
How to Design Game-based Healthcare Applications for Children?
A Study on Children’s Game Preferences
A. F. A. de Vette
1
, M. Tabak
2
and M. M. R. Vollenbroek-Hutten
1
1
University of Twente, Faculty of Electrical Engineering, Mathematics and Computer Science,
Telemedicine Group, P.O. Box 217, 7500 AE Enschede, The Netherlands
http://www.utwente.nl/ewi/bss
2
Roessingh Research and Development, Telemedicine Group, P.O. Box 310, 7500 AH Enschede, The Netherlands
http://www.rrd.nl/
Keywords: Gaming, Game-based, Game Preferences, Gamification, Game Design, Framework, Classification,
Taxonomy, Player Type, Telemedicine, ehealth, Health Informatics, Tailoring, Adherence, Engagement,
Children, Asthma.
Abstract: Game-based design can be used to develop engaging health applications for children. This engagement can
only be realised when design is tailored to their preferences. In this study we investigate game preferences of
children and translate these into design recommendations. Game preferences of children aged 6 to 12 were
assessed through a questionnaire. Outcomes were classified by means of the 7D framework which divides
game content into seven linear domains. Significant differences in mean scores among demographic
subgroups were explored. Sixty-five children participated (M=9 years, SD=0.24, 36 boys, 29 girls, 8 children
with asthma). Data showed high preference for content in domains novelty (M
novelty
=63) and dedication
(M
dedication
=70). Analysis resulted in subdivision of scores based on gender, age and playing frequency.
Striking differences in scores were found between boys and girls in discord (M
boys
=62, M
girls
=19), intensity
(M
boys
=60, M
girls
=27), rivalry (M
boys
=53, M
girls
=31) and threat (M
boys
=64, M
girls
=25). To design games for
children we recommend to stimulate curiosity by offering variation and discovery, to enable achievement,
learning and social contact. A divergence in preferences for boys and girls must be regarded. Opposed to
boys, girls may lose interest in games that have violent or scary content, that are mainly competitive or demand
continuous effort.
1 INTRODUCTION
Health informatics can bridge the distance between
healthcare professionals and enable patients to
receive treatment in their daily living environment
(Jansen-Kosterink, 2014), thereby alleviating the
increasing demand for care and improving the
autonomy and quality of life of patients. Despite that
such telemedicine applications contribute to positive
health outcomes (Huis in 't Veld et al., 2010),
adherence seems restricted to several weeks of
use(Tabak et al., 2014, Evering, 2013). Game-based
design may be a strategy to increase adherence as
introducing elements of game content to telemedicine
applications is hypothesised to better engage the
patient in using the application (Primack et al., 2012),
thereby facilitating underlying treatment objectives
(Baranowski, 2008). Moreover, applying game-based
design may be able to sustain engagement for a
prolonged time.
In order to successfully design game content that
appeals to a specific target group, an understanding of
their preferences regarding this game content is
essential. To express these preferences, we can
describe the user in various ways. Two commonly
used approaches are player taxonomies and game
genre (or form) classifications. A well-known player
taxonomy is the Bartle player typology (Bartle,
1996), which classifies players into four types that
represent the player’s preferred behaviour within the
game. Such player taxonomies like Bartle or e.g.
(Yee, 2005) usually originate from analysis of a
specific type of game and its players, and can
therefore not be generalised or used outside of their
context (Dixon, 2011). Also, the classes the models
consist of are fixed and non-linear, thereby not
422
Vette, A., Tabak, M. and Vollenbroek-Hutten, M.
How to Design Game-based Healthcare Applications for Children? - A Study on Children’s Game Preferences.
DOI: 10.5220/0006584804220430
In Proceedings of the 11th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2018) - Volume 5: HEALTHINF, pages 422-430
ISBN: 978-989-758-281-3
Copyright © 2018 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
forming a complete description of all preferences a
user may have. The other approach, expressing
preferences through game genre or form (such as a
simulation, shooter, educational, role-playing, etc.),
gives an overall representation of a set of game
features, which is not uniformly described among
various game developers (Apperley, 2006). Neither
of these approaches therefore allow for accurate
assessment of preferences that is needed to synthesise
into recommendations for the design of new game
content, as the information on the player from a
player typology is limited and too high level from a
genre classification.
Instead, particularly as we envision to add game
content to healthcare applications to prolong
adherence, information on the player’s preferences
needs to be more detailed. This would correspond to
a model that allows us to describe games by their
actual characteristics, which would enable us to
express preference of the user for specific game
content on a much more profound level. We expect
that by using such a model, we have more insight in
how the individual should be addressed through game
design but also how a group of users should be
approached to realise more engagement.
As such, we developed a model for the
classification of game content in earlier work (De
Vette et al., 2017); the ‘7D framework’. This model
can be used to assess and map the preferences of users
for game content, resulting in a detailed description
of these preferences that can be used to design new
content. The model can be used to gain insight in
whether or not demographic or psychosocial
differences exist that may have implications on the
design of the game content should be taken into
account. The 7D framework can also be used to
analyse and make explicit the content of existing
games. The theoretical foundations for this model
originate from the five factor model of personality
(McCrae and Costa, 2008) and its translation into
gaming semantics, the five domains of play theory
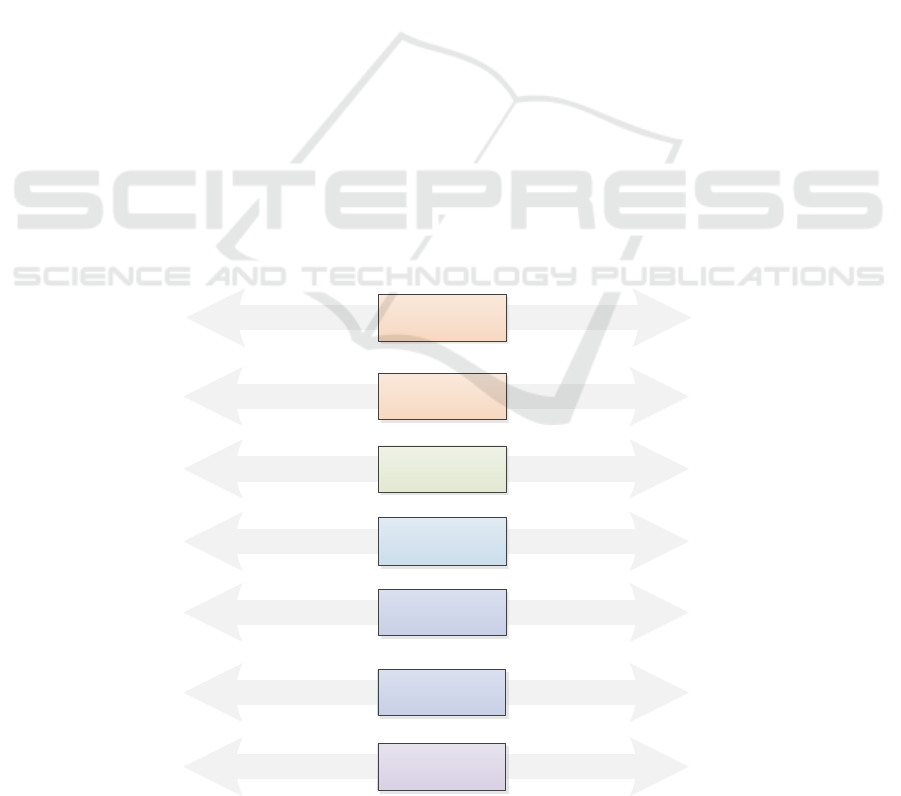
(Vandenberghe, 2012). The 7D framework structures
game content along seven linear domains that are
defined by a set of characteristics per each domain
extreme, as shown in figure 1. Discord and rivalry
were originally represented by a single domain in
previous versions of the model, as were social and
intensity, hence they have been given the same colour
in the figure.
Applying the 7D framework and its precursors to
investigate the preferences of older adults group
showed, in short, their preference for high novelty
content and (cognitive) challenges, and an outspoken
disfavour for intense, violent and frustrating content
(De Vette et al., 2015, 2017). This research resulted
in the development of a game-based self-management
platform for older adults (De Vette et al., 2016) using
a storyline, enabling exploration, containing puzzle-
Figure 1: The 7D framework - a model for game content along seven linear domains.
RivalryCooperation Competition
+-
Novelty
Dedication
Discord
Threat
Habitual
Simplicity
Low self-discipline
Mastery
Achievement
Commitment
Teamplay
Altruism
Fairness
Compassion
Serenity
Gaining, winning
Defeating
Strife
Cruelty
Destruction
Intimidation
Low social engagement
Non-communicative
Company, social interaction
Communicative
Familiarity
Routine
Expectedness
Curiosity
Surprise
Fantasy
Social
Intensity
Pacifism Violence
Casual Devoted
Conventional Novel
Solitary Multi-player
Slow-paced Exciting
Calm Stressful
No time pressure
Short attention span
Low speed
Safety
Comforting
Pleasant
Fast
Intense
Thrilling
Frustration
Gloom
Tension
Domain
+-
Characteristics Characteristics
-
+-
+
+-
-
+-
+
How to Design Game-based Healthcare Applications for Children? - A Study on Children’s Game Preferences
423

oriented mini-games to sustain the motivation of the
user. This game is currently under evaluation to study
its effectiveness, but from preliminary results we find
that the translation of the user preferences into game
design has been successful. Now, we aim to explore
the use of this model to gain insight in the preferences
of other groups.
Unlike the older adult, children are a more
common consumer of video games making the
success of a game-based approach in healthcare
applications more likely. Games are regularly applied
for children outside the goal of entertainment, and
numerous examples of serious games (Charlier et al.,
2016) and game-based learning programs can be
found (De Sousa Borges et al., 2014). However,
additional research is needed to determine the game
design that best promotes effectiveness of games in
health informatics (Baranowski., 2015). Just like
older adults (De Vette et al., 2015), children do not fit
within the researched target groups using existing
user classifications, nor do these models fit the
context of digital healthcare applications. To the best
of our knowledge, we are unaware of an existing
framework that can be used to measure and elaborate
game preferences of children on the level of core
game content.
In this study we aim to gain insight in the
preferences of children regarding game content and
translate these preferences into design
recommendations for engaging game content for
children. To do so, we assess the preferences of
children along the 7D framework and research
whether significant differences in preferences exist
among subgroups of children. This could give us a
starting position in tailoring game-based telemedicine
applications to this target group.
2 METHODS
2.1 Design and Participants
The study is cross-sectional. The participants were
school-going children in the age of 6 to 12 years old.
Local primary schools were invited for a Science Day
taking place at University of Twente, the Netherlands.
During this day, children were taught about the
university and invited to participate in all kinds of
activities related to technological innovation.
Participants and their parents were informed on
beforehand about the activities of the Science Day by
the organisation of the event through an information
letter. In addition, a second group of children with
asthma within the same age range participated one
day later. These participants were recruited via the
children's department at Medisch Spectrum Twente,
Enschede. For both groups, parents gave their
informed consent prior to participation. Also,
children’s participation was voluntary and no
exclusion criteria were applied.
One of the activities was playing on an interactive
playground developed in the AIRPlay project
(Klaassen et al., 2017), to support self-management
of children with asthma and to promote their physical
activity in a fun and unobtrusive manner. This
playground uses floor projection and movement
tracking to generate the playing field for a game
inspired by the children’s game ‘tag’.
2.2 Measures and Materials
We assessed the preferences of children by using a
questionnaire based on the 7D framework. The
domains, as shown in figure 1, are 1) discord, which
features peaceful versus violent content, 2) rivalry
features cooperation versus competition, 3)
dedication the appreciation of a game that requires
low self-discipline (‘casual’) versus a game that is
achievement-oriented (‘devoted’), 4) novelty the
preference for conventional, routinely or real-world
versus fantasy, curiosity and variation, 5) social
features the opposition of the amount of interaction
with others, between solitary and multiplayer, 6)
intensity holds slow and relaxed against fast, intense
and time pressured, 7) threat the acceptable amount
of negative feelings that the game can cause in the
player, ranging from calm and lovely to frustration
and fear.
Each domain is a linear scale (ranging from 0 to
100) described by two extremes. These extremes are
described by characteristics, that can be translated
into actual game features. We deduce our
recommendations for game design from the measured
scores on the different domains, and on our analysis
of scores of identified subgroups.
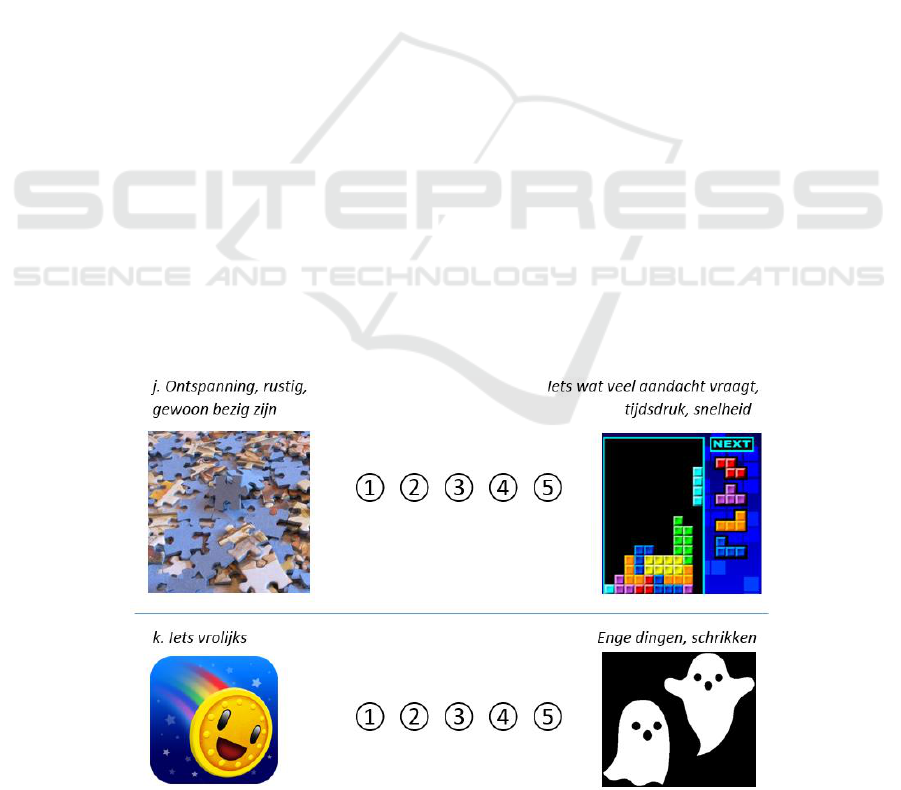
The questionnaire was adapted to the target group
by keeping the questions concise and illustrating them
with simple images. Also, the number of questions
was limited to a minimum of 11 questions by
measuring two aspects of the more complex domains
of rivalry, dedication, novelty and social, and one of
the simpler domains intensity, threat and discord. All
questions were rated on a 1 to 5 scale, each question
was illustrated by two images of the extremes and an
example in text (fig. 2). The question was ‘Which
[example] do you like more in a game?’ (“I like
[example A] better than [example B]”). The average
HEALTHINF 2018 - 11th International Conference on Health Informatics
424
scores were calculated for the seven domains and
expressed in terms of percentages.
Demographics, including information on
favourite games, playing behaviour and access to
devices, were assessed in the questionnaire.
2.3 Procedures
Measurements of both groups took place at
University of Twente and occurred in the same
manner. Groups of up to eight children were invited
to play on the interactive playground. The children
took turns in forming two teams of two players.
Playing continued for approximately five minutes.
Subsequently, the group of 8 participants was asked
to fill in the questionnaire.
2.4 Data Analysis
Data analysis was performed using Statistical
Package for Social Sciences (SPSS v.22). Data
distributions of the domains were analysed using the
Shapiro-Wilk test, descriptives and boxplots. All
domains were found non-normally distributed for all
participants. Results are presented as mean and
median domain scores. Subgroups were identified by
comparing mean scores and analysing significance
levels using the Mann-Whitney test for
nonparametric distributions.
The principal findings are presented in a visual
overview using the domain scores of all participant as
well as the most striking subgroup(s) based on the
highest number of significantly different domain
score means. Univariate linear regression analysis
was used to study the explained variance in the
domains by both gender and playing frequency.
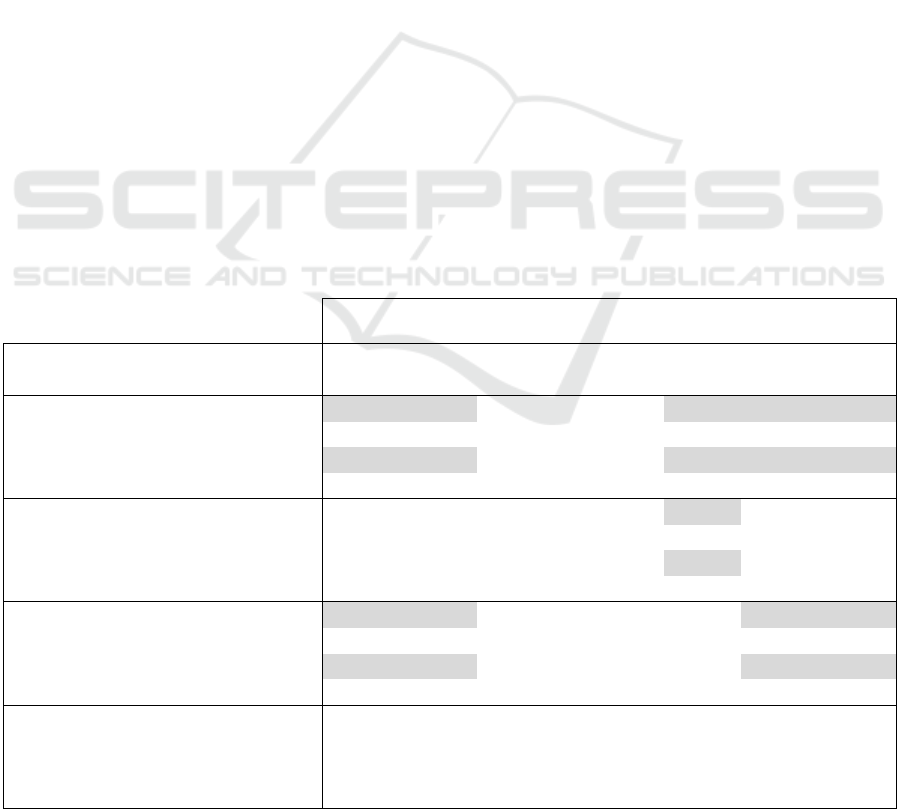
3 RESULTS
Sixty-five children participated (mean age 9, 36 boys
and 29 girls). Table 1 shows the game preferences of
all participants. Subgroups were identified in
comparing means in gender, age and playing
frequency. This resulted in partitioning of gender in
1) boys and 2) girls, age in 1) 6 to 9 years old and 2)
10 to 12 years old, and playing frequency in 1)
frequent players (daily to at least weekly) and 2) non-
frequent players (not regular to never at all). A
trending difference (p < 0,10) was found between the
scores of children with and without asthma on the
domain novelty (M asthma = 47, M non-asthma = 65).
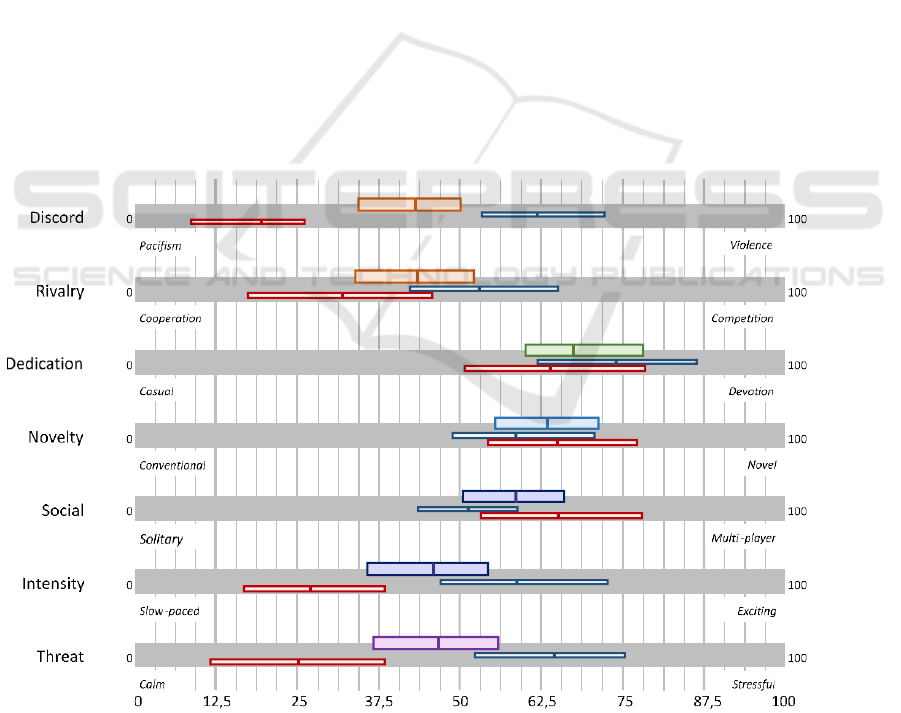
Figure 3 visualises the scores of all participants
and of boys and girls, as this subgroup shows the
largest number of significant differences. This graph
shows the uniformity in scores on dedication, novelty
and social, and the scores on discord, rivalry, intensity
and threat that appear to be determined by the clear
division in scores of boys and girls. The domains
dedication and novelty receive the highest scores
from all participants, indicating an outspoken
preference for content in these domains. The score on
dedication suggests that these children have a
preference for games that require effort and in which
goals can be achieved. The score on novelty suggests
a preference for variation, discovery, fantasy and
creativity instead of more predictable content, such as
football or racing. Significant differences were found
Figure 2: Fragment from the questionnaire (questions measuring intensity and threat).
How to Design Game-based Healthcare Applications for Children? - A Study on Children’s Game Preferences
425
between boys and girls on the domains discord,
rivalry, social, intensity and threat. Social
involvement through a game seems to be preferred by
girls more than boys. On average, girls indicate a
much different preference for discord, rivalry,
intensity and threat. On the scale of discord, in which
participants indicate their preferences between
peaceful and violent content, boys give a high and
girls a low score. A contrast of the same extent can be
found in intensity, that separates a relaxed activity
from one demanding focus and attention, and the
presence of time pressure and speed, and threat,
cheerful against disturbing content. Also in rivalry, in
which preference between working together and
competing as well as helping others to win against
defeating others is measured, boys indicated a much
higher preference for the latter.
A significant difference was found between the
means of the two age groups on the domain social (p
= 0,033). Upon analysis of the histograms of the two
age groups (data not shown) we find that the younger
group is more inclined to choose for the extremes
(values 1, 3 or 5) while the older group is capable of
indicating preferences on a more subtle level (also
using values 2 and 4). All except one participant, who
preferred playing alone, indicated to prefer playing
together with classmates, friends in the
neighbourhood or sports club and/or siblings or other
family members.
Significant differences in scores for different
playing frequencies were found in domains discord,
rivalry, intensity and threat (missing data for 8
children who did not answer this question). Frequent
players score on average about twice as high on these
domains than the less frequent players. 81% of boys
indicates to be a frequent player, of the girls this is
15%. However, there is a high significant correlation
between gender and playing frequency. Gender
shows to be a more important predictor for the
domain scores discord rivalry and threat than playing
frequency based on higher explained variance in
linear regression analyses, while playing frequency
was more important for the domain intensity (data not
shown). Subanalysis of the scores of frequently
playing boys (n = 25) and non-frequently playing
boys (n = 11) shows that their preferences differ on
the domain intensity (M frequent = 72, M non-
frequent = 34).
Looking into favourite devices and games of both
groups we see that children in the high playing
frequency group indicates to favour using consoles
such as PS4 to play games such as Call of Duty and
GTA, and children in the low playing frequency
group often do not indicate a specific favourite or
mention a website offering various mini-games. From
all participants, 14 children indicate a specific
console or PC game as their favourite game, 15
children mention Minecraft (5 of them girls).
Table 1: Average scores on the seven domains (significant differences (α < 0,05) in means highlighted).
Discord
Rivalry
Dedication
Novelty
Social
Intensity
Threat
All (n = 65)
mean
43
43
70
63
58
45
47
median
38
50
75
63
50
50
50
Boys (n = 36)
mean
62
53
74
60
51
60
64
median
63
50
100
63
50
75
75
Girls (n = 29)
mean
19
31
65
66
66
27
25
median
13
25
75
75
75
25
13
6-9 years (n = 28)
mean
47
47
67
64
50
42
49
median
44
50
100
69
50
50
50
10-12 years (n = 31)
mean
38
39
73
61
66
49
44
median
38
50
75
63
75
50
50
Frequent players (n = 29)
mean
58
53
76
66
53
67
66
median
63
50
100
63
50
75
75
Non-frequent players (n = 28)
mean
25
34
64
64
64
26
30
median
25
25
75
69
63
25
13
Asthma (n = 8)
mean
48
41
69
47
55
34
34
median
63
25
63
50
50
0
25
Non-asthma (n = 57)
mean
42
43
70
65
58
47
48
median
38
50
75
63
50
50
50
HEALTHINF 2018 - 11th International Conference on Health Informatics
426
4 RECOMMENDATIONS
Based on the findings of this study we recommend the
following when aiming to engage children through
game design. These recommendations suit the
approach of designing one game to address the full
target group.
Novelty: Focus on Stimulating the Children’s
Curiosity and Avoid Routine.
New game content should be introduced regularly.
Variation can be created through for example new
rules, mechanisms or visual elements. Enabling
children to use their imagination, be creative and add
their own variations to the content, or enable
emergent gameplay, may be a valuable feature. A
novelty theme (fantastical, fictional) may also be
more suitable than a real-world theme.
Dedication: Provide Content that Enables
Achievement.
Games should always be sufficiently challenging. For
children, it may demand an effort to learn skills
necessary to play the game. A trial-and-error
approach to do so can be rewarding. Include clear
feedback on achievements. Making content
unlockable may serve both the preferences on novelty
and dedication.
Social: A Game Should Enable Playing Together.
The preference for social contact is slightly dependent
on the age and gender ratio of the group, but in
general children prefer playing together rather than on
their own.
Discord and Threat: A Neutral Approach Would
Be Advised on Violence and Scary Content.
We observed a preference for violent video games
particularly in boys. Most girls may be put off quickly
by for example fighting games, as most boys will
probably not be interested in overly cute games.
Violent and scary game content should always be age
appropriate.
Rivalry: Competition and Cooperation May Be
Used Alternately to Keep a Game Interesting for
Both Boys and Girls.
In a multiplayer game, team play or 'helper' functions
may be added next to mechanics enabling
competition, such as setting challenges for other
players.
Figure 3: Overview of preferences mapped on the 7D framework (average and 95% interval domain scores) of all participants
(top), boys (middle, blue) and girls (lower, red). The upper box in each domain shows the average score of all users and the
95% interval. The smaller boxes show the scores of boys (middle) and girls (lower) in the same manner.
How to Design Game-based Healthcare Applications for Children? - A Study on Children’s Game Preferences
427

Intensity: A Moderate Intensity Should Address
Both Boys and Girls.
We do however recommend keeping in mind the
preference for lower intensity of most girls. Games
should provide the opportunity to choose an intense
as well as a more laid-back playing style to avoid girls
losing interest from a game that demands continuous
effort, movement or focus. We believe that this is the
case particularly when developing games that involve
physical exercise.
5 DISCUSSION
The aim of this study was to gain insight in the game
preferences of children, in order to synthesise
recommendations for game design to support the
development of engaging game-based telemedicine
applications. Using the 7D framework, the
preferences of 65 children were assessed resulting in
a graphical overview of preferences. The scores
suggest an overall approach towards game design for
this target group when attempting to engage all
members of the target group through one game, which
has been the basis for a set of game design
recommendations.
It is important to identify and take into account
different preferences from subgroups within a
population to avoid that game content is developed
that may either be too much of a compromise or is
disliked by the majority of one of both groups. While
gender was a more important predictor to game
preference in this study, we do not assume that we
should ignore playing frequency. We know that girls
are interested in games but that they prefer much
different characteristics (Kafai, 1998). The current
offer of videogames may determine that mostly boys
are the frequent players. There is a group of boys that
play frequently who indicated a much higher
preference for violent, intense and disturbing content
than the boys that play less often. Also, some have
access to consoles with games that may be considered
inappropriate for their age because of their violent
content. We expect that this subgroup may be hard to
please, if at all, as they are used to high-end games,
which moreover serve a set of preferences that may
put off many others.
Children with chronic conditions may form
another subgroup. Carefully interpreting the scores,
we expect that these children are more reserved
(lower novelty) and choose for a game that is less
intense (lower intensity). Recommendations for game
design for this group may include for example giving
them the chance to discretely take breaks or exhaust
themselves less than the others. More data is needed
to better understand the impact a chronic condition,
such as asthma, may have on game design.
Several aspects of this study lead to limitations
when generalising our findings for a greater public.
Firstly, our sample included children from local
primary schools. Cultural and educational differences
that may be of great influence on the results were not
taken into account. Divergent reading and writing
abilities among participants, not necessarily related to
age, may have led to misinterpretation of the
questions. Also, the Science Day and the playing on
the AIRPlay interactive playground may have
influenced the results. Secondly, validation of the 7D
framework is currently in progress. As such, the
creation of the questionnaire as well as the
interpretation scores into recommendations is to some
extent subjective. It is vital that the intention of the
designer is in accordance with the perception of the
target user on game content, future work should
include measures to align both frames of reference.
For example, a game designer may develop gameplay
that seems very intense for a child, while the child
itself interprets this differently. Furthermore, it
should be noted that the interpretation of the
recommendations given is open to the game designer,
as creating a satisfying game is not merely a sum of
parts but a design process in itself. As an example, a
high score on dedication indicates that it is more
likely that the user prefers game content that demands
devotion to play. This is described by the example
characteristics mastery, achievement and
commitment. In case of a high score on dedication,
we would recommend to include the need for skill
development in order to advance in the game (unlike
a more habitual game that would always require the
same amount of skill). A game designer may then
choose how to realise this aspect. Lastly, this study
included a limited number of participants with
asthma. We expect that minor differences will show
between the asthma and non-asthma group in a larger
dataset. At the time of writing the dataset is being
expanded with the data of more children with asthma.
In current and future work, we aim to fill in a
research gap on the existence of a method to elaborate
the preferences of any target group into a specific
characterisation to provide a starting position for
game-based design in health informatics. To ensure
validity of the 7D framework, we would propose to
extend research with 1) a comparison of the results
with existing literature on children’s playing
behaviour, preferences and personality, 2) creating a
more elaborate questionnaire that includes a larger
number of game content characteristics, as we assume
HEALTHINF 2018 - 11th International Conference on Health Informatics
428

this can lead to more detailed recommendations for
game design, and to 3) apply the design
recommendations in practice to evaluate to measure
their effectiveness in engaging the target group to the
healthcare application. Furthermore, we aim to
investigate if certain domains are more important than
others to the overall engagement when developing a
strategy for game design. In future work we aim to
respond to any differences that may be found in
preferences for children with or without chronic
conditions, in order to predict which strategies may
be successful for these children based on game
preferences, besides attitude or different physical
capabilities.
ACKNOWLEDGEMENTS
We would like to thank all participants and their
parents. This work was part of the AIRPlay project
(www.airplay.nl), financially supported by the
Pioneers in Healthcare Innovation Fund (PIHC round
2015). This fund (provided by University of Twente
and the hospitals Medisch Spectrum Twente and
Ziekenhuisgroep Twente) aims to facilitate the
introduction of innovative technology into the clinic.
REFERENCES
Jansen-Kosterink, S., 2014. The added value of
telemedicine services for physical rehabilitation.
University of Twente. [ISBN:9789082319606]
[PMID:17725187]
Huis in ’t Veld, RMHA., Kosterink, SM., Barbe, T.,
Lindegård, A., Marecek, T., Vollenbroek-Hutten,
MMR., 2010. Relation between patient satisfaction,
compliance and the clinical benefit of a teletreatment
application for chronic pain. J Telemed Telecare,
2010;16(6):322–8. [DOI:10.1258/jtt.2010.006006]
[ISBN:1758-1109 (Electronic)r1357-633X (Linking)]
[PMID:20798426]
Tabak, M., Brusse-Keizer, M., Valk, P. Van Der., Hermens,
H., Vollenbroek-Hutten, M., 2014. A telehealth
program for self-management of COPD exacerbations
and promotion of an active lifestyle: a pilot randomized
controlled trial. International journal of COPD.
DovePress; 2014. p. 935–44.
[DOI:10.2147/COPD.S60179]
Evering, RMH., 2013. Ambulatory Feedback at Daily
Physical Activity Patterns: A Treatment for the Chronic
Fatigue Syndrome in the Home Environment?
University of Twente.
[DOI:10.3990/1.9789036535120]
Primack, B., Carroll, M., McNamara, M., Klem, M., King,
B., et al. 2012. Role of Video Games in Improving
Health-Related Outcomes: A Systematic Review.
American Journal of Preventive Medicine 2012 vol: 42
(6) pp: 630-638.
Baranowski, T., Buday, R., Thompson, D., Baranowski, J.,
2007. Playing for Real: Video Games and Stories for
Health-Related Behavior Change. American Journal of
Preventive Medicine Volume 34, Issue 1, January 2008,
Pages 74–82.e10.
[DOI:10.1016/j.amepre.2007.09.027]
Bartle, RA., 1996. Hearts, clubs, diamonds, spades:
Players who suit MUDs. [URL:
http://mud.co.uk/richard/hcds.htm Archived at:
http://www.webcitation.org/6XvZlirzF]
Yee, N., 2015. Motivations of play in MMORPGs. Proc
DiGRA Conf Chang Views - Worlds Play 2005.
Dixon, D., 2011. Player Types and Gamification. CHI 2011
Work Gamification Using Game Des Elem NonGame
Context. 2011;12–5. [DOI:ACM 978-4503-0268-
5/11/05] [ISBN:9781450302685]
Apperley, TH., 2006. Genre and game studies: Toward a
critical approach to video game genres. Simul Gaming.
2006;37(1):6–23. [DOI:10.1177/1046878105282278]
McCrae, R., Costa, P., 2008. The Five-Factor Theory of
Personality. In: John OP, editor. Handbook of
Personality: Theory and Research, Guilford Press.
Vandenberghe, J., 2012. The 5 Domains of Play: Applying
Psychology's Big 5 Motivation Domains to Games.
De Vette, F., Tabak, M., Hermens, H., Vollenbroek-Hutten,
M., 2017. Mapping game preferences of older adults: a
field study towards a design model for game-based
applications. In progress.
De Vette, A.F.A., Tabak, M,. Hermens, H.J., Vollenbroek-
Hutten, M.M.R., 2015. Game preferences and
personality of older adult users. CHI PLAY
conference, London.
De Vette, F., Tabak, M., Hermens, H., Vollenbroek-Hutten,
M., 2016. Online gaming and training platform against
frailty in elderly people. Games for Health conference,
Utrecht.
Charlier, N., Zupancic, N., Fieuws, S., Denhaerynck, K.,
Zaman, B., Moons, P., 2016. Serious games for
improving knowledge and self-management in young
people with chronic conditions: a systematic review
and meta-analysis. J Am Med Inform
Assoc. 2016;23:230–9. [doi: 10.1093/jamia/ocv100]
De Sousa Borges, S., Durelli, V., Macedo Reis, H., Isotani,
S., 2014. A systematic mapping on gamification applied
to education. Proceedings of the 29th Annual ACM
Symposium on Applied Computing, March 24-28,
2014, Gyeongju, Republic of Korea.
[doi:10.1145/2554850.2554956]
Baranowski, T., Blumberg, F., Buday, R., DeSmet, A.,
Fiellin, L., Green, C., et al. 2015. Games for Health for
Children-Current Status and Needed Research. Games
Health J, 5( 1): 1–12. [doi:10.1089/g4h.2015.0026]
De Vette, F., Tabak, M., Dekker-van Weering, M.,
Vollenbroek-Hutten, M., 2015. Engaging Elderly
People in Telemedicine Through Gamification. JMIR
Serious Games, 3(2):e9, 2015.
How to Design Game-based Healthcare Applications for Children? - A Study on Children’s Game Preferences
429

Klaassen, R., Van Delden, R,. Cabrita, M., Tabak, M.,
2017. AIRPlay: Towards a ‘Breathgiving’ Approach.
Fitfth International Workshop on Behavioral Change
Support Systems (BCSS’17), Persuasive Technology
2017.
Kafai, Y., 1998. Video game designs by girls and boys:
variability and consistency of gender differences. In H.
Jenkins, & J. Cassell (1998) (Eds.), From Barbie to
Mortal Kombat (pp. 90-117). Cambridge, MA: MIT
Press
HEALTHINF 2018 - 11th International Conference on Health Informatics
430
