
Evaluation of the Adaptive Statistical Iterative Reconstruction
Algorithm in Chest CT (Computed Tomography)
A Preliminary Study toward Its Employment in Low Dose Applications,
Also in Conjunction with CAD (Computer Aided Detection)
Patrizio Barca
1,2,3
, Federica Palmas
1,3
, Maria Evelina Fantacci
1,3
and Davide Caramella
4
1
Department of Physics, University of Pisa, Pisa, Italy
2
Unit of Medical Physics, Pisa University Hospital “Azienda Ospedaliero-Universitaria Pisana”, Pisa, Italy
3
INFN, Pisa Section, Pisa, Italy
4
Department of Radiology, Pisa University Hospital “Azienda Ospedaliero-Universitaria Pisana”, Pisa, Italy
Keywords: Chest Computed Tomography, Image Quality, Modulation Transfer Function, Noise Power Spectrum,
Contrast.
Abstract: Lung cancer is one of the leading cause of cancer death worldwide. Computed Tomography (CT) is the best
imaging modality for the detection of small pulmonary nodules and for this reason its employment as a
screening tool has been widely studied. However, radiation dose delivered in a chest CT examination must
be considered, especially when potentially healthy people are examined in screening programs. In this
context, iterative reconstruction (IR) algorithms have shown the potential to reduce image noise and
radiation dose and computer aided detection (CAD) systems can be employed for supporting radiologists.
Thus, the combined use of IR algorithms and CAD systems can be of practical interest. In this preliminary
work we studied the potential improvements in the quality of phantom and clinical chest images
reconstructed trough the Adaptive Statistical Iterative Reconstruction (ASIR, GE Healthcare, Waukesha,
WI, USA) algorithm, in order to evaluate a possible employment of this algorithm in low dose chest CT
imaging with CAD analysis. We analysed both clinical and phantom CT images. Noise, noise power
spectrum (NPS) and modulation transfer function (MTF) were estimated for different inserts in the phantom
images. Image contrast and contrast-to-noise ratio (CNR) of different nodules contained in clinical chest
images were evaluated. Noise decreases non-linearly when increasing the ASIR blending level of
reconstruction. ASIR modified the NPS. The MTF for ASIR-reconstructed images depended on tube load,
contrast and blending level. Both image contrast and CNR increased with the ASIR blending level.
1 INTRODUCTION
Lung cancer is one of the most frequently diagnosed
cancers and the leading causes of cancer death in
men worldwide (Malvezzi et al., 2015; Siegel et al.,
2015). In fact, most of lung cancer cases are
diagnosed in the late stages when the survival rate is
very low. An early detection considerably improves
the survival rate and for this reason the
implementation of screening programs is of relevant
interest. The best diagnostic tool for the detection of
pulmonary nodules is Computed Tomography (CT)
and its employment in screening trials has shown
great results in terms of reduced mortality (The
National Lung Screening Trial Research Team,
2011). An additional tool that can be helpful in lung
cancer screening is represented by computer aided
detection (CAD) systems. In fact, many studies have
shown satisfactory results in terms of sensitivity and
specificity (Lopez Torres et al., 2015; Fantacci et al.,
2017), so as CAD systems can be employed to
reduce radiologist workload and improving the
quality of chest CT scan interpretation in screening
examinations. However, in order to minimise the
risk of radiation induced cancer in patients
(potentially healthy in screening examinations) low-
dose CT is required. Recent advances in CT
technology include different methods of dose
optimisation and reduction (Goo, 2012). In
particular, iterative reconstruction algorithms (IR)
show the potential of improving image quality in
low-dose image acquisitions as compared to
Barca P., Palmas F., Fantacci M. and Caramella D.
Evaluation of the Adaptive Statistical Iterative Reconstruction Algorithm in Chest CT (Computed Tomography) - A Preliminary Study toward Its Employment in Low Dose Applications, Also in
Conjunction with CAD (Computer Aided Detection).
DOI: 10.5220/0006750706880694
In Proceedings of the 11th International Joint Conference on Biomedical Engineering Systems and Technologies (HEALTHINF 2018), pages 688-694
ISBN: 978-989-758-281-3
Copyright
c
2018 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

standard filtered back-projection (FBP)
reconstruction (Willemink et al., 2013). Therefore,
IR algorithms could be employed in low-dose CT
examinations preserving the diagnostic quality of
images (which conversely is degraded when FBP
reconstruction is adopted). For this reason, recent
works were focused on combining IR methods with
CAD systems (Huber et al., 2016; Yoon et al., 2015;
Wielpütz et al., 2015; Harder et al., 2016). These
studies showed that in many clinical situations low-
dose chest CT with IR algorithms does not
significantly worsen the CAD sensitivity obtained
with standard chest CT and conventional FBP
reconstruction. However, some studies have shown
that image quality obtained through iterative
reconstruction depends on image contrast and
radiation dose (Richard et al., 2012; Samei et al.,
2015). Thus, more insights on the performance of IR
algorithms for chest examinations can be of practical
interest.
In a previous phantom study, we assessed the
image quality performance of a CT scanner (Optima
CT660, GE Healthcare, Waukesha, WI, USA) which
implements the Adaptive Statistical Iterative
Reconstruction (ASIR, GE Healthcare, Waukesha,
WI, USA) algorithm (Barca et al., 2017). We
performed a systematic analysis of noise, contrast-
to-noise ratio (CNR) and spatial resolution by
varying the main exposure parameters in a wide
range of values and testing the ASIR’s performance
on different image contrasts. We demonstrated that a
relevant noise reduction and CNR increment in CT
images can be achieved with the ASIR algorithm
with respect to the conventional FBP reconstruction.
Additionally, spatial resolution decreases with
increasing the ASIR blending level of reconstruction
for low dose acquisitions and low contrast objects.
However, only a quality control protocol was
adopted in image acquisition without any clinical
and only phantom images were analysed.
In this study, we investigate potential strengths
of the ASIR algorithm in terms of image quality that
could be of practical interest in conjunction with
lung CAD system at low and very low radiation
exposure levels. We study the dependence of
different image quality parameters on the ASIR-FBP
blending level of reconstruction, both in phantom
and clinical chest images. The analysis performed in
the previous work was repeated to characterise the
quality of images obtained through ASIR in a 128-
slice CT scanner (Discovery 750 HD, GE
Healthcare, Waukesha, WI, USA). However, while
in the previous study images were acquired through
scan protocols often used in quality controls, in this
analysis we employed a clinical chest scan protocol
to acquire the phantom images. Then, we focused
our attention on clinical chest acquisitions of
patients with pulmonary nodules, whose images
were retrospectively reconstructed using different
ASIR-FBP blending levels; we studied noise and
contrast properties of these images in order to
evaluate the employment of ASIR and its effect on
nodule detectability.
2 MATERIALS AND METHODS
Images of the Catphan-504 phantom (The Phantom
Laboratory, NY, USA) were acquired on the
Discovery 750-HD CT using a scan protocol
routinely adopted in chest CT examinations (Table
1) and varying the main exposure parameters in a
wide range of values (Specifically, four values of
tube voltage and eight values of tube load were
employed: 80, 100, 120 and 140 kVp, 32
1
, 63, 84,
105, 126, 147, 168, 189 mAs). The Catphan-504
phantom is composed of 4 modules with cylindrical
shape (internal diameter of 15 cm). We employed
the CTP486 module (a homogeneous water-
equivalent module) and the CTP404 module
(composed of many inserts of different materials in a
water-equivalent background).
Image quality was evaluated through the
assessment of noise, noise power spectrum (NPS)
and modulation transfer function (MTF).
Noise and NPS were computed from images of
the CTP486 phantom section while for MTF
assessment we employed images of the CTP404
phantom section.
Noise was measured by computing the standard
deviation (σ) of Hounsfield units (HU) within a
region of interest (ROI), while for the NPS
assessment we adopted the Siewerdsen et al.
approach: we computed the 3D NPS and then we
obtain a radial representation of the NPS by
selecting the f
z
=0 plane of the 3D NPS and
performing an average of several radial profiles.
The MTFs were derived following the circular
edge method through edge spread function (ESF)
measurements (Richard et al., 2012; Samei et al.,
2015). ESFs were referred to six different inserts of
the CTP404 section (air, PMP, LDPE, polystyrene,
1
In order to evaluate the spatial resolution performance of
the ASIR algorithm at low radiation exposure, a set of
images of the CTP404 section were acquired at 32 mAs
(lowest value used in our analysis). This value was only
employed for MTF evaluation.
delrin and teflon).
Additionally, images of patients that underwent
chest CT clinical examinations were anonymised
and retrospectively reconstructed
2
using different
ASIR-FBP blending levels (from 20% to 100%). In
these images, nodules of different sizes (4 mm to 7
mm) were identified, then, the CNR and the
percentage contrast were computed. The CNR was
estimated as follows:
2
nodule background
2
nodule background
HU HU
CNR =
σ + σ
(1)
where HU
nodule
/σ
nodule
and HU
background
/σ
background
are
the mean/standard deviation of HU values in a
circular ROI in the considered nodule and
background region. The percentage contrast was
defined by the following formula:
%100%
nodule background
background
HU HU
C( ) =
HU
(2)
Uncertainties associated to data values were
computed as standard deviations of repeated
measurements. For some measurements this
approach was not possible (e.g. for contrast analysis
in clinical images). However, we tested the
reproducibility of our measurements adopting the
clinical chest scan protocol and computing the
coefficient of variation (COV) from a set of ten
acquisitions. The COV resulted <0.03 for each
ASIR-FBP blending level employed in the
reconstruction process.
Image data analysis was performed using ImageJ
(Wayne Rasband, National Institute of Health, USA)
and Matlab (The MathWorks, Inc., USA) software
packages.
Table 1: Standard chest scan protocol routinely adopted in
the Discovery 750-HD CT machine for chest
examinations.
Scan protocol standard ches
t
Modality helical
Tube load 126 mAs
Tube voltage 100 -120
*
kVp
Pitch 0.984:1
Slice thickness 2.5 mm
S-FOV M Body
D-FOV 220 mm
Collimation width 40 mm
*
The kVp value could be set to 100 kVp or 120 kVp depending on
the patient size.
3 RESULTS
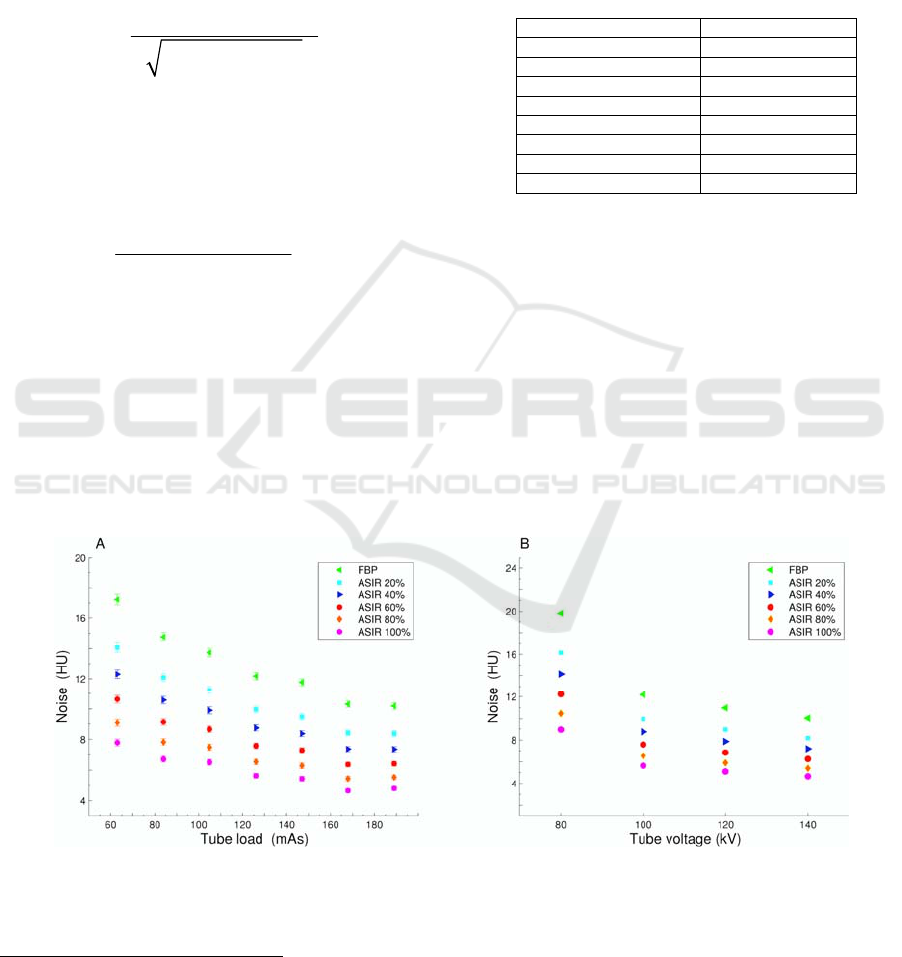
Figure 1 shows the noise obtained varying tube load
and tube voltage for conventional FBP algorithm
and ASIR with different blending levels of
reconstruction (20%, 40%, 60%, 80%, 100%). Noise
decreased non-linearly with the increase of ASIR
blending level of reconstruction as well as with
increasing tube load and tube voltage.
Figure 1: Noise (standard deviation) for conventional FBP algorithm and different ASIR blending levels of reconstruction
(20%, 40%, 60%, 80%, 100%) with varying tube load (panel A) and tube voltage (panel B). Other parameters of acquisition
were set as in Table 1.
2
These images were acquired with the standard chest
protocol (Table 1) and first reconstructed with FBP.
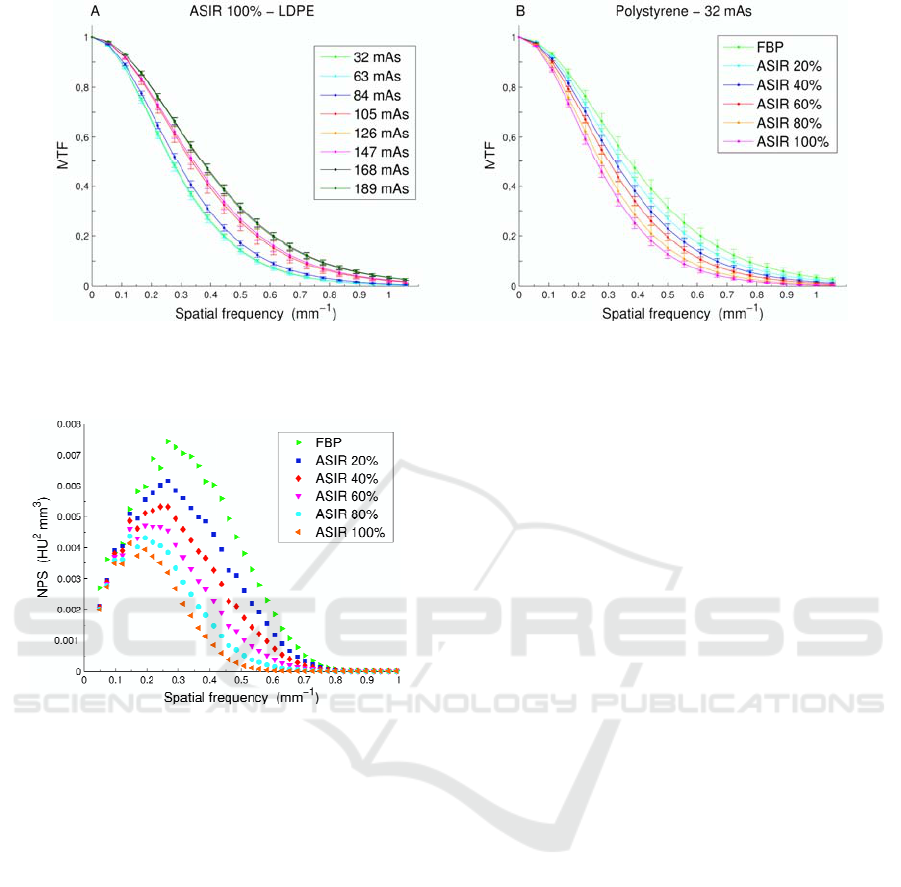
Figure 3: MTF for ASIR-reconstructed CT images (blending level of 100%) and medium-low (LDPE) contrast level, with
varying tube load (panel A). MTF for low (32 mAs) tube load and low (polystyrene) contrast CT images, with varying
reconstruction methods.
Figure 2: Radial NPS for conventional FBP algorithm and
ASIR algorithm with different blending levels of
reconstruction. Images were acquired adopting the chest
scan protocol of Table 1.
Results about NPS are reported in Figure 2.
ASIR algorithm acts as a low pass filter whose effect
increases with the increase of blending level of
reconstruction.
Results about spatial resolution are reported in
Figures 3 and 4. For ASIR-reconstructed CT images
and low contrast level, the MTF decreased with
decreasing tube load (Fig. 3 A). The MTF of ASIR-
reconstructed CT images varied even with the
contrast level (Fig. 4), especially at low tube load. In
particular, the MTF decreased with decreasing
contrast level. While for high contrast objects or
high tube load values ASIR preserves the spatial
resolution obtained by FBP reconstruction, for
medium (e.g. 126 mAs, which is the value adopted
in the standard chest protocol on the Discovery 750-
HD CT) and low (e.g. 32 mAs, the lowest value that
was employed in our study) tube load and contrast
level, the MTF of ASIR-reconstructed CT images
was lower than the MTF of conventional FBP-
reconstructed images, and the first decreased with
increasing blending level of reconstruction (Fig. 3
B).
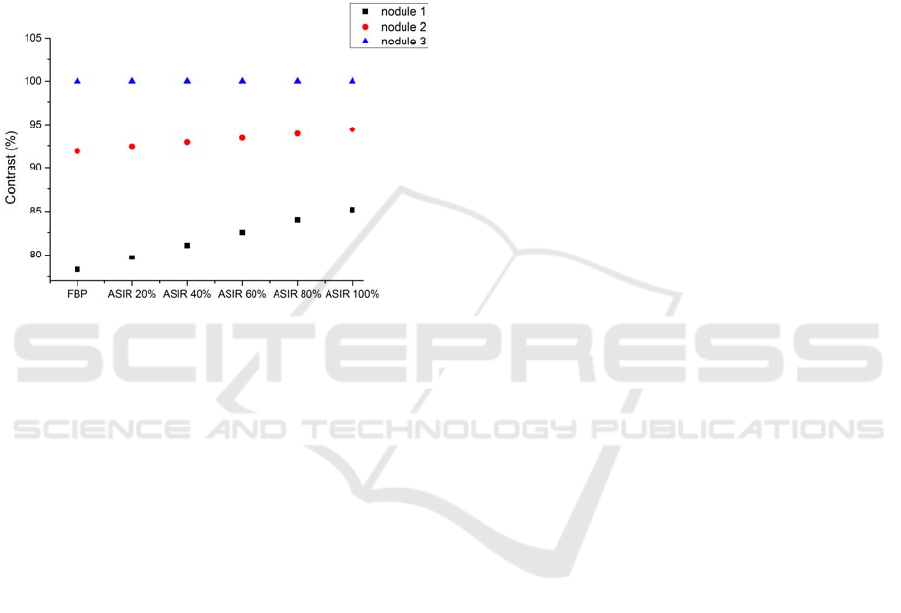
Figure 5 shows one example of clinical image
containing a nodule of 5 mm. Examples of the CNR
and percentage contrast results are reported in
Figures 6 and 7 for nodules of 4, 5 and 6 mm of
diameter. CNR and percentage contrast of the
nodules increased non-linearly with increasing the
ASIR level of reconstruction (up to 43% and 9%
respectively).
4 DISCUSSIONS
In this study we evaluated CT image quality through
the assessment of different indexes related to noise
(noise and NPS), contrast (CNR and percentage
contrast) and spatial resolution (MTF) properties of
phantom and clinical images, comparing the
performance of two different reconstruction
technologies.
As expected, our findings confirm the noise
reduction potential of the ASIR algorithm.
Specifically, when compared to FBP, ASIR can
reduce image noise up to 55 % (Figure 1), showing
the potential of image quality improvement at low
radiation exposures. Furthermore, it seems that
ASIR acts as a non-linear low-pass filter, which can
modify noise texture and affect spatial resolution
especially at low contrast and low radiation exposure
when medium/high blending levels of reconstruction
are employed (Figures 2 and 3).
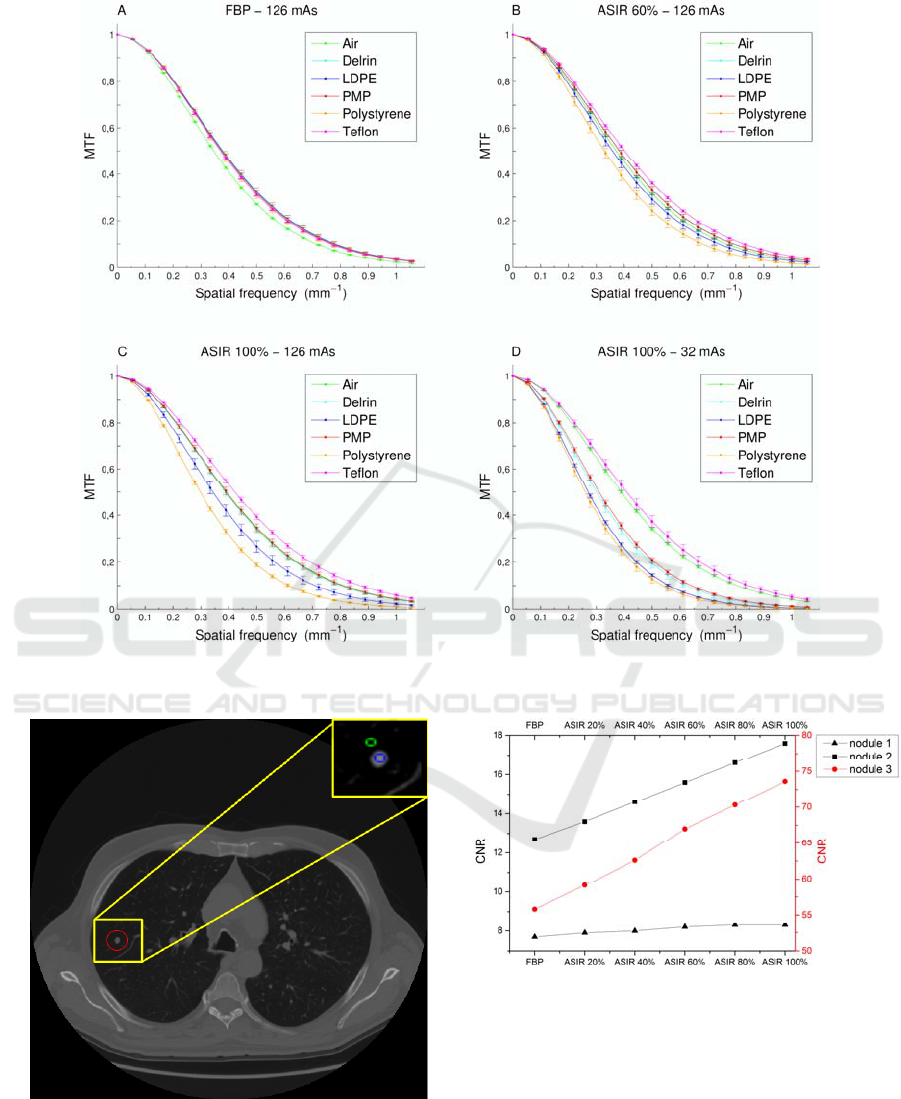
Figure 4: MTF for ASIR-reconstructed CT images (blending level of reconstruction of 0% (panel A), 60% (panel B) and
100% (panels C and D) and medium (126 mAs, panel A, B and C) /low (32 mAs, panel D) tube load.
Figure 5: Example of a pulmonary nodule (5 mm of
diameter) employed for CNR and percentage contrast
evaluation (The ROI in green represented the “background
ROI”, while the ROI in blue represented the “nodule
ROI”).
Figure 6: Examples of CNRs for nodules of 4 mm (nodule
1), 5 mm (nodule 2) and 6 mm (nodule 3) of diameter.
Clinical images were acquired adopting the chest scan
protocol of Table 1.
In addition, chest clinical images reconstructed
with ASIR exhibit interesting properties in terms of
increased CNR and percentage contrast of small
nodules (Figures 6 and 7). These results are in
agreement with previous qualitative studies in which
the detection of lesions seems to be improved when
the ASIR algorithm is employed in the
reconstruction process instead of the conventional.
FBP (Willemink et al., 2013). Another study
highlighted that a 50% ASIR-FBP blending level
allowed to maintain acceptable CNR and image
noise levels in low-dose images of different chest
phantoms (Mathieu et al, 2014). The authors showed
that, as compared to conventional FBP, radiation
dose could be reduced by 40% by using 50% ASIR-
FBP blending level of reconstruction without
affecting overall image quality.
Figure 7: Examples of percentage contrasts for nodules of
4 mm (nodule 1), 5 mm (nodule 2) and 6 mm (nodule 3) of
diameter. Clinical images were acquired adopting the
chest scan protocol of Table 1.
As shown in our results, the quality of ASIR-
reconstructed images is strictly related to the
blending level of reconstruction. However, even
though the choice of the ASIR-FBP blending level is
extremely important to avoid losses in details
detection, ASIR images exhibit considerably better
noise and contrast properties as compared to FBP
images. Notice that while the CNR increment may
be due to the noise reduction performed by ASIR,
the percentage contrast is not directly related to
image noise (Eq. 2). This means that ASIR could
also improve tissue differences in terms of HU
values and thus have positive influences on CAD
performances. Therefore, the ASIR algorithm may
be employed in low-dose chest CT acquisitions
(which are required in screening examinations) and
in combination with CAD systems as suggested by
previous studies (Hyun et al, 2015). It should be
reminded that spatial resolution with ASIR
reconstruction depends also on radiation dose and on
the objects contrast in the images (Figures 3 and 4).
These dependences should be carefully considered
in order to evaluate and optimise the combined
employment of ASIR and the CAD system available
for us (Torres et al., 2015; Fantacci et al., 2017) for
pulmonary nodules detection in ultra-low dose
conditions.
5 CONCLUSIONS
In this work we assessed the noise, contrast and
spatial resolution properties of phantom and human
chest CT images reconstructed through different
ASIR-FBP blending levels.
An important noise reduction and CNR
increment is achieved in images reconstructed
through the ASIR algorithm. Percentage contrast
also increases with the blending level of
reconstruction. For these reasons ASIR may be
employed in low-dose chest CT examinations and it
could positively influence CAD performances.
However, since spatial resolution decreases with the
increasing of the blending level of reconstruction in
low dose acquisitions, this parameter should be
carefully optimised.
Even though further studies are needed, our
findings provide additional insights into the
characterisation of the ASIR algorithm performance
and can be of practical interest toward an its
adequate employment.
REFERENCES
Barca P, Giannelli M, Fantacci ME and Caramella D.
2017. Evaluation of the Imaging Properties of a CT
Scanner with the Adaptive Statistical Iterative
Reconstruction Algorithm; Proceedings of
Proceedings of BIOSTEC 2017, Bioinformatics,
Biodevices; 200-206
Catphan ® 504 Manual - The Phantom Laboratory (NY,
USA).
Den Harder AM, Willemink MJ, van Hamersvelt RW,
Vonken EPA, Milles J, Schilham AMR, Lammers JW,
de Jong PA, Leiner T, Budde RPJ. 2016. Effect of
radiation dose reduction and iterative reconstruction
on computer aided detection of pulmonary nodules:
Intra individual comparison. European Journal of
Radiology; 85:346-351
Fantacci ME, Traverso A, Bagnasco S, Bracco C,
Campanella D, Chiara G, Lopez Torres E, Manca A,
Regge D, Saletta M, Stasi M, Vallero S, Vassallo and
Cerello P. 2017. A Web- and Cloud- based Service for
the Clinical Use of a CAD (Computer Aided
Detection) System, Proceedings of BIOSTEC 2017,
Bioinformatics; 202-209
Goo H W. 2012. CT Radiation Dose Optimization and
Estimation: an Update for Radiologists, Korean
Journal of Radiology; 13(1):1-11

Huber A, Landau J, Ebner L, Bütikofer Y, Leidolt L, Brela
B, May M, Heverhagen and Christe A. 2016.
Performance of ultralow-dose CTwith iterative
reconstruction in lung cancer screening: limiting
radiation exposure to the equivalent of conventional
chest X-ray imaging, European Radiology;
26(10):3643-52
Hyun JY, Myung JC, Hye SH, Jung WM and Kyung SL.
2015. Adaptive Statistical Iterative Reconstruction-
Applied Ultra-Low-Dose CT with Radiography-
Comparable Radiation Dose: Usefulness for Lung
Nodule Detection. Korean Journal of Radiology;
16(5):1132-41
Lopez Torres E, Fiorina E, Pennazio F, Peroni C, Saletta
M, Camarlinghi N, Fantacci ME and Cerello P. 2015.
Large scale validation of the M5L lung CAD on
heterogeneous CT datasets, Medical Physics;
42(4):1477-89
Malvezzi M, Bertuccio P, Rosso T, Rota M, Levi F, La
Vecchia C and Negri E. 2015. Annals of Oncology;
26:779–786
Mathieu KB, Ai H, Fox PS, Godoy MCB, Munden RF, de
Groot PM, Pan T. 2014. Radiation dose reduction for
CT lung cancer screening using ASIR and MBIR: a
phantom study, Journal of applied clinical medical
Physics;15(2):271-80
Richard S, Husarik DB, Yadava G, Murphy SN, Samei E.
2012. Towards task-based assessment of CT
performance: system and object MTF across different
reconstruction algorithms. Medical Physics;
39(7):4115-22
Samei E and Richard S. 2015. Assessment of the dose
reduction potential of a model-based iterative
reconstruction algorithm using a task-based
performance metrology. Medical Physics; 42(1):314-
23
Siegel R L, Miller K D and Jemal A. 2015. CA: a cancer
journal for clinicians; 65:5–29
Siewerdsen JH, Cunningham IA and Jaffray DA. 2002. A
framework for noise-power spectrum analysis of
multidimensional images. Medical Physics;
29(11):2655-71Mathieu KB, Ai H, Fox PS, Godoy
MCB, Munden RF, de Groot PM, Pan T. 2014.
Radiation dose reduction for CT lung cancer screening
using ASIR and MBIR: a phantom study, Journal of
applied clinical medical Physics;15(2):271-80
The National Lung Screening Trial Research Team. 2011.
Reduced lung cancer mortality with low dose
computed tomographic screening, The New England
Journal of Medicine; 365(5):395-409
Wielpütz MO, Wroblewski J, Lederlin M, Dinkel J,
Eichinger M, Koenigkam-Santos M, Biederer J,
Kauczor HU, Puderbach MU and Jobst BJ. 2015.
Computer-aided detection of artificial pulmonary
nodules using an ex vivo lung phantom: influence of
exposure parameters and iterative reconstruction.
European Journal of Radiology; 84:1005–1011
Willemink MJ, de Jong PA, Leiner T, de Heer LM,
Nievelstein RA, Budde RP, Schilham AM. 2013.
Iterative reconstruction techniques for computed
tomography Part 1: Technical principles. European
Radiology; 23:1623–31.
