
A Design of Secure and Reliable Wireless Transmission Channel for
Implantable Medical Devices
1
Lake Bu and Mark Karpovsky
Reliable Computing Laboratory, Electrical and Computer Engineering, Boston University, Boston, U.S.A.
{bulake, markkar}@bu.edu
Keywords:
Implantable Medical Devices, Security, Eavesdropping, Hijack, Tampering, Replay, Man-in-the-middle,
Encryption, Authentication, AES, AMD, Error Control Codes.
Abstract:
Implantable medical devices (IMDs) have increasing impact in people’s life nowadays. With the development
of electrical and computer engineering, the IMDs are of great convenience to patients by their small sizes and
portable wireless monitors or controllers. However, because of the insecure wireless communication between
the devices and their controllers, it makes way for attackers to passively and actively attack the devices and
so the patients. Unlike other attacks which target on victims’ information or property, the medical attacks
threat victims’ life directly. Up to now there are few efficient solutions to those attacks which balance security,
reliability, and power consumption. In response to the situation, this paper proposes a scheme against the
existing and potential attacks to IMDs while keeping a low overhead in hardware and power consumption.
1 INTRODUCTION
Implantable medical devices (IMDs) such as insulin
pumps, pacemakers, and self-powered biosensors are
widely used to save and extend people’s life. These
devices are embedded inside patients’ bodies and
communicate through wireless transmissions with
their controllers or monitors, depending on whether
it is open-loop or closed-loop.
However, these wireless transmissions usually are
not protected due to the consideration of saving bat-
tery life, and capability of allowing the third-party de-
vices’ connection at emergency. This makes it possi-
ble for attackers to maliciously apply remote attacks
to the IMD users. Since all these attacks are applied
on the channel between the devices and the controllers
or monitors, we categorize them into Man-In-The-
Middle (MITM) attacks.
Moreover, since the medical data transmitted
through the wireless channel are highly repetitive or
in a regular pattern such as heart beats or glucose in
the blood, it is not too difficult to predict the infor-
mation even if it is encrypted, which makes the IMDs
more vulnerable to attacks.
Eavesdropping is one of the most commonly seen
passive attacks to wireless channels. The attackers
1
This work was sponsored by the NSF grant CNS
1012910.
simply listen to the unencrypted transmissions and ac-
quire the knowledge of the health of the targeted pa-
tients or victims. Since there is no malicious tamper-
ing to the transmission, it is hard to detect. There are
software and hardware means to eavesdrop the IMDs’
channel. Researches on this type of passive attacks
have been made by (Halperin et al., 2008), (Li et al.,
2011), and (Paul et al., 2011) etc.
If eavesdropping is only the stealth of the vic-
tims’ medical information, then active attacks such
as hijack or replay are more lethal to the victims’
health and even life. The attackers can use radio
transmitters to simply generate commands to the de-
vices implanted inside patients’ bodies. They can ei-
ther send their own forged commands, or replay a le-
gal command eavesdropped and stored previously, if
the transmission is encrypted. These types os attacks
have been explored by (Halperin et al., 2008) over
pacemakers and (Roberts, 2011) over insulin pumps.
Both resulted in a fatal attack in simulation.
As a matter of fact, many IMD manufacturers ac-
tually integrated the Advanced Encryption Standard
(AES) in their devices. However, they are not ac-
tivated due to the concern of increasing power con-
sumption or authentication of the third party devices
(InfoSec, 2014).
Moreover, even if the AES module is activated,
the transmission is encrypted but not properly authen-
ticated. Thus there are still potential threats it is vul-
Bu, L. and Karpovsky, M.
A Design of Secure and ReliableWireless Transmission Channel for Implantable Medical Devices.
DOI: 10.5220/0006270502330242
In Proceedings of the 3rd International Conference on Information Systems Security and Privacy (ICISSP 2017), pages 233-242
ISBN: 978-989-758-209-7
Copyright
c
2017 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
233
nerable to: replay and known-plaintext attacks.
Therefore in this paper we propose a design of se-
cure and reliable wireless transmission channel using
authenticated encryption against both passive and ac-
tive MITM attacks. The major contributions are:
• It uses encryption on transmitted messages
against eavesdropping. It also randomizes the
message to avoid known-plaintext attacks;
• It checks the authenticity of each transmis-
sion against forged messages. The attack mis-
detection probability is almost 0 in a device’s
lifespan;
• All encrypted legal messages are valid for only
once in a device’s lifespan, so that a prior legal
message cannot be stored and replayed to pass
authentication;
• It provides strong reliability to restore the
transmission from random errors;
• When the pre-installed AES module on device
is enabled, the proposed authenticating process
adds less than 5% additional power consump-
tion over it, which is much less than that of
other conventional methods.
The rest of the paper is organized as the following.
Section 2 briefly explains the several IMD transmis-
sion models. Section 3 illustrates the existing and po-
tential attack models against current IMDs. Section
4 explains the criteria of the protection against such
attacks. Section 5 introduces the proposed protection
scheme and its work flow, as well as the theoretical es-
timation of its security level. Section 6 evaluates the
proposed design by experiments and overhead com-
parison with other possible schemes.
2 IMD COMMUNICATION
MODELS
There are a number of various types of wireless IMDs.
They are characterized by different communication
protocols and power supplies. Upon different types
of IMDs, different attacks may apply.
2.1 Closed-loop IMDs
Closed-loop IMDs are self-monitored and self-
managed. They receive wireless transmission from
the sensor inside the patients’ bodies and the actu-
ator determines what therapy to deliver accordingly.
The most commonly seen closed-loop IMDs are pace-
makers and implantable cardiac defibrillators (ICDs)
(Burleson et al., 2014).
Below Skin
Closed-loop IMD
Sensor Actuator
Batt
-ery
Professional Configuration
from Clinics or Hospitals
(not necessary)
Figure 1: Closed-loop IMDs manage themselves based on
the communication between the sensor and the actuator. Al-
though they have no access for the patients to control them,
they do allow configurations from professionals. The com-
munication is not encrypted. The battery is usually not char-
gable and the replacement takes a surgery.
Since the transmissions are not encrypted, the
transmitted messages are plainly from the medical
sensors. Thus it is not too difficult to eavesdrop and
acquire the knowledge of the patient. Based on the
acquired information, the attackers will be able to re-
play some of the messages to the monitor, inducing
the device to react in a certain way. In 2008, (Halperin
et al., 2008) conducted their research on the vulnera-
bilities of pacemakers and ICDs. They successfully
listened and understood the wirelessly transmitted in-
formation of the patient. They even reused the stored
messages to disable the device, which may cause fatal
accident to the patients in real life.
Besides, the power consumption is another major
issue in these IMDs. Usually pacemakers or ICDs are
designed to last for 5 to 7 years. Once the battery runs
out of power, it takes a surgery to replace it. Hijacking
the transmission channel by eavesdropping and replay
can also result in a quick drain of battery by making
the device working in a high-power mode.
2.2 Open-loop IMDs
Open-loop IMDs such as insulin pump systems can
be more assailable. They receive wireless transmis-
sion from the devices’ sensors inside patients, who
are able to respond with remote controls. For exam-
ple, a patient can issue pumps themselves according
to reading of his/her glucose.
Since the communication involves control signals,
the attackers can take advantage of it to apply more di-
rect and harmful attacks to the victims. Furthermore,
these IMDs’ communications are not encrypted or au-
thenticated, making it even less complicated to eaves-
drop the transmission or forge malicious commands.
(Li et al., 2011) have studied the case on insulin
pump systems. They were not only able to acquire the
encrypted information from the device, but also man-
ICISSP 2017 - 3rd International Conference on Information Systems Security and Privacy
234

Below Skin
Open-loop IMD
Sensor Actuator
Batt
-ery
Patient Interface
Monitor Controller
Above Skin
Figure 2: Open-loop IMDs usually come with a monitor
and a controller. The patients monitor their health status
based on the data from the sensor. They are able to issue
commands (such as a dose of medicine or an insulin pump)
by their judgement. The communication is not encrypted.
aged to forge false glucose readings to the monitor.
Finally, they successfully sent their own commands
to the pump due to its lack of authentication process.
Moreover, other researchers such as (Radcliffe,
2011) and (Takahashi, 2011) claimed that they have
gained full control to some of the insulin pump sys-
tems because these devices accept unauthorized radio
signals or commands.
2.3 Biosensors
Biosensors are different from the two types above in
several ways. Firstly they are usually self-powered
inside human bodies. Secondly they are purely trans-
mitters and receive no commands. Biosensors are
widely used to detect glucose, lactate, or cholesterol
etc. The receiver (patches) serves as the middle sta-
tion which powers the sensor while sending the data
to a higher level of monitors or analysts. However,
both the monitor and the patch give no feedbacks in
the form of commands.
Below Skin
Sensor
Patch
Above Skin
Monitor or Analyst
Figure 3: Biosensors send measurement to the patch and
are powered by it. The patch then sends the measurement
to monitors for analysis.
The major threat to biosensors will be eavesdrop-
ping although it is not easy to implement because of
their short communication distance. Other precise
and practical threat models are yet to be developed
(Burleson et al., 2014).
3 EXISTING AND POTENTIAL
ATTACKS TO IMDS
As mentioned in the previous section, for IMDs with
wireless communication, eavesdropping and channel
hijack are two most frequently reported attacks. Also
many IMDs are equipped with AES but have not
enabled the encryption process. Even if they have,
this can only prevent the attackers from eavesdrop-
ping and understanding the patients’ health informa-
tion. Those devices may still be vulnerable in cer-
tain ways under active Man-In-The-Middle (MITM)
attacks such as hijack and replay.
According to the existing reported IMD attacks,
they usually have the following preconditions:
1. The attacker is able to eavesdrop the victim’s
wireless IMD transmission between the sensor
and the monitor/controller (Rostami et al., 2013);
2. Given the device’ serial number, the attacker is
able to use a programmed radio to send forged
or stored commands to the victim’s actuator
(Rushanan et al., 2014);
3. The medical signals such as heart beats or glucose
in the blood are in a regular pattern. Meaning they
are possible to predict (Yury, 2014).
Given the assumptions above, the following sub-
sections will describe the existing and potential at-
tacks to ordinary IMDs and AES protected IMDs.
3.1 IMDs with AES Disabled
As mentioned in Section 2, most IMDs have their
AES disabled, leaving the transmission channel en-
tirely unprotected. Once the attackers eavesdrop and
analyze the transmitted messages, they are capable to
apply various attacks such as replay or spoofing com-
mands. The results can be leakage of patients’ health
information, increase of battery power consumption,
overdose of the medicine, and malfunction or termi-
nation of the implanted devices etc.
3.2 IMDs with AES Enabled
Even if the IMDs activate their AES module to have
each transmitted message encrypted (InfoSec, 2014),
there still can be many potential ways to attack.
3.2.1 Eavesdropping and Known-plaintext
Attacks
Eavesdropping is a type of passive attacks that the
attacker listens to the unencrypted wireless transmis-
sion silently. The attacker does not necessarily apply
A Design of Secure and ReliableWireless Transmission Channel for Implantable Medical Devices
235
any malicious modifications to the transmitted mes-
sages. Usually the goal of eavesdropping is to acquire
the victim’s important health information.
The Advanced Encryption Standard (AES) (Dae-
men and Rijmen, 2013) is a well-known solution that
prevents the attackers from understanding the mes-
sage transmitted even if they record it. However, if the
encrypted cipher can be listened, and the attackers are
able to predict or make a proper guess of the victim’s
health data (precondition 3.), with both the cipher and
plaintext it is possible to apply known-plaintext at-
tacks. This can lead to severe information leakage
such as the secret keys (Bogdanov and Isobe, 2014).
This will be disastrous since the attacker then will be
capable to decrypt and understand any ciphers of the
health data. Moreover, the attacker will have the suf-
ficient knowledge to forge the measurement of health
data to spoof the sensor.
3.2.2 Hijack and Replay
As (Rushanan et al., 2014) have pointed out, some
IMDs have no authentication of the incoming radio
signals. Thus the attackers and establish anonymous
transmissions to either the implanted device or the
monitor/controller.
This gives attackers opportunities to take over the
transmissions between legal sensors and controllers.
The attacker can firstly eavesdrop and record the le-
gal transmitted ciphers without any understanding of
the health data. Then he/she can replay some of the
stored legal ciphers to IMD. Even if every transmitted
message is encrypted and authenticated, the replayed
ciphers will still be considered as legal. Moreover,
if the attacker is able to apply known-plaintext attack
and acquires the information of the secret key, he/she
can choose to inject certain ciphers to harmfully affect
the IMD. For example, very high glucose measure-
ments can be frequently sent to the patient’s monitor,
inducing overdose of insulin pumps. Or commands
of persistent large electric shocks can be sent to the
defibrillator or pacemaker, causing deadly aftermath.
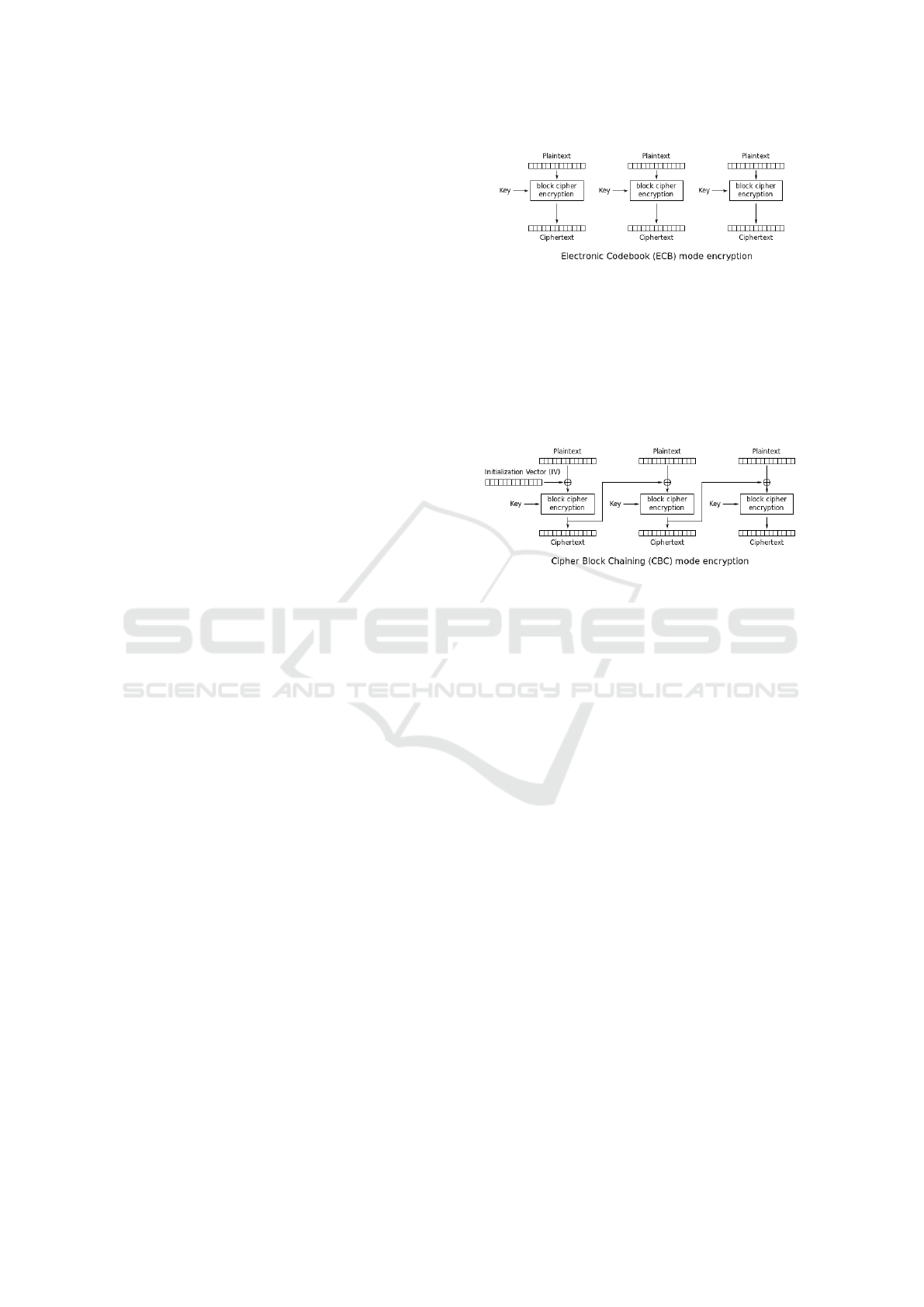
Depending on which AES mode a IMD is quipped
with, the replay attacks will have different effects.
If it is AES in ECB mode, then there is a one-
on-one pairing between the plaintext (health data) and
cipher as shown in the figure below. This makes it ex-
tremely easy for attackers to choose ciphers to inject
into the hijacked channel according to their malicious
purposes.
If it is AES in CBC mode, which is considered
as much more secure than the ECB mode, the cur-
rent plaintext will be randomized by the previous ci-
pher and then sent for encryption. Thus the decrypted
texts are beyond the control of the attackers. How-
Figure 4: In ECB mode the cipher is a function of the secret
key and the plaintext, whose mapping is unique and predi-
catble.
ever, since the health data are usually generated from
microprocessors and sensors of 8 bits, 12 bits, or 16
bits (Chede and Kula, 2008) (McDonald et al., 2011),
it makes the replayed cipher from attackers decrypted
to another legal numeric value with a high probability.
Figure 5: In CBC mode the cipher is effectively randomized
by a function of the secret key, the current plaintext, and the
previous cipher.
Example 3.1: In a 128-bit AES-CBC protected in-
sulin pump IMD system with a 128-bit IV (in hex-
adecimal):
IV = {0x00, 0x01, 0x02, 0x03, 0x04, 0x05, 0x06,
0x07, 0x08, 0x09, 0x0a, 0x0b, 0x0c, 0x0d, 0x0e, 0x0 f }
And a 128-bit secret key (in hexadecimal):
key = {0x60, 0x3d, 0xeb, 0x10, 0x15, 0x ca, 0x71,
0xbe, 0x2b, 0x73, 0xae, 0x f 0, 0x85, 0x7d, 0x77, 0x81}
This insulin pump generates 16-bit measurement
data of glucose in the blood. From a previous eaves-
dropping, the attacker has acquired the legal cipher of
a sensor’s measurement of glucose at moment t
0
as:
cipher(t
0
) =
{0x17, 0x71, 0x98, 0x42, 0xac, 0x9c, 0x9e, 0xe8,
0x87, 0xc6, 0xed, 0x71, 0xd1, 0x1a, 0x78, 0x24}
After a meal at the moment t
1
the patient’s IMD
microprocessor transmits the cipher text for ‘200
mg/dL” high level glucose in the blood to his mon-
itor:
cipher(t
1
) =
{0x0e, 0x11, 0x43, 0x4e, 0x23, 0xb1, 0x32, 0x f 2,
0x4c, 0x12, 0x0a, 0x6d, 0x2c, 0x03, 0x87, 0x1e}
ICISSP 2017 - 3rd International Conference on Information Systems Security and Privacy
236
Then the attacker uses his own programmed radio
to send the pre-stored cipher
0
soon after, although he
has no knowledge of the plaintext that this cipher re-
lates to. According to the CBC mechanism, by the
secret key and the previous cipher(t
1
) the decryption
gets the following plaintext at moment t
2
:
plaintext(t
2
) =
{0x00, 0x8c, 0xe2, 0x41, 0x f 2, 0x5 f , 0x42, 0x07,
0x28, 0x59, 0x2a, 0x44, 0x52, 0xe2, 0x43, 0x5c}
where the measurement bits are {0x00, 0x8c} which
happens to be “140” at the normal range, resulting in
a skip of medication. Similar technique also works
for closed-loop devices such as defibrillators.
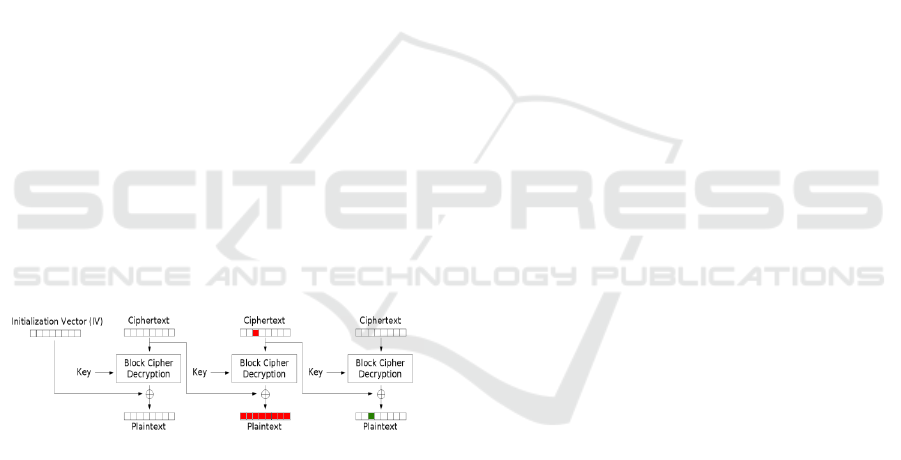
3.2.3 Bit-flipping Attacks
Another type of attack taking advantage of the CBC
mode is bit(byte)-flipping. By maliciously flipping
some of the bits in the previous cipher, the next de-
crypted plain text will be altered in exactly the same
bits.
Even if there is no leakage of the secret key, ac-
cording the the precondition 3, as long as the attacker
can listen to the channel and has a proper guess of
the incoming message, the attack is highly probable
to succeed.
According to the AES-CBC decryption procedure,
a bit-flipping attack can be applied as the following
chart (Swepsie, 2014).
Figure 6: If a previous cipher is flipped by XOR operations
to some bits, the next plain text will be flipped accordingly
by XOR operations in the same bits.
For wireless IMD communications, even if the at-
tacker is not able to modify the legal cipher in the
channel, if he/she can predict the coming message (a
command or a health data measurement), a carefully
selected forged cipher can be injected before the next
legal cipher. Then the plaintext decrypted from the
next legal cipher will be affected by the previously in-
jected forged cipher in certain bits by XOR operation.
Example 3.2: In a 128-bit AES-CBC protected in-
sulin pump IMD system, the 128-bit IV and secret key
are the same as Example 3.1. The system encodes and
decodes 16-bit commands including issuing an injec-
tion {0x00, 0x80}, turning on the device{0x80, 0x00},
and turning off the device {0x08, 0x00} etc.
After the patient finishes his meal and the glu-
cose reading is at a high level, and the patient will be
ready to issue a command of insulin injection which
is {0x00, 0x80}. And if the attacker can predict this
event, he can simply inject a forged command cipher
at moment t
0
as:
cipher(t
0
) =
{0x08, 0x80, 0x35, 0x f 6, 0x88, 0x28, 0x6e, 0xc1,
0x3a, 0xd0, 0x87, 0x60, 0x10, 0x90, 0xd5, 0xe0}
This forged command itself does not fall into any
legal command. However, as the patient sends a fol-
lowing command of insulin injection, after decryp-
tion in the CBC mode at moment t
1
the command be-
comes:
plaintext(t
1
) = {0x00 → 0x 08, 0x80 → 0x00,
0x60, 0x3d, 0xeb, 0x10, 0x15, 0xca, 0x71,
0xbe, 0x2b, 0x73, 0xae, 0x f 0, 0x85, 0x7d}
And this is the command to turn off the device
instead of insulin injection.
As for closed-loop devices such as defibrillators,
this type of attack is not that straightforward but still
possible. Since those IMDs only accepts professional
configuration from a clinic or a hospital, it demands
the attackers to have access to those locations. How-
ever once the attackers can be physically close to the
configuration, this bit-flipping attack can still work in
a similar way. This causes even grave danger to turn
a defibrillator off.
4 SYSTEM DESIGN CRITERIA
The goals of the proposed security system are to pro-
tect the IMD wireless channels from all the MITM at-
tacks mentioned above while keeping low power con-
sumption overhead. In addition, the design should
modify the current secure scheme (AES-CBC) on
IMDs as less as possible, so that it can be smoothly
adopted by the current IMD manufacturers.
4.1 Data Block Size
We assume that the current IMDs equipped with AES
will enable the encryption module in either 128 or
192-bit mode, where the 128-bit mode is the most
common used and the 256-bit mode is an overkill to
both security and power consumption and thus much
less applied. Each health data or command packet is
encrypted into a 128 or 192-bit data block. We aim
not to increase the number of blocks or the size of
blocks needed for each packet.
A Design of Secure and ReliableWireless Transmission Channel for Implantable Medical Devices
237

4.2 Against Eavesdropping and
Known-plaintext Attacks
The current AES-CBC scheme is sufficient against
eavesdropping. It takes hundreds of years to de-
crypt(understand) the patient’s encrypted health data
or command by brute force without the security key.
However it is not sufficient against known-
plaintext attacks in the case of IMDs. As stated
in preconditions 1, it is possible for an attacker to
eavesdrop and store a number of legal ciphers. Pre-
condition 3 suggests that an attacker is also able to
make a proper guess of the encrypted health data
or commands (plaintexts), since they are usually in
highly regular patterns. For example, the glucose
level is usually between 70 to 200 mg/dL, and car-
diac rhythms are known to be the biological signa-
tures of each person. The packet formats of the com-
mands of controllers are even easier to find from their
technical specifications. Then the attackers can pair
up the ciphers and plaintexts to implement known-
plaintext attacks. Since the plaintexts are predictable,
they should be properly randomized. However, even
if they are in the CBC mode (by XORing the current
health data or command bits with and the previous ci-
pher), the attackers still can analyze them since the
ciphers have already been eavesdropped.
Therefore a more sophisticated randomization
should be involved so that even with a record of ci-
phers and plaintexts, the attack is still not able to pair
them up for known-plaintext attack.
4.3 Against Hijack, Replay, and
Bit-flipping Attacks
Firstly the transmission should be authenticated, so
that unauthorized or replayed radio signals should not
be accepted as a legal sensor reading or commands.
AES itself does not provide this feature and extra
modules for authentication is required.
There are various ways for authentication. Keyed-
hash Message Authentication Code (HMAC) pro-
vides strong security but requires a huge amount of
extra bits for the digest, which contradicts with the
first design criterion by bringing considerable modifi-
cation (each data packet uses more than one blocks)
to the current AES-CBC scheme. Here we propose
to use the Algebraic Manipulation Detection (AMD)
codes which is a light weight keyless message authen-
tication code (Wang and Karpovsky, 2011b). Unlike
HMAC which has a fixed length over 160 bits, it is
very flexible to work on different sizes of data pack-
ets by which its security level is determined. More-
over, the AMD codes bring in a random vector so that
the plaintext is randomized even if the health data or
commands are non-uniformly distributed, which effi-
ciently prevents the known-plaintext attacks.
Secondly, each authenticated cipher should be
valid only once in a lifetime. It indicates that even
if the attacker stores all the authenticated and en-
crypted transmissions, he/she will not be able to reuse
any of them in future. Thus it is necessary to use a
self-incrementing timestamp in each transmission as
part of the authentication process. The system always
keeps track of the latest timestamp. If an incoming
message has a timestamp smaller or equal to the high-
est one known by the system, it is illegitimate.
The medical devices usually use low frequency
sensors with sampling rates from 1Hz to 1kHz. And
an IMD can last from 1 to 10 years. The security
module should guarantee that within these years un-
der the health data sampling rate, not a single replay
or bit-flipping attack can succeed. Therefore based on
these parameters, the attack mis-detection probability
should be at least 2
−32
for IMDs working under low
frequency of up to 10Hz and at least 2
−40
for higher
frequency of up to 1kHz.
4.4 Against Random Errors
Random errors are not attacks. They are usually
caused by unstable transmissions or minor change of
voltages etc. Upon the presence of random errors the
readings of health data might be imprecise or the com-
mands might be distorted. The reliability against ran-
dom errors can be enhanced by applying error con-
trol codes (ECC) to the plaintexts (Burleson et al.,
2014). In this design we will use double error correc-
tion codes which is more than enough for the channel.
4.5 Power Consumption
Since wireless IMDs are mostly battery powered (ex-
cept the self-powered biosensors), the design should
also aim for low power consumption overhead com-
paring with other possible methods.
5 SYSTEM DIAGRAM AND
WORKFLOW
The proposed protection scheme uses authenticated
encryption with timestamps. Its encoding procedure
is MAC-then-Encrypt (MtE). In this way the IMD’s
information part (health data from sensors or com-
mands from controllers), the timestamp, and the au-
thentication signature can be wrapped all under 128
ICISSP 2017 - 3rd International Conference on Information Systems Security and Privacy
238

bits or 192 bits depending on the demand. As a re-
sult, it adds no extra transmission overhead to the
current IMDs equipped with 128 or 192-bit AES in
CBC mode. Although MtE is not considered as the
most generically secure in all authenticated encryp-
tion modes, it has been proved to be secure with the
AES-CBC mode (Krawczyk, 2001).
5.1 Notations
To help describe and evaluate this protection mecha-
nism, we introduce the following notations.
5.1.1 Finite Field Operators
We denote the Galois finite field by GF, and the num-
bers of bits in each data packet by b. Then · is the
multiplication in the GF(2
b
) finite field, ⊕ the addi-
tion in GF(2
b
), namely bitwise XORs, and
L
as the
accumulated sum operator. || represents concatena-
tion of two vectors.
5.1.2 Elements in Data Packets
The information part carrying the health data from
sensors or commands from controllers is denoted by
k, and r is the ECC redundancy to protect k from ran-
dom errors. y = k||r is the concatenation of both. The
self-increment timestamp is denoted by i, the random
vector by x, and the AMD code’s signature by ω.
5.1.3 Attacks
e represents the injected error by attackers to each
data packet and so e = {e
ω
, e
y
, e
i
, e
x
}. Any packet
tampered by e is marked by ˜ . The attack mis-
detection probability is denoted by P
miss
.
5.1.4 Random Error Correction
The ECC’s check matrix H is used with ˜y to compute
the syndrome S for random error correction.
5.2 AMD Codes
The AMD codes have been known as a class of
low weight but highly secure attack detecting codes
against strong attacks, where the attackers have
proper knowledge of the information part, the encod-
ing scheme, and are able to issue any modifications to
the message in channel. It often cooperates with cryp-
tographic systems as a keyless authentication code
(Wang and Karpovsky, 2011a). Because of its ran-
dom vector x, AMD codes performs excellently with
uniform security even under non-uniform distribution
of the information part, which covers the vulnerability
of the highly repetitive health data or commands.
Construction 5.1: Let the random variable
x = {x
1
, x
2
, ··· , x
t
}, and the information part y =
{y
1
, y
2
, ··· , y
t
}, then the AMD codes are constructed
by (Luo et al., 2013):
ω =
t
M
j=1
(x
j
· y
j
⊕ x
3
j
); ω, x
j
, y
j
∈ GF(2
b
). (1)
If the error e
y
on y is non-zero (for an attack to
make sense), then the term x
3
j
can be omitted. For
the proposed protection scheme, t = 1 since y = k||r
is in one packet. y can be robustly combined with the
self-incrementing timestamp i by y·i (K.J.Kulikowski
et al., 2005), where · is the finite field multiplication.
The signature ω of the AMD code is computed by:
ω = y ·i · x = (k||r) · i · x; i, x, y ∈ GF(2
b
). (2)
If the injected errors to each component is repre-
sented as e
ω
, e
y
, e
i
and e
x
, the error masking equation
will be:
ω ⊕ e
ω
= [(k||r) ⊕ e
y
] · (i ⊕ e
i
) · (x ⊕ e
x
). (3)
It has been verified that the right-hand side of the
equation is always a non-zero polynomial of x of de-
gree 1. It is easy to prove that for a certain message
and an error e, the error missing probability is at most:
P
miss
= 2
−b
. (4)
b should be at least 32 or 40 to ensure that no at-
tack will succeed in an IMD’s lifetime.
5.3 Error Correction Codes for
Random Errors
Usually there is little error correcting code’s (ECC)
redundancy added to information part of the IMD sen-
sors or controllers to restore the message from ran-
dom errors. Since the proposed scheme should be en-
coded into at least 32-bit packets and the information
part is at most 16 bits, the rest of the bits can be allo-
cated for the ECC’s redundancy.
To ensure fast decoding and low hardware com-
plexity, we propose to use the Orthogonal Latin
Square Codes (OLSCs) (Yalcin et al., 2014). The er-
ror correction procedure is:
H · (
˜
k||˜r) = S (5)
where
˜
k ∈ GF(2
16
) or less and ˜r ∈ GF(2
16
) are dis-
torted information part and redundancy, H is a 16×32
binary matrix, and S is a 16-bit binary vector which is
used for one-step majority voting error correction (Bu
and Karpovsky, 2016) of up to 2 random errors in k.
A Design of Secure and ReliableWireless Transmission Channel for Implantable Medical Devices
239
5.4 System Diagram
As stated prior this section, the proposed scheme is
structured by authenticated encryption with MAC-
then-Encrypt work flow. The AES-CBC encryption
process will protect the system from eavesdropping
on k the health data or commands. The ECC’s redun-
dancy r enables correction of up to 2 random errors
in k. The timestamp i will guarantee that each trans-
mitted cipher can never be replayed again to spoof a
legal command or health data. The random vector x
randomizes the plaintext ((k||r)||i||x||ω) so that the
attackers cannot apply known-plaintext attacks even
if they have a proper guess of the patient’s medical
data as stated in the precondition 3 (Kulikowski et al.,
2008). The AMD authenticating finally signature ω
verifies if the message is authentic or not.
For IMDs working under lower sampling fre-
quency of up to 10Hz, the block size is 128 bits and
each data packet 32 bits. For IMDs working under
frequency up to 1kHz, the block size should be 192
bits and data packet at least 40 bits. However since
each block includes 4 packets, each packet can be
made to 48 bits to fully utilize the space while en-
hancing the security lever.
IMD Info: k
ECC Redun-
dancy: r
Timestamp
Counter: i
Random Vector:
x
AMD
Signature: w
AES Encryption
Secret Key
IMD Info: k
ECC Redun-
dancy: r
Check if
i
t+1
> i
t
?
Random Vector:
x
AMD
Redundancy: w
AES Decryption
Wireless Channel
Secret Key
ECC Decoder
AMD Decoder
MITM Attacks
Attack?
32 bits
32 bits
32 bits
32 bits 32 bits
32 bits 32 bits 32 bits
128 bits
128 bits
128 bits
128 bits
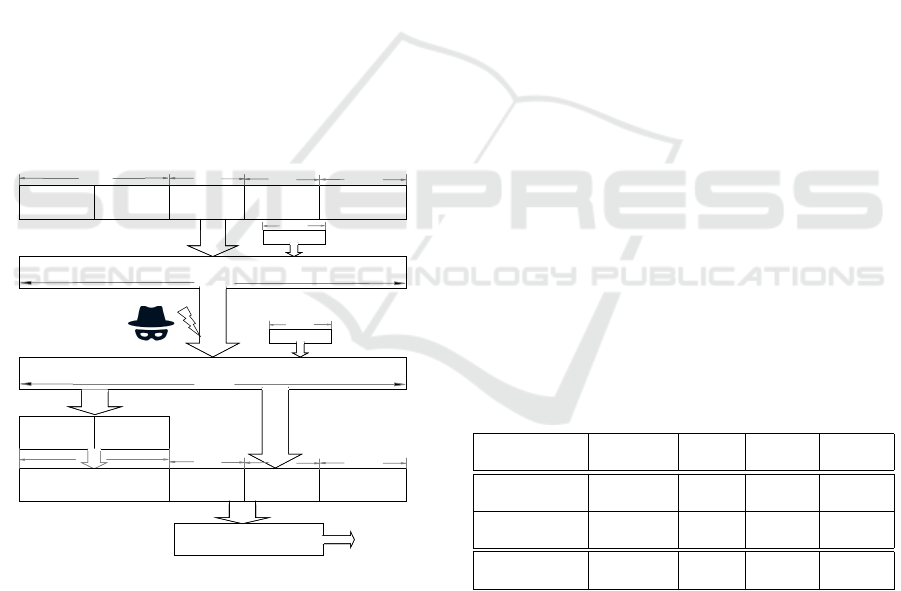
Figure 7: The lower frequency secure system’s diagram.
The higher frequency system has the same workflow except
the block size is 192 bits and packet size 128 bits.
The diagram of the lower frequency system is
shown in Figure 7. The system firstly encodes the
16-bit health data from the sensors or commands from
the controller k into the 32-bit information part y, with
a double-error correcting OLSC code’s redundancy
r. Secondly they are encoded with the timestamp i
and random vector x into ω by the message authen-
tication code AMD. Then the 128-bit ((k||r)||i||x||ω)
will serve as the randomized plaintext to be encrypted
by the 128-bit AES under CBC mode. The Man-In-
The-Middle attacks occur in the wireless transmis-
sion channel by eavesdropping, hijack, replay, and
bit-flipping. On the receiver end, the AES firstly de-
crypts the plaintext and the first 32 bits are sent to
the OLSC decoder for random error correction. Then
it checks if the timestamp i is larger than the previ-
ous one. Finally the entire plaintext is verified by the
AMD decoder for attack detection.
6 EVALUATIONS
In this section the proposed scheme’s security and
power consumption overhead will be evaluated.
6.1 Error Mis-detection Probabilities
To verify this probability we have run through tests
on over 3 billions simulated IMD radio transmissions
of sensor’s health data and controller’s commands,
which is about the total number of an ordinary IMD’s
transmissions in 10 years under a lower frequency
of 10Hz. During the simulation the system mimics
an IMD sending and receiving messages, and the at-
tacker applying hijack, replay, and bit-flipping attacks
alternatively in every around, while the receiver veri-
fying the timestamps and the AMD signatures.
Since the 32-bit and 48-bit system provides so
strong security that not a single attack was missed
in our experiment, we apply various sizes of data
blocks (from 8 to 48 bits) due to AMD codes’ flex-
ibility to observe how much the experimental error
mis-detection probability matches P
miss
= 2
−b
in (4).
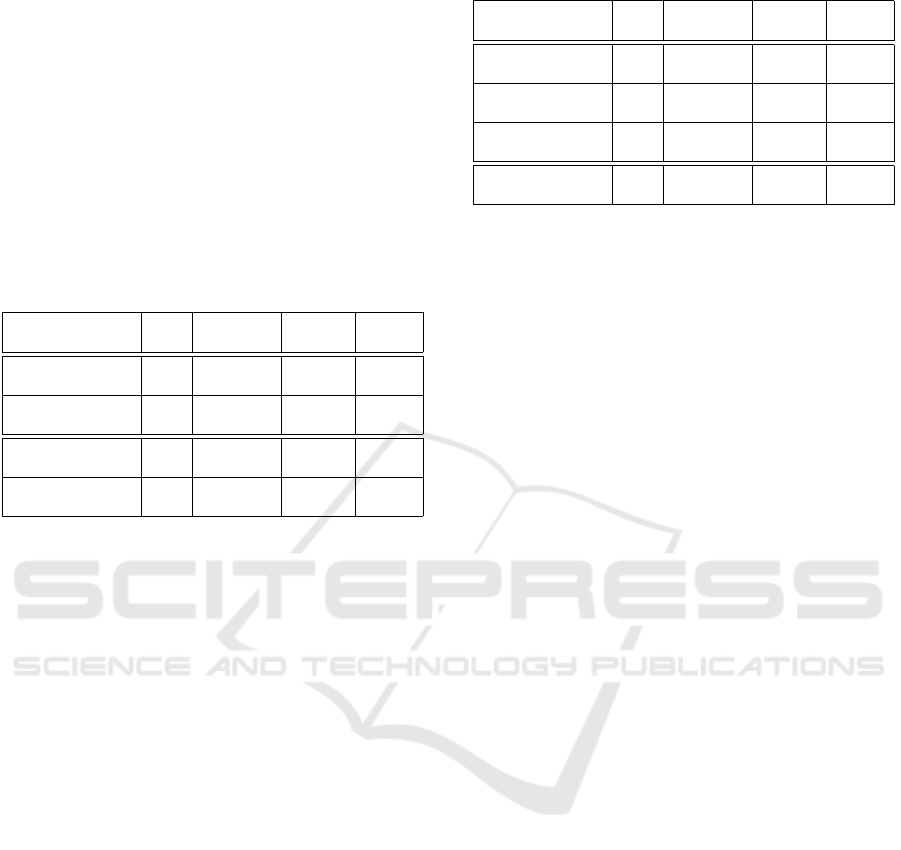
Table 1: P
miss
under 3,154,043,200 Active MITM Attacks.
P
P
P
P
P
P
P
Missing
b
8 16 32 48
Missed Errors
12,321,649 48,032 0 0
in Experiments
Experimental
3.91e-3 1.52e-5 0 0
P
miss
Theoretical
3.91e-3 1.53e-5 2.33e-10 3.55e-15
P
miss
= 2
−b
I
Under 3 billions MITM attacks modeled in Section 3, not a single error
was mis-detected by the 32-bit and 48-bit packet-sized systems.
The experimental result not only shows that the
proposed protection scheme works well according to
the theoretical estimation of 2
−b
error mis-detection
probability precisely, but also demonstrates that the
32-bit and 48-bit schemes are secure enough for miss-
ing 0 attack under 3 billions of malicious hijack, re-
play, and bit-flipping attacks, providing sufficient se-
curity during the IMD’s lifespan.
ICISSP 2017 - 3rd International Conference on Information Systems Security and Privacy
240
6.2 Power Consumption Overhead
As mentioned above, AMD codes are light weight
message authentication codes. With the AES en-
abled in the IMDs, the AMD encoding and authen-
tication add minimum power consumption overhead
while providing the security demanded. This is criti-
cal to the power sensitive IMDs such as defibrillators
whose battery replacement takes a surgery.
The following overhead comparison was made
based on the implementation on Xilinx Vertex 4
FPGA and Cadence SOC Encounter.
Table 2: Power Overhead Comparison Based on AES en-
abled.
P
miss
Extra Bits Area Energy
Over AES (um
2
) (nJ)
Proposed Scheme
2
−32
0 3093.6 2.10
(32-bit packets)
AES
N/A N/A 57520.3 67.03
(128 bits)
Proposed Scheme
2
−48
0 4765.9 4.05
(48-bit packets)
AES
N/A N/A 66732.7 91.36
(192 bits)
I
The proposed authentication module adds only 3.1% energy to the
128-bit AES encryption module, and 4.4% to the 192-bit AES
module, resulting in an ignorable energy consumption overhead
while providing sufficient security.
On another hand, one alternative approach is
AES + HMAC + timestamps. However the popular
HMAC requires at least 160 bits to provide 2
−80
mis-
detection probability which is an overkill to the secu-
rity required and brings too much modification to the
existing AES based systems.
As for the 32-bit and 48-bit AMD code and times-
tamp based scheme, since all computations are done
in the 32-bit or 48-bit finite field, it saves largely
the transmission overhead, hardware area, and power
consumption over the HMAC authentication method.
Even if the scheme upgrades x and ω to 80 bits to
achieve the same P
miss
as the HMAC based scheme, it
still saves tremendously the power consumption.
7 CONCLUSION
This design is proposed under the motivation of the
existing and potential Man-In-The-Middle attacks to
the IMDs with wireless communication. We have
proved by theory and experiments that by authenti-
cated encryption with a random vector and a times-
tamp encoded by AMD codes, it mis-detected 0 errors
in a device’s lifespan. Moreover, the proposed au-
thentication module’s energy consumption is merely
Table 3: Transmission and Power Overhead Comparison.
P
miss
Extra Bits Area Energy
Over AES (um
2
) (nJ)
Proposed Scheme
2
−32
0 3093.6 2.10
(32-bit packets)
Proposed Scheme
2
−48
0 4765.9 4.05
(48-bit packets)
Proposed Scheme
2
−80
128 6274.8 7.49
(80-bit packets)
HMAC Based
2
−80
128 58813.7 58.06
(160 bits)
I
Even when the authentication process is brought up to error mis-
detection probability of 2
−80
which is the same as HMAC, the
energy cost is only 12.9% of the later, making the proposed
lightweight scheme an economic choice for the IMDs.
3 ∼ 4% of the pre-installed AES module’s. Also
comparing with other authentication techniques such
as HMAC, it consumes only 13% energy of the later
while providing the same security level. These advan-
tages make the proposed scheme a secure and reliable
solution to the IMDs against MITM attacks, while ex-
tending the lifespan of IMDs by saving their batteries.
The power analysis of this paper is based on
the AES module that has already been integrated in
IMDs. However AES is not the best choice in an en-
ergy efficient design. Since the AMD message au-
thentication code is lightweight itself, it is recom-
mended to also use a lightweight encryption scheme
to have a better saving of the battery life in IMDs.
REFERENCES
Bogdanov, A. and Isobe, T. (2014). How secure is aes under
leakage. International Conference on the Theory and
Application of Cryptology and Information Security.
Bu, L. and Karpovsky, M. G. (2016). A hybrid self-
diagnosis mechanism with defective nodes locat-
ing and attack detection for parallel computing sys-
tems. IEEE International On-Line Testing Symposium
(IOLTS).
Burleson, W., Clark, S. S., Ransford, B., and Fu, K. (2014).
Design challenges for secure implantable medical de-
vices. Springer New York.
Chede, S. and Kula, K. (2008). Design overview of proces-
sor based implantable pacemaker. Journal of Comput-
ers.
Daemen, J. and Rijmen, V. (2013). The design of rijndael:
Aes-the advanced encryption standard. Springer Sci-
ence and Business Media.
Halperin, D., Heydt-Benjamin, T. S., Ransford, B., Clark,
S. S., Defend, B., Morgan, W., Fu, K., Kohno, T., and
Maisel, W. H. (2008). Pacemakers and implantable
cardiac defibrillators: Software radio attacks and zero-
power defenses. Proceedings of the 29th IEEE Sym-
posium on Security and Privacy.
A Design of Secure and ReliableWireless Transmission Channel for Implantable Medical Devices
241

InfoSec (2014). Hacking implantable medical de-
vices. http://resources.infosecinstitute.com/hcking-
implantable-medical-devices/. [Online].
K.J.Kulikowski, G.Karpovsky, M., and A.Taubin (2005).
Robust codes for fault resistant cryptographic hard-
ware. Proc of Int. Workshop on Fault Detection and
Tolerance in Cryptography.
Krawczyk, H. (2001). The order of encryption and authenti-
cation for protecting communications (or: How secure
is ssl?). Springer Berlin Heidelberg.
Kulikowski, K., Wang, Z., and Karpovsky, M. G. (2008).
Comparative analysis of robust fault attack resistant
architectures for public and private cryptosystems.
IEEE 5th Workshop on Fault Diagnosis and Tolerance
in Cryptography.
Li, C., Raghunathan, A., and Jha., N. K. (2011). Hijack-
ing an insulin pump: Security attacks and defenses
for a diabetes therapy system. Proceedings of the 13th
IEEE International Conference on e-Health Network-
ing, Applications, and Services.
Luo, P., Z.Wang, and M.G.Karpovsky (2013). Secure nand
flash memories resilient to strong fault-injection at-
tacks using algebraic manipulation detection codes.
Proc. Int. Conference on Security and Management,
SAM.
McDonald, J., Dean, S., Niewolny, D., Garcia, D., Chhabra,
N., and Chang, L. (2011). Integrated Circuits for Im-
plantable Medical Devices.
Paul, N., Kohno, T., and Klonoff., D. C. (2011). A review of
the security of insulin pump infusion systems. Journal
of Diabetes Science and Technology.
Radcliffe, J. (2011). Hacking medical devices for fun and
insulin: Breaking the human scada system. Black Hat
Conference.
Roberts, P. (2011). Blind attack on wireless insulin pumps
could deliver lethal dose. https://threatpost.com/blind-
attack-wireless-insulin-pumps-could-deliver-lethal-
dose-102711/75808/. [Online].
Rostami, M., Burleson, W., Koushanfar, F., and Juels, A.
(2013). Balancing security and utility in medical de-
vices? Proceedings of the 50th Annual Design Au-
tomation Conference.
Rushanan, M., Rubin, A. D., Kune, D. F., and Swanson,
C. M. (2014). Sok: Security and privacy in im-
plantable medical devices and body area networks.
2014 IEEE Symposium on Security and Privacy.
Swepsie (2014). Bypassing encrypted session
tokens using cbc bit flipping technique.
http://swepssecurity.blogspot.com/2014/05/bypassing-
encrypted-session-tokens.html/. [Online].
Takahashi, D. (2011). Excuse me
while i turn off your insulin pump.
http://venturebeat.com/2011/08/04/excuse-me-
while-i-turn-off-your-insulin-pump. [Online].
Wang, Z. and Karpovsky, M. G. (2011a). Algebraic ma-
nipulation detection codes and their applications for
design of secure cryptographic devices. IEEE 17th
International On-Line Testing Symposium (IOLTS).
Wang, Z. and Karpovsky, M. G. (2011b). Manipulation de-
tection codes and their application for design of secure
cryptographic devices. Proc of International Sympo-
sium on On-Line Testing (IOLTS).
Yalcin, G., Islek, E., Tozlu, O., Reviriego, P., Cristal, A.,
Unsal, O. S., and Ergin, O. (2014). Exploiting a fast
and simple ecc for scaling supply voltage in level-1
caches. IEEE International On-Line Testing Sympo-
sium (IOLTS).
Yury, C. (2014). Your heartbeat
may soon be your only password.
http://wired.com/insights/2014/06/heartbeat-may-
soon-password/. [Online].
ICISSP 2017 - 3rd International Conference on Information Systems Security and Privacy
242
