
WorkUp: A Mobile Application to Support Health Guidelines
Vinicius dos Santos
1
, Henrique Yoshikazu Shishido
1
, Francisco Pereira Junior
1
and Gabrielle Jacklin Eler
2
1
Departament of Computing, Federal Technological University of Paran
´
a, 1640 Alberto Carazzai Avenue,
86300000, Corn
´
elio Proc
´
opio, Paran
´
a, Brazil
2
Collegiate of Nursing, Federal Institute of Paran
´
a, 600 Jo
˜
ao XXIII, 86060370, Londrina, Paran
´
a, Brazil
Keywords:
Health Status, Indicators, Public Health, Monitoring.
Abstract:
Objective: This paper presents a model of mobile application to assess patients and prescribe physical exer-
cises offering interaction among health professionals and patients. Methods: The project is based on mobile
platform and implemented using client-server architecture and cloud computing for data synchronization in
different devices. Results: Health professionals and patients tested our application and answered question-
naire. The results indicate that the functionality and usability are satisfactory adhesion to our app design.
Conclusion: Our approach may be a candidate model to government agencies to support in prevention of
obesity and improve the health indicators of the patient to a healthier life.
1 INTRODUCTION
Communicable and non-communicable diseases are
increasing in south of Brazil, becoming the main
cause of death along with obesity risk factors (Capil-
heira et al., 2008). Prevention and early diagnosis of
obesity are important for health promotion and the re-
duction of morbidity and mortality. Obesity has a di-
rect impact in the individual’s social acceptance due
to the aesthetic concept widespread in contemporary
society (Schmidt et al., 2011). A study conducted
by the Brazilian Institute of Geography and Statis-
tics showed overweight in 50.1% of men and 48%
of women (da Sa
´
ude, 2014). Actually, there is evi-
dence that the percentage of overweight in the global
population has reached approximately 60% (Popkin,
2011).
Mobile health (mHealth) is the use of mobile com-
puting and communication technologies in health care
and public health (Free et al., 2010). Mobile applica-
tions are an option to support government agencies
in order to monitor population health indicators, and
manage the physical activities both of children and
adults. In Brazil, government programs developed by
the Ministry of Health, such as Food and Nutrition
Surveillance, Family Health Strategy, and the School
Health Program are part of the National Policy for
Health Promotion. These programs have the physi-
cal activity as one of their priorities. Individuals diag-
nosed with chronic diseases and abnormal anthropo-
metric data, should be referred to the Health Unit for
treatment and monitoring (da Sa
´
ude, 2014).
Numerous systems have been developed in health-
care using mobile technologies. The applications
enable collect data, usually by a questionnaire to
assist public policies of disease control (Morrison
et al., 2014). Recent studies have covered appli-
cations that promote the practice of physical activi-
ties that meet fundamental characteristics of mHealth
and tracks physical activity and food comsuption be-
havior data (Al Ayubi et al., 2014). According to
a recent mHealth apps review (Knight et al., 2015),
there is no application that supports specifically pub-
lic guidelines for aerobic physical activity (Tucker
et al., 2011).
This study aimed to develop a mobile applica-
tion model that supports public guidelines for aerobic
physical activity. This paper is not focused neither
in deploy nor test the app on site. It provides an op-
portunity to support government health programs. We
show the development of application, called WorkUp.
It enables the health professional such as physical ed-
ucator linked to government health programs to evalu-
ate patients and track medical histories with a variety
of methods, such as: a) calculation of body fat in-
dex; b) determination of types of exercises and daily
activities; c) class scheduling; d) interaction between
both professional and patient; and, e) app data can be
accessed with any mobile device connected on the In-
ternet.
dos Santos V., Yoshikazu Shishido H., Pereira Junior F. and Eler G.
WorkUp: A Mobile Application to Support Health Guidelines.
DOI: 10.5220/0006142902970304
In Proceedings of the 10th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2017), pages 297-304
ISBN: 978-989-758-213-4
Copyright
c
2017 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
297

The remaining part of the paper proceeds as fol-
lows: we discussed about related studies in second
section. Section three presents the technologies, de-
velopment process, software architecture, and tests
and validation methods. In section four, the project
implementation is presented. The fifth section is pre-
sented a qualitative evaluation about our design ac-
ceptance through users interview. Finally, we present
our conclusion and limitations of our study in the sec-
tion six.
2 RELATED WORK
Studies in several countries show success in com-
bating obesity using physical activity together with
combined interventions: changes to food/diet, in-
creased physical activity, and behavioral strategies
(Jebb et al., 2011; Turner et al., 2012). Face-to-face
approaches are effective, but they are relatively ex-
pensive to implement, difficult to scale up, and do not
suit those who work or live far from venues. The addi-
tion of mHealth apps in everyday life offers a practical
and potentially cost-effective solution to the barriers
of face-to-face approaches (Waterlander et al., 2014).
Researches demonstrated strong support for a
mHealth weight management intervention; with 75%
saying they would use a mobile app for weight man-
agement intervention (Gorton et al., 2011). Another
study showed that the widespread use of information
and communication technology tools offers an inno-
vative and potentially beneficial avenue to increase
the level of physical activity in Heart Failure (HF) pa-
tients (Franklin, 2015).
A survey performed in 2012, shows 50 applica-
tions available in Brazil within the health field, of
which 20 belong only to the Android platform, 19 to
the iOS platform, 6 on the Windows Phone platform,
1 supporting the three platforms (Diet and Health),
and 4 common to Android and iOS platforms (SUS
Procedures, SAESP, Measure One and Emagrecen-
tro). They are mostly free (32 apps), but the Android
platform leads to greater amount of paid applications.
The content of more than half of these applications is
aimed at professionals. The applications targeting the
consumer public deal primarily with issues related to
diet and physical conditioning (Bonome et al., 2012).
But still, comprehensive applications that enable a
range of information about the patient and that allow
the participation in the evolution process of his gen-
eral state of health and weight are necessary. This is
why we purposed and developed the WorkUp, based
on users’ needs becoming part of a National Policy
for Health Promotion.
WorkUp, as other studies, has shown interest and
adherence on the part of those involved. Some authors
demonstrated that the success level of health services
depends on the level of user acceptance and adoption
(Sezgin and Yıldırım, 2014). Additional research is
needed to explore several hypotheses. For example, if
more engaging user interfaces, including easier nav-
igation, simpler layouts, and refined aesthetics can
contribute to the adherence of mHealth apps. Then,
from this point of research design, the emerging stud-
ies should include more qualitative approaches and
longitudinal studies in order to effectively understand
the user’s needs (Kaplan and Maxwell, 2005), which
can strengthen the qualitative research conducted for
the WorkUp.
3 METHODS
For the application’s development, the system plan-
ning, design, and implementation were performed.
Later, an evaluation of usability was applied in pa-
tients and health professionals.
3.1 Technologies and Tools
We adopted Android platform due to its highly used
technology, its ability to support wide hardware com-
patibility, and to offer many components that provide
a good user interaction. The codification is based on
Java and eXtended Markup Language (XML) files de-
scribe in the user interface. The Android Develop-
ment Toolkit (ADT) was adopted for application test
through the use of its virtual device emulator.
The artefacts and requirements were modelled in
Unified Modelling Language (UML) to design sys-
tem diagrams using Astah Community Edition. The
database was designed in BrModelo software that
generates database script commands. SQLite was the
system database employed for data persistence due to
its native support for Android, good performance and
low resources usage. In Android Development Tools
(ADT) contains a manager for SQLite databases in
order to handle data manually during development.
WorkUp data is stored on the cloud to get a wide
geographic access and allow users access to their syn-
chronized data, regardless of the device. Web service
technology was chosen to synchronize the local data
with the cloud, as it works as a neutral technology that
can transmit data and be easily adapted to any other
technology.
HEALTHINF 2017 - 10th International Conference on Health Informatics
298
3.2 Data Synchronization
The application server was deployed on Amazon EC2
Services. The operating system was Linux Ubuntu
14.04, Java 8, and MySQL database to store all data
through web services.
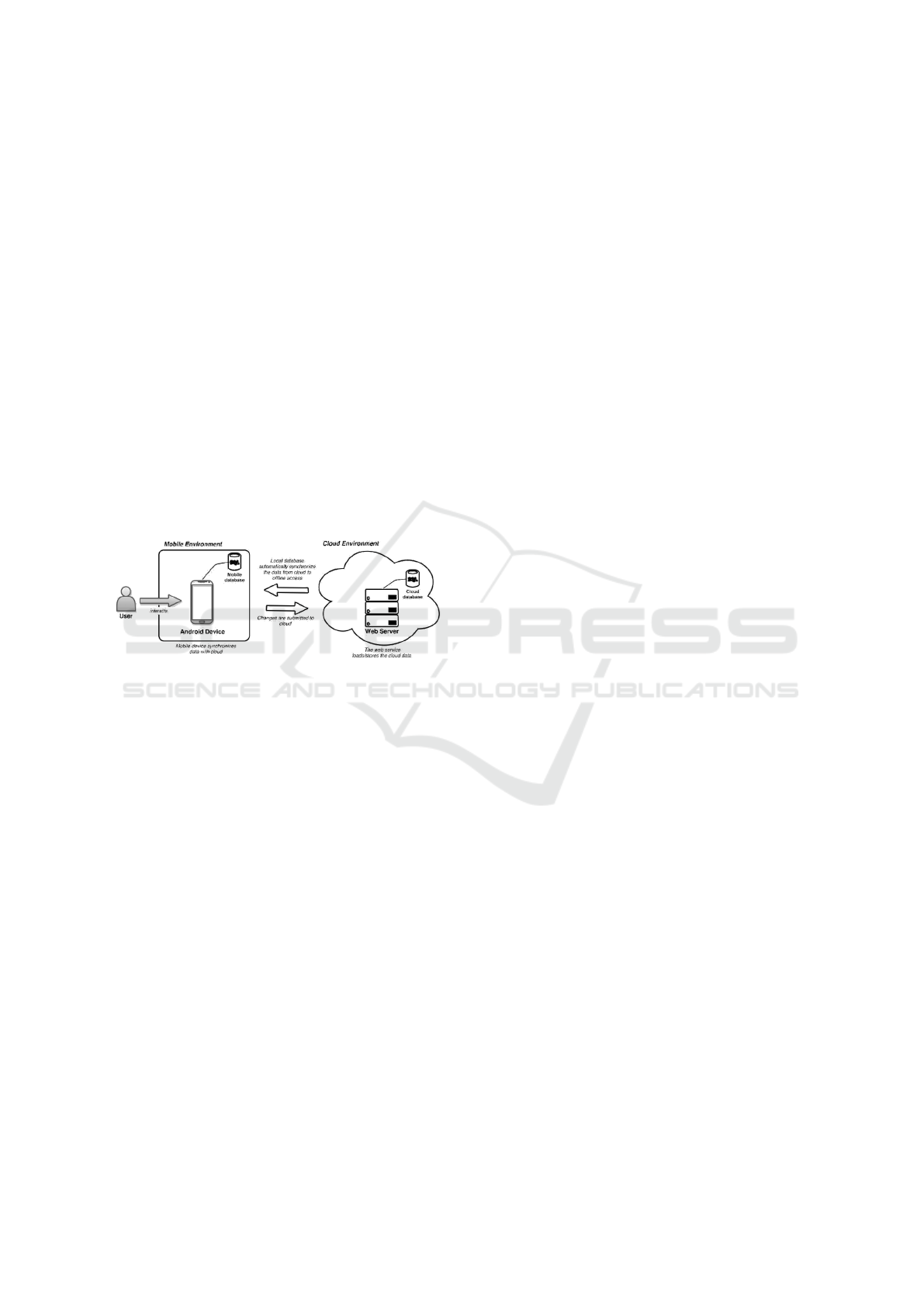
When our application is installed on a mobile de-
vice, it starts a service that periodically communicates
with the data synchronization web service. Clients
perform a query to check available updates in cloud
database. The communication model is represented
in Figure 1. If there is an update, the appropriate rou-
tine will be started automatically to synchronize the
data.
The security of data communication can be treated
in three ways. Firstly data is encrypted before it will
be sent to server or retrieved from it. Before the data
transmission to cloud, data is encrypted and its in-
tegrity is checked when arrives on the other side. In
local SQLite database, there are libraries to encrypt
data such as SQLCipher and SQLiteCrypt.
Figure 1: Data synchronization model of WorkUp.
4 PROJECT RESULTS
This section describes our app structure and use-flow.
Our application has two user types: health profes-
sional (HP) and patient (P). Each one performs differ-
ent activities on app. Both user type share functionali-
ties such as account activities and view patient assess-
ment, training set and class schedule. However, there
are particular functions, which each user type can ac-
cess. Health professional are able to create patient
assessments, create or reuse training sets and manage
class schedules. These functionalities are organized
in modules, which are detailed in Table 1.
The basic use-flow consists in both user types cre-
ate an account on app. After, health professional
should add a relationship with his respective patients.
The patients list of a health professional must be de-
fined by the health unit. The patient must accept the
request for relationship with the health professional.
For each patient, the health team can schedule an as-
sessment in order to verify patient health indicators.
This assessment can be performed periodically in or-
der to track the patients’ health progress. Then, the
physical educator can create a training set based on
patient’s physical needs and send it to him. The exe-
cution of exercises is registered by the patient on app,
and it can be visualized by the physical educator. Ac-
cording to health program policy, there is an option to
the HP schedule classes with patients individually or
in groups. If the patient agrees with proposed sched-
ule, he can accept it. Otherwise, the patient can mes-
sage his health professional asking another available
time.
4.1 Profile Management and User
Communication
Local data persistence and guidelines to allow com-
munication between the mobile app and web service
to validate login (F1) were some of the features imple-
mented. The Facebook API was integrated to provide
access to the app using a Facebook account (F2). A
notification and synchronization service (F16) had to
be created in order to keep communication between
the patient and the professional. We have also de-
veloped functions such as search user (F5), with the
option of adding other users to the contact list. As
stated earlier, a professional can establish connection
with several patients. When clicking on a patient, the
professional can manage his patients through an inter-
face that allows access to assessments, training pre-
scriptions, class schedule, and the removal of the pa-
tient (F6) from his list. The concern of the third sprint
was the implementation of the interfaces for personal
data handling through control panels, where the user
has access to information and can update it as desired
(F7).
4.2 Management of Assessments
The second module deals with the management of as-
sessments. It was concerned in keeping some char-
acteristics in data collection, such as the interfaces
understanding, separation of each type of evaluation,
upload to web server, and both view and delete as-
sessments.
The patient assessment tool (F8) was divided into
four parts: a) verification of goals with the new
training routine and verification of cardiorespiratory
health through the maximum blood pressure during
exercise and blood pressure at rest, as shown in Fig-
ure 2a; b) questionnaire of medical history through
Pfeiffer questionnaire, which detect if there is any
history or risk involving cardiorespiratory shortcom-
ings, pain, recurrent chronic problems in implement-
ing physical activity, loss consciousness, coronary
problems or some other risk factors (Figure 2b); c)
WorkUp: A Mobile Application to Support Health Guidelines
299
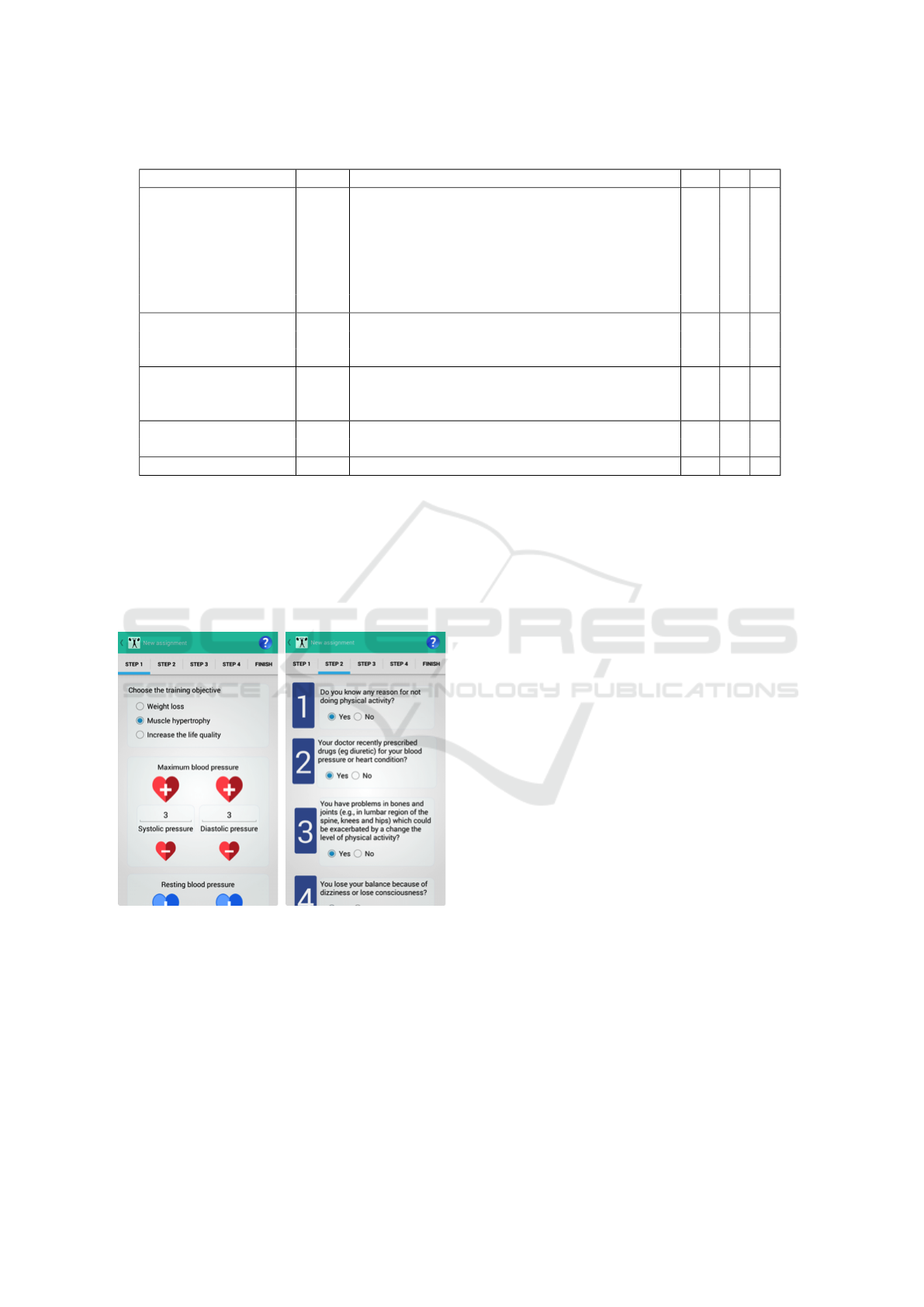
Table 1: Functionalities of each use-case allowed for Health Professional (HP), Patient (P), and System (S).
Use Case ID Functionality HP P S
Manage Profile
(F1) Standard login X X -
(F2) Facebook login X X -
(F3) Create a standard account X X -
(F4) Request relationship to professional X - -
(F5) Search a user X X -
(F6) View assessments, training set, schedule of patient X X -
(F7) Update account X X -
Perform Assessment
(F8) Create a new patient assessment X - -
(F9) Send collected data to server - - X
(F10) Notify patient if new assessment is available - - X
Training Management
(F11) Create a training set X - -
(F12) Send completed exercise to server - - X
(F13) Reuse a training set X - -
Class Schedule
(F14) Schedule a new class X - -
(F15) Confirm a class schedule - X -
Non-functional (F16) Notification and synchronization service - - X
the body fat assessment through a variety of skin-
fold methods; and, d) perimetry assessment, which
enables log measures of body parts. Beyond the nu-
merical evaluation functionality was integrated using
the smartphone camera for photographic record of the
evaluated body members.
(a) (b)
Figure 2: Evaluation management screens: (a) Objectives
and blood pressure; (b) Questionnaire (QPAF); (c) Body fat
calculation.
Existent apps adopt a unique skinfold method.
However, each professional need a specific applica-
tion, according to the physical characteristics of the
patient. So, in this sense, WorkUp has a variety of
skinfold methods to calculate body fat. We have im-
plemented both Jackson Pollock 3 and 7-site, and
Guedes methods. At the end of each assessment, the
professional needs Internet access to send the col-
lected data (F9) and automatically notify the patient
(F10) that there is a new assessment available.
4.3 Training Management
The training has two types of exercises, which can
be created by the own professional. Some rules were
added to the application to improve system usability.
After, it was marked by the inclusion of functionality
to create a training list (F11) according to the purpose
of the patient, inserting both aerobic and anaerobic
exercises. Only the professional can mount the train-
ing set, leaving the patient with the exercises only.
Following the conclusion of training, the patient’s col-
lected data are sent to a web database (F12) and will
be available for professional access to track the pa-
tient’s evolution.
These functionalities were developed and are
shown in Figure 3. The training sessions that have al-
ready been created can be reused by the professional
(F13), as shown in Figure 3a. In order to add a new
training, it is necessary to enter a name, add exer-
cises by clicking on the +1 button (Figure 3b), and
view the registered exercises classified between aer-
obic and anaerobic (Figure 3c), with name, duration,
repetition times, and rest duration (Figure 3d).
4.4 Class Management
This module allows the application to control the class
scheduling (F14) to improve communication between
patient/professional. To use it, the patient needs to
bound to the professional, so the patient can schedule
HEALTHINF 2017 - 10th International Conference on Health Informatics
300

(a) (b)
(c) (d)
Figure 3: Training management screens: (a) My trainings;
(b) Edit training; (c) Registered exercises; (d) Characteris-
tics of exercises.
a new class and the health professional can accept it or
not. For a confirmation of a new class (F15), it is nec-
essary that both agree and confirm the date and time.
If there are any changes, both users will be notified by
the system.
For the scheduling of a new class, the interface
displayed in Figure 4a was built, requiring the pa-
tient/professional to select a date and time, with the
ability to verify if the selected time is available. Users
are notified to change the status of the class to con-
firmed, registering the schedule of classes. (Figure
4b).
In addition, we have considered good practices for
interface design in order to assist the user of our ap-
plication.
(a) (b)
Figure 4: Classes management screens: (a) Schedule new
class; (b) User calendar.
5 EVALUATION
In order to validate our purpose, we adopted the quali-
tative research approach because it reveals a target au-
dience’s range of behaviour and perceptions. It uses
in-depth opinions of small groups of people to sup-
port the construction of hypotheses through descrip-
tive statements. The categories extracted from the
answers of the participants were: a) effective regis-
tration method; b) ability to monitor more patients;
c) accessibility of information; d) information distor-
tion; and, e) interface and restrictions.
Sixteen participants, including health profession-
als and patients in both Corn
´
elio Proc
´
opio and Ser-
taneja cities, located in south Brazil, tested our appli-
cation.
Several interfaces were sketched and tested by
four health professionals and twelve patients. The app
validation was performed by 17 questions focused on
usability of the system. Participants were divided into
HP1 to HP4 (Health Professional) and P1 to P12 (Pa-
tients). Participants were asked to download the ap-
plication in order to explore and test the app func-
tionality. Next, the participants were requested to an-
swer the questionnaire. All data, comments, sugges-
tions and detected problems were analyzed and used
as a source of information to evaluate the system. Re-
sponses were categorized and described19-21 as: a)
effective registration method for physical educators;
b) ability to monitor more patients; c) accessibility of
information; d) information distortion; and, e) inter-
face and restrictions.
• Effective registration method As main results,
WorkUp: A Mobile Application to Support Health Guidelines
301
participants emphasized that the control of phys-
ical activity is important for physical educators.
Interviewed professionals highlighted the need to
establish goals and analyze if the results obtained
have achieved them. According to the answers, it
is difficult to investigate the causes of inefficiency
in the physical training because of the lack of ef-
fective registration methods to collect the patient’s
exercise routine. Table 2 presents the users reports
referring to the registration method.
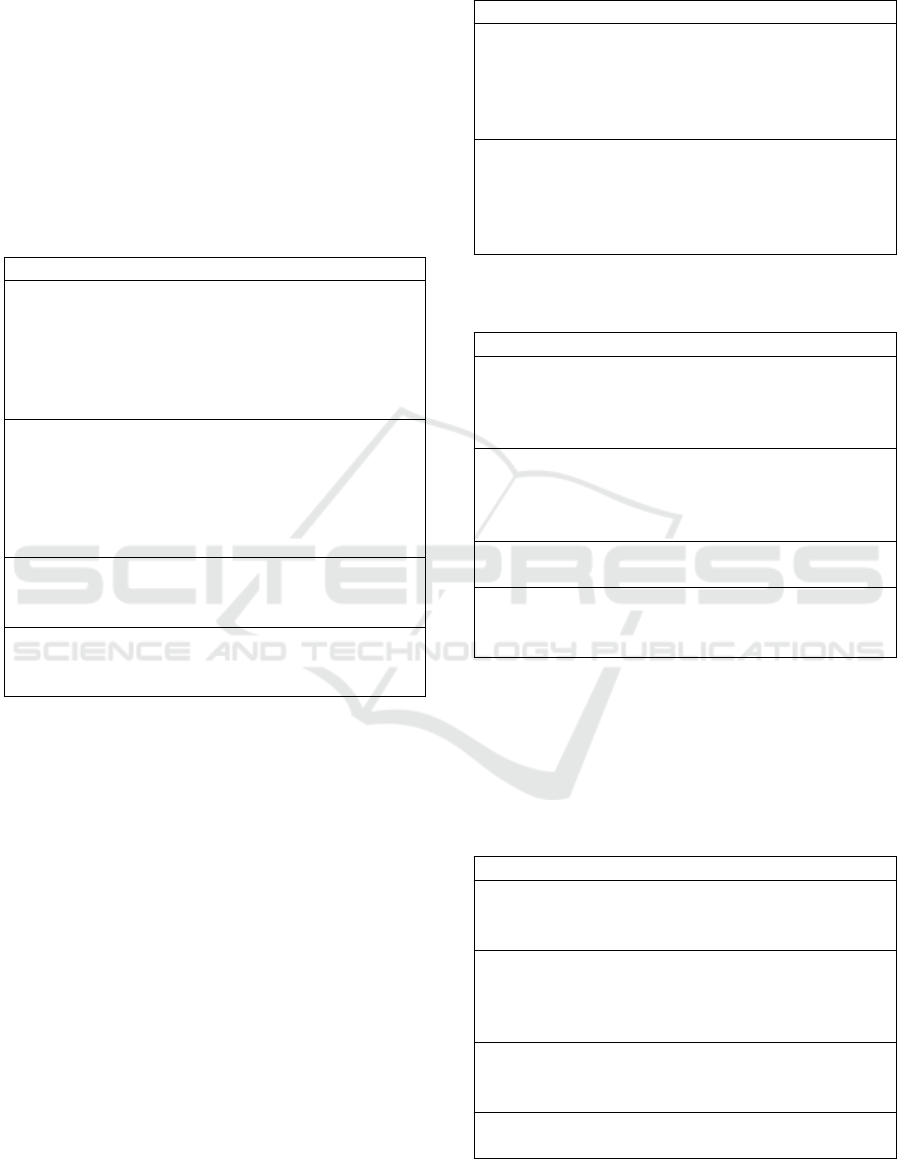
Table 2: User experience report about effective registration
method from Health Professionals (HP).
User experience report
HP 1: “It is difficult to monitor patients efficiently
without a digital record. Most of the time there
is only an initial assessment and a pre-prepared
program for the patient to conduct over a period
of time without a complete record of case histories
and prescribed activities.”
HP 2: “You need an environment where the
teacher can record all information, such as
lessons, exercises and schedules, in order to effec-
tively monitor the patient. In addition, through the
systematization of information, you can organize
and visualize where the gaps are in training.”
HP 3: “It is necessary to check how the patient’s
training was in relation to the time for without this
analysis, all is vague.”
HP 4: “I need to know if the patient is actually
losing weight with the training, and if the tracing
objective is being achieved.”
• Ability to monitor more patients It is common for
a health professional to track multiple patients at
the same time. This scenario is unfavorable for
the quality of training provided to patients. Some
interviewees pointed out that our app could help
professionals to follow a larger number of patients
with high quality. Table 3 shows the discourse of
users that have tested the application, analyzing
the resources to follow multiple patients.
• Accessibility of information Among the ques-
tions, the accessibility of the information required
for patients’ assessment was mentioned. The
health professionals noted that some data are rela-
tively complicated to extract, but are necessary for
the proper development of activities, as described
in Table 4.
• Information distortion The professionals point out
that, in some cases, patients promote distortions
in data collection, omitting important information
about their health status (Table 5). There are cases
Table 3: User experience reports about ability to monitor
more patients.
User experience report
HP 2: “... I have on hand an easy way to record
the data of my patients, which this training should
follow. In addition, the
schedule allows better distribution of times so I
can organize myself.”
HP 3: “It bothers me not keeping up with the pa-
tients, and not even knowing their workout for that
day, because I cannot handle
looking at the previous training and make the out-
line of the next.”
Table 4: User experience report about accessibility of infor-
mation.
User experience report
HP 1: “... I have on hand an easy way to record
the data of my patients, which this training should
follow. In addition, the schedule allows better dis-
tribution of times so I can organize myself.”
HP 2: “It bothers me not keeping up with the pa-
tients, and not even knowing their workout for that
day, because I cannot handle looking at the previ-
ous training and make the outline of the next.”
P4: “I think the data is very specific and under-
standing it is complex.”
P11: “At first sight, the need for data is difficult to
understand, but once it is properly explained it is
easy to understand its importance.”
where patients find unnecessary to fill out per-
sonal data in the application. The patient gener-
ally has no idea of the importance of evaluation
for the prescription of activities.
Table 5: User experience report about distortion of informa-
tion.
User experience report
HP 1: “There are some points that can be filled in-
correctly, which can work as a motivation to create
new ways to reduce distortions.”
HP 2: “The system as presented does not have
methods that can prevent inconsistencies, for ex-
ample, a patient who does not perform the exer-
cises correctly.”
P7: “We cannot guarantee that the data entered by
the patients during the execution of exercises are
really reliable.”
P10: “This app would be of little use because I’m
not used to perform this type of control.”
• Interface and restrictions When participants were
HEALTHINF 2017 - 10th International Conference on Health Informatics
302

asked about the interface, system language, ef-
ficiency in performing the activities, arrange-
ment of dialog boxes, error messages, and system
iconography, there were no serious abnormality
highlighted. But the health professionals pointed
out that a more restrictive system would be inter-
esting for more effectiveness in achieving results
(Table 6).
Table 6: User experience report about interface and appli-
cation restrictions.
User experience report
HP 3: “The application is very pleasing to the eye
and easy to understand.”
HP 4: “It would be interesting if there was a way
to make it easier for patients to access the training
to be carried out.”
P6: “The interface is pretty nice and does not
show navigation problems.”
P9: “I found no serious problems.”
P12: “Some data is complicated to collect and un-
derstand, it needs an improved interface.”
6 CONCLUSION
Physical evaluation software has been developed to
desktop computers. However, with popularization of
mobile technologies, the adoption of mobile apps is
undoubtedly a useful solution. For health profession-
als, the advantage of portability overcomes some bar-
riers and allows the tracking of training, improving
professional-patient communication, and allowing the
follow-up of training guidelines with more effective-
ness.
The WorkUp can be a model to support health
agencies to promote a healthier life and keep record of
the patient physical assessments. The application also
provides users with the ability to keep tracking im-
portant health indicators that show the patient’s evo-
lution. As pointed out earlier, mobile technology is
constantly evolving in the applications market, that
is, every day there are new startups focusing on health
and exercise routines. Therefore, WorkUp has to add
up to this scenario, providing important information
for health professionals. This information can assist
professionals to achieve better results and improve the
quality of life of their patients.
A limitation of this study relates to the perfor-
mance of physical activities, as WorkUp currently re-
stricts to patients the ability to perform physical ac-
tivities proposed by a professional. However, these
mechanisms are dependent on the use of the correct
interface. The system is not integrated to sensors.
Thus, for future work the integration of these tech-
nologies will be accomplished to provide better con-
trol of physical activities.
ACKNOWLEDGEMENTS
The authors acknowledge the support of UTFPR.
REFERENCES
Al Ayubi, S. U., Parmanto, B., Branch, R., and Ding, D.
(2014). A persuasive and social mhealth application
for physical activity: A usability and feasibility study.
JMIR mHealth and uHealth, 2(2).
Bonome, K. d. S., Di Santo, C., Prado, C., Sousa, F.,
and Pisa, I. (2012). Disseminac¸
˜
ao do uso de aplica-
tivos m
´
oveis na atenc¸
˜
ao a sa
´
ude. In XIII Congresso
Brasileiro de Inform
´
atica em Sa
´
ude.
Capilheira, M. F., Santos, I. S., Azevedo Jr, M. R., and
Reichert, F. F. (2008). Risk factors for chronic non-
communicable diseases and the carmen initiative: a
population-based study in the south of brazil. Cader-
nos de Saude Publica, 24(12):2767–2774.
da Sa
´
ude, M. (2014). Strategies for the care of the per-
son with chronic disease: Obesity. Departamento de
Atenc¸
˜
ao B
´
asica.
Franklin, N. C. (2015). Technology to promote and increase
physical activity in heart failure. Heart failure clinics,
11(1):173–182.
Free, C., Phillips, G., Felix, L., Galli, L., Patel, V., and Ed-
wards, P. (2010). The effectiveness of m-health tech-
nologies for improving health and health services: a
systematic review protocol. BMC Research Notes,
3(1):250.
Gorton, D., Dixon, R., Maddison, R., Mhurchu, C. N., and
Jull, A. (2011). Consumer views on the potential use
of mobile phones for the delivery of weight-loss inter-
ventions. Journal of Human Nutrition and Dietetics,
24(6):616–619.
Jebb, S. A., Ahern, A. L., Olson, A. D., Aston, L. M.,
Holzapfel, C., Stoll, J., Amann-Gassner, U., Simpson,
A. E., Fuller, N. R., Pearson, S., et al. (2011). Primary
care referral to a commercial provider for weight loss
treatment versus standard care: a randomised con-
trolled trial. The Lancet, 378(9801):1485–1492.
Kaplan, B. and Maxwell, J. A. (2005). Qualitative re-
search methods for evaluating computer informa-
tion systems. In Evaluating the organizational im-
pact of healthcare information systems, pages 30–55.
Springer.
Knight, E., Stuckey, M. I., Prapavessis, H., and Petrella,
R. J. (2015). Public health guidelines for physical ac-
tivity: is there an app for that? a review of android and
apple app stores. JMIR mHealth and uHealth, 3(2).
WorkUp: A Mobile Application to Support Health Guidelines
303

Morrison, Z., Fernando, B., Kalra, D., Cresswell, K., and
Sheikh, A. (2014). National evaluation of the bene-
fits and risks of greater structuring and coding of the
electronic health record: exploratory qualitative inves-
tigation. Journal of the American Medical Informatics
Association, 21(3):492–500.
Popkin, B. M. (2011). Is the obesity epidemic a national
security issue around the globe? Current opinion in
endocrinology, diabetes, and obesity, 18(5):328.
Schmidt, M. I., Duncan, B. B., e Silva, G. A., Menezes,
A. M., Monteiro, C. A., Barreto, S. M., Chor, D., and
Menezes, P. R. (2011). Chronic non-communicable
diseases in brazil: burden and current challenges. The
Lancet, 377(9781):1949–1961.
Sezgin, E. and Yıldırım, S.
¨
O. (2014). A literature review on
attitudes of health professionals towards health infor-
mation systems: from e-health to m-health. Procedia
Technology, 16:1317–1326.
Tucker, J. M., Welk, G. J., and Beyler, N. K. (2011). Physi-
cal activity in us adults: compliance with the physical
activity guidelines for americans. American journal of
preventive medicine, 40(4):454–461.
Turner, M., Burns, S. M., Knight, L., Ward, K., Garo,
A., Morris, T., Hooper, E., and Conaway, M. (2012).
Weight management practices among heart and vas-
cular health care providers in an ambulatory setting.
Medsurg Nursing, 21(4):222.
Waterlander, W., Whittaker, R., McRobbie, H., Dorey, E.,
Ball, K., Maddison, R., Smith, K. M., Crawford, D.,
Jiang, Y., Gu, Y., et al. (2014). Development of an
evidence-based mhealth weight management program
using a formative research process. JMIR mHealth
and uHealth, 2(3):e18.
HEALTHINF 2017 - 10th International Conference on Health Informatics
304
