
ACTIVITY CREDITING IN
DISTRIBUTED WORKFLOW ENVIRONMENTS
Eric D. Browne, Michael Schrefl, James R. Warren
School of Computer & Information Science
University of South Australia
Keywords:
workflow, adaptive, goal, activity, crediting, health, healthcare, care plans.
Abstract:
Workflow Management Systems (WfMSs) are increasingly being introduced to deal with cooperative inter-
organisational business processes. There are many situations in these distributed workflow environments,
where, for a given business process, activities might be undertaken in one enterprise that overlap with, or re-
peat activities undertaken elsewhere. This paper examines such situations in the context of healthcare, where
duplicated tests and procedures are costly and can have negative health impacts on patients undergoing un-
necessary tests and interventions. Our approach is based on a two-tier goal/process representation of business
processes and an execution model comprising a candidate discovery phase, followed by a component crediting
phase. We introduce the notions of full vs. partial crediting, goal-level vs. activity-level crediting and examine
the role that termporal constraints play in determining candidate components for crediting.
1 INTRODUCTION
Distributed workflow management systems (WfMSs),
where an overall business process is undertaken by a
number of different organisations, can lead to a situa-
tion where similar tasks might be undertaken by dif-
ferent organisations to achieve the same goal or part
thereof. This duplication of services is inefficient, can
lead to delays in achieving the overall goal, and can
impact on the quality of the services being provided.
This is particularly true in healthcare, where unneces-
sary interventions can have tragic consequences. Pa-
tients being managed for one or more chronic condi-
tions, can be particularly prone to such adverse im-
pacts of repeated interventions. A common exam-
ple of this is with the prescription of medications,
whereby several clinicians could be prescribing the
same medication without being aware of similar pre-
scriptions provided by other clinicians, either for the
same, or sometimes for different reasons.
This paper introduces to workflow process mod-
elling the concept of activity crediting, whereby an
activity scheduled to be undertaken somewhere in the
overall workflow, can be credited, either in part or in
full, against a similar activity elsewhere in the work-
flow. Such crediting could be determined to some ex-
tent, at schema definition time, but quite often, with
dynamically created workflows or subworkflows, the
crediting may need to be undertaken at run-time, af-
ter the specific workflow instance has started. The se-
mantics and rules for such crediting can be quite com-
plex, with temporal aspects often playing an impor-
tant role. Temporal deadlines and activity-outcome
time to live parameters need to be taken into consider-
ation when determining the potential for activity cred-
iting to be viable. Another confounder discussed in
this paper is the effect of intermediate tasks on activi-
ties that might be candidates for crediting.
There are also related but disimilar issues to activ-
ity crediting - those of activity discrediting, activity
dependence, and activity conflict, some of which we
also raise in this paper.
2 WORKFLOW in HEALTHCARE
In this section we look at the specific problem we
are trying to address in healthcare, and how our re-
search contributes towards a solution to this problem.
We also introduce the notion of different activity tar-
get objects, which arise in healthcare workflows to a
greater extent than in most other domains. For those
readers unfamiliar with the domain of healthcare, it is
important to appreciate that workflow in this domain,
245
D. Browne E., Schrefl M. and R. Warren J. (2004).
ACTIVITY CREDITING IN DISTRIBUTED WORKFLOW ENVIRONMENTS.
In Proceedings of the Sixth International Conference on Enterprise Information Systems, pages 245-253
DOI: 10.5220/0002631702450253
Copyright
c
SciTePress

is highly complex, varies substantially from case to
case, is subject to many extraneous and unforeseeable
inputs, and decisions are subject to incomplete and
often imprecise data.
2.1 Problem
The motivations for the use of Workflow Management
Systems in healthcare are twofold, firstly to improve
health outcomes for individual patients, and secondly
to make healthcare service provision more efficient.
The primary focus of this paper is to address the dupli-
cation of services that often arise in healthcare service
delivery. Such duplication affects both the quality of
patient care, as well as the efficiency and cost of care
delivery.
2.2 Requirements
Below, are outlined the primary requirements that
need to be considered when addressing the above
problem. Some additional issues related to these re-
quirements, are mentioned at the conclusion to this
paper.
2.2.1 Crediting Scenarios
Our requirements are based on a set of scenarios that
enable crediting to be classified according to the fol-
lowing perspectives:
Full Crediting: Under some circumstances, the cred-
iting of a goal or activity could be complete, in the
sense that the goal or activity could be uncondition-
ally dropped from the overall business process.
Partial Crediting: In many instances, it is unlikely
that the completion of an activity somewhere in a
workflow schema will make another activity com-
pletely redundant. However, the second activity may
need to be modified to take into account the effects of
the first activity. We refer to such compensations as
“partial crediting”. Partial crediting equates to con-
straints being placed on the crediting operations that
modify the workflow schema at runtime. Such con-
straints restrict the validity of the crediting and could
be based on time or on specific events.
Temporary Crediting: Temporary crediting refers to
crediting being conditional upon the respective time
at which similar activities occur. Depending upon
their temporal dispositions, this could lead to one ac-
tivity being cancelled entirely, postponed for some pe-
riod, or foreshortened in duration.
Permanent Crediting: Sometimes, it will be appro-
priate for a goal, activity or data item to be dropped
permanently from the workflow since its enactment
or acquisition has been made redundant by a prior ac-
tion.
2.2.2 Overlapping Tasks
It is important not to eliminate a target task, if its func-
tion overlaps that of the prior crediting or source task.
For example, if a prior task achieves a blood pressure
of 130/80 by, say medication, and a later task aims
to achieve a blood pressure of 135/85 by exercise, it
may be desirable not to credit the first task in order
to eliminate the second, since there may be additional
benefits gained by the exercise task. For the WfMS to
be able to identify such overlaps, there must be suffi-
cient detail expressed explicitly in the task definition,
in this case as a post-condition of the exercise task.
2.2.3 Intervening Tasks
Even though an activity might have been identified
as a candidate for crediting, it is possible that some
intervening task, occuring after the first task, but prior
to the second task in the crediting pair, could cause the
crediting to no longer be valid.
2.2.4 Extraneous State Changes
Similar to the case of intervening tasks invalidat-
ing crediting as just described, we could have situa-
tions where unexpected state changes occur, to any
of workflow state, patient state, environment state or
resource state that similarly invalidate a possible ac-
tivity credit. For example, a patient could be un-
dergoing treatment for diabetes, whereby an exercise
regime to reduce blood pressure credited and allowed
for the skipping of a medication-based hypertension
treatment. If the patient was physically incapacitated
by some accident, then the exercise regime would no
longer be a valid activity for treating hypertension,
and the medication-based treatment might need to be
reinstated into the workflow.
2.2.5 Unwanted Crediting
Unwanted crediting refers to situations whereby it is
undesirable to cancel an activity because it has al-
ready been undertaken somewhere earlier in the work-
flow. For instance, a second opinion on a diagnosis
may be an integral part of a workflow schema, in cases
where it is important to have near certainty before pro-
ceeding down a path. Automatic crediting, and con-
sequential cancelling of such second opinions would
not be wanted or warranted.
2.2.6 Conflict Resolution
Akin to activity crediting is the notion of activity
avoidance, due to potential conflict of outcome. Tra-
ditional WfMSs are unable to deal with such conflicts,
since considerable domain knowledge is required to
ICEIS 2004 - INFORMATION SYSTEMS ANALYSIS AND SPECIFICATION
246

determine potential conflicts. Just like crediting, such
conflicts could be resolved either at the goal level,
or at the level of individual activities. Any facili-
ties provided by an extended WfMS could be utilised
to help resolve a conflict once it has been identified.
E.g. users could be notified and workflow schemas
adapted to help provide a solution. A WfMS could
identify all actors in the healthcare team for a given
patient care plan, and notify each actor through their
appropriate communication channels. An additional
activity could be automatically inserted into the cur-
rent workflow schema to ensure that the conflict is re-
solved to the satisfaction of a nominated actor.
2.2.7 Quality Assurance
It is essential in any healthcare system to ensure that
mistakes are minimized. Any form of activity credit-
ing should be highly conservative, and subject to run-
time validation and manual authorisation by approved
and appropriate clinicians. There should be “break-
glass” emergency exception handling to allow clini-
cians to overide perceived system-based activity cred-
iting. Where crediting has already been approved by
one clinician, such crediting should be made known
to other relevant care providers for that patient.
2.3 Contributions
In this paper we describe mechanisms for eliminating
redundant activities as well as partially crediting the
work achieved by previous activities in a given work-
flow instance. Our contributions include the use of
a two-tier methodology for representing and viewing
business processes, based on separate goal and pro-
cess views, and a two-phase methodology for firstly
discovering, and secondly crediting selected compo-
nents of the overall business process. We call the
first phase candidate discovery, and the second phase
component crediting. We identify two classes of
crediting, namely permanent crediting and temporary
crediting. We also describe a set of still unresolved
issues that need to be addressed for activity crediting
to be supported effectively in the clinical setting.
2.4 Approach Overview
The strategy we have adopted to address the problem
of duplicated services hinges firstly on an approach to
discovering candidate business process components
for crediting and secondly on an approach to manage
the crediting process itself. For candidate discovery,
we utilise a two-tier methodology based on the sepa-
ration of high-level goals from lower-level processes.
For component crediting we adopt a self-modifying
workflow architecture that embeds specific workflow
modification activities into the workflow schema it-
self. These activities make use of dedicated crediting
operators to achieve and manage the component cred-
iting at runtime. In order to support these two aspects,
we introduce a representational model and an execu-
tion model.
3 REPRESENTATIONAL MODEL
The representational model uses a two-tier
goal/process architecture and a library and on-
tology of predefined task definitions as described
below.
3.1 Two-tier Architecture
The two-tier representational model is based on defin-
ing a high-level goal view via a goal hierarchy (see
3.1.1), and a corresponding lower-level process view
via a workflow schema (see 3.1.2). The workflow
schema is derived from the goal hierarchy as de-
scribed by (Browne et al., 2003). These two views
provide for visually representing and interacting with
the workflow for each instance.
3.1.1 Goals
Our approach builds on previous work (Browne et al.,
2003), which introduces a two-tier model, based on
the separation of high level goals from lower level
processes. Although rarely addressed in the con-
text of workflow systems, high level goals have been
used extensively as a basis for Requirements Engi-
neering specification (Dardenne et al., 1993; Jacobs
and Holten, 1995; Gross and Yu, 2001; Mylopoulos
et al., 1999) and have also been discussed extensively
by the authors and proponents of the Asbru clinical
guideline language, (Miksch et al., 1997) who couch
goals in terms of plan intentions. Each activity in a
workflow schema can be associated with the achieve-
ment of one or more high level goals. By decompos-
ing goals into a goal hierarchy whereby the root goal
corresponds to the overall objective of the health care
for the patient, one can often identify and annunciate a
range of ever-more specialised goals, culminating in
goals which can be implemented by known specific
best-practice activities. The goal hierarchy can then
be mapped into a workflow schema for the patient,
using a combination of clinical guidelines and organ-
isational business rules and constraints. It is possible
to identify potential candidates for activity crediting,
even at the goal level.
We will use an example from Non-Insulin Depen-
dent Diabetes Mellitus (NIDDM) management to il-
lustrate a possible goal hierarchy, since diabetes man-
ACTIVITY CREDITING IN DISTRIBUTED WORKFLOW ENVIRONMENTS
247
agement can involve many service providers ( gen-
eral practitioner, diabetes educator, nurse, endocri-
nologist, dietician, opthalmologist, podiatrist) and
many potential activities. Consider the following goal
hierarchy:-
0
G
3
G
4
G
6
G
7
G
1
G
5
G
8
G
8
G
’
9
G
’
10
G
’
2
G
9
G
10
G
manage diabetes
Beta−blocker
therapy therapy
Ace−inhibitor
X
1
manage
hypertension
level
achieve fitness
2
low fat
diet
determine
exercise
regime
exercise
BMI<30
smoking
quit
determine
exercise
regime
exercise
low fat
diet
HBA1c<7%
Figure 1: Goal View for Diabetes Management (simplified).
In fig.1 most goals are achieved by the achieve-
ment of all their immediate child goals, indicated by
a single arc. Alternative goals are indicated by a
double arc, as in goals G
6
(Beta-blocker therapy) and
G
7
(ACE-inhibitor therapy). These two goals are mu-
tually exclusive ( annotated in the figure by an X ),
and are prioritised, such that ACE-inhibitor therapy is
the preferred goal.
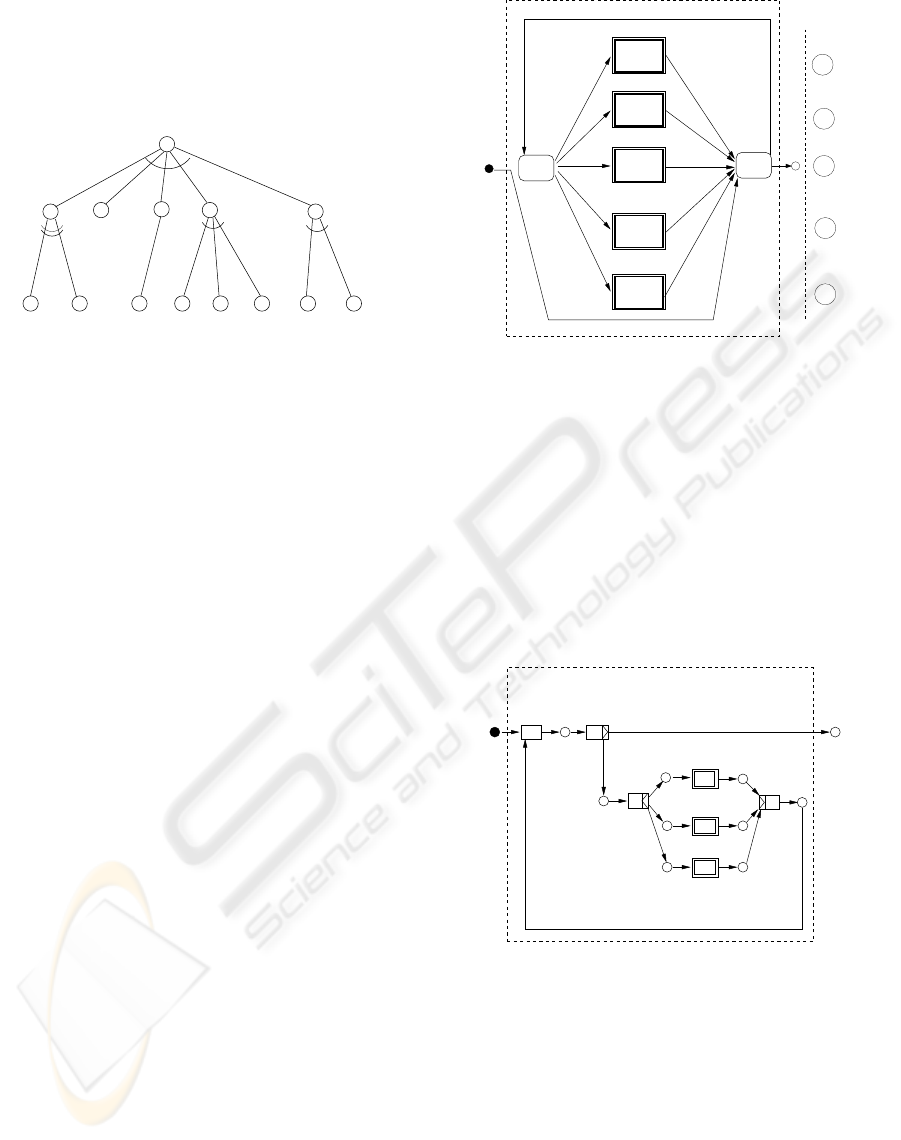
3.1.2 Processes
A process is a set of tasks or activities that achieves a
goal. A process is implemented by a workflow en-
gine that controls the activities, by either invoking
specific activities itself, or placing them on the work-
lists of participants and flagging them as ready to be
undertaken. The ordering of activities in a process
is governed by a workflow schema. Thus, a process
is an enactment of a workflow schema to achieve a
specific goal. Workflows, and thus processes, may
be nested and referred to as subworkflows or subpro-
cesses. Each subprocess is designed to achieve a sub-
goal of the overall objective (root goal) of the goal
hierarchy for that case. Such a process skeleton, de-
rived from the diabetes management goal hierarchy is
shown in fig 2, where each goal corresponding to its
respective process is illustrated on the right-hand side
at the corresponding vertical position in the diagram.
In moving from the goal view to the process view,
we are adding domain, organizational and environ-
ment knowledge in order to elucidate the explicit set
of activities, resources, conditions and control flow
that needs to be applied. Every process P, designed
to achieve a goal G, will have a set of activities A; a
set of one or more objects upon which the process acts
O (described below); a set of edges E that join ac-
tivities, defining temporal dependence (flow) between
activities; an associated set of resources R; achieve-
ment conditions G; and a goal validity time V . i.e.
G
1
G
2
G
3
G
4
G
5
P
5
P
4
P
3
P
2
P
1
BMI<30
GOALS
smoking
START HbA1c < 7%
END
lower BMI
quit smoking
alter
assess
0
P
lower BP
BP < 140/90
quit
achieve
fitness
achieve fitness
lower HbA1c
Figure 2: Process model for Diabetes Management (simpli-
fied).
P is described by the tuple (G, A, E, O, R, V ). G
expresses the boundary conditions on the goal, such
as the achievement level, achievement tolerance, goal
preference, goal priority, etc.
Fig.3 shows the expanded form of subworkflow P
4
of fig.2. This workflow illustrates the 3 processes cor-
responding to the subgoals needed to achieve a lower
Body Mass Index(BMI). The first of these goals, low-
fat diet is also a subgoal of G
3
, lower-HbA1c.
9
P
10
P
A
4ν
A
4δ
8
P
’
assess
START
11
R
12
4
BP < 140/90
END
alter
low−fat
diet
R
exercise−regime
determine
exercise
do
P
Figure 3: Process model for subworkflow P
4
- LowerBMI.
3.1.3 Task Library and Task Classification
In order for activity crediting to be viable, the WfMS
needs to be aware of details of each activity in a
given workflow schema. The best approach, based on
goals as described previously, is for each schema to
be derived from the goal hierarchy, as a set of nested
subworkflows. Each subworkflow corresponding to
a leaf goal is then constructed by assembling appro-
priate activities from a common organisational task
ICEIS 2004 - INFORMATION SYSTEMS ANALYSIS AND SPECIFICATION
248

library. This task library should be built from best-
practice clinical guidelines (Field and Lohr, 1990),
and should vary in scope according to the skills of the
organisation. Tasks are classified according to an in-
formation model of healthcare concepts, so that tasks
to accomplish similar goals are grouped/classified to-
gether. The intention, generic pre-conditions and
generic post-conditions of each task are made explicit
and stored in the task library. Candidates for activ-
ity crediting are then identified by the activity’s path
in the task hierarchy, the activity’s intention, and the
activity’s data pre/post-conditions.
3.1.4 Activity Target Objects
In this section, we introduce the concept of an activity
target object in order, firstly, to support those special
activities in our self-modifying schemas that act on
the workflow schema instance itself to perform cred-
iting, and secondly, to support the necessary temporal
constraints that may be required for crediting.
Workflow models are typically viewed as acting on
a workflow case. Sometimes this case corresponds to
a physical product, such as the production of an air-
craft. Sometimes the case corresponds to a business
service such as an insurance claim, travel booking
or document processing. However, in the healthcare
context, there are often a number of objects, or tar-
gets of a given activity or set of activities that need to
be considered. At the highest level, we are concerned
with providing a healthcare service. The particular
service is often the major objective of the workflow
schema. In this sense, we have two similar process
targets:- the completion of the service, and the im-
proved health of the patient that corresponds to this
service case. The success of the former is often mea-
sured by the quality of service provided, independent
of the patient outcome. The latter is measured by a
change of state of the patient.
However, some parts of the workflow schema may
act on secondary targets. For instance, a patient spec-
imen, preparation of resources such as an operating
theatre, analysis of patient data, analysis of the en-
vironment. An activity could be undertaken which
teaches a carer how to care for a diabetic foot. Here
the target might be regarded as a resource, or even
part of the environment, since the carer may not be a
participant in the usual sense of an initiator of a mod-
elled activity, but merely the recipient of an activity
undertaken by another service provider. Because of
the flexibility required in the healthcare domain, we
even introduce activities that act on the current work-
flow schema itself, in order to adapt the schema for
changed conditions. A corresponding set of state pa-
rameters can be introduced to represent the state of
these different targets at any one time. These are:-
• workflow state, S
W
• patient state, S
P
• environment state, S
E
• resource state, S
R
Workflow state S
W
is further comprised of two com-
ponents,
• control state, S
W c
, representing the workflow be-
haviour, and
• data state, S
W d
The reason for explicitly defining data state, S
W d
is to clearly differentiate information that is a snap-
shot of real, continually changing, physical informa-
tion from the physical information itself. For in-
stance, a patient’s blood pressure continually changes
with time, whereas recorded blood pressure is a dis-
crete set of zero or more values taken at specific in-
stances of time. Theoretically, we can measure a pa-
tient’s blood pressure at any future time t, but we may
only have access to a small set of readings from the
past, and may be unable to determine what the blood
pressure was at any given moment in the past. Thus,
a workflow data variable can be represented by a set
of tuples, where any one s ∈ S
W d
can be expressed
as s = (n, d, a, v
s
, v
e
), where n is the name of the
state variable, d is the data value, a is the workflow
activity that acquired or set this data value, v
s
is the
time at which data value became valid, and v
e
is the
time for which the data value is no longer valid. Thus
v
e
−v
s
represents the validity duration or time-to-live
of the data value. Some temporal databases (Snod-
grass and Ahn, 1985) only capture the start validity
timestamp, assuming that updates to the data variable
will automatically define the end of the previous va-
lidity time. In healthcare, we often have data being
contributed from different sources whereby it is possi-
ble to have overlapping validity timestamps entering a
shared repository. Many temporal databases also cap-
ture transaction time. In the healthcare context, we
assume that all data is implicitely timestamped with
its transaction time as would normally occur in patient
Electronic Health Record (EHR) repositories. Some
EHR-based systems may capture additional metadata
regarding each data variable, such as the accuracy;
the clinician’s confidence in the value; a reference to
the clinician who was responsible for this value of the
data for a given activity.
Thus an activity target object O can be any one ele-
ment of the set {C, P, W, E, R} where C is the work-
flow case, P is the patient, W is the workflow schema,
E is the environment, R is the set of resources in-
volved in the case.
Healthcare activities are often categorised into In-
vestigations/Observations, Evaluations/Assessments
and Interventions/Treatments. From our definitions
of state above, we can say that Investigations mea-
sure patient state (S
P
) in order to change workflow
ACTIVITY CREDITING IN DISTRIBUTED WORKFLOW ENVIRONMENTS
249

data state (S
W d
); Assessments change S
W d
, often
by temporal, spacial and other algorithms applied to
prior values from S
W d
; Interventions are intended to
change patient state (S
P
).
4 EXECUTION MODEL
The two-phase execution model consists of a candi-
date discovery phase followed by a component cred-
iting phase. These two phases are invoked at the com-
mencement of the execution of each case, and when-
ever a change occurs to the status of any of the com-
ponents identified by the candidate discovery phase
as being involved in potential crediting.
4.1 Candidate Discovery Phase
Synergy refers to the similarity between two or more
concepts. Workflow crediting aims at determining
which elements of a business process are highly syn-
ergistic, and therefore candidates for crediting. We
identify three types of components for which synergy
can occur, namely those of goals, activities and data.
A goal, activity or data variable has a high degree of
synergy with another, if it contributes in a similar way
to the overall objective of the business process. Tax-
onomies or classifications of concepts are important
for the determination of synergy.
Before detailing the mechanism for candidate dis-
covery, we first examine how goal discovery is un-
dertaken using our goal-level representational model,
whilst activity and data discovery are undertaken at
the process-level.
Goal-level Matching refers to the identification of
duplicate goals in a goal hierarchy for a specific
healthcare service. Such goal hierarchies might be
quite extensive in the treatment and/or management
of chronic conditions, especially where comorbidi-
ties i.e. several concurrent conditions exist. Subpro-
cesses (sets of activities) that would normally be en-
acted to achieve alternative or duplicated goals would
be candidates for dropping or bypasssing in the over-
all workflow schema. Goal-level crediting allows lo-
calisation of modifications to specific areas of the
workflow schema, minimising the overhead and side-
effects of schema modification.
Process-level Matching refers to the identification of
particular activities or redundant activity data items
(state variables) that might be collected by different
activities in the overall workflow. It is not sufficient to
simply use the name of the activity as a means of iden-
tifying where such redundancies might occur. Many
activities in healthcare are aimed at assessing or deter-
mining patient state variables, such as blood pressure,
weight, blood lipid levels, etc. Many tasks could have
the determination of these variables as either a direct
or indirect target of the activity.
Candidate components for crediting are determined
firstly by a goal-space search of the goal-hierarchy
for matching goals. This is undertaken by follow-
ing each path of the directed acyclic graph, from the
root, to all leaves. Duplicate candidates are identified
by the name of the goal and are further matched by
their target achievement level. Temporal conditions
are checked using the prescribed validity times asso-
ciated with each goal. Once completed, if candidates
are found, then these are placed on a candidate list for
later processing. Mutually exclusive activities ( alter-
natives ) are checked, and if any in an alternative set
has been commenced, then the remainder of the set is
placed on the candidate list.
Next, the corresponding workflow schema is
searched for synergistic activities. These are identi-
fied by the name and position in the task library of
the template task used to create each activity. Any
candidate activities are also placed on the list. Next,
a search for data in activity post-conditions is under-
taken to determine activities which collect or set iden-
tical data variables.
Finally, the candidate list is passed to the compo-
nent crediting phase, which undertakes the crediting
as described next.
4.2 Component Crediting Phase
Self-modifying Workflow: Activity crediting re-
quires operators to support instance-level adaptation
of workflow schemas, together with the coopera-
tive interaction of healthcare participants. To sup-
port the required level of flexibility, we extend upon
work (Browne et al., 2004) which introduces explicit
schema modification tasks into workflow models of
healthcare to ensure and facilitate the adaptation and
modification of an abstract workflow schema at run-
time for each patient case. Such activities are de-
signed to change workflow state S
W
(both S
W d
and
S
W c
), resulting in additional activities, altered activ-
ities, replaced activities, deleted activities or altered
flow. As such, these modification activities differ
from conventional activities in that they act on their
own workflow schema instance as the target object of
the activity - hence the label, self-modifying. Con-
siderable research, e.g. by (Ellis et al., 1995; Re-
ichert and Dadam, 1998; Sadiq and Mangan, 2002;
Manolescu and Johnson, 1999) and many others has
formed the basis for much of the ideas leading to the
concept of self-modifying workflow.
Every goal in the goal hierarchy has a correspond-
ing workflow process in the workflow schema, such
that the goal hierarchy maps to a nested set of sub-
workflows. Each subworkflow contains a goal assess-
ment activity (assess) and a workflow alteration ac-
ICEIS 2004 - INFORMATION SYSTEMS ANALYSIS AND SPECIFICATION
250
tivity (alter). Component crediting is implemented
by crediting operators, which are activity methods of
the top-level alter activity (refer fig. 2), or in a sim-
ilar alter activity in one of the subworkflows (e.g.
within P
1
...P
5
of the same figure). These alter ac-
tivities have the workflow schema itself as the target
object of the activity, rather than the patient, a re-
source, or the environment. A crediting workflow ac-
tivity is invoked as part of each alter task and placed
on the worklist of users who belong to the crediting
role. Any candidate goals, activities or data variables
are presented to the creditor for acceptance, if they
correspond to the goal/subworkflow that is currently
being executed. If the change is accepted by the cred-
itor, then the corresponding crediting operator is used
to apply the change to the running workflow schema,
and to the goal hierarchy if appropriate.
Crediting operators refer to the set of workflow
modification operators that play a part in any form
of crediting. They are intended to alter the workflow
schema, downstream of current activities, and do so
by bypassing, adding, deleting, replacing or altering
activities. Altering of activities may mean adding,
deleting, replacing or changing data parameters of ac-
tivities, specified as either pre- or post-conditions of
the activity. We have identified the following work-
flow modification operators which specifically ad-
dress changes to workflow schemas where one activ-
ity in the schema can be identified as providing some
functionality similar to that of another activity in the
same schema. These operators can be expressed as an
ACTI VETFL (M
¨
uller, 2002) formula, where appropri-
ate, utilising the temporal semantics available therein
to conditionally apply a change to a schema, either by
restricting the change to apply for some duration only,
or in response to a specified event. Thus changes to
the workflow can be specified as either permanent or
temporary. Temporary operators, in turn, may need to
credit, or uncredit a workflow component, and cred-
iting can be done conditionally where the temporal
constraint is known at the time of crediting, or else un-
conditionally, in which case a corresponding uncredit
component is required. Temporal constraints are the
most likely candidates to influence the viability of ac-
tivity crediting. We need to tag certain state measure-
ments and state changes with their validity time, or
else have a mechanism by which the workflow engine
can obtain this information generically from clinical
knowledge. Pre-conditions for activities will often be
specified in terms of predicates on state variables. E.g.
“if patient blood pressure is greater than 150/90mm
Hg, then ..”. If the patient’s blood pressure has al-
ready been measured by a previous activity, then not
only does this need to be known, for activity crediting
to be possible, but also, both the time of last record-
ing, as well as the validity time, need to be known.
Here is a summary of the crediting operators
supported:-
• disableGoal: disable a goal in the goal hierarchy,
such that the corresponding workflow process is
not undertaken. Goals are identified by their ab-
solute path in the goal hierarchy, e.g.
disableGoal(ManageDiabetes/BM Ilt30/lowF atDiet)
• enableGoal: (re)enable a goal in the goal hierar-
chy. A goal may need to be reinstated if the cred-
iting goal is not achieved, or if extraneous state
changes cause a service provider to deem it desir-
able to reachieve the goal.
• deleteGoal: delete a goal from the goal hierarchy,
such that the corresponding workflow process is re-
moved and no longer undertaken.
• skipActivity: skip an activity from the current
schema instance, for some or all of the remaining
execution of the current case. The following rule:
W HEN completed(A
1
)
T HEN skipActivity(A
2
)
V ALID−T IME[now,now+(7,day)],
states that activity A
2
should be skipped for 7 days
on the completion of activity A
1
.
• restoreActivity: remove the bypass from a skipped
activity.
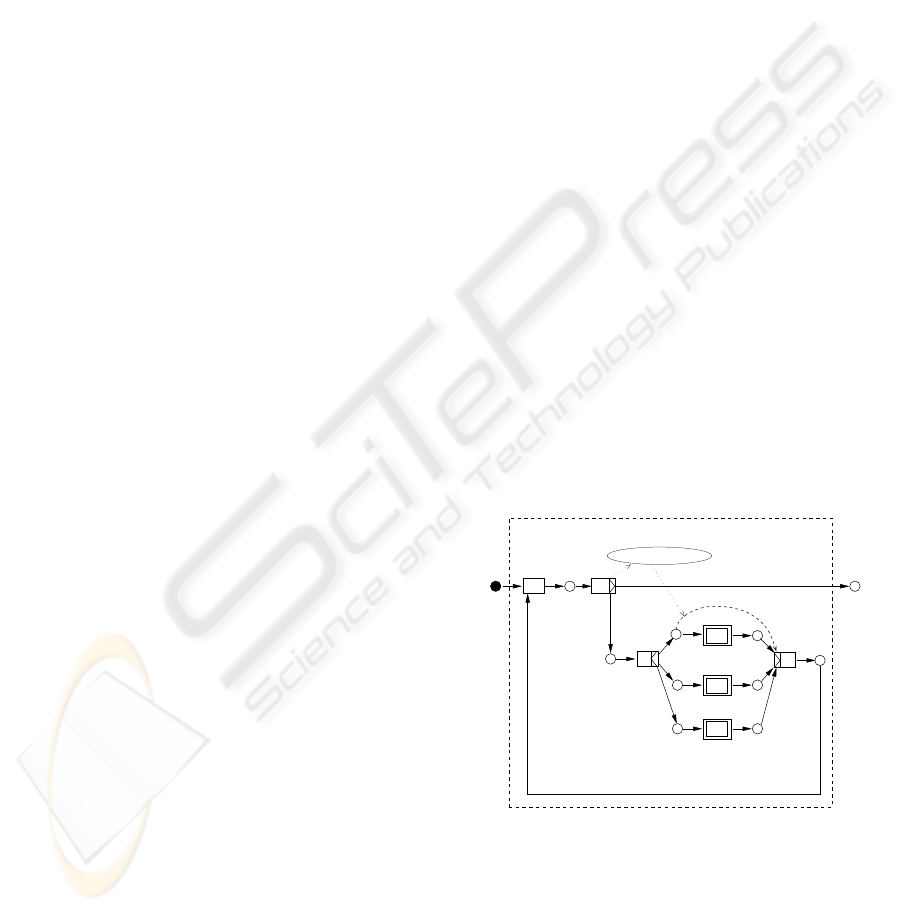
• skipConcurrentActivity is a specialisation of
skipActivity, which bypasses a path from a con-
current path set. This operator is illustrated in
fig.4, being used to credit (skip) the low-fat diet
subworkflow.
9
P
10
P
A
4ν
A
4δ
8
P
’
assess
START
11
R
12
P
4
BP < 140/90
END
alter
low−fat
diet
determine
exercise−regime
do
exercise
R
skipConcurrentActivity
Figure 4: applying a crediting operator to skip lowfat diet
• restoreConcurrentActivity: remove the bypass
from a skipped activity belonging to a set of con-
current activities.
• skipChoiceActivity is a specialisation of skipActiv-
ity, which bypasses a path from an exclusive-OR
(choice) path set. If this operator is temporally
ACTIVITY CREDITING IN DISTRIBUTED WORKFLOW ENVIRONMENTS
251

constrained, it may need to be reinstated at a later
date/time. E.g.
skipChoiceActivity(A
2
)
Unless hypertensive(P ) V ALID−T IME now,
The above formula states that activity A
2
should be
skipped unless patient P has become hypertensive.
• restoreChoiceActivity: remove the bypass from a
skipped activity belonging to a set of alternative ac-
tivities.
• deleteActivity: delete a named activity from the
workflow schema for this case.
• deletePostcondition: delete a data item required as
an output of a specific activity. e.g.
deleteP ostcondition(A,parameter=BP ),
where A is the activity, and parameter = BP
represents the requirement to collect the patient’s
blood pressure through this activity.
• addPostcondition: add a data item required as an
output of an activity.
• addTempPostcondition: temporarily add a data
item required as an output of an activity.
• deleteTempPostcondition: temporarily remove a
data item required as an output of an activity.
• alterPostcondition: alter a postcondition on an ac-
tivity.
• disablePrecondition: disable a precondition on an
activity.
• enablePrecondition: enable a precondition on an
activity.
• alterPrecondition: alter a precondition on an activ-
ity. This might be used, for example to relax or fur-
ther constrain a data value, required for a particular
activity. e.g.
alterP recondition(A,parameter=BP,
condition=
00
BP >140/85
00
)
5 IMPLEMENTATION
Activity crediting relies on participants’ understand-
ing of the entire care process or workflow schema for
each patient. Good process monitoring tools are es-
sential for this understanding, and for each activity,
or change in workflow, a snapshot of the case, includ-
ing rationale for any changes, needs to be available to
all relevant participants. An annotated runtime view
of the goal hierarchy can be presented to clinicians
as a synoptic view of the case, showing which goals
have been achieved, supplemented with times and du-
rations.
We have based our implementation methodol-
ogy on a prototype workflow engine that ex-
tends several of The Workflow Management Coali-
tion’s Application Programming Interfaces (API)
(Fischer, 2001), by providing support for goal
views through a Goal Definition Language and
Goal to Process Transformer. We provide sup-
port for runtime workflow schema alteration through
Event/Condition/Action (ECA) rules similar to those
developed for the ACTI VETFL framework used in the
workflow management system AG ENTWORK WfMS
(M
¨
uller, 2002). AGEN TWORK has been applied in
HE MATOWORK(Universit
¨
at Leipzig, 2003) for the
management of hemato-oncology, which covers the
diagnosis, therapy and follow-up of cancer patients
suffering diseases of the hematological and lymphatic
node system.
6 CONCLUSION
In this paper, we have outlined the requirements, and
introduced a methodology for addressing the dupli-
cation of services that might occur in business pro-
cesses in complex domains such as healthcare. We
are currently implementing this approach in a proto-
type WfMS being developed specifically to support
goal-based flexible workflow schemas.
Several other issues should be considered when im-
plementing activity crediting mechanisms in practice.
These include cost implications and resource recov-
ery. When crediting one activity against the other, for
partial or complete elimination of one activity from
the workflow, it may be important to compare the cost
of each activity, and to consider this in determining
which activity might be (partially) skipped. The ef-
ficiency motivation for activity crediting is premised
on the saving of resources. Any recovery of resources
no longer required to service activities that have been
credited, should itself be handled efficiently to maxi-
mize the advantage of such recovery.
ACKNOWLEDGEMENTS
This work is supported by Australian Research Coun-
cil SPIRT (Strategic Partnership with Industry Re-
search and Training) grant C00107117 in partnership
with the South Australian Department of Human Ser-
vices.
REFERENCES
Browne, E., Schrefl, M., and Warren, J. (2003). A two
tier, goal-driven workflow model for the healthcare
ICEIS 2004 - INFORMATION SYSTEMS ANALYSIS AND SPECIFICATION
252

domain. In 5th International Conference on Enter-
prise Information Systems.
Browne, E., Schrefl, M., and Warren, J. (2004). Goal-
focused self-modifying workflow in the healthcare do-
main. In 37th Hawaii International Conference on
System Sciences (HICSS37). to appear.
Dardenne, A., van Lamsweerde, A., and Fickas, S. (1993).
Goal-directed requirements acquisition. Science of
Computer Programming, 20(1-2):3–50.
Ellis, C., Kling, R., Mylopoulos, J., and Kaplan, S., ed-
itors (1995). Dynamic change within workflow sys-
tems, Milpitas, California. ACM SIGOIS, ACM Press,
New York.
Field, M. and Lohr, K., editors (1990). Clinical Practice
Guidelines: Directions for a New Program. National
Academic Press, Washington, DC.
Fischer, L. (2001). Workflow handbook 2001. Technical
report, Workflow Management Coalition (WfMC).
Gross, D. and Yu, E. (2001). Evolving system archi-
tecture to meet changing business goals: an agent
and goal-oriented approach. In ICSE-2001 Work-
shop: From Software Requirements to Architectures
(STRAW2001), pages 13–21, Toronto, Canada.
Jacobs, S. and Holten, R. (1995). Goal-driven business
modelling: Supporting decision-making within in-
formation systems development. Technical report,
RWTH, Aachen.
Manolescu, D.-A. and Johnson, R. E. (1999). Dynamic ob-
ject model and adaptive workflow. OOPSLA’99 Meta-
data and Active Object-Model Pattern Mining Work-
shop.
Miksch, S., Shahar, Y., and Johnson, P. (1997). Asbru: A
task-specific, intention-based, and time-oriented lan-
guage for representing skeletal plans. In 7th Workshop
on Knowledge Engineering: Methods & Languages
(KEML-97), Milton Keynes, UK.
M
¨
uller (2002). Event-Oriented Dynamic Adaptation of
Workflows: Model, Architecture, and Implementation.
PhD thesis, Fakult
¨
at f
¨
ur Mathematik und Informatik
der Universit
¨
at Leipzig.
Mylopoulos, J., Chung, L., and Yu, E. (1999). From object-
oriented to goal-oriented requirements analysis. Com-
munications of the ACM, 42(1):31–37.
Reichert, M. and Dadam, P. (1998). ADEPT flex -
supporting dynamic changes of workflows without
losing control. Journal of Intelligent Information Sys-
tems, 10(2):93–129.
Sadiq, S. and Mangan, P. (2002). On building work-
flow models for flexible processes. In Thirteenth
Australasian Database Conference, volume 5, Mel-
bourne, Australia. Australian Computer Society, Inc.
Snodgrass, R. and Ahn, I. (1985). A taxonomy of time
databases. In Proceedings of the 1985 ACM SIG-
MOD international conference on Management of
data, pages 236–246.
Universit
¨
at Leipzig (2003). Hematowork: A work-
flow system for protocol-directed care in
distributed hemato-oncology. http://dbs.uni-
leipzig.de/de/Research/hemato.html.
ACTIVITY CREDITING IN DISTRIBUTED WORKFLOW ENVIRONMENTS
253
