
Length of Hospital Stay Prediction through Unorganised Turing
Machines
Luigi Lella
1
and Ignazio Licata
2
1
Azienda Sanitaria Unica Regionale delle Marche, Ancona, Marche, Italy
2
Institute for Scientific Methodology, Bagheria, Sicily, Italy
Keywords: Data Mining, Pattern Recognition and Machine Learning, Healthcare Management Systems.
Abstract: Length of hospital stay (LoS) prediction is one of the most important goals in Health Informatics, due to the
fact that through this it is possible to optimize the management of health structure resources. In Italian local
healthcare systems we are experimenting an health cost containment process and the minimization of care
costs is considered an important objective to be achieved. For this reason we have tested several datamining
models trained with hospital discharge data, capable to make accurate LoS predictions. In another work we
have reached encouraging results by the use of unsupervised models which detect autonomously the subset
of non-class attributes to be considered in these classification tasks. Here we are interested in studying also
another intelligent data analysis model, the Turing unorganised A-type machine, that is capable to represent
the acquired knowledge in a logic formalism. In other terms this solution can explain its predictions by the
use of a set of self-acquired knowledge base rules.
1 INTRODUCTION
Length of hospital stay (LoS) prediction is
considered an important strategic objective for the
optimization of healthcare system resources (Wright
et al., 2003, Gomez and Abasolo, 2009). As a matter
of fact this kind of knowledge can lead to costs
containment by the reduction of hospital stays and
readmission rates (Chang et al., 2002, Robinson et
al., 1966). This is considered a factor of vital
importance in Italian States like Marche Region
where the central maneuver of health costs
containment has led to the overall reorganization of
healthcare system processes and to a consistent
reduction of hospital structures and beds. But this
kind of prediction can have also important clinical
outcomes, not just economic results. It has been
proved that the knowledge of the potential discharge
date can improve also long term care activities or
discharge activities planning (Rowan et al., 2007).
Several solutions have been adopted to cope with
LoS prediction. A first group is based on statistical
algorithms such as t-test, one-way ANOVA and
multifactor regression (Arab et al., 2010).
A second kind of methods is based on IA algorithms
such as decision trees and artificial neural networks
(ANN). ANN have produced important results in the
context of postoperative phase of cardiac patients
(Rowan et al., 2007) or in emergency rooms (Wrenn
et al., 2005).
Indeed the best results have been achieved by the
adoption of ensemble models (Jiang et al., 2010).
Learning techniques in general are based on a
structural knowledge representation, both symbolic
and subsymbolic. Subsymbolic models reach the
best results in LoS prediction (Tu and Guerriere,
1992). These models can be further subdivided in
classification algorithms (Jiang et al., 2010, Tu and
Guerriere, 1992), association algorithms (Agrawal
and Srikant, 1994), clustering algorithms (Kohonen,
1999, Van Hulle, 2012, Licata and Lella, 2007).
In classification learning a system is trained with a
set of samples to provide a class output to new
presented inputs. Unfortunately this approach is
effective only when the correlation among the class
and non-class attributes is clearly known
beforehand.
In LoS context this prerequisite cannot be
guaranteed. Sometimes the adoption of new
therapies and diagnostic techniques can result in an
increase of hospital stay. For this reason could be
very difficult to determine beforehand a classified
402
Lella, L. and Licata, I.
Length of Hospital Stay Prediction through Unorganised Turing Machines.
DOI: 10.5220/0006577804020407
In Proceedings of the 11th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2018) - Volume 5: HEALTHINF, pages 402-407
ISBN: 978-989-758-281-3
Copyright © 2018 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

set of samples, especially when there is a lack of
guidelines or clinical pathways.
In association learning classes are not defined at all.
The system just tries to detect interesting
correlations among attributes. But these kind of
systems don’t cope very well with LoS classes
prediction.
Finally clustering algorithms are “unsupervised”, in
other words there is not a set of classified examples
which can be used in the training phase of the
system. Just selecting the class attribute (i.e. the LoS
class), the system is simply capable to extrapolate
different clusters characterized by certain LoS
values. In this way it can be easily argued that
human expert knowledge is not needed.
SOM models are the clustering algorithms
(Kohonen, 1999) which have been used in LoS
prediction (Gorunescu et al., 2010), but in another
work (Lella and Licata, 2017) we have successfully
deployed an unsupervised algorithm which can
operate in contexts, like the LoS one, where there is
not a strong correlation among the class attribute and
the other ones. The Growing Neural Gas (GNG)
model by B. Fritzke (1994) that we have used, is
able to detect the exact number of needed attributes
to predict the class of hospital stay. We have
achieved interesting prediction accuracy levels, but
this subsymbolic model was not able to explain the
result using a logic formalism.
In this preliminary work we are studying another
unsupervised clustering algorithm which is based on
the Turing A-type unorganised machine (Turing,
1948). The Turing’s unorganised machine is
generated “in a unsystematic and random way” from
a set of two-input NAND gates. Turing chose a
NAND gate because every other logical operations
can be accomplished by a set of NAND units. A
Turing A-type unorganised machine can be
considered “a kind of Boolean neural network
without a layered structure, due to the fact that
recurrent connections are allowed with no
constraints” (Teuscher and Sanchez, 2000). We used
a genetic algorithm (GA) (Mitchell, 1996) to
determine the best A-type network configuration.
GAs are used to find high quality solutions in
optimization and search problems by relying on bio-
inspired operators of natural selection like mutation,
crossover and selection.
After the evolution, i.e. the training phase, the best
A-type network configuration is able to make LoS
predictions, providing an explanation of the results
through a logic formalism.
2 DATASET PREPROCESSING
We have processed the hospital discharge summary
forms provided by our health structures. In particular
we considered just a part of this dataset, which were
the attributes being filled at the admission of the
patients. The set of non-class attributes was:
recovery regimen, admission discipline, admission
division, provenance, recovery type, trauma, hospital
day care reason, hospital day care recovery type,
main diagnosis, main intervention, complications,
sex, age, marital status, qualification. The hospital
stay period was codified in a discretized form as
class attribute: one day hospital stay, two day
hospital stay, three days hospital stay, below
regional threshold stay, over regional threshold stay
(5 days).
Weka platform (Witten et al., 2011) was used to
launch Zero-R, One-R and J48 algorithms which
need a conversion of all the discretized values in a
nominal form by the use of “NumericToNominal”
filter.
We assumed that all the technologies and processes
of care have been kept unchanged in 2013, and we
processed all the hospital discharge summary forms
of the year. The initial dataset, made up of 274962
instances of hospital stay, was reduced to 1374
instances in order to speed up the training phase of
the tested models by the use of Weka “Resample”
filter.
The chosen self-organizing networks (SOM, GNG
and A-type network) were trained using the
methodology suggested by Kohonen (1999). Each
input vector was built by a concatenation of a
context part representing the length of hospital stay
of the instance and a symbol part consisting of the
other attributes. The symbol part and the context part
formed a vectorial sum of two orthogonal
components such that the norm of the second part
predominated over the norm of the former. Both the
symbol part and the context part were encoded in a
binary way. In particular discrete variables having
relatively few values were encoded using a one-hot
code system. For example the context part was
codified by 5 bits, with just one of them capable to
be in high (1) state. The main diagnosis and the main
intervention attributes were instead coded in binary
(base-2) representations. In this way each of the
hospital discharge cases was codified by an array of
104 bits for the symbol part (the binary
representation of the non-class attributes) and an
array of 5 bits for the context part.
Length of Hospital Stay Prediction through Unorganised Turing Machines
403
3 TRAINING AND TEST
The 66% of the resampled dataset was used as a
training set, while the remaining 34% was used as
test set. Both the symbol part and the context part of
the training set was used for the self-organizing
networks (SOM, GNG and A-type network), while
just the context part of the test set was used to test
the predictive accuracy of these models.
The first tested algorithm was the ZeroR (Witten et
al., 2011) that is used in many cases as a benchmark.
ZeroR predicts always the majority class in case of a
nominal class attribute, and it is considered the
simplest predictive algorithm.
The second tested algorithm was the OneR (Witten
et al., 2011, Holte, 1993), standing for “one rule”,
that generates a decision tree defined by just one
level. Each attribute value is assigned by a rule to
the most frequent class attribute. At the end of the
training phase just the rule with the lowest error rate
is used to make the predictions in the test phase.
This method has revealed a predictive power that is
a little lower than the ones belonging to other
decision tree models.
The third tested algorithm was the J48 (Witten et al.,
2011), that is the eighth version of C4.5 (Quinlan,
1993) that is the last version distributed as free
within this family of algorithms. J48 is based on a
“divide and conquer” algorithm and its decision tree
is recursively generated. At each training step the
node having the highest information quantity is
selected and a branch for each of its possible values
is created. This process stops when all the instances
belong to the same attribute class value.
The fourth tested algorithm was the SOM (Kohonen,
1999). A Self Organizing Map is a mapping of a
higher-dimensional input space. A two-dimensional
mapping was tested in this work. During the training
phase different parts of the network can respond
similarly to certain input patterns. The training is
based on competitive learning, that is just one unit
for each training input vector is selected as winner,
the one whose weight vector is closer to the input.
The fifth tested model was the GNG (Fritzke, 1994)
that is based on the Competitive Hebbian Learning
(CHL) (Martinetz, 1993) and the Neural Gas (NG)
(Martinetz and Shulten, 1991) algorithms. The
former deploys an initial number of centers, i.e.the
weight vectors of the units having the same
dimension of the input space, and subsequently adds
topological connections among the couples of
closest centers to the presented inputs. The other
algorithm adapts the k nearest centers, with k
decreasing from a large initial value to a small final
value. In this way the network topology is generated
incrementally by CHL, with a locally varying
dimensionality. The NG algorithm is used to move
the centers of the nearest unit and its topological
neighbours to the input signal by fractions
v
and
n
respectively of the total distance.
At last we chose an A-type model consisting of 24
NAND gates.
The first three algorithms were tested with Weka
default parameters.
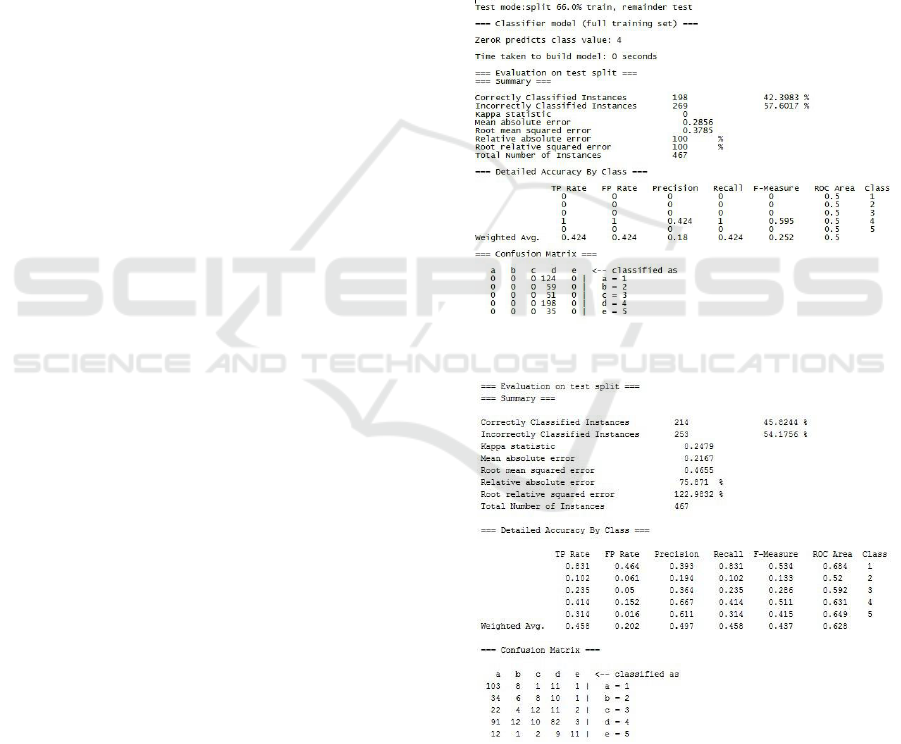
The output of ZeroR, OneR, J48 algorithms
provided by Weka Explorer are represented in
figures 1,2,3. As expected J48 seems to perform
better than the other two.
Figure 1: ZeroR prediction accuracy.
Figure 2: OneR prediction accuracy.
HEALTHINF 2018 - 11th International Conference on Health Informatics
404
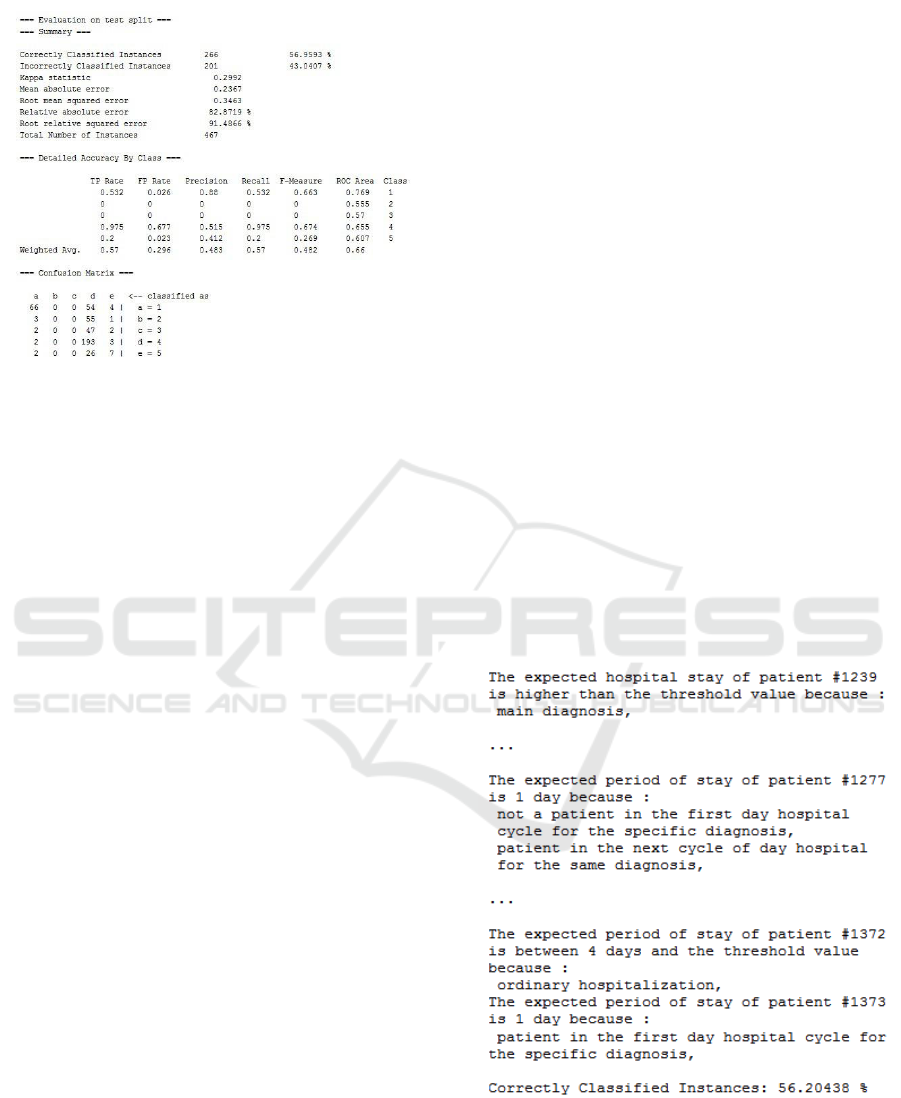
Figure 3: J48 prediction accuracy.
SOM and GNG models have been developed by
two Java implementations. The resampled dataset
was pre-processed as explained in section 2,
obtaining a 109-bits training set and a 109-bits test
set. In the test set we replaced the 5 bits representing
the context part by a zero padding.
A 12x12 SOM was trained for 500 epochs with
the following parameters: start =1, start =0.1, start
=0.5, end =0.005.
The GNG model was tested with the following
parameters:
v
n
max
The training was stopped when the
main square error, i.e. the main of the local square
error related to each unit (expected distortion error),
dropped below the threshold of E=1.
The prediction accuracy of 96,3597% of the GNG
model was considerably higher than the 87,5912%
of the SOM algorithm and the 56,9593% of the J48
algorithm.
Finally the A-type unorganised Turing machine was
tested by a Java implementation. The output of the
network was provided by just 5 units, to give a one-
hot answer. Each of the two inputs of the logic gates
was represented by the output of another NAND
gate or an input unit, that is one of the bits used to
codify the non-class attributes of the hospital
admission form. The overall network was made up
of 128 units, that is the sum of the 104 input units
(non-class attributes) and the 24 NAND gates.
Each of these units were codified by a 7-bit vector,
which is able to represent 128 units. The resulting
chromosome of the GA algorithm, modelling a
certain network configuration, was made up of an
array of 7x2x24=336 bits.
We evolved a population of 7000 chromosomes with
a mutation rate of 0.015.
We employed a tournament selection method (Miller
and Goldberg, 1995). Tournament selection involves
running several "tournaments" among a few
individuals, i.e. the chromosomes, chosen at random
from the population. The winner of each tournament,
that is the one with the best fitness rate, is selected
for crossover. Selection pressure is easily adjusted
by changing the tournament size. If the tournament
size is larger, weak individuals have a smaller
chance to be selected. We chose a tournament size
of 30 individuals. Crossover was implemented in the
single crossover point version.
We also employed the elitism (Baluja and Caruana
1995), meaning that at the end of each generation
the most performing individual was preserved by the
effects of mutation and crossover operators.
The fitness of the network was defined as the
number of correctly classified cases.
The evolution was stopped until we have reached a
prediction accuracy similar to the J48 one.
The evolution of the chromosomes population just
needed an average of 30 generations after that the
system was also able to justify its answers.
We took into consideration just the inputs of the
activated output unit to decode the answer.
Only few attributes were taken into consideration by
the system to give an answer as represented in figure
4.
Figure 4: A-type prediction accuracy.
The right answers provided by the system were
subsequently validated by a team of human experts
chosen within the ASUR medical staff.
Length of Hospital Stay Prediction through Unorganised Turing Machines
405

4 CONCLUSIONS
We actually know that there are not universal
datamining techniques or methodologies to deal with
every kind of problem or task. For length of hospital
stay prediction we think that only unsupervised
models can achieve the best results, because there is
a lack precise guidelines and best practices capable
to infer exactly the period of staying of patients,
especially in those contexts characterized by rapid
changes in technologies and organizational settings.
In other words the knowledge of human experts in
these cases cannot be exploited to define an accurate
LoS prediction system.
For this reason in our research we have focused on
unsupervised machine learning algorithms, in
particular clustering algorithms and self-organizing
networks.
We have obtained encouraging results through the
use of subsymbolic models like the Growing Neural
Gas by B. Fritzke in a previous research work, but
now we are trying to develop more “intelligent” data
analysers which are also capable to give a human-
understandable explanation of their predictions. A
response produced according to a logic formalism
could indeed support decision makers in their health
resources and services management activities.
That is why we have chosen an A-type unorganised
Turing machine to process the admission forms of
hospital patients. The structure itself of the model
could be used like a kind of “dynamic” guideline to
be taken into consideration by a group of human
experts in order to optimally organize the healthcare
activities performed on patients.
The knowledge acquired by an unorganised Turing
machine through its pattern of NAND gates
connections could also be used to produce an
explanation of the reasons that led the system to its
LoS predictions as we have demonstrated in this
preliminary work.
We stopped the training just after having reached the
prediction accuracy of the most performant decision
tree algorithm represented by the J48. Also this
model could be used to build a knowledge
representation to approach the LoS prediction
problem. But its tree-like structure probably is too
simple to generate the complex set of rules to be
used in these kind of decision processes.
We think that these first results can be further
improved adopting another unorganised Turing
machine model, that is the B-type one (Turing,
1948). Also a B-type may contain any number of
NAND gates connected in any pattern. Turing just
added the further condition that each unit-to-unit
connection must pass through a modifier device. The
modifier state can be set in “pass mode”, in which
the output of a NAND gate passes through it
unchanged, or in “interrupt mode”, in which the
signal is always 1, no matter what the output of the
NAND gate is (Copeland and Proudfoot, 1996). The
presence of the modifiers can enable what Turing
described as “appropriate interference, mimicking
education”.
We are going to design and test a two-phase
training, similar to the one proposed by Teuscher
and Sanchez (2000), with a first “evolutive” phase
where the best network configuration is selected,
and a “learning” phase where the switches of
NAND gates are enabled and properly configured to
optimize the prediction accuracy rate.
ACKNOWLEDGEMENTS
Special thanks go to Eng. Antonio Di Giorgio for his
support in Weka datamining processes.
REFERENCES
Agrawal R., Srikant R., 1994. Fast Algorithms for Mining
Association Rules. Proc. Of the 20th VLDB
Conference, Santiago, Chile, 1994.
Arab M., Zarei A., Rahimi A., Rezaiean F., Akbari F.,
2010. Analysis of factors affecting length of stay in
public hospitals in Lorestan Province, Iran, Hakim
Res, Vol. 12, No.4, 2010, pp.27-32.
Baluja S., Caruana R., 1995. Removing the genetics from
the standard genetic algorithm ICML.
Chang K.C., Tseng M.C., Weng H.H., Lin Y.H., Liou
C.W., Tan T.Y., 2002. Prediction of length of stay of
first-ever ischemic stroke, Stroke, Vol. 33, No.11,
2002 pp.2670-4.
Copeland B.J., Proudfoot D., 1996, Alan Turing’s
forgotten ideas in computer science. Sci.Am. n.280,
pp. 76-81.
Fritzke B., 1994. A Growing Neural Gas Network Learns
Topologies. Part of: Advances in Neural Information
Processing Systems 7, NIPS, 1994.
Gomez V., Abasolo J.E., 2009. Using data mining to
describe long hospital stays, Paradigma, Vol. 3, No.1,
2009, pp.1-10.
Gorunescu F., El-Darzi E., Belciug S., Gorunescu M.,
2010. Patient grouping optimization using hybrid Self-
Organizing Map and Gaussian Mixture Model for
length of stay-based clustering system, Intelligent
Systems (IS), 2010 5
th
International Conference.
Holte R.C., 1993. Very simple classification rules perform
well on most commonly used datasets, Machine
Learning, 1993.
HEALTHINF 2018 - 11th International Conference on Health Informatics
406

Jiang X., Qu X., Davis L., 2010. Using data mining to
analyze patient discharge data for an urban hospital,
In: Proceedings of the 2010 International Conference
on Data Mining, 2010 Jul 12-15; Las Vegas, NV., pp.
139-44.
Kohonen T., 1999. The Self Organizing Map, Proc. Of the
IEEE, vol.78, No.9, 1999.
Lella L., Licata I., 2017. Prediction of Length of Hospital
Stay using a Growing Neural Gas Model, in
Proceedings of the 8
th
International Multi-Conference
on Complexity, Informatics and Cybernetics (IMCIC
2017), pp. 175-178
Licata I., Lella L., 2007. Evolutionary Neural Gas (ENG):
A model of self-organizing network from input
categorization, EJTP, Vol.4, No.14, 2007.
Martinetz T.M., 1993. Competitive Hebbian learning rule
forms perfectly topology preserving maps. In
ICANN’93: International Conference on Artificial
Neural Networks, pp. 427-434. Amsterdam. Springer,
1993.
Martinetz T.M., Schulten K.J., 1991. A neural gas network
learns topologies. In T. Kohonen, K. Kakisara, O.
Simula, and J. Kangas, Editors, Artificial Neural
Networks, pp. 397-402. North-Holland. Amsterdam,
1991.
Miller B., Goldberg D., 1995. Genetic Algorithms,
Tournament Selection, and the Effects of
Noise, Complex Systems. 9, pp. 193–212.
Mitchell M., 1996. An Introduction to Genetic Algorithms,
Cambridge, MA: MIT Press, 1996.
Quinlan J. R., 1993. C4.5: Programs for Machine
Learning, Morgan Kaufmann Publishers, 1993.
Robinson G.H., Davis L.E., Leifer R.P., 1966. Prediction
of hospital length of stay, Health Serv Res Vol.1,
No.3, 1966 pp.287-300.
Rowan M., Ryan T., Hegarty F., O'Hare N., 2007. The use
of artificial neural networks to stratify the length of
stay of cardiac patients based on preoperative and
initial postoperative factor,. Artif Intell Med, Vol. 40,
No.3, 2007 pp.211-21.
Teuscher C., Sanchez E., 2000. A Revival of Turing’s
Forgotten Connectionist Ideas: Exploring
Unorganized Machines. In Proceedings of the 6th
Neural Computation and Psychology Workshop,
NCPW6, University of Lige, 2000.
Tu J.V., Guerriere M.R., 1992. Use of a neural network as
a predictive instrument for length of stay in the
intensive care unit following cardiac surgery, Proc
Annu SympComput Appl Med Care, pp. 666-72,
1992.
Turing A., 1948. Intelligent Machinery, in Collected
Works of A.M.Turing:Mechanical Intelligence. Edited
by D.C.Ince.Elsevier Science Publishers, 1992.
Van Hulle M.M., 2012. Self Organizing Maps, Handbook
of Natural Computing, pp. 585-622, 2012.
Witten I.H., Frank E., Hall M.A., 2011. Data Mining
Practical Machine Learning Tools and Techniques,
Morgan Kaufmann Publishers, 2011.
Wrenn J., Jones I., Lanaghan K., Congdon C.B., Aronsky
D., 2005. Estimating patient's length of stay in the
Emergency Department with an artificial neural
network, AMIA Annu Symp Proc pp. 2005-1155,
2005.
Wright S.P., Verouhis D., Gamble G., Swedberg K.,
Sharpe N., Doughty R.N., 2003. Factors influencing
the length of hospital stay of patients with heart
failure, Eur. J Heart Fail, Vol. 5, No.2, 2003, pp. 201-
9.
Length of Hospital Stay Prediction through Unorganised Turing Machines
407
