
Developing a Sensor based Homecare System
The Role of Bluetooth Low-Energy in Activity Monitoring
Luke Power, Lisa Jackson and Sarah Dunnett
Department of Aeronautical and Automotive Engineering, Loughborough
University, Epinal Way, Loughborough, U.K.
Keywords: Sensor, Homecare System, Activity Monitoring, Lifestyle Monitoring, Indoor Positioning System.
Abstract: Home healthcare systems have become a focus of research due to the shifting care requirements of the elderly.
Malnourishment, independence and activity are becoming vital metrics when monitoring patient illness.
Monitoring devices described in research however express issues in the consistent remote capture of these
metrics. This work presents the role of Bluetooth Low-Energy Beacons (BLE) in community based healthcare
by examining how passive activity monitoring can assist patients coping with independence and disease
management within their homes as an indoor Proximity System (IPS). BLE sensors will be placed on the
patient, in their home and on objects of interest (OOI) such as water bottles, kettles and microwaves. Research
described in this paper will focus on accuracy of BLE beacon as an IPS for lifestyle monitoring and its
application to intelligent healthcare. This is achieved by creating a model of patient care requirements
structured using activities of daily living (ADL) which is evaluated using patient activity pattern recognition
in captured sensor data. Pattern analysis uses the changing distance values between BLE sensors to determine
movement motion and location which contribute to the activity, sensor based care model. Results support
efficacy when using BLE beacons as an IPS with patient activity patterns becoming observable through
monitoring with a consistent ability to distinguish interactions in activity patterns capture. Future experiments
will focus on analysis captured sensor metrics to determine care outcomes.
1 INTRODUCTION
National healthcare systems have been placed under
strain with hospitals nearing capacity and staff
shortages threating to affect the quality of care
provided. Research has often focused on technology
as a method to deliver more efficient processes. With
over 65s accounting for more than 60% of hospital
emissions (Office for National Statistics, 2012),
healthcare prioritises treating elderly patients at home
rather than having them cared for at hospitals.
Community nurses which operate as home care givers
are in decline however, by 2025 due to high demand
and diminishing numbers the profession may no
longer exist (CarersUK, 2015). Independent care
givers often fill the gap left by declining community
nurses with CareUK estimating one in eight people
provide informal care for a relative, friend or
neighbour where professional nurses are not available
(CarersUK Policy Briefing, 2015). The diseases
elderly patients suffer from have changed drastically
with improving living conditions and access to
modern medicines. Infectious diseases such as
measles, whooping cough and scarlet fever which
would require hospital treatment have been declining
worldwide (Armstrong, G. L., 1999). Non-
communicable diseases (NCDs) have been on the rise
however, conditions such as stroke, cancer, heart
disease which are not infectious now account for 68%
of total deaths worldwide (WHO, 2012) and present
unique challenges for home based care (Dye, 2014).
NCDs such as Dementia, a degrative
neurological condition (DNC) are now the leading
cause of death (Office for National Statistics, 2016)
in England and Wales, with the elderly population of
65 and over four times more likely than other age
groups to suffer from a NCD (Office for National
Statistics, 2016), this makes this age group the focus
of NCD and DNC care research outcomes and a
potential avenue for reducing healthcare system strain
through home monitoring. Healthcare research has
identified lifestyle, activity, nutrition and
independence as key factors in the progression and
management of NCDs for elderly patients (Katz,
1983). Current research describes devices which can
remotely monitor patients and has successfully shown
598
Power, L., Jackson, L. and Dunnett, S.
Developing a Sensor based Homecare System - The Role of Bluetooth Low-Energy in Activity Monitoring.
DOI: 10.5220/0006722305980606
In Proceedings of the 11th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2018) - Volume 5: HEALTHINF, pages 598-606
ISBN: 978-989-758-281-3
Copyright © 2018 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

efficacy in delivering remote care. This paper will
describe the reasoning for exploring BLE (Bluetooth
Low-Energy) for IPS (Indoor Proximity System) as
an application of Intelligent Healthcare.
2 INTELLIGENT HEALTHCARE
Intelligent Healthcare aims to examine methods of
caring for patients in their homes while maintaining
acceptable standards which a community nurse could
provide, using technology. A substantial amount of
the research in this area place within a smart home or
health smart home, the augmentation of the home
environment to accommodate technology which will
benefit the occupant through remote monitoring.
Various technologies work to keep a patient or elderly
person safe in their home and keep them from being
readmitted to hospital. Research areas such as
telehealth and telecare look to alert care givers and
other care stakeholders to potential events taking
place inside the home which may require their
attention such as fall detectors, changes sedentary
levels and possible malnourishment (Stowe, S., &
Harding, S., 2010). Research within intelligent
healthcare has substantiated the efficacy of remote
caring technologies for NCDs such as heart disease
and diabetes through increased monitoring in the
home (Allard et al., 2014).
2.1 Remote Patient Monitoring
Remote Patient Monitoring (RPM) is an effective
method for providing intelligent healthcare remotely
to patients suffering from NCDs such as Chronic
Heart Failure (CHF), Chronic obstructive pulmonary
disease (COPD) and diabetes. Nakamura et al has
demonstrated the efficacy of this method of remote,
technology assisted care by examining the
effectiveness of RPM in reducing the risk of mortality
for CHF patients compared to ‘usual care’ (Nakamura
et al, 2013. A significant factor in reducing mortality
when using RPM has been the higher frequency of
measurements from the patient as this allows for a
greater amount of data to be examined and thus an
intervention made timelier. Measurements taken with
RPM devices may include bodyweight, blood
pressure and heart rate. During Nakamura et al
experiments, patients with medication management
via RPM could have their medication dosage
managed accurately from the more frequent data
captures thus reducing the likelihood of mortality by
CHF. RPM appears to be an effaceable approach to
delivering intelligent healthcare, by capturing data
reportedly and analysing it using medical models it
can be possible to predict, prevent and manage illness
without the need of hospital or nurse visits to collect
this data. Clinical effectiveness of patients submitting
frequent clinical measurements from the home
environment to allow a greater spectrum of data
points (Nakamura et al, 2013) is a clear factor in the
success of the technology and the patients outcomes.
However, NCDs often have a wider variety of
care requirements, where CHF can be measured
remotely using a simple heart or pulse monitor, NCDs
have a wide variety of ailments and symptoms
associated with their acceleration. Factors such as
loss of independence, inability to perform motions,
deviations from normal tasks over time and
dehydration at home. Research has attempted to
capture this data and use RPM technique to remotely
provide visibility to these symptom changes over time
with varied success. As such, RPM forms a
significant basis for the underlying research presented
in this paper as the mechanism of using multiple data
points in activity monitoring evaluation with a focus
on selecting and testing devices which may accurately
capture the required data.
2.2 Activity Monitoring
Patient activities are a key determinant when
assessing independent living for elderly patients.
Chiauzzi et al described activity monitoring as
“sensors which monitor patient’s domestic routines
and daily activities such as movement around the
house, bed and chair occupancy, the opening of
cupboards, doors, fridges and wardrobes, and use of
electrical devices such as kettles, TVs and lamps”
(Chiauzzi et al., 2015). Factors which can affect the
development of a NCD in the elderly are measured
using the Activities of Daily Living (ADL), a set of
standards by which professional caregivers observe
and assess patients care outcomes. Activity
monitoring for ADL uses passive sensors recording
the domestic environment and patient interactions
there within. Data captured using monitoring is
observed for patterns and the recognition of
significant deviations from what is expected under
ADL guidelines which guide care efforts, provide
timely interventions and assist in future diagnosis.
2.2.1 Devices for Activity Monitoring
Devices which employ sensors to be used in activity
monitoring vary greatly in operation and accuracy.
Consumer wearable devices for activity tracking have
shown promise in post-surgery recovery in cardiac
Developing a Sensor based Homecare System - The Role of Bluetooth Low-Energy in Activity Monitoring
599
patients, pulmonary rehabilitation, and activity
counselling in diabetic patients, among others
(Chiauzzi et al., 2015). Research however, has
described several limitations when using intelligent
healthcare focused activity monitoring to obtain the
data required for ADL analysis. Nangalia et al
describe how sensors such as occupancy and door
sensors, which are used to determine sedentary levels,
have deficiencies which reduce accuracy or become
limited when used in homes with multiple occupants
(Nangalia et al., 2010) and therefore can’t be relied
upon for RPM of activity. Positioning sensors also
have natural barriers with line of sight (LOS), passive
infrared (PIR) sensors which monitor patients, rely on
microwave emissions to detect motion which can be
intercepted by walls, objects or additional occupants
(Barlow et al., 2007).
2.3 Indoor Proximity Systems
Indoor Proximity Systems (IPS) use sensors to
approximate position within a structure. Proximity
sensors capture locational data by broadcasting an
advertisement radio wave which is intercepted by a
receiver located on a person (Feil, 2016). The
distance between the sensor which emits the wave
and the receiver is calculated using received signal
strength indication (RSSI). As radio wave accuracy is
highly dependent on environment the RSSI is used to
interpret distance from an advertising sensor and thus
location is estimated based on proximity.
Environments using proximity for activity
monitoring have several advantages over currently
implemented remote activity monitoring devices.
Radio wave advertising can pass through solid
objects, eliminating the issue of requiring LOS
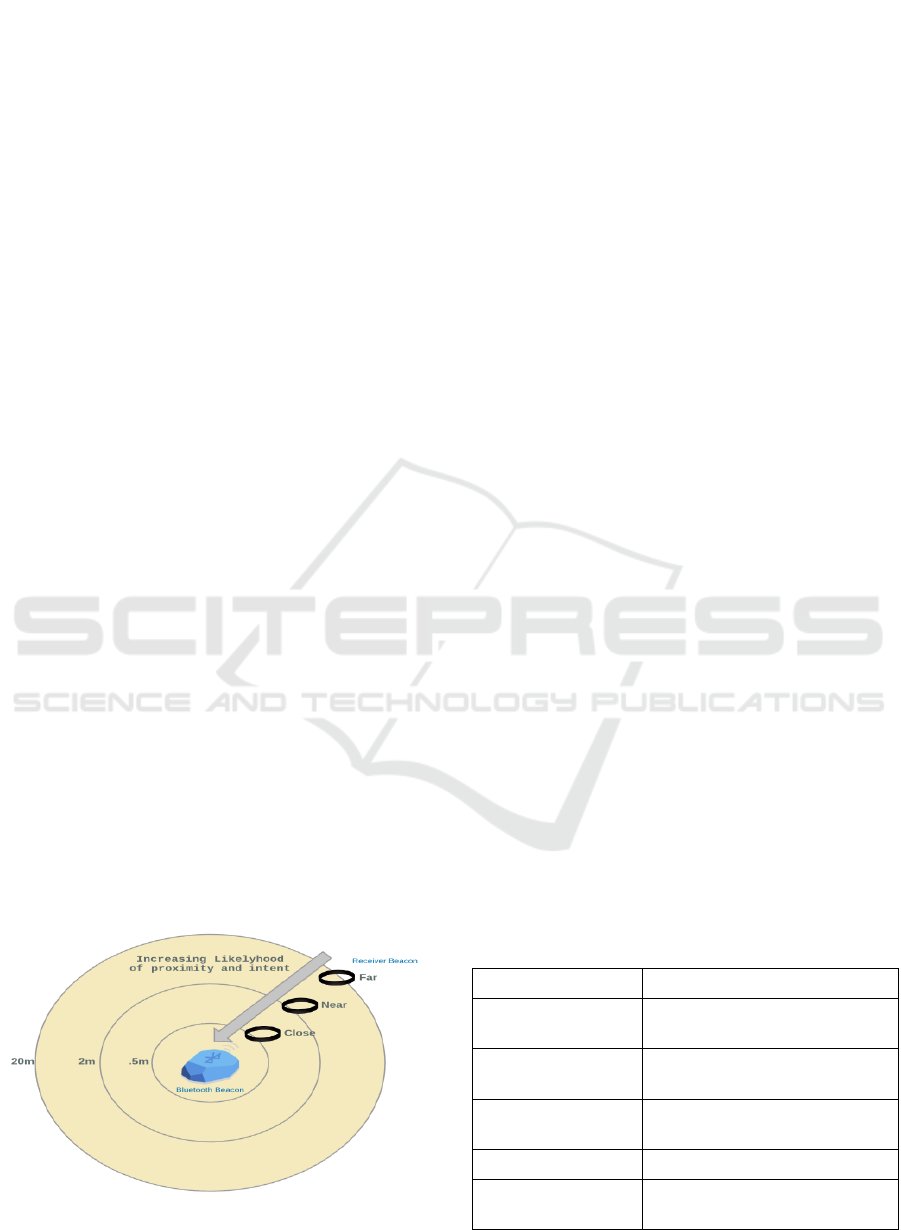
(Kyoung Nam Ha et al., 2016). Radio waves could
determine intention and movement through
increasing or decreasing proximity from a sensor to
the receiving device as illustrated in figure 1. As RSSI
Figure 1: Proximity ranges from emitter to approaching
receiver.
grows stronger between a sensor and a receiver,
locality, motion, intention and proximity can be
determined (Kim et al., 2015). Among the challenges
of using proximity for Activity RPM is the use of
RSSI. Multiple advertisement points could increase
approximation within a home but the efficacy of this
is largely untested in that environmental context.
Multiple advertisement points could increase
approximation within a home but the efficacy of this
is largely untested in that environmental context. As
such this paper will outline experiments to increase
accuracy and ultimately form pattern recognition of
patient activity using IPS.
2.3.1 Bluetooth Beacon IPS
Bluetooth Low-energy was chosen as the device to be
incorporated into a potential IPS for activity
monitoring. Developed as Bluetooth version 4.0 and
primarily designed to reduce the power consumption,
BLE is a universally recognised standard of radio
signal, interpretable by any number of devices within
the last 15 years. Able to fit onto small circuit boards
and operate up to 2 years before exhausting its
battery. The potential for use in intelligent healthcare
is wide in scope due to the interoperability with
devices, low cost and low power output (Feil, 2016).
As with all proximity based devices BLE beacons
broadcast an RSSI to understand and capture
approximate locations of receivers in its range.
2.3.2 Recognising Patterns in IPS Data
Using BLE as a remote IPS to gather activity patterns
of elderly patients requires the implementation of a
standard of observation with efficacy in homecare
environments such as the activities of daily living
(ADL) (Katz, 1983). Interactions captured should
align with ADL conditions for independence and
health as table 1 outlines.
Table 1: ADL By Room or Item Interaction.
ADL Condition
Room or Item Indication
Sedentary Levels
Movement through proximity
ranges
Eating
Immediate Proximity to Fridge,
Microwave, Oven
Drinking
Manipulation and Proximity to
BLE Water Bottle
Toileting/Bathing
Near Proximity to Bath
Motion/Transferring
Movement between Proximity
Beacons over time
HEALTHINF 2018 - 11th International Conference on Health Informatics
600

By placing BLE beacons throughout patient’s homes,
various rooms of the home will emit proximity radius.
A patient wearing a receiver would move between,
stay sedentary or interact with objects in these radii.
This research proposes it may be possible to capture
and align these activity events to ADL conditions to
remotely determine lifestyle factors which may affect
a patients NCD. Figure 2 below, illustrates possible
configuration of proximity ranges to determine ADL
conditions as described in table 1. An occupant with
a receiver would invariably be in range of several
beacons organised and identified by their rooms or
objects. The strongest signal strength to the receiver
worn by the patient will reveal the occupant’s
location at any given time while showing intention
through the movements between ranges of BLE.
Figure 2: BLE Beacons: Room placement in fictional
environment.
This method of monitoring has gained efficacy
through research such as by Zhao et al., applying
proximity zones by room to an experimental
workplace employee activity they observed
individuals could be tracked with current occupation
approximated, i.e. taking a break or working at their
desk (Zhao et al., 2014). This research has also
conducted experiments to determine the best method
of IPS placement. The focus of experiments in the
work reported here however will rest with
distinguishing ADL interactions in proximity zones,
captured and extracting patterns from data which fits
into a predictive healthcare algorithm to determine
ADL conditions.
3 EXPERIMENTS
Experiments conducted in this paper form an iterative
process of implementing and testing the efficacy of
BLE beacons for intelligent healthcare based RPM of
ADL in elderly patients. The overall goals of
experiments will be to initially establish accuracy of
beacons in simple, predictable environments and
expand their monitoring capabilities in complex
environments experienced in home healthcare.
3.1 Experiment Conditions and
Metrics
Experiments take place within an appartment
building with a variety of rooms including a
bathroom, bedroom, living room, kitchen and office.
These enviroments are mapped to potential
conditions sought by ADL standards, described in
table 1, toilet signfiying likely bathing etc. Accuracy
between beacon and receiver is measured by placing
both inside a room with no barriers to radio signal, the
actual distance is then measured across a horizontal
plane between the two. Physical distance is measured
between the BLE beacon and the receiver using
measuring tape while the reported distance is
determined using beacon RSSI transmited to the
receiver. The forementioned metrics used in
experiments are displayed in table 2.
Table 2: Metrics used in experiments.
Metric
Description
Received Signal
Strength (RSSI)
Measurement of the power present
in a received radio signal.
TX Power
TX is the power transmitted in
decibels per milliwatt (dBm) (Garg,
K. and Pandey, 2016)
Advertisement
Interval (MS)
The time interval between packets
has broadcasted measured in micro
seconds (MS)
Major/Minor
The UUID parameters of beacon
identifiers.
Distance
Reported
Distance in metres calculated from
RSSI and TX Power
Actual Distance
Physical measured distance in
metres from beacon and receiver
3.2 Experiment Stages
Experiments take place in stages as future work will
depend on initial experiments to obtain acceptable
degrees of accuracy across multiple use cases such as
using a variety of power outputs, identification of
rooms and use of objects by occupant wearing a
receiver. Experiments are performed within an empty
room in the test apartment with no barriers between
the beacon and receiver.
Developing a Sensor based Homecare System - The Role of Bluetooth Low-Energy in Activity Monitoring
601

3.2.1 Proximity Accuracy
Proximity accuracy experiments seek to establish
how accurate BLE beacons are when estimating the
distance between the beacon and the receiver when
within its radius of advertisement. Several factors
could affect this including TX Power output,
advertisement interval and physical barriers to radio
waves. Accuracy tests first measure RSSI and thus
distance over distances between sender and receiver
such as .1 metres, .5 metres and 1 metre etc. Further
tests then moved beacons either closer or further
away and measured accuracy of distance
interpretation. TX Power outputs were also altered to
access impact of proximity accuracy.
3.2.2 Multiple Room Patterns
Proximity devices placed in multiple rooms of the test
apartment builds on what is understood from the
previous experiment. With established accuracy,
obtained by altering TX Power and advertisement
interval, within one room the beacons are then placed
in multiple rooms while a receiver is placed in one
room. RSSI and distance reported is measured
between all beacons and the receiver. The receiver
will, depending on the test, remain stationary in one
room or be placed in different rooms with the
movement event between rooms captured in data.
3.2.3 Objects of Interest
Further experiments will test beacons placed on
objects with the intention to understand how frequent,
if at all an occupant manipulates an item such as a
microwave, kettle or water bottle. Experiments will
include time set manipulations of these objects by a
participant wearing a receiver and random
manipulations of OOI. The goal is to witness
interactions between patients and objects of
importance to their ADL.
3.2.4 Data Analysis Experiments
With proximity, multiple room and object
manipulation accuracy established experiments focus
on incorporating ADL into an automated algorithm
which recognises relevant ADL patterns in activity
monitored data. Experiments to determine accuracy
of recognitions will take place with a participant
performing tasks within the test environment and the
data examined to pair the interaction with proximity
variables.
3.2.5 Participant Experiments
With established data analysing algorithms, partici-
pants experiments will explore activity monitoring
capabilities across a variety of circumstances
including using different testing environments such
as houses, number of beacons, participants on
schedules and experiments without participants
schedules to follow. These experiments demonstrate
the effectiveness of BLE beacons for both accurately
capturing interactions relevant to ADL analysis
within intelligent healthcare and the use in the RPM
of NCDs as an aide to care givers.
4 RESULTS & DISCUSSION
Results described in this section cover proximity
accuracy and multiple room pattern experiment
subsections. Tests for accuracy follow a standard of
multiple distances measured vs actual with multiple
power outputs. Multiple room tests refer to average
distance reported to determine which of the multiple
rooms the receiver is currently in, during all
experiments the receiver is moved to different
locations and new actual distances recorded.
4.1 Proximity Accuracy: Calibration
Table 3 shows the accuracy of reported distance vs
actual distance when both TX Power and
advertisement interval are altered. For alternating
tests, the corresponding value is set to maximum, for
TX Power this is -4dbm and for interval it is 100ms.
Each test displayed is an average of over 1000
captures using BLE beacons and a phone application
acting as the receiver.
Table 3: TX Power & Interval Effect on Accuracy.
TX Power and
Advertisement Interval
Reported Distance vs
Actual Distance
Accuracy (AVG, 1000
Captures)
-4dbm (Interval 100ms)
77% Accurate
-10dbm (Interval 100ms)
73% Accurate
-20dbm (Interval 100ms)
70% Accurate
-40dbm (Interval 100ms)
69% Accurate
200ms (TX -4dbm)
77% Accurate
500ms (TX -4dbm)
76% Accurate
800ms (TX -4dbm)
74% Accurate
1000ms (TX -4dbm)
74% Accurate
HEALTHINF 2018 - 11th International Conference on Health Informatics
602

Perhaps not surprisingly, using the highest power
output of -4dbm achieved the highest accurate value
between distance reported and actual measured
distance, with the same being true of advertisement
interval although the affect was not as noticeable
possibly due to the fact captured results are
aggregated. Illustrating this result visually, figure 3
shows the results from a proximity accuracy
experiment with 1200 captures and maximum values
for both advertisement interval and TX Power.
During the experiment the beacon maintained a
stationary position while the receiver moved closer
across a horizontal surface. The movement intervals
were 2.5M to 2M to 1M with 15 minutes of captures
recorded in each state. Figure 3 illustrates an erratic
line which represents beacon reported distance and a
solid line which represents actual distance from
beacon to receiver.
Figure 3: Beacon Accuracy: Actual vs Reported Distance.
As the receiver moves closer during predetermined
distance changes it is clear the beacon records this
interaction with signal strength increasing following
for a smaller reported distance which becomes more
accurate the closer the receiver gets to the beacon
with an overall accuracy of 78.1% which is in line
with previous experiments using this TX Power and
advertisement interval. All further tests would use
these values
4.2 Multiple Room: Distinguishing
Values
The goal of the multiple room testing phase was
essentially to determine which room an occupant was
both in and moving towards with multiple beacon
outputs being intercepted by one receiver.
Distinguishing values would be the highest
relative RSSI when compared to competing beacon
signal, the factor of this accuracy would need to be
determined.
Table 4: Multiple Room: Stationary Receiver Test.
Beacon
Location
Distance
from
Office
Distance
from
LR
Distance
from
Bedroom
Office
(Reported)
1.18m
3.32m
3.14
Office (Actual)
1.3m
4.12m
3.2m
Table 4 shows a signal experiment in which the
receiver was placed in the office of the experiment
environment. Without moving from its location over
30 minutes of captures recorded its location as being
nearest to the office beacon, while being almost
equally far from the bedroom as from the sitting room
which is an accurate result. This test also recorded
good accuracy between actual and reported distances
through barriers such as walls. Further to multiple
room experiments examined in non-stationary tests
were also carried out which involved the same beacon
layout as the experiment detailed in table 4. Each
predetermined movement event occurred within 15
minutes and one 30-minute interval with the receiver
being moved between rooms while recording
showing a pattern of motion between areas as RSSI
fluctuated between beacons.
Figure 4: Beacon Accuracy: Bedroom Beacon.
The results can be seen in figure 4,5 and 6 while
location and times can be seen in table 5. Figures 4,5
and 6 show the data captured by the BLE bedroom
beacon between the times of 9:45 and 11:00.
Table 5: Multiple Room: Receiver Movement Between
Rooms.
Timeframe
Receiver Location
9:45 - 10:00
Office
10:00– 10:30
Bedroom
10:30– 10:45
Sitting Room
10:45– 11:00
Bedroom
Developing a Sensor based Homecare System - The Role of Bluetooth Low-Energy in Activity Monitoring
603
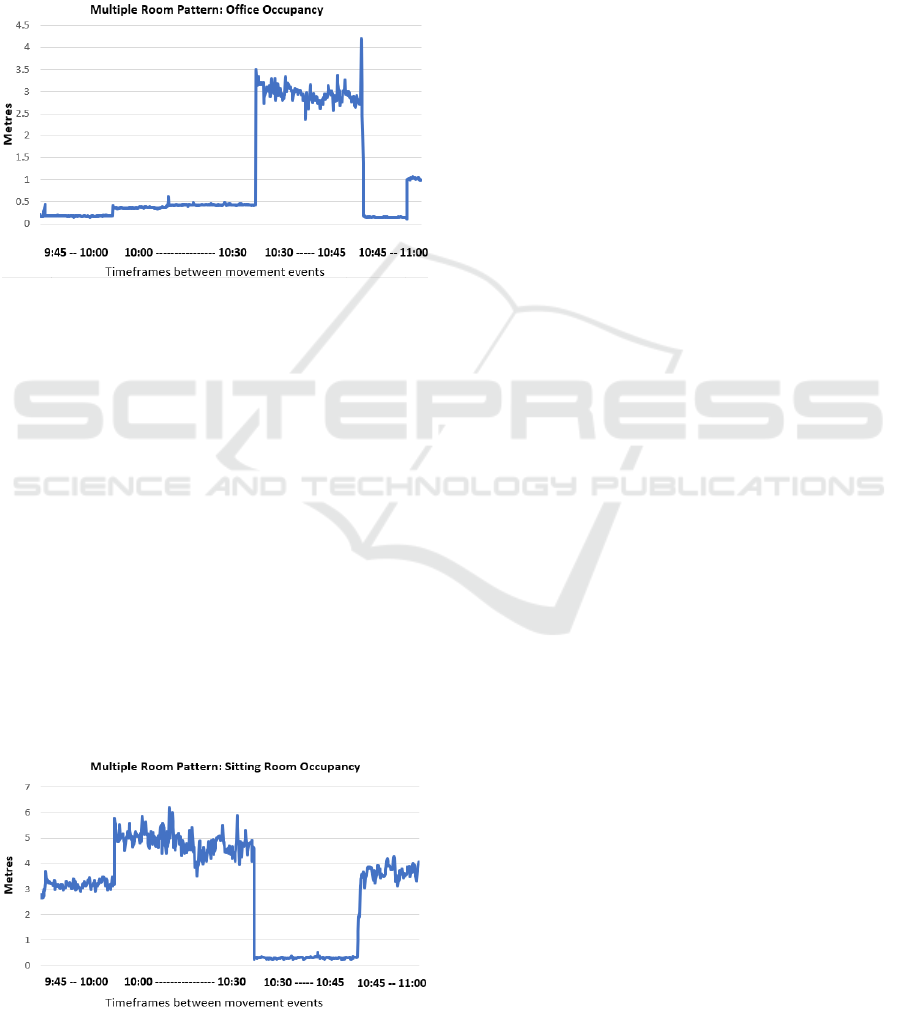
The beacon estimates proximity during early
timeframes as the beacon is in the adjacent room, the
office. From 10:00 to 10:30 the bedroom beacon
reports very close proximity as now the receiver is
physically in the bedroom. From 10:30 to 10:45 the
bedroom beacon reports a now significant gap
between itself and the receiver of up to 8 metres
which is accurate as the receiver as moved some
distance and between two walls to the sitting room.
Figure 5: Beacon Accuracy: Office Beacon.
The pattern continues as the receiver is moved from
the bedroom to the sitting room, the office beacon just
has a wall between and it and the receiver and this is
visible in the data. Figure 5 illustrates the data
captured from the office beacon. The initial office
timeframe reports proximity accurately between 9:45
and 10:00, this is slightly increased in line with the
movement event from office to bedroom. And finally
figure 6 shows this multiple room experiment from
the point of view of the sitting room beacon. During
the early periods between 9:45 and 10:30 there is
significant distances from this beacon between the
closer office and bedroom beacons. This distance
reported is almost inversely proportional to distance
gaps observed from the office and bedroom
perspectives. With a consistent accuracy observed
between 10:30 and 10:45 when the receiver is placed
in the beacons near radius emission.
Figure 6: Beacon Accuracy: Sitting Room Beacon.
4.3 Discussion
The experiments conducted within the first two
phases of the planned efficacy process indicates a
reasonable, predictive degree of accuracy can be
obtained by BLE beacons used as part of an IPS for
activity monitoring. With consistent results of RSSI
used for distance calculations, multiple room beacon
experiments have begun to show data which can be
interpreted to ascertain the movement events of a
receiver device. Patient patterns are expected to be
more erratic and unpredictable, and hence further
experiments within these phases will be conducted to
continue building upon the efficacy of these devices
in these individual scenarios before experiments
using occupants with intentionally erratic schedules.
Following this phase described in figure 6, focus
will turn to experiments to develop consistent reliable
ADL based triggers within data analysis and overall
answering the question as to the role of BLE in
intelligent healthcare monitoring.
4.4 Conclusions
National healthcare services cannot continue to coupe
under the strain the aging population and the rise of
NCDs have placed upon them. This leaves
technology based ‘intelligent’ forms of healthcare as
one of the few remaining realistic solutions
(Campling, 2014). As discussed, activity monitoring
has a significant role in the management, treatment,
diagnosis and in some cases prevention of NCDs
which the elderly suffers from the most and which
cause not only the largest strain on the healthcare
system but also account for most deaths in the UK.
Research into intelligent healthcare solutions for this
problem is however limited by the technology itself.
Although sensors used in RPM have proven to be
successful (Nakamura et al, 2013), activity and
lifestyle monitoring has become an issue while using
occupancy technologies such as PIR sensors, door
sensors and chair sensors. There is also a large gap in
the ability to provide monitoring for elderly who
suffer from dehydration and malnourishment, a
significant attributor to NCDs and death in that age
group (Lavizzo-Mourey, Johnson and Stolley, 1988).
This paper has considered, BLE Beacons in use as
a part of an IPS which utilises successful RPM
techniques to potentially fill the gap left by inaccurate
devices and lack of ability to approximate use of
objects which would indicate a patient keeping
themselves nourished and dehydrated. Currently this
is completed by a community care nurse, as
profession rapidly disappearing (Royal College of
HEALTHINF 2018 - 11th International Conference on Health Informatics
604

Nursing, 2012) Results so far indicate a high degree
of approximate accuracy with limited obstacles using
a single BLE beacon. Motion and movement of a
receiver within range of a beacon is easily identifiable
within captured data as BLE has demonstrated the
ability to output a high advertisement interval without
compromising on battery, a significant barrier to
other devices (Samarrai and Greene, 2011).
5 FUTURE WORK
Additional experiment phases such as the multiple
room experiments have shown that using multiple
BLE beacons with one receiver, it is possible to
accurately determine the room the receiver is
currently occupying. Further tests showed the pattern
of movement and the potential path this receiver took
while moving between BLE beacon ranges
accurately. Additional phases of experiments need to
take place however, the most significant of which
involves incorporating pattern reading algorithms
using ADL to read and flag ADL condition
degeneration over a period. Although the outcomes of
using BLE as an IPS are speculated to be beneficial
to care givers both informal and formal the extent of
BLE application scope for home healthcare may not
be predicted without additional experimental phases
using OOI and data analysis algorithms.
REFERENCES
Allard, M., Husky, M., Catheline, G., Pelletier, A.,
Dilharreguy, B., Amieva, H., Pérès, K., Foubert-
Samier, A., Dartigues, J.-F. and Swendsen, J. (2014)
‘Mobile technologies in the early detection of cognitive
decline’, PLoS ONE, 9(12), p. e112197
Armstrong, G.L. (1999) ‘Trends in infectious disease
mortality in the United States during the 20th century’,
JAMA, 281(1), p. 61. doi: 10.1001/jama.281.1.61.
Barlow, J., Singh, D., Bayer, S. and Curry, R. (2007) ‘A
systematic review of the benefits of home telecare for
frail elderly people and those with long-term
conditions’, Journal of Telemedicine and Telecare,
13(4), pp. 172–179.
Campling, P. (2014). Intelligent Kindness: professional
healthcare and the future of the UK NHS. European
Journal for Person Centered Healthcare, 2(2), p.235.
CarersUK (2015) Https://www.Carersuk.Org/for-professio
nals/policy/policy-library/facts-about-carers-2015).
Chiauzzi, E., Rodarte, C. and DasMahapatra, P. (2015).
Patient-centered activity monitoring in the self-
management of chronic health conditions. BMC
Medicine, 13(1).
Dye, C. (2014) ‘After 2015: Infectious diseases in a new era
of health and development’, 369(1645).
Feil, C. (2016). Indoor Positioning: Opportunities and
implementation strategies of Bluetooth Low
Energy. GI_Forum, 1, pp.94-105.
Garg, A., K., R. and Pandey, M. (2016). Review of Energy
Harvesting Techniques for Wireless Sensor Nodes.
Communications on Applied Electronics, 5(7), pp.1-4.
Goats, G. (1988). Appropriate Use of the Inverse Square
Law. Physiotherapy, 74(1), p.8.
Katz, S. (1983). Assessing Self-maintenance: Activities of
Daily Living, Mobility, and Instrumental Activities of
Daily Living. Journal of the American Geriatrics
Society, 31(12), pp.721-727.
Kim, D., Kim, S., Choi, D. and Jin, S. (2015). Accurate
Indoor Proximity Zone Detection Based on Time
Window and Frequency with Bluetooth Low Energy.
Procedia Computer Science, 56, pp.88-95.
Kyoung Nam Ha Kyung Chang Lee, Suk Lee (2006).
Development of PIR Sensor Based Indoor Location
Detection System for Smart Home. Journal of Control,
Automation and Systems Engineering, 12(9), pp.905-
911.
Lavizzo-Mourey, R., Johnson, J. and Stolley, P. (1988).
Risk Factors for Dehydration Among Elderly Nursing
Home Residents. Journal of the American Geriatrics
Society, 36(3), pp.213-218.
Lavizzo-Mourey, R., Johnson, J. and Stolley, P. (1988).
Risk Factors for Dehydration Among Elderly Nursing
Home Residents. Journal of the American Geriatrics
Society, 36(3), pp.213-218.
Office for National Statistics (2015). Population Estimates
for UK, England and Wales, Scotland and Northern
Ireland, Mid-2014 - ONS. [online] Available at:
http://www.ons.gov.uk/ons/rel/pop-estimate/populatio
nestimates-for-uk--england-and-wales--scotland-and-
northern-ireland/mid-2014/index.html [Accessed 25
January. 2017].
Office for National Statistics (2016) Deaths registered in
England and wales: 2015. Available at: https://www.
ons.gov.uk/peoplepopulationandcommunity/birthsdeat
hsandmarriages/deaths/bulletins/deathsregisteredineng
landandwalesseriesdr/2015 (Accessed: 08 February
2017).
Royal College of Nursing (2012) The Community Nursing
Workforce in England, Available at: https://my.rcn.
org.uk/__data/assets/pdf_file/0003/450525/09.12_The
_Community_Nursing_Workforce_in_England.pdf
(Accessed: November 2016).
Stowe, S., & Harding, S. (2010). Telecare, telehealth and
telemedicine. European Geriatric Medicine, 1(3), 193–
197. http://doi.org/10.1016/j.eurger.2010.04.002
Samarrai, T. and Greene, C. (2011). Clinician Acceptance
of Computerized Alerts for Public Health Surveillance.
Journal of Health & Medical Informatics, 7(4).
Nakamura, N., Koga, T., & Iseki, H. (2013). A meta-
analysis of remote patient monitoring for chronic heart
failure patients. Journal of Telemedicine and Telecare,
20(1), 11–17. doi:10.1177/1357633x13517352
Developing a Sensor based Homecare System - The Role of Bluetooth Low-Energy in Activity Monitoring
605

Nangalia, V., Prytherch, D. and Smith, G. (2010). Health
technology assessment review: Remote monitoring of
vital signs - current status and future challenges.
Critical Care, 14(5), p.233
Vegesna, A., Tran, M., Angelaccio, M. and Arcona, S.
(2017) ‘Remote patient monitoring via non-invasive
digital technologies: A systematic review’,
Telemedicine and e-Health, 23(1), pp. 3–17. doi:
10.1089/tmj.2016.0051. WHO (2014) Global health
workforce shortage to reach 12.9 million in coming
decades. Available at: http://www.who.int/media
centre/news/releases/2013/health-workforce-
shortage/en/ (Accessed: 05 February 2017).
WHO (2012) Deaths from NCDs. Available at:
http://www.who.int/gho/ncd/mortality_morbidity/ncd_
total/en/ (Accessed: 05 February 2017).
Zhang, D., Wang, W. and Lv, L. (2017). Research on
Algorithm of Indoor Positioning System Based on Low
Energy Bluetooth 4.0. ITM Web of Conferences, 11,
p.03007.
Zhao, X., Xiao, Z., Markham, A., Trigoni, N. and Ren, Y.
(2014). Does BTLE measure up against WiFi? A
comparison of indoor location performance. In:
European Wireless 2014. [online] VDE. Available at:
http://ieeexplore.ieee.org/abstract/document/6843088/
[Accessed 13 Jul. 2017].
HEALTHINF 2018 - 11th International Conference on Health Informatics
606
