified at runtime. Depending on the
predefined configurations there is a code generation
component that is able to create a visual
representation of the Archetype contents and
implement the business rules that govern them.
Among the features provided by the module it
should be pointed the following: i) abstraction of
data access and business rules; ii) customization of
fields and web components (e.g. data type,
maximum size or validation constrains); iii)
automatic update of the template whenever there is a
definition of new components; iv) automatic
generation of custom forms for viewing, entering
and editing data; and v) versioning management.
There are four types of views that can be
configured, namely: i) insertion view; ii) edit view;
iii) presentation view (i.e. a view to present data
from a register); and iv) data list view.
In order to allow having presentation services
truly flexible and extensible independently of the
application environment it is necessary to provide a
mechanism to define and modify business rules of
the final application.
The most common validations are pre-
programmed accordingly to rules based on the
Archetypes definition. Additionally, there is the
possibility to validate one or more fields of a
presentation entity in a different way that the one
initially foreseen. For example, if we had two date
type fields whose validation rules include the
requirement that the content of the field should be
posterior to the first one, and this had not been
planned, it should be possible to add a rule to
validate this condition. Beyond this basic case there
are many others cases that may rely on the rules
engine to allow the application modification without
recompilation and deployment costs
A rules engine helps to reduce the problems and
difficulties inherent to the development and
maintenance of the business logic of an application
(e.g. the recompilation and deployment costs).
HEALTHINF2014-InternationalConferenceonHealthInformatics
420

5 CONCLUSIONS
Through the use of different application scenarios it
was possible to verify that the RIM based
information container is able to support a wide range
of information structures. Furthermore, the formal
structure of the Archetype was proven to be useful
for the development of the user interactions
mechanisms. In particular, the validation process
demonstrated that user interfaces can be automatic
generated from the Archetypes structure.
Currently, a full version of the platform is being
prepared to be evaluated in real conditions,
supporting different services and applications related
with health and quality of life domains.
ACKNOWLEDGEMENTS
This work was supported by COMPETE - Sistema
de Incentivos à Investigação e Desenvolvimento
Tecnológico, Projectos de I&DT Empresas em co-
promoção, under QREN TICE.Healthy.
REFERENCES
Beale T., 2002. Archetypes: Constraint-Based Domain
Models for Future-Proof Information Systems. 11th
OOPSLA Workshop on Behavioral Semantics: Serving
the Customer, 16-32, Boston.
Bos, L., 2012. pHealth. Proceedings of the 9th
International Conference on Wearable Micro and
Nano Technologies for Personalized Health, Porto,
Portugal.
Crawford, C., Bate, G., Cherbakov, L., Holley, K., &
Tsocanos, C., 2005. Toward an on Demand Service-
Oriented Architecture. IBM Systems Journal, 44(1).
Eysenbach, G., 2001. What is e.health? Journal of
Medical Internet Research, 3 (2).
Glass, T., &. McAtee, M., 2006. Behavioral Science at the
Crossroads in Public Health: Extending Horizons,
Envisioning the Future. Social Science & Medicine,
62(7), 1650 - 1671.
Hafner, M., Memon, M., & Breu, R., 2009. SeAAS - A
Reference Architecture for Security Services in SOA.
Journal of Universal Computer Science, 15(15), 2916-
2936.
ISO/HL7 21731, 2006. Health informatics - HL7 version 3
- Reference Information Model - release 1. Geneva:
International Organization for Standardization.
Katehakis, D., Sfakianakis, S., Kavlentakis, G.,
Anthoulakis, D., & Tsiknakis, M., 2006. Delivering a
Lifelong Integrated Electronic Health Record Based
on a Service Oriented Architecture. IEEE
Transactions on Information Technology in
Biomedicine, 11 (6), 639-650.
Queirós, A., Carvalho, S., Pavão, J., & Rocha, N., 2013.
AAL Information Based Services and Care
Integration. Proceedings HealthInf 2013, 403-406.
SCDH, 2004. Defining the Electronic Social Care Record.
London: Information Policy Unit - Social Care
Department of Health.
Schloeffel, P., 2003. openEHR Archetypes: Putting the
Clinician Back in the Driver's Seat. Proceedings of the
Health Informatics Conference, Sydney.
Santana, S., Dias, A., Souza, E., & Rocha, N., 2007. The
Domiciliary Support Service in Portugal and the
Change of Paradigm in Care Provision. International
Journal of Integrated Care, 7.
Teixeira, A., Braga, D., Coelho, L., Fonseca, J.,
Alvarelhão, J., Martín, I., Queirós, A., Rocha, N.,
Calado, A. & Dias, M. 2009. Speech as the Basic
Interface for Assistive Technology. DSAI 2009 -
Proceedings of the 2th International Conference on
Software Development for Enhancing Accessibility
and Fighting Info-Exclusion.
Teixeira, A.
et al., 2011. A New Living Lab for Usability
Evaluation of ICT and Next Generation Networks for
Elderly@Home. AAL 2011 - 1st Int. Living Usability
Lab Workshop on AAL Latest Solutions, Trends and
Applications.
PlatformtoSupporttheDevelopmentofInformationServicesforInformalandFormalCare
421
