
eXiTCDSS: A Framework for a Workflow-based CBR
for Interventional CDSS
Application to Transcatheter Aortic Valve Implantation (TAVI)
Andres El-Fakdi, Francisco Gamero, Joaquim Mel
´
endez and Roberto Petite
Control Engineering and Intelligent Systems Group eXIT, University of Girona, Campus Montilivi Building PIV, 17071
Girona, Spain
Keywords:
Clinical Decision Support Systems, Case-based Reasoning, TAVI, Clinical Workflow.
Abstract:
The work presented in this paper presents a workflow-based Clinical Decision Support System (CDSS) de-
signed to give case-specific assessment to clinicians during complex surgery or Minimally Invasive Surgerys
(MISs). Following a perioperative workflow, the designed software will use a Case-Based Reasoning (CBR)
methodology to retrieve similar past cases from a case base to give case-specific advice at any particular point
of the process. The graphical user interface allows easy navigation through the whole support progress, from
the initial configuration steps to the final results organized as sets of experiments easily visualized in a user-
friendly way. The tool is presented giving advice to an example application, a complex minimally invasive
surgery which is receiving growing attention lately, the Transcatheter Aortic Valve Implantation (TAVI).
1 INTRODUCTION
Nowadays, medicine and health fields are getting
more and more involved with computer science.
Among all branches, the main focus of the current re-
search points towards Artificial Intelligence (AI) to
improve the performance of Clinical Decision Sup-
port Systems (CDSSs). In a general term, CDSSs
comprise a large spectrum of systems which provide
clinicians, staff, patients, and other individuals with
knowledge and person-specific information, intelli-
gently filtered and presented at appropriate times, to
enhance health and health care (Berner, 2009).
CDSSs are classified into two main groups,
depending on whether they are knowledge-based
systems, or nonknowledge-based systems (Berner,
2009). The knowledge-based CDSSs are the most
common type of CDSSs used in clinics and hospi-
tals. They are structured around rules mostly in the
form of IF-THEN statements. Most of knowledge-
based systems consist of three parts, the knowledge
base, inference engine, and mechanism to communi-
cate (Wyatt and Spiegelhalter, 1991). The rules are as-
sociated with compiled data extracted from a knowl-
edge base. The inference engine combines the rules
from the knowledge base with the patient’s data. The
communication mechanism will allow the system to
show the results to the user as well as have input
into the system. Nonknowledge-based CDSSs use AI
through machine learning techniques, which allow the
computer to learn from past experiences and to recog-
nize patterns in the clinical data (Marakas, 1999).
Artificial Neural Network (ANN) (Baxt, 1995) and
genetic algorithms (Laurikkala et al., 1999) are two
common types of nonknowledge-based systems. The
fusion of a knowledge base with nonknowledge-based
machine learning techniques results into an hybrid
system. Hybrid systems extract the best from both
methodologies, finally resulting into an overall im-
provement of the system performance and thus pro-
viding an optimal solution for clinical decision sup-
port systems (Demmer-Fushman and Lin, 2007). This
paper will focus on this kind of hybrid systems, pre-
senting a software framework for CDSS which uses
a well-known lazy learning technique called Case-
Based Reasoning (CBR) (Aamodt and Plaza, 1994)
and a past patients case base to asses clinicians.
This paper work presents a workflow-based CDSS
designed to give case-specific assessment to clini-
cians during complex surgery. Following a periop-
erative workflow, the designed software will use a
CBR methodology to retrieve similar past cases from
a case base to give case-specific advice at any partic-
ular point of the process. The graphical user inter-
face allows easy navigation through the whole sup-
port progress, from the initial configuration steps to
201
El-Fakdi A., Gamero F., Meléndez J. and Petite R..
eXiTCDSS: A Framework for a Workflow-based CBR for Interventional CDSS - Application to Transcatheter Aortic Valve Implantation (TAVI).
DOI: 10.5220/0004233802010206
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2013), pages 201-206
ISBN: 978-989-8565-37-2
Copyright
c
2013 SCITEPRESS (Science and Technology Publications, Lda.)

the final results organized as sets of experiments eas-
ily visualized in a user-friendly way. The eXiTCDSS
tool is presented giving advice to an example appli-
cation, assisting a recent complex minimally invasive
surgery which is receiving growing attention lately,
the Transcatheter Aortic Valve Implantation (TAVI).
This paper is structured as follows. In Section 2
a description of the workflow management during an
intervention is detailed. Also, recent applications of
CDSS for surgical processes are reviewed. Section 3
introduces the eXiTCDSS framework. In Section 4,
the eXiTCDSS demonstrates its performance with its
application to a TAVI procedure. Finally, conclusions
are included in Section 5.
2 CDSS INTEGRATION WITH
CLINICAL WORKFLOW
Examples of successful applications of CDSSs into
clinical workflows comprise computer based patient
record systems (Patel et al., 2000), knowledge man-
agement systems for biomedical engineering (Rinkus
et al., 2004) and computer based training systems in
pathology (Crowley et al., 2003). From the successful
applications mentioned before it can be extracted that
integration with workflow is key to success. How to
integrate the CDSS with clinician workflow, however,
remains a challenge, in part because there are no cur-
rent standards for clinical workflow (Das and Eichner,
2010).
Although there is no universally agreed upon defi-
nition of the term workflow, for the purpose of this ar-
ticle, we have taken the workflow definition stated in
(Carayon et al., 2010) which defines a clinical work-
flow as a modular sequence of tasks, with a distinct
beginning and end, performed for the specific pur-
pose of delivering clinical care. In order to implement
a workflow-based CDSS, tasks, timing and involved
subprocesses must by identified first. Therefore, the
proposed workflow has been specified at up to four
level of detail: 1) clinical workflow, 2) phase, 3) task,
and 4) attribute. Figure 1 shows a schematic workflow
of an exemplified operative process where the previ-
ously mentioned levels have been illustrated. The first
level of the workflow represents the particular work-
flow itself. The second level describes the phases,
being a phase the primordial division of the specific
clinical workflow. For the particular example shown
in Figure 1, each phase corresponds to the pre, intra,
and post-operative periods. In the same way, every
phase has been split into tasks, a task being any partic-
ular step taken during each phase e.g. apply anesthe-
sia, initial puncture location or valve final placement.
Each task has a different number of distinguishable
items or attributes associated. These attributes refer
to all the important values or considerations that the
medical staff will take into account during the resolu-
tion of a task. The attributes can be described as nu-
merical data, text data, categorical data, and boolean
data. As numerical data it can be considered blood
count, coagulation parameters, age, size, or specific
physiologic measurements. The text data comprises
those textual items regarding the patient’s patholog-
ical or surgical history as well as possible allergies.
The categorical, in fact ordered categorical data, com-
prises attributes which measure a certain degree of
intensity, e. g. amount of calcification or valve re-
gurgitation while the boolean data confirms or denies
the presence of an attribute, for example the vascu-
lar tortuosity or the existence of coronary flow dam-
age. During the intervention execution and according
to the current information being generated, the CDSS
has to be capable to identify the phase, the task, and
the attributes involved. Then, the software will use the
CBR engine to retrieve the most similar cases to the
current one. The framework eXiTCDSS presented in
this article provides the required tools to define a case
structure for any clinical procedure based on a work-
flow.
3 THE eXiTCDSS FRAMEWORK
Case-Based Reasoning (CBR) is a technique of arti-
ficial intelligence that attempts to solve a given prob-
lem within a specific domain by adapting established
solutions to similar problems (Aamodt and Plaza,
1994). CBR has been formalized for purposes of rea-
soning and learning based on the exploitation of ex-
isting similar historical records as humans do. It has
been argued that CBR is not only a powerful method
for computer reasoning, but also a pervasive behavior
in everyday human problem solving; or, more radi-
cally, that all reasoning is based on past cases person-
ally experienced. These features make CBR a good
contender for any decision support system.
Four main phases of action are defined in the CBR
methodology: retrieve, reuse, revise and retain. For
example, in TAVI, a case base contains information
about patients that have been operated in the past. Us-
ing this case base, a CBR system is able to give advice
to future TAVI cases by following the four phases: re-
trieve, reuse, revise and retain. First, in the retrieve
phase, the current case is compared with all the past
experiences in the case base, and the most similar are
recovered. Given a target problem, during the retrieve
step, cases from memory that are relevant to solving
HEALTHINF2013-InternationalConferenceonHealthInformatics
202
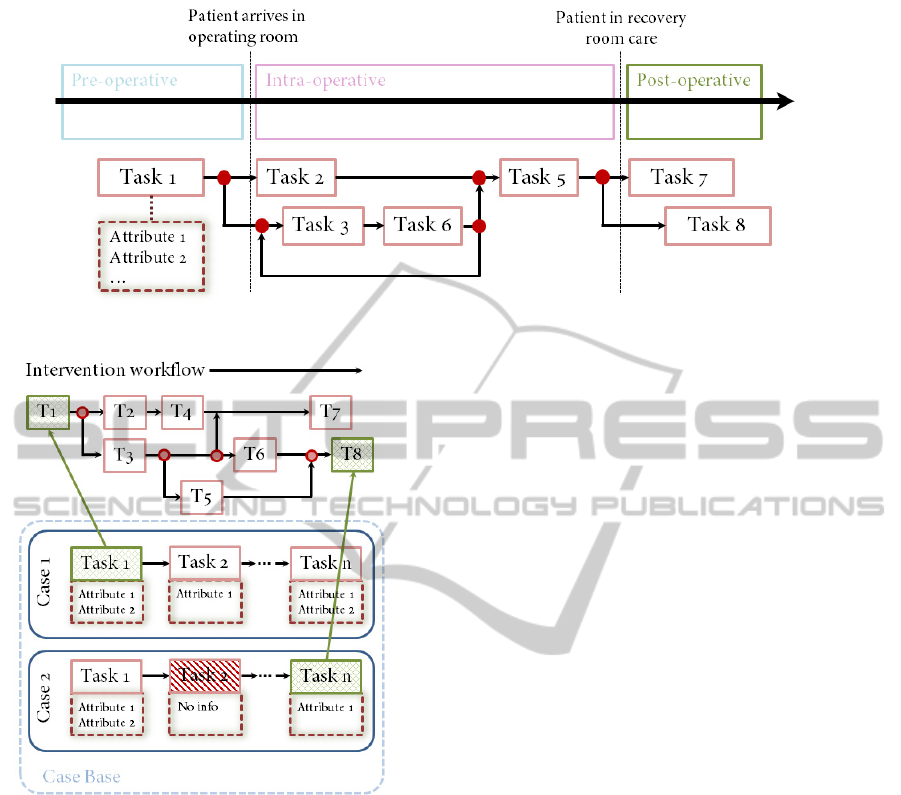
Figure 1: Schematic workflow showing an exemplified operative process.
Figure 2: Case structure and retrieval process along the op-
erative workflow.
it are recovered. A case is a whole although usu-
ally two parts can be identified according to the prob-
lem to be solved: problem and solution space. Prob-
lem space can incorporate specific case information
and also contextual information useful for solving the
problem whereas solution space incorporates infor-
mation directly related with the solution for solving
the problem. Next, in the reuse phase, a solution to
the current case is determined based on the solutions
found in the retrieved cases, which are mapped to tar-
get the actual problem. This may involve adapting the
solution as needed to fit the new situation. Third, the
computed solution is evaluated in the revise phase. Fi-
nally, the retain phase analyzes whether to retain the
case in the case base.
When the intervention begins, parallel to the
workflow progression described in Figure 2, the CBR
mechanism retrieves specific and contextual problem
information of similar past cases. Such assessment
step determines which cases address problems most
similar to the current problem, to identify them as
starting points for solving the new problem. Once the
operation ends, clinicians proceed with the new case
revision, which evaluates and adjusts the adapted so-
lutions and, if suitable, the new case will be retained
with the system learning from the situation by stor-
ing the result as a new case for future use. The soft-
ware has been designed to work either on-line inside
the Operation Room (OR) or off-line, as a knowledge
database for patient study.
As the eXiTCDSS framework goes beyond pure
CBR prototyping and aims to support workflow-
oriented decision support, other elements are required
in addition to the basic CBR modules. In order to ma-
nipulate the data, a common representation of cases
is required. Also, three main components are distin-
guished: the workflow editor, the CBR engine and
the results navigator. These components are described
next.
3.1 Case Representation
eXiTCDSS requires a plain Coma Separated Value
(CSV) file to handle the data. Each row corresponds
to a case, and each column to attributes of the cases.
The first four rows describe the attributes as follows.
The first row corresponds to the attribute descriptions
(for example, ”Annular calcification”). The second
row corresponds to the attribute name (usually in a
compressed form, as for example, ”Annularcalcifica-
tion”). The third row corresponds to the attribute type
(-1 ignore, 0 boolean, 1 numerical, 2 textual, 3 cate-
gorical). The fourth row corresponds to the attribute
weight (relevance). This representation covers most
of the data used in medical applications and is easy to
manage and general enough to be used by any of the
eXiTCDSS:AFrameworkforaWorkflow-basedCBRforInterventionalCDSS-ApplicationtoTranscatheterAorticValve
Implantation(TAVI)
203

current CBR techniques (mainly distance functions).
3.2 The Workflow Editor
To support a workflow-oriented CDSS software, a
workflow editor tool has been developed inside the
main application so that users can define a workflow
file. All the needed features to describe any type of
workflow are displayed in a window independent in-
terface that can be accessed from the tools label in the
top area of the main window frame of the platform.
This functionality includes a shapes menu with all the
types of boxes, containers and arrows used to define
the workflow structure with all the needed phases and
tasks. The created figures are editable and colorable,
with a label for its identification. After the structure
definition, on the right side of the window, the user
proceeds with the attributes-to-task association. By
loading the CSV file presented in Section 3.1, the user
can access to all the attributes which define a patient’s
case and associate them to its correspondent task of
the workflow. Once the workflow creation is com-
pleted, the workflow file is saved as an Extensible
Markup Language (XML) file which can be loaded
later on by the eXiTCDSS main application in order
to proceed with the project development.
3.3 The CBR Engine
All the information required to set up a CBR system
according to user requirements is stored in the config-
uration file. The CBR engine is responsible for read-
ing this file, extracting the selected XML and CSV
files, methods and parameters and, finally, calling and
executing the related CBR algorithms. Therefore,
once the configuration file is set, the eXiTCDSS loads
the patient case base and the associated workflow file.
Then, the engine compares the stored cases with the
current patient data, and selects the most similar cases
from the case base. There are local and global simi-
larity measures. Local similarity measures compare
two attribute values. Global similarity measures com-
bine different local similarity outcomes to determine
the similarity between two cases. The application al-
lows the user to track the different tasks of the inter-
vention workflow with its associated attributes while
consulting the case base. In addition, the software
offers the possibility to load/save different attributes
pre-selection. These presets allow clinicians to look
for similarities between cases by just working with
a specific set of attributes or only considering a sin-
gle phase of the workflow, for example for carrying
out patient studies during the pre-operative phase. As
output of the retrieve phase, the CBR engine creates
a distance matrix that depicts the similitude between
the new case and the cases in the case base. This ma-
trix is shown in the results navigator window.
3.4 The Results Navigator
The results navigator window contains a table with
the most similar cases to the current case. The re-
sults table contains some features to enhance decision
support. Thus, clinicians can rearrange the resultant
table to see the most and the least similar cases to the
current case. Also, if the medical staff needs addi-
tional information for decision making, every case of
the case base is linked to its complete clinical history
where clinicians can consult any image or file. Fi-
nally, the results window allows the user to choose the
number of similar cases to the current case to retrieve.
Possibilities include selecting the k-nearest neighbors
or selecting the cases with a similarity degree higher
than a pre-fixed threshold.
One of the most significant advances of using a
CBR engine is that the knowledge database is con-
tinuously updating. Thus, new, revised cases will be
added to the case base for future use. eXiTCDSS has
been developed using the Java language. It is compat-
ible with the Linux and Windows OS.
4 eXiTCDSS SUPPORTS
TRANSCATHETER VALVE
IMPLANTATION
In Transcatheter Aortic Valve Implantation (TAVI)
(Webb and Cribier, 2011), a synthetic valve is trans-
ported to the heart through a small hole made in groin.
This procedure can be compared to that performed
when placing a stent, or performing balloon angio-
plasty. This technique was first developed in Europe,
where it was initially performed in 2002. Since then,
more than 10000 patients have benefited from it and
the results have shown the procedure to be effective
in improving functioning in the patients with severe
aortic stenosis. In the recent years TAVI is assuming
a major role in the routine management of patients
with aortic stenosis and now TAVI is considered the
standard in patients who are not candidates for con-
ventional surgical Aortic Valve Replacement (AVR).
On the basis of almost 10 years of experience TAVI
also appears to be a reasonable option for some opera-
ble, but high-risk patients. Nevertheless considerable
work needs to be done before TAVI is expanded into
lower risk groups.
Next lines describe an example application of the
HEALTHINF2013-InternationalConferenceonHealthInformatics
204
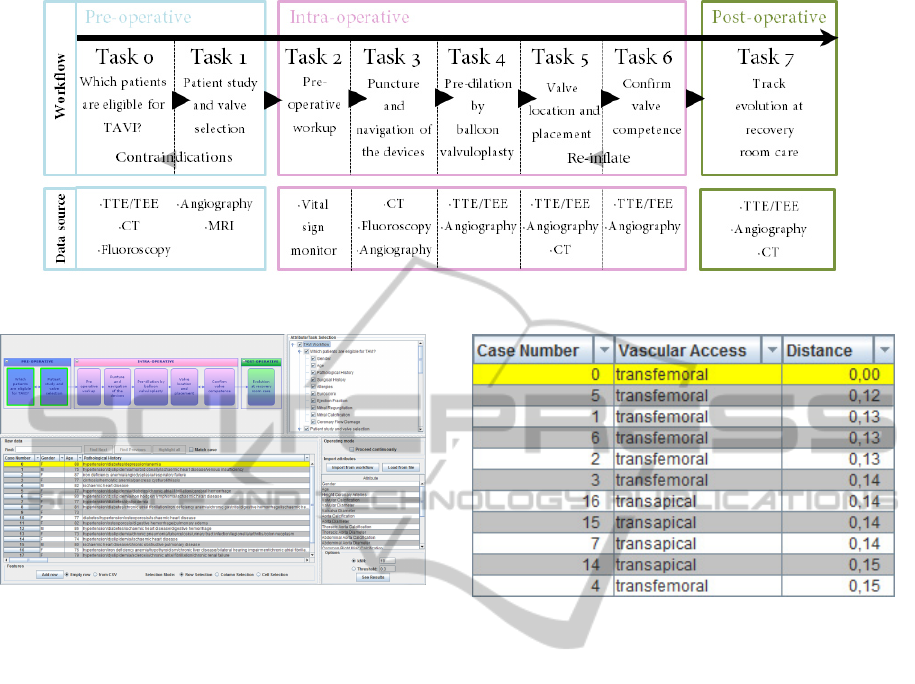
Figure 3: TAVI workflow showing tasks and data source where attributes are extracted from.
Figure 4: The main working window of the eXiTCDSS sup-
port tool.
eXiTCDSS performance. Figure 3 shows the specific
workflow for the TAVI intervention. As can be ap-
preciated, the procedure (from pre-operative to post-
operative treatment) is subdivided in 8 different tasks,
starting with a study of patient suitability for TAVI in
Task 0, to Task 7 where the patient is finally trans-
ferred to the Intensive Care Unit (ICU). Parallel to
the workflow progress, all the tasks are linked with
the different information sources which will provide
the necessary attribute data required for defining the
patient case model. The TAVI workflow together with
the CSV file containing the patient case base are both
loaded into the workflow editor in order to produce
the correspondent XML workflow file. Pre-selected
workmods mentioned in Section 3.3 are available at
this point so the user can load or save a desired selec-
tion of whatever attributes and/or operation tasks he
wishes to receive support from.
For demonstration purposes, the application
shows its capabilities while giving support to a one
particular aspect discussed during Tasks 1 and 2 of
a TAVI intervention, which aims to answer a ba-
sic question: Which access? Nowadays, the most
common approaches in TAVI are the transfemoral,
the transapical, and the subclavian way. These ap-
proaches are selected after studying the patient’s pro-
Figure 5: The table shows an ordered list of similar cases to
the query case 0.
file. The eXiTCDSS support for this demonstration
starts by, from all the attributes list available at Task
1 and 2, selecting those ones considered by clinicians
as the most relevant for deciding the vascular access
(see Figure 4). Next, the case number 0 is selected as
the new query case from a case base of 20 cases. It
is important to remark that, in a real clinical situation,
the vascular access of the query case is not known and
thus, this attribute has not been selected so it remains
unknown for the program. The results offered by the
eXiTCDSS application after the retrieve phase are il-
lustrated in Figure 5. The table depicts the 10 most
similar cases to the query case based on the similarity
distance described in Section 3.3. Also, the vascular
access selected in every case is shown. As can be ap-
preciated, the closest cases to the query case used the
transfemoral approach, the same approach that was
used with the query case. The eXiTCDSS engine re-
trieves similar transfemoral approaches when asked
for a new access way, advising clinicians about which
access way is the best based on similarities with past
patients. Next, experts will be able to study all the
profiles of the retrieved cases or launch another re-
trieve search based on some other attributes.
eXiTCDSS:AFrameworkforaWorkflow-basedCBRforInterventionalCDSS-ApplicationtoTranscatheterAorticValve
Implantation(TAVI)
205

5 CONCLUSIONS
This paper presents eXiTCDSS, a workflow-based
CDSS designed to give case-specific assessment to
clinicians during complex surgery or MISs. The
framework facilitates interaction with physicians,
which are guided along the application in a user-
friendly way. Its workflow structure offers high ver-
satility allowing the clinicians to decide in which
steps of the procedure they wish to receive sup-
port. The tasks and attributes selection can easily
be saved/loaded into independent files for future use.
Although it has been designed to give support to a
wide range of interventions, the eXiTCDSS has been
initially applied to give support to TAVI interven-
tions. The tool has demonstrated its performance giv-
ing support to a specific step of a TAVI procedure with
good results. Current work is focused with improv-
ing the user interface, specially during the OR phase.
Software architecture modifications will provide the
application with voice activation and gesture recog-
nition tools. Finally, the feedback received from the
numerous physicians consulted has been very positive
and the interest showed in this project is encouraging.
Clinicians agree that CDSS are of high value specially
in recently growing MIS like TAVI where the number
of interventions per year is still low compared to com-
mon surgery and which also require expert hands due
to its complex procedure.
ACKNOWLEDGEMENTS
We would like to give our special thanks to the Hos-
pital Clinic of Barcelona, the Centre Hospitalier Uni-
versitaire de Rennes and the Laboratoire Traitement
du Signal et de l’Image from the University of Rennes
for helping us with the case model definition and giv-
ing us example cases of TAVI patients. This work
has been financed by the Spanish Government Com-
mission Ministerio de Industria, Turismo y Comer-
cio (MITyC) under the project PLAN AVANZA 2 la-
beled by Information Technology for European Ad-
vancement 2 (ITEA2).
REFERENCES
Aamodt, A. and Plaza, E. (1994). Case-based reasoning:
Foundational issues, methodological variations, and
system approaches. Artificial Intelligence Communi-
cations, 7:39–52.
Baxt, W. (1995). Application of artificial neural networks
to clinical medicine. Lancet, 346(8983):1135–1138.
Berner, E. (2009). Clinical decision support systems:
State of the art. AHQR publication no. 09-0069-EF,
Agency for Healthcare Research and Quality.
Carayon, P., Karsh, B., Cartmill, C., Hoonakker, P., Hundt,
A., Krueger, D., and Thuemling, T. (2010). Incor-
porating health information technology into workflow
redesign. Technical Report 10-0098-EF, Center for
Quality and Productivity Improvement, University of
Wisconsin-Madison.
Crowley, R., Naus, G., and Friedman, C. (2003). Develop-
ment of visual diagnostic expertise in pathology: An
information processing study. Journal of American
Medical Informatics Association, 10(1):39–51.
Das, M. and Eichner, J. (2010). Challenges and barriers
to clinical decision support design and implementa-
tion experienced in the agency for healthcare research
and quality cds demonstrations. AHQR publication
no. 10-0064-EF, Agency for Healthcare Research and
Quality.
Demmer-Fushman, D. and Lin, J. (2007). Answering
clinical question with knowledge-based and statisti-
cal techniques. In Association for Computational Lin-
guistics, pages 63–103.
Laurikkala, J., Juhola, M., Lammi, S., and Viikki, K.
(1999). Comparion of genetic algorithms and other
classification methods in the diagnosis of female
urinary incontinence. Methods of Information in
Medicine, 38:125–131.
Marakas, G. (1999). Decision support systems in the 21st
century. Prentice Hall, Upper Saddle River, New Jer-
sey.
Patel, V., Kushniruk, A., Yang, S., and Yale, J. (2000). Im-
pact of a computer-based patient record system on
data collection,knowledge organisation, and reason-
ing. Journal of American Medical Informatics Asso-
ciation, 7(6):569–85.
Rinkus, S., Walji, M., Johnson-Throop, K., Malin, J., Tur-
ley, J., and Smith, J. (2004). Human-centerd design of
a distributed knowledge management system. Journal
of Biomedical Informatics, 38:4–17.
Webb, J. and Cribier, A. (2011). Percutaneous transarterial
aortic valve implantation: what do we know? Euro-
pean Heart Journal, 32:140–147.
Wyatt, J. and Spiegelhalter, D. (1991). Field trials of medi-
cal decision-aids: potential problems and solutions. In
15th Symposium on Computer Applications in Medi-
cal Care, pages 3–7, Washington, USA.
HEALTHINF2013-InternationalConferenceonHealthInformatics
206
