
Advances in Building BodyInNumbers Exercise and Wellness Health
Strategy Framework
Petr Br˚uha
1, 2
, Roman Mouˇcek
1,2
, V´ıtˇezslav Vacek
1
, Pavel
ˇ
Snejdar
1
, Luk´aˇs Vaˇreka
1, 2
, V´aclav Kraft
1
and Peter Rehor
1
1
Department of Computer Science and Engineering, Faculty of Applied Sciences,
University of West Bohemia, Univerzitn´ı 8, Pilsen, Czech Republic
2
NTIS - New Technologies for the Information Society, Faculty of Applied Sciences,
University of West Bohemia, Univerzitn´ı 8, Pilsen, Czech Republic
Keywords:
Exercise and Wellness, Chronic Disease, Health Related Data, Brain Data, Health Information Systems, Body
In Numbers Software System, Physical Performance, Cognitive Performance, Data Security.
Abstract:
Smoking, excessive drinking, overeating and physical inactivity are well-established risk factors decreasing
human physical performance and increasing incidence of chronic diseases. Moreover, epidemiological work
has identified modifiable lifestyle factors, such as poor diet, physical and cognitive inactivity that are associ-
ated with the risk of reduced cognitive performance. Chronic diseases present an enormous burden to society
by increasing medical costs and human suffering. Exercise and wellness health strategy frameworks aiming at
influencing modifiable lifestyle risk factors in voluntarily enrolled individuals and thus decreasing incidence
of chronic diseases are then very beneficial. However, such frameworks also need a supporting software in-
frastructure. The advances in building of such software infrastructure, the BodyInNumbers software system
for rapid collection and analysis of health related data, are presented in this paper. They include the changes
in the system architecture, redefinition of user roles related to data and metadata security and design, imple-
mentation and integration of new modules for collection and management of electroencephalographic/P300
event-related potential data and new modules for collection and management of data from measurements of
physical strength and balance. The results of the system testing are finally described.
1 INTRODUCTION
Chronic diseases present an enormous burden to so-
ciety by increasing medical costs and human suf-
fering. Recent data estimate that physical inactivity
and poor diet caused 40,000 deaths in 2000 (Ellison
et al., 2016), ranking second only to tobacco. Nu-
merous studies link cardiovascular disease risk with
the high glycaemic index/load of carbohydrate-based
diets (Grasgruber et al., 2016). Approximately one
tenth of the world population suffer from obesity and
prevalence of obesity among children and adults has
doubled in 73 countries since 1980 (Afshin et al.,
2017). Physical activity and a balanced diet are ef-
fective interventions as an essential weapon in the
war on chronic disease. Clearly, there is overwhelm-
ing evidence linking most chronic diseases seen in the
world today to physical inactivity and inappropriate
diet consumption.
Over the past decades, considerable knowledge
has accumulated concerning the significance of exer-
cise in the treatment of a number of diseases, includ-
ing diseases that do not primarily manifest as disor-
ders of the locomotive apparatus. Today, exercise is
indicated in the treatment of a large number of medi-
cal disorders. In the medical world, it is traditional to
prescribe the evidence-based treatment known to be
the most effective and entailing the fewest side effects
or risks. The evidence suggests that in the selected
case exercise therapy is just as effective as medical
treatment and in special situations more effective or
adds to the effect. In this context, exercise therapy
does not represent a paradigm change it is rather that
the accumulated knowledge is now so extensive that
it has to be implemented.
Data also suggest that aerobic exercise is associ-
ated with a reduced risk of cognitive impairment and
dementia; it may slow dementing illness. A com-
pelling argument can be made for this via two plau-
sible biologic pathways. First, a convergence of evi-
548
Br˚uha, P., Mou
ˇ
cek, R., Vacek, V., Šnejdar, P., Va
ˇ
reka, L., Kraft, V. and Rehor, P.
Advances in Building BodyInNumbers Exercise and Wellness Health Strategy Framework.
DOI: 10.5220/0006655205480554
In Proceedings of the 11th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2018) - Volume 5: HEALTHINF, pages 548-554
ISBN: 978-989-758-281-3
Copyright © 2018 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

dence from both animal and human studies suggests
that aerobic exercise may attenuate progression of
neurodegenerative processes and age-related loss of
synapses and neuropil. This may occur via a direct
influence on neurodegenerative disease mechanisms
or facilitation of neuroprotective neurotrophic factors
and neuroplasticity. Not to be overlooked, however,
is a second pathway, cerebrovascular disease. Cere-
brovascular burden contributes to dementia risk, es-
pecially via small vessel disease (e.g. lacunes and
leukoaraiosis). Vascular risk factors are well known
to be reduced by aerobic exercise. Thus, ongoing,
moderate-intensity physical exercise should be con-
sidered as a prescription for lowering cognitive risks
and slowing cognitivedecline across the age spectrum
(Matura et al., 2017).
Numerous noncognitive, nonvascular benefits ad-
ditionally benefit from exercise, which may be es-
pecially relevant to aging population. This includes
reduction of osteoporosis and fracture risk (Rizzoli
et al., 2009) age-related sarcopenia (Thomas, 2010)
and benefits directed at depression (Thomas, 2010)
and anxiety (Conn, 2010). An exercise program
may improve behavioral management in seniors with
dementia (Dunn, 2010) and fall risk (Teri et al.,
2003). Importantly, long-term physical activity and
fitness reduce mortality risk in the general popula-
tion. (Kokkinos et al., 2011; Allan et al., 2009).
Mounting evidence shows regular exercise helps
reduce levels of brain loss and helps our cognitive
abilities as we age. A Florida study demonstrated
that exercise at midlife may reduce the odds of de-
mentia in older adults by up to 60 percent (Lee et al.,
2010). Such extraordinary findings were corroborated
by several other studies, including University of Lis-
bon study that found that physical activity benefits
happen independently of age, education, vascular his-
tory or diabetes (Andel et al., 2008).
To address modifiable lifestyle health risk factors,
many different wellness intervention projects around
the world have been introduced. This paper presents a
progress report of such a wellness project that is cur-
rently conducted at the Department of Computer Sci-
ence and Engineering, University of West Bohemia
in the Czech Republic, and is called BodyInNum-
bers (Bruha et al., 2017).
Its focus is on definition and automation of the
data collection process in order to capture a huge
amount of heterogeneous health related data from
many users in various environment in a short time.
The architecture of an underlying application has
been extended and changes in the architectural design
related to the management of user roles and related
data and metadata security have been made. A new
module for collection and management of electroen-
cephalographic/P300 event-related potential data and
new modules for collection and management of data
from measurements of physical strength and balance
have been designed, implemented and integrated into
the system. A questionnaire given to participants has
been digitized. Finally, the related mobile application
for rapid collection of health data has been improved.
The paper is organized in the following way. The
next section shortly deals with the state of the art in
the field of publicly available health related applica-
tions that focus on cognitive and/or physical health of
its users. Section 3 takes a closer look on the archi-
tecture of the BodyInNumbers software system and
especially deals with the definition of user roles re-
lated to the data and metadata security issues. The 3.2
section brings changes in the system implementation.
The last section summarizes the parts of the system
that have been already implemented and introduces
the future steps.
2 STATE OF THE ART
The effects of a healthy lifestyle on physical and cog-
nitive functions are of interest not only to researchers
or physicians, but also to people who feel their own
responsibility for their health. Then a well designed,
user friendly and secure exercise and wellness sys-
tem containing a large collection of annotated hu-
man health related data could be suitable for fur-
ther analysis of lifestyle influence on human cognitive
and physical performance. The acquisition of human
health related data must be also efficient and flexible,
both in non-lab and lab conditions. Only a sufficient
set of data and metadata (e.g. age, gender and sum-
mary of the participant’s current life style and health)
allows researchers to perform further analysis, e.g. to
detect early symptoms of starting chronic diseases.
There are many applications that allow collection
of health related data, e.g. the Apple Health App or
Google Fit are their well known representatives. An-
other prime example is Vitabot that specializes in nu-
trition programs and goal tracking, with the ability
to connect personal fitness trainers with users, widely
used in the fitness industry (Vitabot.com, 2017). In-
dares.com (Chmel´ık et al., 2017) has been developed
with the aim to support education and research in
the field of physical activity. A variety of games
is usually used for cognitive training, e.g. the Lu-
mino City puzzle game (State of Play games, 2014) or
My Happy Neuron (HAPPYneuron, 2017). There are
also projects utilizing reaction time as a physiological
measure (e.g. (Harris et al., 2010; Bolandzadeh et al.,
Advances in Building BodyInNumbers Exercise and Wellness Health Strategy Framework
549

2015; Fenesi et al., 2016)).
In contrast to these systems and applications, our
BodyInNumbers software system is able to collect
and manage two very different data and metadata
groups - heterogeneous health related data (including
reaction times) and electroencephalographic (EEG)
/event-related potential data (ERP) recordings. To the
authors best knowledge, there are no systems publicly
available that would contain such various data: re-
action time data, P300 event-related component data
and other supportive health-related data (color vi-
sion, spirometry, electrocardiography, blood pressure,
blood glucose, body proportions and flexibility) to-
gether with corresponding metadata (except others,
for example, a summary of the participant’s current
lifestyle and health).
The set of supportive health-related data was se-
lected from two points of view: it has to represent a
basic characteristics of human physical performance
and the data have to be easily collected also in non-
lab conditions.
3 BODY IN NUMBERS
SOFTWARE SYSTEM
3.1 Architecture and Design
The architecture of the BodyInNumberssoftware sys-
tem is shown in Figure 1. The system design fully
follows the strict legislative requirements for stor-
ing and managing personal and sensitive data and
metadata. The architecture of the system is thus de-
signed to fit these needs and includes pseudonymiza-
tion, anonymization and encryption of all sensitive
and personal information stored or processed within
the system. A set of user roles is defined to access
the system functionalities and the data and metadata
stored in the system.
The system itself is divided into five essential
components: kernel, data warehouse, remote logger,
API, and web interface.
3.1.1 User roles
On the basis of activities that a user can perform
within the BodyInNumbers software system and on
the basis of privileges when accessing the data and
metadata stored in the system the following user
groups have been proposed:
• Data acquisition group – people who are per-
mitted to set a data recording procedure/collect
data/manage and verify collected data.
– coordinator – a person responsible for the defi-
nition of a data collection procedure, he/she can
determine the data collection procedure within
the application,
– leading experimenter – a person responsible for
the correct conduction of a specific measure-
ment and for the quality of resulting data and
metadata, he/she can view measured data and
edit them in the application,
– experimenter – a person responsible for the
measurement itself, he/she can insert new data
into the application.
• Control authority group – executives have access
to the data stored in the system.
– ethics committee – can view a list of exper-
iments and measured data in anonymous and
pseudonymous form,
– top management of the corresponding depart-
ments, faculties and research centers– can view
anonymous and pseudonymous measured data.
• Research group – people who work with mea-
sured data. They have access to any data accord-
ing to their permissions.
– data analyst – can view and export any data in
the anonymous form,
– nutritional counselor – can view any measured
person in the anonymous and pseudonymous
form,
– physiotherapist – can view any measured per-
son in the anonymous and pseudonymousform,
– cognitive trainer – can view any measured per-
son in the anonymous and pseudonymousform.
• Technical support group – people who can view
all data and have full access to the application.
– data manager – person with full permission to
view, edit and delete measured data. He/she is
the only person who can access personal data
and metadata via the web interface,
– security administrator – person with an access
inside server for configuration,
– system operator – owner of the system.
• Participants group – people who participated in
the measurement can access only their data and
metadata.
3.1.2 Kernel
Kernel is the most vital and secured componentof the
system. It is accessible only within a private network
and direct access is granted to a very limited num-
ber of users and services. The main responsibility
HEALTHINF 2018 - 11th International Conference on Health Informatics
550
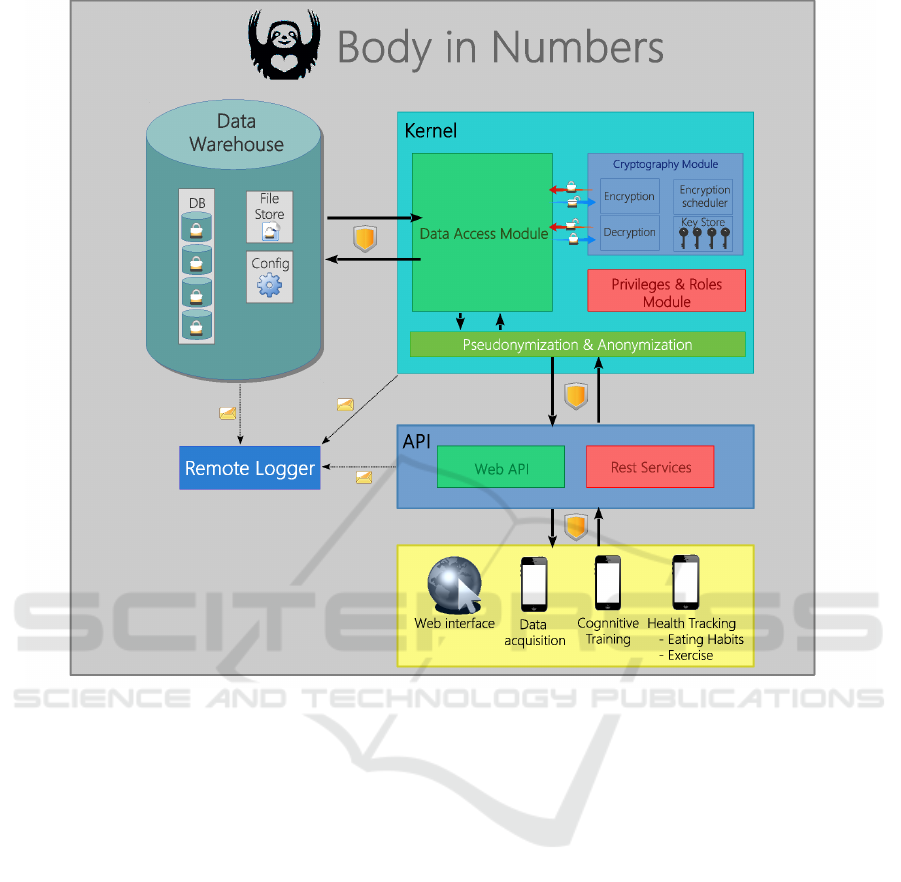
Figure 1: Software prototype architecture.
of the kernel is encryption and decryption of health
related data based on asymmetric cryptography and
anonymization of all personal data when these are
transferred out of the kernel.
Health related data processed inside the kernel are
divided into several groups (based on their content,
sensitivity, etc.). Each data group has its unique pair
of keys, one key for data encryption and the sec-
ond one for data decryption. The keys are associated
with the presented user roles and privileges within the
BodyInNumbers system.
For example, John who is a diabetes data analyst
has a privilege to read measured data inside the dia-
betes data group only, this privilege is associated with
the single decryption key of this data group. Jane as a
member of the data acquisition group has privileges
associated only with the encryption keys, i.e. she
is able to encrypt and send measured data but can-
not read them (or any other data) after their encryp-
tion. Moreover, the user does not bear any knowledge
about cryptography procedures running in the back-
ground.
Decryption is handled only by the kernel, while
encryptionmay be delegated to the client side in some
cases to decrease the server load. The data processed
and encrypted inside the kernel are persistently stored
in the data warehouse.
3.1.3 Data Warehouse
The collection of personal data and design and imple-
mentation of their storage are managed according to
law. The data warehouse component consists of sev-
eral database servers running on separate machines. It
ensures data replication to prevent possible data loss
and suitable data distribution, i.e., for example that the
subject’s informed consent containing subjects name
and contact is not stored on the same physical ma-
chine as subjects measured data to prevent any possi-
ble personal information leakage.
Advances in Building BodyInNumbers Exercise and Wellness Health Strategy Framework
551

3.1.4 API
The application programming interface (API) is a
component which serves as a gateway to the BodyIn-
Numbers system. Communication with API is en-
sured by using a secured channel (https, authentica-
tion tokens,...). The request or measured data are
passed to the kernel when authentication and autho-
rization is finished.
3.1.5 Web Interface
The web interface component (the bottom part of Fig-
ure 1) enables users to visualize, edit, insert and ex-
port health related data. It is also provides necessary
functionality for data acquisition group (scheduling
of measuring sessions, planning of technical and hu-
man resources etc.) and basic statistical and analytical
functionality. All requests of this component are han-
dled by the REST based API.
3.2 Implementation and Deployment
3.2.1 Kernel and API
The design takes into account the appropriate storage
and backup of health related data. The disadvantage is
that every operation over the data is expensive (dele-
gation of requests, multiple encryption). For this rea-
son, the optimized source code of server-side compo-
nents will be re-implemented in C++.
3.2.2 Web Interface
The web interface is based on the Flask micro python
framework and MVC pattern. All functionality is
structured into separated modules covering specific
parts of the system. The functions of modules are tied
to the kernel of the system. Every operation which re-
quires data must request the system kernel for them.
Rest API is defined for collecting data from client de-
vices.
• The General module covers functionalities afford-
able also for non-logged users.
• The Admin module serves for the administration
of users and application setting.
• The Measurement module includes the definition
of the measurement procedure and overall data
management including viewing, adding, editing
and deleting records.
• The Experiment module provides features for
adding, editing and deleting experiments.
• Each experiment requires its own set of measur-
ing devices. The Equipment module stores them
in the database and provides tools for their man-
agement.
• The QR generator module generates QR codes
into a PDF document given to the participant.
Each person has his/her numerical identifier in-
cluded in his/her QR code.
• The File Storage module provides an interface for
uploading and downloading files.
• The Brain module serves for the P300 event-
related potential data processing.
• The Reaction module has features for statisti-
cal processing of hand and leg reaction time and
graph view.
• The Cardio module computes basic statistics from
heart and blood data
• The Respiration module shows statistics from
spirometry and stress spirometry data.
• The Fitness module is processing body for pro-
portion, strength and balance data.
While the Brain and Fitness modules were newly
designed, implemented and integrated within the soft-
ware system, other modules were only partly re-
designed and reimplemented.
3.3 Testing
The software prototypehas been tested on 124 healthy
participants both in lab and non-lab environment (e.g.
during the Days of science and technologies 2017 that
were held on the Pilsen main square in September
2017) according to the following procedure.
After registering and signing the informed con-
sent within the mobile application, each participant
obtained a QR code ticket and continued to fill in
an electronic motivational questionnaire containing
a set of 19 single choice questions to provide a basic
overview of participant’s current lifestyle and health
condition. Immediately after that participants took
part in individual measurements organized at nine in-
dividual sites located in a big tent. Each site was
equipped with appropriate hardware and software
tools related to the specific measurement. It was op-
erated by at least one human expert who also pro-
vided the participant with information about the re-
lated measurement. There was an information desk
that served both for registration of participants and
provision of measurements results.
Although there was a recommended route be-
tween individual measurement sites, in fact, the par-
ticipants could visit them in any order (see the schema
HEALTHINF 2018 - 11th International Conference on Health Informatics
552
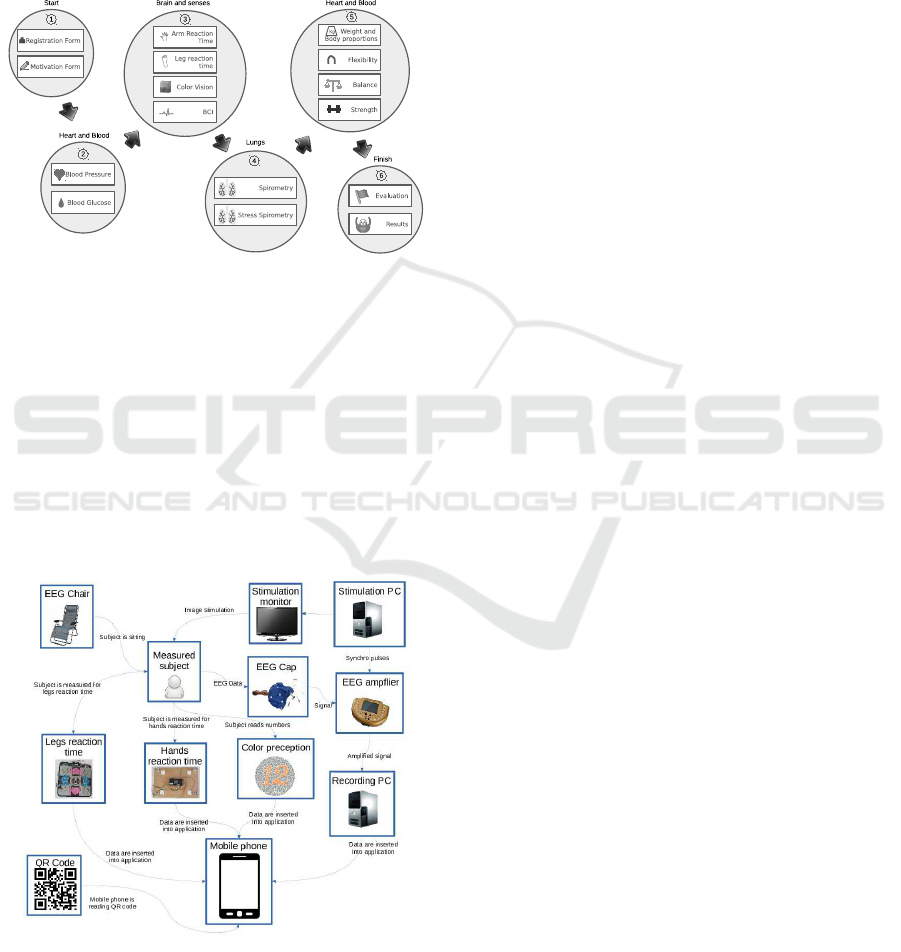
of measurement sites and the recommended route in
Figure 2). They were also not required to complete
all the measurements and could have interrupted the
measurement cycle at any time. Only in the best case
they visited all the measurement sites and filled in all
questions in the questionnaire. The complete data col-
lection procedure took approximately 30 minutes.
Figure 2: Schema of measurement sites and recommended
route between them.
When a single measurement was completed (see
e.g. the schema for the Brain and senses measure-
ment site in Figure 3), the obtained data were inserted
using the web interface into the BodyInNumbers soft-
ware system. When the participant finished his/her
last measurement, he/she was provided with the re-
sults (measured values) from all visited measurement
sites. The results were organized on the web page ac-
cording to the participant’s QR code.
Figure 3: Schema of the measurement site Brain and senses.
4 CONCLUSIONS
In this paper we presented an extension of the
BodyInNumbers software system for the exercise and
wellness health strategy framework. This software
system serves not only for rapid collection of health
related data but finally for the wellness intervention
program aiming at modifiable lifestyle factors that of-
ten contribute to incidence of chronic diseases. The
most important extended parts of the software system
include the definition of the user roles that have a di-
rect impact on the security of the data and metadata
stored in the system and design, implementation and
integration of the Brain and Fitness modules that en-
able greater variability of collected data and metadata.
The system functionalities were validated during its
real deployment.
The next steps in the system design and develop-
ment include the revision of used terminologies and
extension of data processing methods. The system is
planned to be deployed within an intervention pro-
gram to store, analyze and visualize health-related
data and their interpretations.
ACKNOWLEDGMENTS
This publication was supported by the UWB grant
SGS-2016-018 Data and Software Engineering for
Advanced Applications and the project LO1506of the
Czech Ministry of Education, Youth and Sports under
the program NPU I.
REFERENCES
Afshin, A., Forouzanfar, M. H., Reitsma, M. B., Sur, P., Es-
tep, K., Lee, A., Marczak, L., Mokdad, A. H., Moradi-
Lakeh, M., Naghavi, M., et al. (2017). Health ef-
fects of overweight and obesity in 195 countries over
25 years. The New England journal of medicine,
377(1):13–27.
Allan, L. M., Ballard, C. G., Rowan, E. N., and Kenny, R. A.
(2009). Incidence and prediction of falls in demen-
tia: a prospective study in older people. PloS one,
4(5):e5521.
Andel, R., Crowe, M., Pedersen, N. L., Fratiglioni, L., Jo-
hansson, B., and Gatz, M. (2008). Physical exercise
at midlife and risk of dementia three decades later: a
population-based study of swedish twins. The Jour-
nals of Gerontology Series A: Biological Sciences and
Medical Sciences, 63(1):62–66.
Bolandzadeh, N., Kording, K., Salowitz, N., Davis, J. C.,
Hsu, L., Chan, A., Sharma, D., Blohm, G., and Liu-
Ambrose, T. (2015). Predicting cognitive function
Advances in Building BodyInNumbers Exercise and Wellness Health Strategy Framework
553

from clinical measures of physical function and health
status in older adults. PloS one, 10(3):e0119075.
Bruha, P., Moucek, R.,
ˇ
Snejdar, P., Bohmann, D., Kraft, V.,
and Rehor, P. (2017). Exercise and wellness health
strategy framework. BIOSTEC 2017, page 477.
Chmel´ık, F., Fr¨omel, K., Kˇren, F., Stelzer, J., Engelov´a,
L., Kudl´aˇcek, M., Mit´aˇs, J., et al. (2017). Interna-
tional database for research and educational support.
Indares.com. Online; accessed 2017-10-06.
Conn, V. S. (2010). Depressive symptom outcomes of phys-
ical activity interventions: meta-analysis findings. An-
nals of behavioral Medicine, 39(2):128–138.
Dunn, A. L. (2010). exercise programmes reduce anxiety
symptoms in sedentary patients with chronic illnesses.
Evidence-based mental health, 13(3):95–95.
Ellison, J., Nagamuthu, C., Vanderloo, S., McRae, B., and
Waters, C. (2016). Estimating chronic disease rates in
canada: which population-wide denominator to use?
Health promotion and chronic disease prevention in
Canada: research, policy and practice, 36(10):224.
Fenesi, B., Fang, H., Kovacevic, A., Oremus, M., Raina, P.,
and Heisz, J. J. (2016). Physical exercise moderates
the relationship of apolipoprotein e (apoe) genotype
and dementia risk: A population-based study. Journal
of Alzheimer’s Disease, (Preprint):1–7.
Grasgruber, P., Sebera, M., Hrazdira, E., Hrebickova, S.,
and Cacek, J. (2016). Food consumption and the ac-
tual statistics of cardiovascular diseases: an epidemi-
ological comparison of 42 european countries. Food
& nutrition research, 60(1):31694.
HAPPYneuron, G. S. (2017). My happy neuron. happy-
neuron.com/. Online; accessed 2017-10-06.
Harris, A., Waage, S., Ursin, H., Hansen,
˚
A. M., Bjorvatn,
B., and Eriksen, H. R. (2010). Cortisol, reaction time
test and health among offshore shift workers. Psy-
choneuroendocrinology, 35(9):1339–1347.
Kokkinos, P., Sheriff, H., and Kheirbek, R. (2011). Physical
inactivity and mortality risk. Cardiology research and
practice, 2011.
Lee, D.-c., Artero, E. G., Sui, X., and Blair, S. N. (2010).
Mortality trends in the general population: the im-
portance of cardiorespiratory fitness. Journal of Psy-
chopharmacology, 24(4
suppl):27–35.
Matura, S., Fleckenstein, J., Deichmann, R., Engeroff,
T., F¨uz´eki, E., Hattingen, E., Hellweg, R., Lienerth,
B., Pilatus, U., Schwarz, S., et al. (2017). Effects
of aerobic exercise on brain metabolism and grey
matter volume in older adults: results of the ran-
domised controlled smart trial. Translational psychi-
atry, 7(7):e1172.
Rizzoli, R., Bruy`ere, O., Cannata-Andia, J. B., Devoge-
laer, J.-P., Lyritis, G., Ringe, J., Vellas, B., and Re-
ginster, J.-Y. (2009). Management of osteoporosis in
the elderly. Current medical research and opinion,
25(10):2373–2387.
State of Play games (2014). Lumino city. luminoci-
tygame.com/. Online; accessed 2017-10-06.
Teri, L., Gibbons, L. E., McCurry, S. M., Logsdon, R. G.,
Buchner, D. M., Barlow, W. E., Kukull, W. A.,
LaCroix, A. Z., McCormick, W., and Larson, E. B.
(2003). Exercise plus behavioral management in pa-
tients with alzheimer disease: a randomized con-
trolled trial. Jama, 290(15):2015–2022.
Thomas, D. R. (2010). Sarcopenia. Clinics in geriatric
medicine, 26(2):331–346.
Vitabot.com (2017). Vitabot, online meal planning.
vitabot.com/web. Online; accessed 2017-10-06.
HEALTHINF 2018 - 11th International Conference on Health Informatics
554
