
Using Healthcare Planning Features to Drive Scientific Workflows
on the Web
Bruno S. C. M. Vilar, Andr
´
e Santanch
`
e and Claudia Bauzer Medeiros
IC - UNICAMP, 13083-852, Campinas, SP, Brazil
Keywords:
Scientific Workflows, Context-Adaptation, Task-Network Model, Healthcare.
Abstract:
Automated healthcare planning (care-flow) systems are usually designed to afford the dynamicity of health
environments, in which changes occur constantly as a patient’s treatment progresses. This dynamic adaptation
mechanism is based on blocks of activities, triggered and combined according to contextual data, producing a
plan, which emerges from the interaction between these blocks and the context. However, tools that implement
care-flow systems are still incipient, missing support for features like extensibility, collaboration and traceabil-
ity of procedures. On the other hand, these features can be found in workflow systems that are widely used in
a variety of environments (in business and scientific domains), with consolidated standards and technologies.
However, workflow systems are not well suited to address the dynamicity of healthcare environments. In this
paper we argue that care-flow and workflow systems have complementary characteristics and we present a
software architecture that incorporates the emergent and context-driven approach of care-flow systems into
workflow systems. We present a prototypical implementation validating the key concepts of our proposal,
which uses an ontology representation of workflows combined with an ontology and SWRL rules.
1 INTRODUCTION
The growth in the number of patients of a hospital
brings the challenge of managing appointments, ad-
missions and surgical interventions. There is the need
to increase the efficiency and flexibility to manage as-
sociated data. The use of computational resources to
address this challenge implies on more technical re-
quirements. The possibility of using data available on
the Web has added a new dimension to this problem,
with additional heterogeneity factors.
Some researchers (Unertl et al., 2009), in the con-
text of chronic disease care, identified requirements
that should be fulfilled by systems to be applied to the
health domain, among which we single out: (i) Sup-
port for the shared needs and behaviors in care; (ii)
Allow customization for disease-specific needs and to
support the needs of different types of users; (iii) Ex-
plore new approaches for information input into the
EHR (Electronic Health Record) as well as transfer,
efficiently, data from medical devices into them.
Care-flow is at the core of healthcare manage-
ment, involving directly or indirectly the requirements
presented by (Unertl et al., 2009). As a consequence,
one natural approach to start to deal with the prob-
lem has been to use Computer-Interpretable Guide-
lines (CIGs). Informally, a CIG is a specification in
some kind of computer interpretable language that de-
fines the flow of steps to be taken in each situation
met by a health professional. Those guidelines man-
age the care-flow, customize needs and details for pa-
tient treatment and deal with data gathered, clinical
guidelines, while preserves the rationale of healthcare
professionals. Though CIGs are suitable for guiding
the care-flow, from the perspective of the planning of
the paths chosen, the tools that implement a CIG ap-
proach are still incipient, missing support to extensi-
bility, reuse and share of content, collaboration among
professionals and traceability.
Even though it is possible to define guidelines for
“blocks of actions”, the whole process involved in the
healthcare of a given patient is driven by the context,
which is captured during the process itself. In a typ-
ical scenario, data from given care-flow step will de-
fine the next steps to be followed. The flow of ac-
tions emerge from the interaction between available
blocks and the context. Therefore, one of the most
successful approaches for CIG is the Task-Network
Model (TNM) (Peleg et al., 2003), which mimics this
context-driven evolution. The process starts by a seed
block of actions, which is unfolded according to con-
text data collected during its execution.
49
Vilar B., Santanchè A. and Medeiros C..
Using Healthcare Planning Features to Drive Scientific Workflows on the Web.
DOI: 10.5220/0004844500490056
In Proceedings of the 10th International Conference on Web Information Systems and Technologies (WEBIST-2014), pages 49-56
ISBN: 978-989-758-024-6
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)
Scientific workflows, on the other hand, are con-
cerned with the planning and flow of tasks, but associ-
ated to scientific experiments and general tasks. They
have been developed for years and tested on areas
such as Astronomy, Biology, Gravitational Physics
and Earthquake Science (Bharathi et al., 2008). As
a result, those tools have consolidated mechanisms to
deal with large amounts of data, collaboration, exten-
sibility of their resources, and association with exter-
nal sources of data, tools and algorithms. In general,
Scientific Workflow Management Systems (SWfMS)
manage experiments’ provenance, keeping detailed
and meaningful records of data involved on experi-
ments and processes that affect the data. Provenance
is fundamental for scientific processes because it pro-
vides important documentation that is key to preserve
the data, to determine data quality and authorship, and
to reproduce as well as validate the results of such
processes (Davidson and Freire, 2008).
Workflow execution has been adopted where re-
sources are distributed on the Web, helping the coor-
dination and monitoring of processes. They are being
increasingly used to create complex Web applications
by Web service composition or by providing a thin
client, accessible through a browser, to conduct large
scale processes and experiments (Wei Tan, 2013). In
order to enhance their applicability, research efforts
are concerned with providing workflow mechanisms
with more flexibility, including in the healthcare sce-
nario such as (Dang et al., 2008), or (Schick et al.,
2012). Even though there are mechanisms that can
be used to pre-define exceptions and alternative paths
along workflows, they were not designed to dynami-
cally evolve the workflow specification driven by the
context, e.g., unfolding blocks of actions according to
contextual data collected during a process execution.
Compared to CIG systems, workflow systems
have been widely adopted and have consolidated stan-
dards and tools. In order to exploit the advantages of
workflow systems in the health context, this work pro-
poses to incorporate into workflows the dynamic and
context-driven approach followed by care-flow sys-
tems. This is based on our experience (Vilar et al.,
2013) that shows that the effort to do this is less com-
plex than the process to adapt CIG systems so that
they can acquire the features that are causing scien-
tific workflows to become widely adopted. This pa-
per analyses the features that confer high flexibility
to CIGs – mainly those based on the TNM due to its
emergent behavior – and presents our initial approach
to bring them to a SWfMS.
2 CLINICAL PRACTICE
GUIDELINES AND
TASK-NETWORK MODELS
Clinical Practical Guidelines (CPGs) are written
guidelines that describe the evidence-based proce-
dures to be followed during diagnosis, treatment, and
clinical decision making for a specific disease. Their
textual format can be easily diffused, but not easily
used in daily work (Panzarasa and Stefanelli, 2006),
because of a multitude of forms and specialized vo-
cabulary. Moreover, they depend heavily on the ex-
pertise of health professionals.
An approach to solve these problems is the
dissemination of guidelines’ content in machine-
interpretable representations, which are more suit-
able for use in individual clinical decision support
(Panzarasa and Stefanelli, 2006). This approach has
led to the creation of Computer-Interpretable Guide-
lines (CIGs), which implement guidelines in ac-
tive computer-based decision support systems. CIGs
adopt models to represent the content to support de-
cisions. Some examples of such models are Task-
Network Models (TNMs), Medical Logic Modules
(MLMs) and Augmented Decision Tables (ADTs).
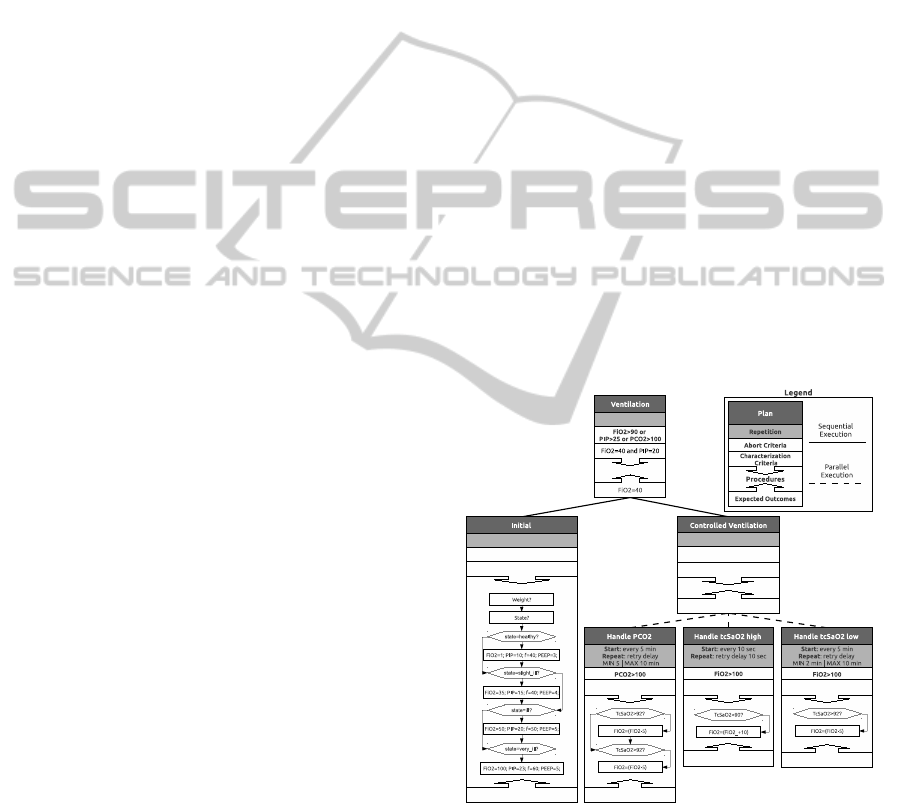
Figure 1: Example of CIG structure for a Controlled Venti-
lation plan.
(Gooch and Roudsari, 2011) identified 8 knowl-
edge models implemented, related to clinical deci-
sions, concluding that TNM was the most commonly
adopted. The authors characterize TNM in two ways:
general and formal. General TNMs are “flowcharts
or process maps without formal semantics”. For-
mal TNMs are “guideline-based clinical tasks – ac-
WEBIST2014-InternationalConferenceonWebInformationSystemsandTechnologies
50

tions, decisions, queries – that unfold over time, with
a formal syntax and semantics”. According to (Pe-
leg et al., 2003), TNMs succeed over alternative ap-
proaches, such as MLMs and ADTs, because they do
not provide full support for conceptualizing a multi-
step guideline that unfolds over time. Considering
those aspects, in this work we focus on TNMs.
Figure 1 shows a usual structure of a TNM. As
the ‘Legend’ (top right) shows, the basic component
is a plan and it represents a procedure to be applied
to some case. In each box, a rectangle with a label is
the name of the plan. The top plan – labeled Ventila-
tion– is the starting (seed) plan. The following plans
(below) are sub-plans that can be triggered by the up-
per plan according to rules. To decide whether a plan
should be applied or not, there are Characterization
Criteria that define conditions to be analyzed in order
to match the patient case to the diagnosis. Another
aspect that can be used to determine if the plan is suit-
able to the case is the Expected Outcomes. The flow
of actions and conditions appear whithin the Proce-
dures box. Whenever a plan is recognized as a way
to achieve the same result desired by the healthcare
professional, the plan will be triggered.
A triggered plan will follow the Procedures that
are recommended to be applied to the patient. The
repetition of those internal procedures is guided ac-
cording to the Repetition specification associated to
the plan. Also, it is possible to associate Abort Cri-
teria to interrupt the plan when a specific situation
is achieved. A plan can trigger potential sub-plans,
allowing to modularize and reuse plans that already
encapsulate needed practices. The fact that the re-
sults can be unexpected, and consequently the sub-
plans will be selected during the execution, produces
an emergent behavior in the flow of activities. Sev-
eral potential flows, constrained by rules, will dynam-
ically shape one flow on-the-fly during the execution,
interacting with contextual values. This work cap-
tures this rule-based and context-driven emergent be-
havior and adapts it to workflows.
To explain the characteristics of TNMs we use the
same scenario that Aigner and Miksch (Aigner and
Miksch, 2006) adopt to validate the CareVis platform:
Infants Respiratory Distress Syndrome (I-RDS). As
Miksch (Miksch et al., 1998) explains, “after I-RDS
is diagnosed, a plan dealing with limited monitoring
possibilities is activated, called initial-phase. Then
follows, depending on the severity of the disease,
three different kinds of plans, controlled-ventilation,
permissive-hypercapnia, or crisis-management. Only
one plan at a time can be activated, however the or-
der of execution and the activation frequency of the
three different plans are depending on the severity of
the disease”.
The scenario is shown on Figure 1. The plan exe-
cution order is read as top-down, left to right. Dashed
lines from a plan represent alternative sub-plans that
are used according to the conditions. To represent
the internal
Procedures
, we use the same represen-
tation as CareVis: flow-charts. An internal procedure
is described as a flow of CareVis ‘single-steps’. Each
single-step is either a variable assignment, a if-then-
else construct (hexagon), an ask element (rectangle).
The Ventilation plan is activated when the charac-
terization criteria FiO2>40 and PIP=20 is satisfied.
The plan and all sub-plans are aborted if the condition
FiO2>90 or PIP>25 or PCO2>100 is achieved. As
Ventilation plan does not have internal procedures, the
Initial plan is executed, following the sequential or-
der specified. The Initial plan just has a set of internal
procedures, such as ask weight and state of the patient
and define variable values according to the state value
(healthy, slightly ill, ill and very ill).
3 WORKFLOWS
A workflow is defined as the movement of tasks
through a work process describing how tasks are
structured, who performs them, the resources needed
and their relative order (Dallien et al., 2008). On a
computational context, a workflow specification can
be seen as an abstraction that allows the structured
composition of programs as a sequence of activities
aiming a desired result (Ogasawara et al., 2009).
Business and science are the two main driving
forces behind the development of Workflow Manage-
ment Systems (WfMSs). According to Sonntag et
al. (Sonntag et al., 2010), business workflows are
focused on the control of the flow, adopt agreed-
upon communication standards, in order to facili-
tate interoperation between different software sys-
tems and companies, and commonly are concerned
about fault handling, transactions, or quality of ser-
vice features. Scientific workflows, on the other hand,
are focused on data transformation, commonly may
involve computation-intensive tasks, and are con-
cerned with the specification of explicit data flow, the
exact reproducibility of workflows, or processing of
data streams.
The Workflow Management Coalition (WfMC)
is one important participant of those driving forces
behind WfMSs development. Because of its in-
volvement on the earlier stage of the creation of
workflows, it defines the workflow components
under the business perspective. In this work we use
the WfMC definitions, relaxing them to a broader
UsingHealthcarePlanningFeaturestoDriveScientificWorkflowsontheWeb
51
perspective that also covers scientific workflows
(WfMC, 1999). Here we differentiate between a
workflow specification and its instantiation (an actual
execution). Moreover, we use the term ‘task’ as
a synonym for ‘activity’ (where an activity is “a
description of a piece of work that forms one logical
step of a process” (WfMC, 1999). We likewise
distinguish Process definition from Process/Activity
Instance.
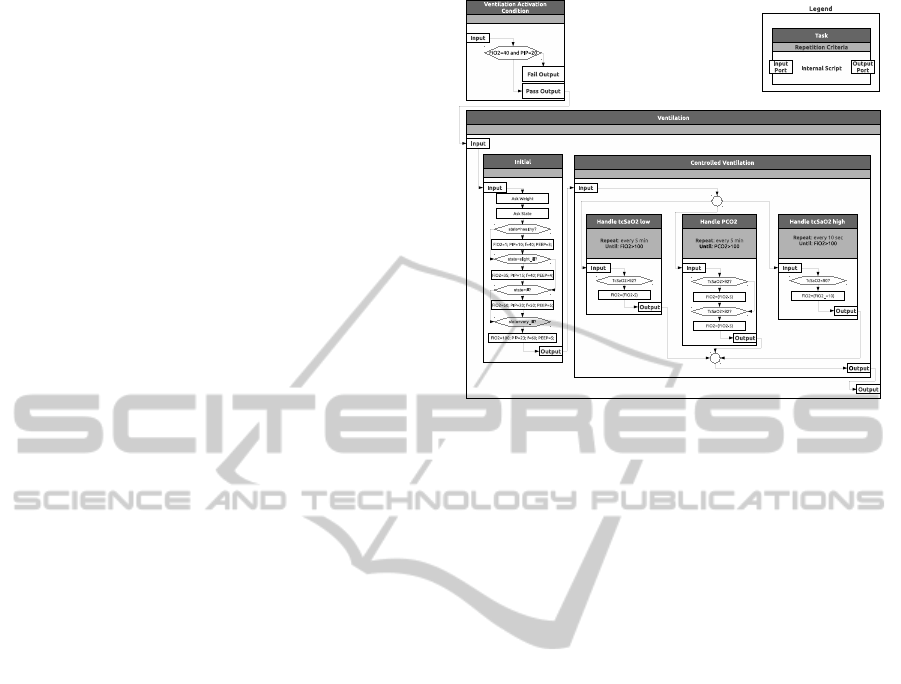
In order to help compare workflow and TNM ap-
proaches, we re-engineered the Controlled Ventilation
plan of Section 2 using part of the graphical notation
of flow-charts used on TNMs, but following a repre-
sentation similar to that adopted by the Taverna (Hull
et al., 2006) workflow system – see Figure 2.
The ‘legend’ (top right) shows the basic notion of
structure of a process. The top rectangle with a text is
the name of the process. The second one is the repe-
tition criteria, which allows to define criteria to repeat
the process and an interval for each repetition. Like
TNMs, workflows may contain internal procedures,
specified program code or instructions, that allows to
perform activities. For instance, processes ‘Handle
PCO2’ contains repetition criteria and embeds code
that is repeated according to the criteria.
An important distinction between TNMs and
workflows is the access to the variable values. While
on TNM each value may act as a global variable,
which can be accessed from anywhere in a plan, on
workflows the values should be explicitly passed for
each process through a port. Input ports receive the
values of a process, while outport ports contains the
result of a process. Of course, processes can read and
write from a common storage, but this approach re-
duces the generality of processes.
To exemplify the use of a workflow, consider
again the Controlled Ventilation plan, now executed
as a workflow depicted in Figure 2. To determine
whether the Ventilation process should be executed,
the Ventilation Activation Condition process is intro-
duced. If the condition FiO2=40 and PIP=20 is sat-
isfied, the result is passed to the Pass Output port,
which indicates that the Ventilation process should be
performed. If the condition is not satisfied, the result
is passed to Fail Output port, finishing the execution
of the workflow. Ports thus enable conditioning the
path according to the obtained result.
Considering that the Ventilation Activation Condi-
tion process generated a Pass Output value, the Venti-
lation process receives an input value and passes it to
its internal processes. As well as on Figure 1, Initial
and Controlled Ventilation are sequentially executed.
This execution is explicitly defined by the fact that the
Figure 2: Controlled Ventilation plan re-engineered by us
as a workflow structure.
Initial Output port is connected to the Controlled Ven-
tilation Input port. While the Initial process uses its
internal script to obtain the values of weight and state,
Controlled Ventilation has sub-processes that are per-
formed on any order. In fact, differently from TNMs,
those sub-processes can be executed at the same time.
The split-join, represented by a circle before and after
the processes, indicates that any process (among Han-
dle tcSaO2 low, Handle PCO2 and Handle tcSaO2
high) can be executed. The split-join allows to exe-
cute different processes and then combines the results
so that can be passed to another process or port.
If we proceed mapping a TNM specification to a
workflow, the alternatives in each stage will grow ex-
ponentially. This effect shows the limits of trying to
directly map a TNM specification in a classic work-
flow specification. Our proposal addresses this prob-
lem. It blends the TNM rule-based context-driven
mechanism in a workflow system, providing an equiv-
alent TNM ability of adapting itself according to the
context.
4 DATA-DRIVEN VS
PROCESS-DRIVEN
APPROACHES
In order to summarize some of the main distinctions
between the Workflow and TNM approaches is: sci-
entific workflows are process driven and TNMs are
data driven. Thus, bringing TNM characteristics into
scientific workflows will make the latter both data and
process driven.
WEBIST2014-InternationalConferenceonWebInformationSystemsandTechnologies
52

TNMs are built to reduce the complexity to deal
with large amounts of content that must be interpreted
and to guide the use of procedures that are recom-
mended to achieve some state. Because a patient may
change his/her condition unexpectedly, TNMs allow
to activate or deactivate content (guides and proce-
dures) to treat the current state of the patient. All
guides and procedures are pre-specified according to
the recommendations of medical councils and well es-
tablished procedures.
Scientific workflows are focused on processing
high amounts of data. Usually there are two com-
mon situations: (i) a scientist wants to represent and
automate a well known/consolidated experiment and
execute it with different data (parameters) with none
or few changes during the execution; (ii) the scientist
wants to create an experiment to test a new hypothe-
sis, so (s)he starts to build a workflow including and
changing processes and parameters after different ex-
ecutions to analyze the results.
The difference between both approaches can be
observable on the basic component of each one.
TNMs have plans that associate content, procedures
and other plans. Also, there are criteria that must be
satisfied to activate the plan; such criteria allow se-
lecting a plan over all other possible situations that
may occur. Scientific workflows have processes that
can be associated to others to create the flow of data
and transform/process it. The data that is passed from
one process to another can lead to different paths, but
commonly the possible number of paths and changes
are not as high as on TNMs. When a new situation oc-
curs and there is a need to incorporate a new process,
the scientist changes the workflow – e.g., choosing
from a repository of processes, including an external
tool or creating a new process.
Another factor is that, to deal with all resources
involved, it is necessary to provide tools to visualize
and filter information, as well as be aware of the ori-
gin and the involvement of resource with respect to
the data. A key issue is to maintain provenance in-
formation on data and procedures – e.g., what kind of
data was used where, how and by whom. Here, work-
flow systems already provide some sort of traceability
mechanism.
In this paper we focus on the main features re-
quired to achieve a data-driven workflow: changing
workflow tasks to adapt them to a situation. Our ap-
proach is presented next.
5 TOWARDS MAKING
SCIENTIFIC WORKFLOWS
DATA-DRIVEN
As presented in previous sections, a key factor to
produce workflows able to adapt to the high dy-
namic health environments is the rule-based TNM
approach, which triggers modules according to con-
text values, producing an emergent behavior. Differ-
ent from TNM specifications, which start from a seed
and expands the flow, a workflow has a predefined
starting flow. Therefore, we translated the mechanism
of unfolding new activities on-the-fly according rules
(TNM) to a mechanism of adapting the existing work-
flow on-the-fly according to rules (our approach).
In order to fully support dynamic workflow
changes according to context, and give more flexibil-
ity to workflow execution, we decided to adopt rea-
soning capabilities and combine them with domain
semantics. The solution found was to (a) use on-
tologies as the basis for workflow and concept rep-
resentation, and (b) create adaptation rules to repre-
sent experts’ knowlege. An adaptation rule character-
izes a situation (cause) and defines the change (conse-
quence) that should be performed to workflow so that
it can be adapted to the context.
Given that there exist distinct workflow represen-
tations and formats (according to the WfMS adopted),
the overall dynamic adaptation cycle can be described
as follows. The workflow execution on the Web is
monitored at each activity.Every new workflow state
is mapped to an ontology instance, to which reason-
ing is applied, resulting in a new ontology instance
(containing recommended modifications to that state).
This new instance is transformed back to the work-
flow representation of the WfMS adopted, which is
shown back to the user on the Web interface, to be
validated or modified.
The architecture of our work is presented in Figure
3, where CRec (Context Record) is the linearized rep-
resentation of an ontology, representing a workflow
state. The main components are the following. A Sci-
entific Workflow Management System (SWfMS)
used to create and execute workflows, through a
Web Interface, extended to incorporate the adaptation
mechanism. A Context-Aware Extension, respon-
sible for monitoring workflow execution and identi-
fying the events that occur during that execution. A
Semantic Mapper that is responsible for translating
a workflow to a CRec and vice-versa, allowing the
Context-Aware Extension to update the original work-
flow on SWfMS. An Ontology that specifies the main
classes used to represent workflow activities and their
parameters. Also, there are additional classes used to
UsingHealthcarePlanningFeaturestoDriveScientificWorkflowsontheWeb
53
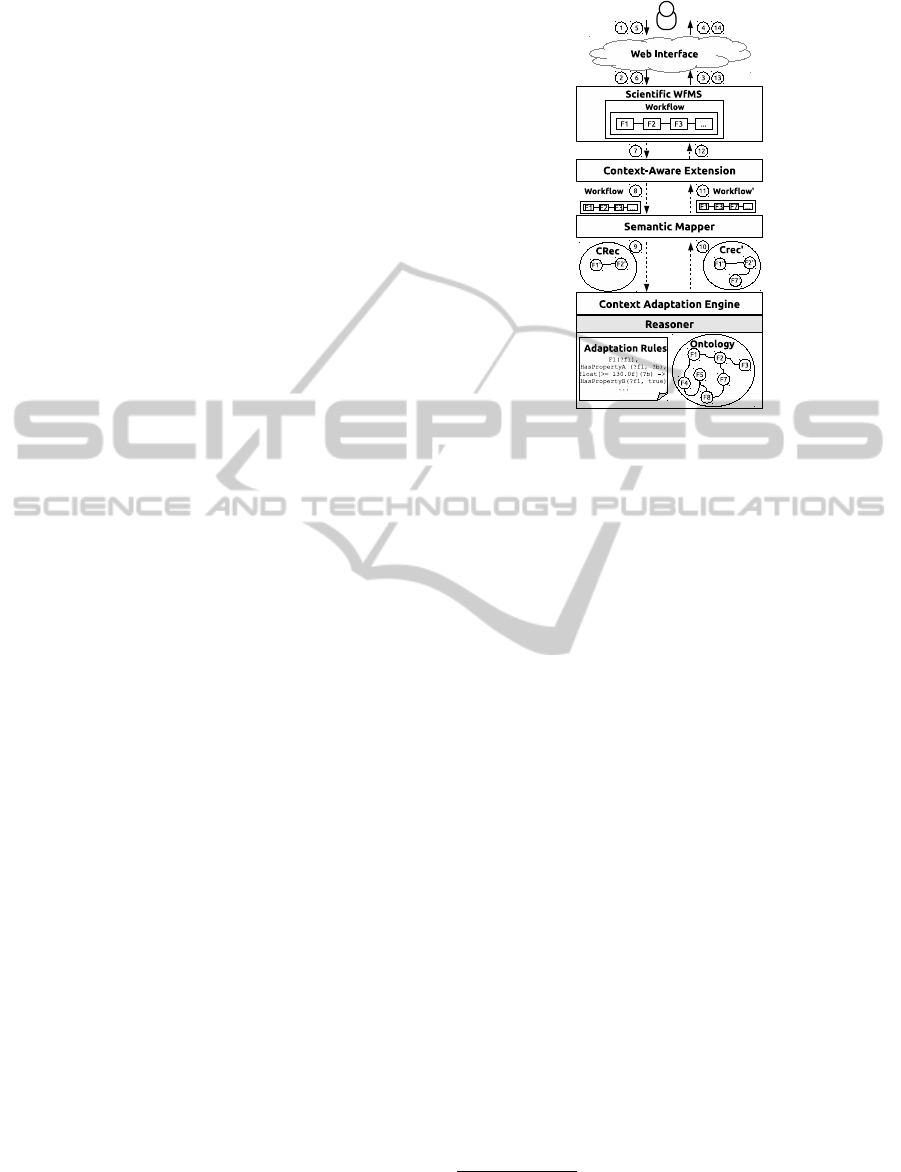
complement activity information (such as activation
status) and associated content (for instance, patient
data). A CRec (resp. CRec’) is a Context Record
that is an ontology instance that represents the current
state of a workflow and all information regarding the
patient under care. A set of Adaptation Rules (AR),
written in SWRL, that will be used with an Ontology
and a CRec to identify the changes recommended to
the current situation. A Context Adaptation Engine
(CAEng) that uses an Ontology Reasoner to process
the AR combined to an Ontology and a CRec. The
reasoning updates CRec to guide the adaptations that
should be made on workflow.
The architecture enables dynamic adaptation of
workflows to a context as follows. A SWfMS is ac-
cessed through a Web Interface (Figure 3, interaction
1). A workflow is assigned to be executed on the
SWfMS (on interaction 2) and the SWfMS loads it
(interaction 3) and updates the Web Interface (inter-
action 4). A user requests the SWfMS to start the
executing workflow (interactions 5 and 6). When an
activity is performed, the Context-Aware Extension
captures the workflow state (interaction 7) and passes
it to the Semantic Mapper (interaction 8). Next, the
Semantic Mapper uses the workflow state to create
an ontology instance that represents it (interaction 9)
– CRec. The CAEng combines AR, Ontology, and
CRec to identify the adaptations recommended to the
workflow and apply them to CRec, creating a new
version of it (CRec’. The Semantic Mapper receives
CRec’(interaction 10) and maps its data to the work-
flow representation, passing it back to the Context-
Aware Extension (interaction 11). The workflow on
the SWfMS is updated by the Context-Aware Exten-
sion according to the new workflow (interaction 12).
The SWfMS updates the Web Interface (interaction
13). Finally, the user sees the adapted version of the
workflow (interaction 14).
Our architecture may be used on different sce-
narios and on different SWfMS, but its components
created must be changed according to the scenario
(e.g., rules and ontology customization) and platform
adopted (e.g., Semantic Mapper).
6 INSTANTIATION ON THE WEB
We applied the principles behind our architecture to
the context of nursing care to attest the flexibility of
execution of the workflows. The tasks used to con-
struct the ontology and the rules were based on the
PROCEnf system (Peres et al., 2009), developed and
adopted by the hospital of the University S
˜
ao Paulo.
PROCEnf is also in process of adoption at the our
Figure 3: Architecture for context-based workflow adapta-
tion.
University Hospital
1
. Like most such systems, PRO-
CEnf is heavily centered on offering health profes-
sionals sets of forms to fill.
We chose PROCEnf among other reasons, be-
cause we can reuse its components. Moreover, given
our need to validate our implementation with actual
users, this choice offers to the nursing staff of our Uni-
versity Hospital a set of forms and vocabulary they are
familiar with.
Based on PROCEnf and on the work described in
(Doenges and Moorhouse, 2008), we described the
flow of a patient’s admission and monitoring process
in a hospital. In a general way, the process includes
an iterative step which is started by an anamnesis in-
terrogation, which is an assessment phase to evaluate
the patients’ conditions. Next, there is the analysis
of recorded data to diagnose the problem and to iden-
tify expected outcomes (prognosis). Based on those
expected outcomes, health interventions are planned
and applied. To identify whether the outcomes were
achieved or not, the intervention results are analyzed
and the amamnsesis records are updated. If the treat-
ment achieves the expected outcomes, the patient can
be released. Otherwise, a new iteration occurs.
To model PROCEnf forms as workflow activities,
we created an ontology. In our current stage of re-
search, we have about 30 activity classes involved
with the diagnosis phase. Those classes are directly
related to the PROCEnf system. As can be seen on
1
The hospital complex of the University of Camp-
inas alone receives about 500,000 appointments, with over
43,000 admissions and 34,000 surgical interventions per
year.
WEBIST2014-InternationalConferenceonWebInformationSystemsandTechnologies
54

classes ‘CardiacFunction’ and ‘VitalSigns’, there are
different attributes that can be filled to draw a diagno-
sis. Depending on how an attribute is filled, distinct
decisions have to be taken – i.e., the workflow has to
be changed dynamically.
Another issue we faced was the integration of
workflow structures, rules, and reasoning capabilities.
As explained before, this was solved by treating all
information within a single ontology-based reason-
ing framework. The Semantic Mapper transforms the
workflow structures (together with a current work-
flow state) into an ontology instance, that is enhanced
with the current patient state. This is then treated
by the reasoner as any other ontology, using adapta-
tion rules that encode domain and user knowledge.
Such adaptations are performed based on the adapta-
tion rules we created in SWRL. Those rules can be
classified into four types: I) Propagate field (param-
eter) value: repeat the value of a field to related fields,
avoiding the need to fill the value in other forms. II)
Infer field (parameter) value: the value of a field
according to the value of other fields. III) Change
form (activity) position: the order in forms which are
filled can be changed, increasing or decreasing filling
priority, making related forms closer and unrelated or
unlikely forms more distant in the filling order. IV)
Include/Remove form (activity): a form can be re-
moved when a field makes it incompatible with the
purpose of the form (e.g., pregnancy issues related to
men). Inclusion occurs whenever a situation makes a
previoulsy removed form viable.
Table 1 presents a subset of the rules, highlight-
ing the types and some of their potential. The
rules are specified in SWRL and are specified in
cause/consequence form. The cause (antecedent) can
be defined according to the value of fields and forms,
by the composition of different predicates. A conse-
quence (consequent) is the result of checking the an-
tecedent, e.g., changing of a property value, including
or removing values. For instance, rule R2 says that
when the Systolic Blood Pressure value of Vital Signs
is large than 130, then the field Has Systolic Blood
Pressure Out of Expected Range should be true.
Let us exemplify how adaptation rules are used in
the reasoning process. Consider the following sce-
nario: a nurse should fill a set of forms about dif-
ferent patient conditions, including vital signs, self-
care, and comfort. At the beginning of the process,
the professional fills a form about Vital Signs. If the
value of systolic blood pressure is filled with value
large than 130, rule R2 (Table 1) has its antecedent
condition satisfied, so the inference engine applies the
consequent which characterizes the patient as having
a systolic pressure out of expected range. As a re-
sult, two other rules are to be executed, leading to the
new adaptations: R1, to propagate the value of sys-
tolic blood pressure to the Cardiac Function task and
R4 to increase the priority of the Cardiac Function
task, which will put this form closer to the Vital Signs
form. This order change highlights the need to pro-
vide additional information about Cardiac Function
details and to avoid the loss of focus and information
regarding this problem.
7 CONCLUSIONS
In this paper, we presented a proposal to adapt scien-
tific workflows to the context of healthcare manage-
ment, and its Web implementation. Our modifications
to an SWfMS place such systems closer to the domain
of healthcare, thanks to the inspiration from CIGs and
to the fact that such systems, thanks to the data-driven
flow, are suitable to dynamic scenarios.
We designed the model in which an SWfMS is ex-
tended by a layer which uses ontologies combined to
rules as a means to make scientific worflows more
data-driven than just process-driven. This in turn,
brings more flexibility to the execution of the tasks
as well as allows to choose whether a task should be
executed according to more sophisticated conditions.
Future steps of this research will cope with TNM
features, presented in Section 4, working on the bet-
ter graphical integration and adaptation of the work
with the SWfMS, allowing to: (i) Integrate the on-
tology content to the workflow tasks, allowing users
to navigate through the concepts of ontologies and
use those concepts also as a way to filter tasks and
conveniently find resources on SWfMS; (ii) Provide
support to the hierarchical organization of workflow
tasks, giving more dynamic flow to task execution as
well as making it more similar to the TNM approach.
ACKNOWLEDGMENTS
Work partially financed by FAPESP (grant
2011/17196-0), FAPESP/Cepid in Computa-
tional Engineering and Sciences (2013/08293-7),
the Microsoft Research FAPESP Virtual Institute
(NavScales project), CNPq (MuZOO Project),
FAPESP-PRONEX(eScience project), INCT in Web
Science, and individual grants from CNPq. We
also thank healthcare providers from University of
Campinas and University of S
˜
ao Paulo, who provided
us support in this research.
UsingHealthcarePlanningFeaturestoDriveScientificWorkflowsontheWeb
55
Table 1: Adaptation Rules.
Rule Antecedent Consequent Type
R1 CardiacFunction(?cf), VitalSigns(?vs), systolicBloodPressure(?vs, ?x) systolicBloodPressure(?cf, ?x) Propagate Value
R2 VitalSigns(?vs), systolicBloodPressure(?vs, ?x), float[>= 130.0f](?x) hasSystolicPressureOut-
OfExpectedRange(?vs, true)
Infer Value
R3 VitalSigns(?vs), isActive(?vs, true), hasSystolicPressureOutOfExpectedRange(?vs, false), CardiacFunc-
tion(?cf)
position(?cf, 99) Decrease Priority
R4 VitalSigns(?vs), hasSystolicPressureOutOfExpectedRange(?vs, true), isActive(?vs, true), CardiacFunc-
tion(?cf), position(?vs, ?po)
position(?cf, ?po) Increase Priority
R5 ValuesAndBeliefs(?va), Evaluation(?e), hasPatient(?e, ?p), isActive(?e, true), hasAge(?p, ?age), inte-
ger[<= 12](?age)
isRemoved(?va, true) Remove
R6 ValuesAndBeliefs(?va), Evaluation(?e), hasPatient(?e, ?p), isActive(?e, true), hasAge(?p, ?age), inte-
ger[>12](?age), isRemoved(?va, true)
isRemoved(?va, false) Include
REFERENCES
Aigner, W. and Miksch, S. (2006). Carevis: Integrated
visualization of computerized protocols and tempo-
ral patient data. Artificial Intelligence in Medicine,
37(3):203–218.
Bharathi, S., Chervenak, A., Deelman, E., Mehta, G., Su,
M.-H., and Vahi, K. (2008). Characterization of sci-
entific workflows. 2008 Third Workshop on Workflows
in Support of Large-Scale Science, pages 1–10.
Dallien, J., MacCaull, W., and Tien, A. (2008). Initial work
in the design and development of verifiable workflow
management systems and some applications to health
care. In Proceedings of the 2008 5th International
Workshop on Model-based Methodologies for Perva-
sive and Embedded Software, MOMPES ’08, pages
78–91, Washington, DC, USA. IEEE Computer Soci-
ety.
Dang, J., Hedayati, A., Hampel, K., and Toklu, C. (2008).
An ontological knowledge framework for adaptive
medical workflow. Journal of biomedical informatics,
41(5):829–36.
Davidson, S. and Freire, J. (2008). Provenance and sci-
entific workflows: challenges and opportunities. In
SIGMOD Conf., pages 1345–1350. Citeseer.
Doenges, M. and Moorhouse, M. (2008). Application of
nursing process and nursing diagnosis: an interactive
text for diagnostic reasoning. G - Reference, Informa-
tion and Interdisciplinary Subjects Series. F.A. Davis.
Gooch, P. and Roudsari, A. (2011). Computerization of
workflows, guidelines, and care pathways: a review of
implementation challenges for process-oriented health
information systems. Journal of the American Medi-
cal Informatics Association : JAMIA, 18(6):738–48.
Hull, D., Wolstencroft, K., Stevens, R., Goble, C., Pocock,
M. R., Li, P., and Oinn, T. (2006). Taverna: a tool for
building and running workflows of services. Nucleic
acids research, 34(-):W729–32.
Miksch, S., Kosara, R., Shahar, Y., and Johnson, P. D.
(1998). AsbruView: Visualization of Time-Oriented,
Skeletal Plans. pages 11–18.
Ogasawara, E., Paulino, C., Murta, L., Werner, C., and Mat-
toso, M. (2009). Experiment line: Software reuse in
scientific workflows. In Winslett, M., editor, Scientific
and Statistical Database Management, volume 5566
of Lecture Notes in Computer Science, pages 264–
272. Springer Berlin Heidelberg.
Panzarasa, S. and Stefanelli, M. (2006). Workflow manage-
ment systems for guideline implementation. Neuro-
logical sciences : official journal of the Italian Neu-
rological Society and of the Italian Society of Clinical
Neurophysiology, 27 Suppl 3:S245–9.
Peleg, M., Tu, S., Bury, J., Ciccarese, P., Fox, J., Greenes,
R. A., Miksch, S., Quaglini, S., Seyfang, A., Short-
liffe, E. H., Stefanelli, M., and et al. (2003). Compar-
ing computer-interpretable guideline models: A case-
study approach. JAMIA, 10:2003.
Peres, H. H. C., Cruz, D. D. A. L. M. D., Lima, A. F. C.,
Gaidzinski, R. R., Ortiz, D. C. F., Trindade, M. M. E.,
Tsukamoto, R., and Conceic¸
˜
ao, N. B. (2009). Desen-
volvimento de Sistema Eletr
ˆ
onico de Documentac¸
˜
ao
Cl
´
ınica de Enfermagem estruturado em diagn
´
osticos,
resultados e intervenc¸
˜
oes. Revista da Escola de En-
fermagem da USP, 43(spe2):1149–1155.
Schick, S., Meyer, H., Bandt, M., and Heuer, A. (2012). En-
abling yawl to handle dynamic operating room man-
agement. In Daniel, F., Barkaoui, K., and Dustdar,
S., editors, Business Process Management Workshops
(2), volume 100 of Lecture Notes in Business Infor-
mation Processing, pages 249–260. Springer.
Sonntag, M., Karastoyanova, D., and Deelman, E. (2010).
Bridging the gap between business and scientific
workflows: Humans in the loop of scientific work-
flows. In e-Science (e-Science), 2010 IEEE Sixth In-
ternational Conference on, pages 206–213.
Unertl, K. M., Weinger, M. B., Johnson, K. B., and Lorenzi,
N. M. (2009). Describing and modeling workflow
and information flow in chronic disease care. Jour-
nal of the American Medical Informatics Association
: JAMIA, 16(6):826–36.
Vilar, B. S. C. M., Medeiros, C. B., and Santanch
`
e, A.
(2013). Towards adapting scientific workflow systems
to healthcare planning. In HEALTHINF - Interna-
tional Conference on Health Informatics.
Wei Tan, M. Z. (2013). Business and Scientific Workflows:
A Web Service-Oriented Approach. Wiley.
WfMC (1999). Terminology and Glossary Document Num-
ber WFMC-TC-1011 - Issue 3.0. Technical report,
Workflow Management Coalition.
WEBIST2014-InternationalConferenceonWebInformationSystemsandTechnologies
56
