
Exercise and Wellness Health Strategy Framework
Software Prototype for Rapid Collection and Storage of Heterogeneous Health
Related Data
Petr Br˚uha
1, 2
, Roman Mouˇcek
1,2
, Pavel
ˇ
Snejdar
1
, David Bohmann
1
, V´aclav Kraft
1
and Peter Rehor
1
1
Department of Computer Science and Engineering, Faculty of Applied Sciences, University of West Bohemia,
Univerzitn´ı 8, Pilsen, Czech Republic
2
NTIS - New Technologies for the Information Society, Faculty of Applied Sciences, University of West Bohemia,
Univerzitn´ı 8, Pilsen, Czech Republic
Keywords:
Exercise and Wellness, Chronic Disease, Health Related Data, Health Informatics Systems, Software
Prototype.
Abstract:
Unwillingness of many people to assume responsibilities for a personal health, fitness and wellness seems to
be widespread. This can be partially remedied by individualized exercise and wellness program that integrates
the basic knowledge domains: lifestyle, sports and fitness, and nutrition and personal/environmental health.
However, collection, management and analysis of data and metadata related to these domains is demanding
and time consuming task. Moreover, the appropriate annotation of raw data is crucial for their next process-
ing. To promote such a program a software infrastructure for collection, storage, management, analysis and
interpretation of health related data and metadata has been proposed and part of this infrastructure has been
developed and tested outside laboratory conditions. This software prototype allows experimenters to collect
various heterogeneous health related data in a highly organized and efficient way. Data are then evaluated and
users can view relevant information related to their health and fitness.
1 INTRODUCTION
In the countries of the European Union (EU) deaths
due to chronic diseases are projected to increase. It
was estimated that out of the projected millions of
people who would die by 2015, 64% of them die
of a chronic disease – unless urgent action is taken
(Tunstall-Pedoe, 2006). Given that both physical in-
activity and obesity are strong independent causes
and predictors of chronic illness and disability, it has
been estimated that they impose a significant eco-
nomic burden on the health-care system in EU. The
most recent research in EU indicates that only 7.5%
of children and 15% of adults are physically active
for at least 150 minutes per week, while over 18%
are obese and over 46% are overweight (Busse, 2010;
Organization et al., 2010; Webber et al., 2014).
It is apparent that physical activity is essential in
the prevention of chronic disease and premature death
(Lee and Skerrett, 2001). Chronic diseases develop
over ones lifetime, with clinical symptoms occurring
many years after the underlying origins of the disease
have occurred. As we move ahead in the 21st century,
cardiovascular diseases, i.e. coronary artery disease
(CAD) hypertension, stroke, and heart failure, type
2 diabetes, metabolic syndrome, and cancer are the
leading killers in westernized society and are increas-
ing dramatically in developing nations. Physical inac-
tivity is a modifiablerisk factor for cardiovasculardis-
ease and a widening variety of other chronic diseases,
including diabetes mellitus, cancer (colon and breast),
obesity, hypertension, bone and joint diseases (osteo-
porosis and osteoarthritis), and depression 1-14 (Tay-
lor et al., 2004; Blair et al., 2001; Shephard, 2001).
The onset of progression of chronic diseases is
mediated in the vast majority of cases by an interac-
tion between genetic factors and their interaction with
environmental factors. These environmental factors
are largely lifestyle factors, namely physical activity
and dietary patterns, but also include other influences,
such as smoking, alcohol consumption, stress, and
hazardous environmental compounds. These factors
are modifiable, and, as such, disease manifestations
from these factors are largely preventable.
To cope with these modifiable factors exercise and
wellness intervention programs have been introduced,
mainly in the United, States, Canada and Australia.
This paper presents the first steps that have been done
BrÅ
´
rha P., MouÄ ek R., Å
˘
anejdar P., Bohmann D., Kraft V. and Rehor P.
Exercise and Wellness Health Strategy Framework - Software Prototype for Rapid Collection and Storage of Heterogeneous Health Related Data.
DOI: 10.5220/0006296604770483
In Proceedings of the 10th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2017), pages 477-483
ISBN: 978-989-758-213-4
Copyright
c
2017 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
477

to introduce such exercise and wellness health strat-
egy framework and related academic program within
the European Union. Its attempt is to create profes-
sionals who are capable influence self-care practices
positively, reinforce healthy habits and prepare re-
sponsible citizens for the future. This innovative, ap-
plied and unique initiative combines three tradition-
ally exclusive disciplines (Etiology of Chronic Dis-
ease, Exercise Science and Behavioral Psychology)
into one comprehensive curriculum that addresses
two major front page challenges in Europe: chronic
disease management and sedentary lifestyle. It is be-
ing applied through extensive clinical and fieldwork
experiences, the degree will provide students with the
theoretical knowledge, practical skills, and prerequi-
sites that are necessary to provide a professional guid-
ance during lifestyle changes.
Such exercise and wellness health strategy frame-
work needs a supportive software infrastructure that
besides others promotes collection of health related
data and metadata followed by their further annota-
tion, processing and visualization. This paper intro-
duces the first version of such software infrastruc-
ture,a software prototype that focuses on definition
and automation of the data collection process in order
to capture a huge amount of heterogeneous health re-
lated data from many users in various environment in
a short time. It is assumed that the procedure of data
collection has to be as short and user friendly as pos-
sible to significantly promote the initial participants’
motivation to cope with the most important step, a de-
sired change of participants’ behavior leading to their
better physical, emotional and mental health.
The paper is organized in the following way.
The next section discusses some questions related to
chronic illnesses, personal physical, emotional and
mental well-being and the necessity of exercise and
wellness strategy framework to cope with these mat-
ters. The third section introduces a supportive soft-
ware infrastructure for such a framework. The sub-
sections then present the first version of this software
infrastructure from architectural, implementation, de-
ployment and testing points of view. The last section
brings concludingremarks and introduces future steps
and improvements.
2 EXERCISE AND WELLNESS
HEALTH STRATEGY
FRAMEWORK
Chronic illness has profound effects on a persons
physical, emotional, and mental well-being, which of-
ten make it difficult to carry on with daily routines and
relationships. Over the past decades, considerable
knowledge has accumulated concerning the signifi-
cance of exercise in the treatment of a number of dis-
eases, including diseases that do not primarily mani-
fest as disorders of the locomotive apparatus. Today,
exercise is indicated in the treatment of a large num-
ber of additional medical disorders. In the medical
world, it is traditional to prescribe the evidence-based
treatment known to be the most effective and entail-
ing the fewest side effects or risks. The evidence sug-
gests that an exercise therapy is just as effective as
medical treatment in selected cases and even more ef-
fective or improving the final effect in special situa-
tions. In this context, exercise therapy does not repre-
sent a paradigm change, it is rather that the accumu-
lated knowledge is now so extensive that it has to be
implemented.
There is a growing interest in the use of exercise
for clients with chronic diseases and disabilities. It
is thus suitable to provide a framework for determin-
ing functional capacity and developing exercise strat-
egy in persons with chronic diseases and/or disabil-
ities. The basic principles for exercise testing and
training stated provides the foundation for program
design. However, some special situations created by
a disease pathology, disability, or treatment alter these
basic principles. For example, exercise testing is an
important aspect of the approach used, but some peo-
ple will not have completed an exercise test before
starting an exercise program. Participation in regular
physical activity can enhance functional capacity, and
a primary goal is to get more individuals physically
active. Thus, for many people, exercise testing may
not be absolutely necessary before starting a low-level
physical activity program.
Many people who have chronic disease or disabil-
ity enter a downward spiral toward exercise intoler-
ance, so exercise intervention programs should be de-
signed to resist this spiral and optimize functional ca-
pacity. Within any given population, there is a wide
range of abilities determined by several factors; pro-
gression of the disease, response to treatment, and
presence of other concomitant illnesses. Expected
outcomes of exercise training are not always known.
Realistically, optimal exercise and medical program-
ming may yield improvements or merely prevent fur-
ther deterioration. There may be recommended tests
or programs that have not been validated, but that ex-
perience has shown to be successful. It is hoped that
optimal management will bring the individual greater
independence and improved quality of life.
In general, our society has a bias toward curative
rather than palliative medicine, toward making the
HEALTHINF 2017 - 10th International Conference on Health Informatics
478
disease go away rather than finding ways to cope with
disease. An unfortunate consequence of this perspec-
tive is that for persons with chronic disease or dis-
ability, we devalue the palliative benefits of preserv-
ing functionality and well-being. Since the 1960s,
exercise has been promoted as a method of extend-
ing life, largely through prevention and moderation of
cardiovasculardisease. In recent years we discovered,
however, that perhaps the greatest potential benefit
of exercise is its ability to strengthen musculoskele-
tal system structure and function, enhance function-
ing of cardiovascular, digestive and endocrine system
and to augment mental capacity through changes in
body chemistry. Its side effects unlike other pharma-
cological interventionsare positive (improvement and
preservation in functional capacity, freedom, and in-
dependence).
The frameworks and applications that cope with
the questions of health and wellness and that are avail-
able to the broad public audience are described e.g.
in (Banos et al., 2015; Joo et al., 2012; Laakko et al.,
2008).
3 SUPPORTIVE SOFTWARE
INFRASTRUCTURE
3.1 Software Requirements
Specification
This section introduces a supportive software infras-
tructure for the exercise and wellness health strategy
framework. This infrastructurewill providemeans for
definition of the data collection procedure and data
collection itself, repository for storing and long term
management of health related data and metadata in
a standardizedway, data processing and interpretation
methods and/or defined interfaces for the application
of data processing and interpretation methods. Last
but not least visualization tools providing views on
collected/analyzed data and their interpretations will
be included.
An important aspect of this supportive software
infrastructure is its wide range that includes collect-
ing data from classic measurements such as blood
pressure to relatively rare kinds of measurements such
as acquisition of brain frequencies or brain event re-
lated potentials. It means that also experience of
experimenters from the neuroinformatics lab (refer-
ence omitted for a review process) in measuring brain
waves highly contributed to the definition of the first
set of collected health related human body parame-
ters.
Since big health related data (from at least thou-
sands of people) are planned to be stored in the reposi-
tory of this software infrastructure, the future analysis
of interdependence between brain parameter values,
other physiological and body proportion values and
personal lifestyle recordswould bring valuable results
for the targeted application of exercise and wellness
health framework strategies.
Thus the whole infrastructure will enable to find
out complex information related to health conditions
of each participant and derive statistical results when
defining various cohorts. With long-term and re-
peated measurements appropriate software modules
will be able to detect and depict personal trends and
changes in measured values.
However, the preliminary version of the soft-
ware infrastructure presented in this article (hereafter
called a software prototype) is required to help exper-
imenters to efficiently collect all health related data
and metadata outside the laboratory environment in
one session according to the procedure that could be
defined even on site. The schema of such experimen-
tal procedure (that contains a limited set of measure-
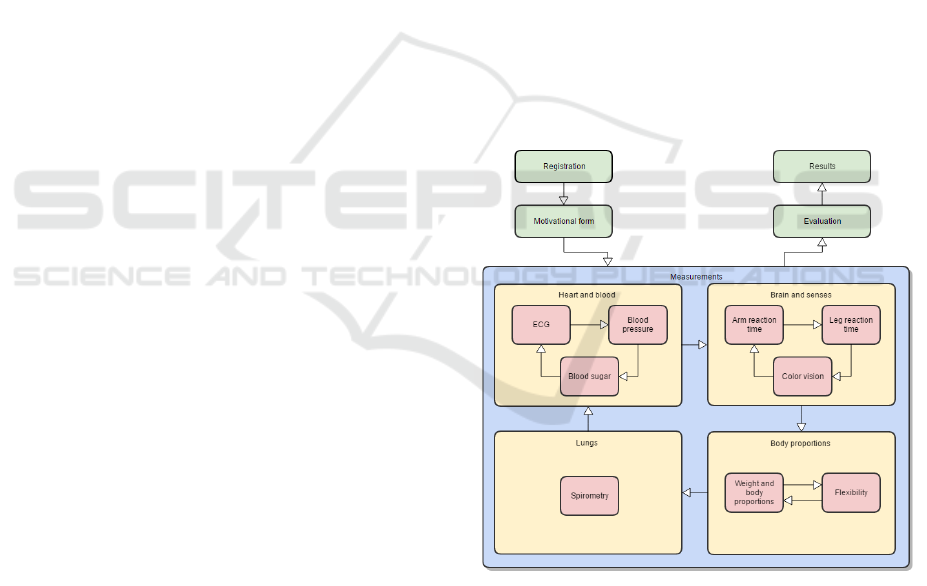
ments) is depicted in Figure 1.
Figure 1: Experimental procedure.
The measured person starts with his/her registra-
tion, where he/she agrees with the collection and pro-
cessing of his/her personal and health related data (in-
formed consent) and provides basic information about
himself/herself (name, sex, age, etc.). After the regis-
tration he/she proceeds to fill in a motivational ques-
tionnaire containing a set of 10-15 single choice ques-
tions related to his/her lifestyle. Then the measure-
ment cycle starts (as shown in Figure 1). Individual
Exercise and Wellness Health Strategy Framework - Software Prototype for Rapid Collection and Storage of Heterogeneous Health Related
Data
479

measurementsare grouped into sections depending on
measured parameters of human body. Every section
includes one or more physical sites where the exper-
imenter takes the measurement. When a single mea-
surement is completed, the acquired data are inserted
via a user interface into the system and sent to the
server. When the whole set of measurements is com-
pleted, the data are evaluated, sent back to the client
application and the participant can see his/her results
extended with additional information. The whole pro-
cedure shown in Figure 1 takes approximately 10–15
minutes.
The following list contains the current set of de-
fined physical sites and health related data acquired at
these sites:
1. Brain
• P300 latency [ms]
• Fundamental frequency during concentration
[Hz]
• Fundamental frequency during meditation [Hz]
2. Body proportions
• Height [cm]
• Weight [kg]
• Muscle mass [kg] or [%]
• Body fat [kg] or [%]
• Body water [kg] or [%]
• Body Mass Index (BMI)
3. Electrocardiography (ECG)
• Heart rate [BPM]
• ST segment [ms]
• QRS complex [ms]
4. Blood pressure
• Heart rate [BPM]
• Systolic pressure [mm Hg]
• Diastolic pressure [mm Hg]
5. Blood sugar
• Concentration of glucose [mmol/l]
6. Spirometry
• FVC (Forced Vital Capacity) [l]
• FEV1 (Forced Expiratory Volume in 1st sec-
ond) [l]
• PEF (Peak Expiratory Flow) [l/s]
7. Hand reaction time
• Average reaction time [ms]
• Number of falsely pressed buttons
• Number of missed buttons
8. Leg reaction time
• Average reaction time [ms]
• Best reaction time [ms]
• Worst reaction time [ms]
• Standard deviation [ms]
9. Flexibility
• Difference between fingers and foot during
deep forward bend [cm]
10. Color vision
• Number of wrongly recognized pseudoisochro-
matic tables
The whole software infrastructure as well as the
current software prototype is designed in a way that
allows easy enrollment of any future health related
data category, it means with any new collection of
health related data and metadata that could be de-
fined even on site (just before the measurement). This
put further requirements on the flexibility of the data
model itself and the technologies used for its repre-
sentation.
The software prototype can work in the online (de-
fault) or offline mode. When it is connected to the
Internet, it sends all input data directly to the main
server and receives back results and additional data.
When the Internet connection is not available, the pro-
totype switches to the offline mode. In this mode all
data are stored to a local repository and sent to the
server immediately when the Internet connection is
again available.
The parametric requirements on the prototype ap-
plication include its performance (input of health re-
lated data does not produce any visible delay), mobil-
ity (application can be used outside laboratory con-
ditions when several hundreds people are measured
during a day), simplicity and user friendliness (exper-
imenters are able to work with the application after
five minutes of training in the worst case).
3.2 Architecture and Design
The architecture of the software prototype is shown
in Figure 2. It follows the MVC architectural pattern
and client server architectural style.
The functionalities are encapsulated in modules
that can be added as plugins.
• The General module covers functionalitiesafford-
able also for non-logged users.
• The Admin module serves for the administration
of users and application setting.
• The Auth module is responsible for user registra-
tion and login.
HEALTHINF 2017 - 10th International Conference on Health Informatics
480
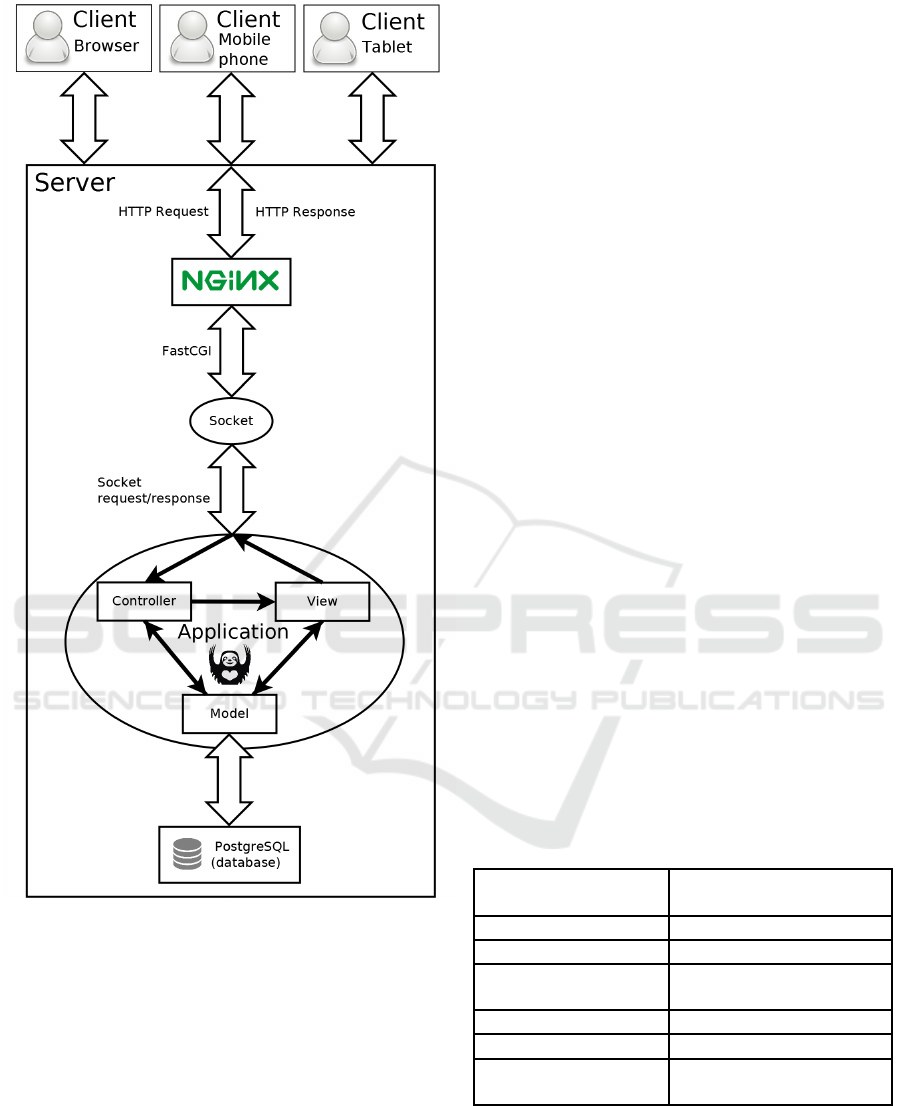
Figure 2: Software prototype architecture.
• The Measurement module includes definition of
measurement procedure and overall data manage-
ment.
• The Experiment module provides features for
adding, editing and deleting experiments.
• Every experiment needs own equipment for mea-
suring devices. The Equipment module stores
them in the database and provides tools for their
management.
• The QR generator module generates QR codes
into a PDF document given to the participant.
Each person has his/her number identifier in-
cluded in his/her QR code.
• The Statistics module currently includes a func-
tion for simple statistics of reaction time.
Rest API is defined for collecting data from client
devices.
3.3 Implementation and Deployment
The software prototype has been written in Python 3
language and uses the Flask micro framework that is
based on the Werkzeug toolkit and Jinja2 template en-
gine. The used languages and technologies include
Python, HTML5, CSS3, Flask, Sqlalchemy, and Post-
gre SQL.
The Postgre SQL database is used for storing data.
As a representative of open source object-relational
database system it offers significant support for stor-
ing and retrieving JSON documents. Object relational
mapping is provided by the SqlAlchemy framework.
The current ERA model of the software prototype is
shown in Figure 3.
The application is hosted by a virtualized server
having the technical parameters provided in Table 1.
The web server NGINX listens on two ports (the
first port is used for the release version and the sec-
ond one for the development version). NGNIX ex-
tends HTTP requests for non-standard headers CORS
(cross-origin resource sharing) technology which is
important for communication with mobile devices.
NGINX passes requests to the python application
with FastCGI protocol by a socket. Both development
and release versions run five instances. The process
describing how the requests are handled by the server
is shown in Figure 2.
Table 1: Server hardware and software specifications.
Processor
Intel(R) Xeon(R) CPU
E5-4620 v2 @ 2.60GHz
Memory 8036MB
Hard disk capacity 100GB
Operating system
Debian 8.4 with kernel
2.6
Web server
NGINX 1.6.2
Database Postgres 9.4
Language and tech-
nologies
Python 3 using frame-
work Flask
3.4 Testing
The software prototype has been tested on 346 people
in real environment (e.g. Days of science and tech-
nologies that were held in large tents on the square)
Exercise and Wellness Health Strategy Framework - Software Prototype for Rapid Collection and Storage of Heterogeneous Health Related
Data
481
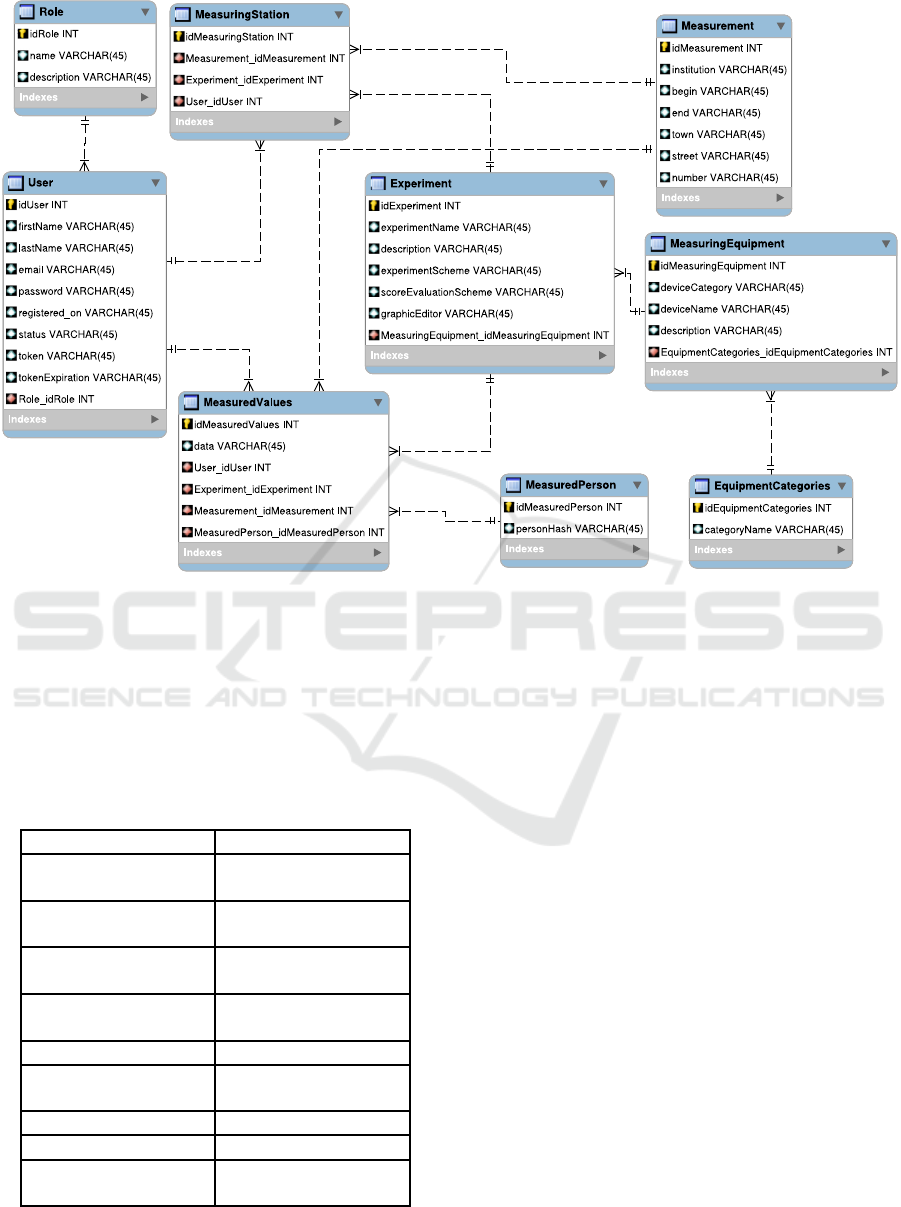
Figure 3: ERA model.
and has been continuously improved according to op-
eration difficulties.
The list of devices which were used during the
testing is shown in Table 2. The control software for
impact dance is described in (omitted for the review
process).
Table 2: Used devices.
Site Device name
Body proportions
Medisana BS 440
Connect
Electrocardiography
ReadMyHeart Hand-
held ECG
Blood pressure
Omron M6 Comfort
IT
Blood sugar
FORA Diamond
Mini
Spirometry SP10W
Hand reaction time
Device for cognitive
research
Leg reaction time
Impact Dance Pad
Flexibility Podium and ruler
Color vision
Pseudoisochromatic
tables
4 CONCLUSIONS
In this paper we presented an idea of the exercise
and wellness health strategy framework and the first
steps that were done to support this framework by an
appropriate software architecture. The proposed and
developed software prototype covering a part of the
whole infrastructure, namely rapid collection, stor-
age and visualization of heterogeneous health related
data, was successfully tested on more than three hun-
dreds participants outside laboratory conditions.
The presented software prototype enables its users
to quickly set the health related data to be collected
and the whole data collection procedure. Then the
data are collected, stored and visualized in an efficient
way. Currently the prototype enables not only col-
lection of classical data, but also non-traditional data
(such as brain data) gathering. The software proto-
type design follows proven architectural patterns and
styles, its modular structure facilitates its further ex-
tension.
In the future work we will focus on continuous ex-
tension of the software prototype to cover other parts
of the intended software infrastructure for exercise
and wellness health strategy framework. This include
e.g. the modules for food and exercises recommenda-
HEALTHINF 2017 - 10th International Conference on Health Informatics
482

tions, overall data evaluation or improved data visual-
ization.
ACKNOWLEDGMENTS
This publication was supported by the UWB grant
SGS-2016-018 Data and Software Engineering for
Advanced Applications, the project LO1506 of the
Czech Ministry of Education, Youth and Sports under
the program NPU I and the 2nd Internal grant scheme
of UWB School of Computing, 2016.
REFERENCES
Banos, O., Amin, M. B., Khan, W. A., Ali, T., Afzal, M.,
Kang, B. H., and Lee, S. (2015). Mining minds:
An innovative framework for personalized health and
wellness support. In Pervasive Computing Technolo-
gies for Healthcare (PervasiveHealth), 2015 9th Inter-
national Conference on, pages 1–8. IEEE.
Blair, S. N., Cheng, Y., and Holder, J. S. (2001). Is physical
activity or physical fitness more important in defining
health benefits? Medicine and science in sports and
exercise, 33(6; SUPP):S379–S399.
Busse, R. (2010). Tackling chronic disease in Europe:
strategies, interventions and challenges. Number 20.
WHO Regional Office Europe.
Joo, M.-I., Chung, G.-S., and Lee, T.-G. (2012). Wellness
information system for smart healthcare. Journal of
Advanced Information Technology and Convergence,
2(2):25–34.
Laakko, T., Leppanen, J., Lahteenmaki, J., and Nummi-
aho, A. (2008). Mobile health and wellness applica-
tion framework. Methods of Information in Medicine,
47(3):217–222.
Lee, I.-M. and Skerrett, P. J. (2001). Physical activity and
all-cause mortality: what is the dose-response rela-
tion? Medicine and science in sports and exercise,
33(6; SUPP):S459–S471.
Organization, W. H. et al. (2010). Global recommendations
on physical activity for health.
Shephard, R. J. (2001). Absolute versus relative intensity of
physical activity in a dose-response context. Medicine
and science in sports and exercise, 33(6 Suppl):S400–
18.
Taylor, R. S., Brown, A., Ebrahim, S., Jolliffe, J., Noorani,
H., Rees, K., Skidmore, B., Stone, J. A., Thompson,
D. R., and Oldridge, N. (2004). Exercise-based re-
habilitation for patients with coronary heart disease:
systematic review and meta-analysis of randomized
controlled trials. The American journal of medicine,
116(10):682–692.
Tunstall-Pedoe, H. (2006). Preventing chronic diseases. a
vital investment: Who global report. geneva: World
health organization, 2005. pp 200. chf 30.00. isbn
92 4 1563001. also published on http://www. who.
int/chp/chronic
disease report/en. International Jour-
nal of Epidemiology, 35(4):1107–1107.
Webber, L., Divajeva, D., Marsh, T., McPherson, K.,
Brown, M., Galea, G., and Breda, J. (2014). The
future burden of obesity-related diseases in the 53
who european-region countries and the impact of ef-
fective interventions: a modelling study. BMJ open,
4(7):e004787.
Exercise and Wellness Health Strategy Framework - Software Prototype for Rapid Collection and Storage of Heterogeneous Health Related
Data
483
