
Technologies for Ageing in Place to Support Home Monitoring of
Patients with Chronic Diseases
Alexandra Queirós
1
, Luís Pereira
2
, Ana Dias
3
and Nelson Pacheco Rocha
4
1
Health Sciences School, University of Aveiro, Campo Universitário de Santiago, 3810-193 Aveiro, Portugal
2
Medtronic Portugal, Torres de Lisboa, Rua Tomás da Fonseca, Torre E - 11º andar, 1600-209 Lisboa, Portugal
3
Department of Economicas, Management, Industrial Engineering and Tourism, University of Aveiro, Campo
Universitário de Santiago, 3810-193 Aveiro, Portugal
4
Department of Medical Sciences, University of Aveiro, Campo Universitário de Santiago, 3810-193 Aveiro, Portugal
Keywords: Technologies for Ageing in Place, Home Monitoring, Chronic Diseases, Older Adults.
Abstract: Objectives - This study aims to identify: i) the most relevant chronic diseases in terms of the use of
technologies for ageing in place to support home monitoring; and ii) types, outcomes and impacts of
technologies for ageing in place being used to support home monitoring. Methods - A systematic review of
reviews and meta-analysis was performed based on a search of the literature. Results - A total of 35 reviews
and meta-analysis across 4 chronic diseases, diabetes, congestive heart failure, chronic obstructive
pulmonary disease, and hypertension, were retrieved. These studies compare home monitoring supported by
different technologies with usual care. Conclusion - Home monitoring has positive effects in various health
related outcomes, but further research is required to allow its incorporation in the clinical practice.
1 BACKGROUND
The active ageing concept refers not only to the
ability to be physically active or have an occupation,
but also to be able to participate in social, economic,
cultural, civil or spiritual matters (Kickbusch and
Nutbeam, 1998; World Health Organization, 2002).
Therefore, the older adults, even when having some
kind of pathology or disability, should continue to
contribute actively in social terms, together with
their family, friends and community (Kickbusch and
Nutbeam, 1998). In this context, information
technologies have a key role in the promotion of
human functioning and in the mitigation of
limitations, particularly the ones resulting from the
natural ageing process (Queirós, 2013; 2015).
Technological solutions emerge as potentially
cost-effective to meet the needs of citizens and to
promote the services reorganization (Genet et al.,
2011), which are the aims of concepts such as
Medicine 2.0 (Eysenbach, 2008), connected health
(Kvedar, Coye, and Everett, 2014), or holistic health
(Mori et al., 2013; Koch, 2013). In particular,
technologies for ageing in place (Connelly, Mokhtari
and Falk, 2014) can overcome multiple impairments,
including declines in cognitive and functional
abilities (Teixeira et al., 2013; Cruz et al., 2013;
2014) and, consequently, can allow older adults to
live safely, independently, autonomously, and
comfortably, without being required to leave their
own residences, but with the necessary support
services to their changing needs (Pastalan, 1990).
The present study is part of a medium term
project that aims to systematize current evidence of
technologies for ageing in place. Particularly, a
systematic review of reviews and meta-anaysis was
perform to identify technologies being used to
support home monitoring of patients with chronic
diseases, not specifically designed for older adults,
but that can be used by this population, and to
analyse how these tecnologies impact health related
outcomes.
There are several reviews of reviews related to
home care of patients with chronic diseases
(Househ, 2014; McBain, Shipley and Newman,
2015; Kitsiou, Paré and Jaana, 2015; Slev, 2016).
However, these reviews focus on specific
technologies (e.g. short message services (Househ,
2014), or specific pathologies (e.g. congestive heart
failure (Kitsiou, Paré and Jaana, 2015)). Therefore,
the broad analysis of the study reported in the
present article is useful to inform: i) the practitioners
66
Queirøss A., Pereira L., Dias A. and Pacheco Rocha N.
Technologies for Ageing in Place to Support Home Monitoring of Patients with Chronic Diseases.
DOI: 10.5220/0006140000660076
In Proceedings of the 10th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2017), pages 66-76
ISBN: 978-989-758-213-4
Copyright
c
2017 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

about the available home monitoring solutions; and
ii) the researchers about home monitoring issues that
are being object of research.
2 METHODS
Considered the aforementioned objective, the
systematic review of reviews and meta-analysis
reported in the present article was informed by the
following research questions:
What are the most relevant chronic diseases in
terms of the use of technologies for ageing in
place to support home monitoring?
What are the types, outcomes and impacts of
technologies for ageing in place being used to
support home monitoring?
In order to determine the most appropriate search
strategy, an initial scoping study was conducted. The
outcomes of this process were discussed with
various researchers and captured in a review
protocol with explicit descriptions of the methods to
be used and the steps to be taken.
The resources considered to be searched were
two general databases (i.e. Web of Science and
Scopus) and two specific databases (i.e. PubMed, a
medical sciences database, and IEEE Explorer, a
technological database).
The list of keywords for the systematic review
was created through three steps:
First, health related and technological terms
were selected for a draft search strategy based
on the terminology that the authors were
familiar due to their background readings. A
preliminary search with the identified
keywords was tested by two authors.
Afterwards, the two authors carried out a hand
search of the table of contents of three
relevant journals: Journal of Telemedicine and
Telecare, Telemedicine and Ehealth and
Journal of Medical Internet Research.
Finally, new keywords were introduced in
order to gather articles of the mentioned
journals that were not retrieved in the previous
queries.
The queries that resulted from these successive
refinements intended to include: i) all the reviews
where any of the keywords ‘telecare’, ‘telehealth’,
‘telemedicine’, ‘homecare’, ‘telemonitoring’, ‘home
monitoring’, ‘remote monitoring´, ehealth´,
‘telerehabilitation’, ‘mobile health’, ‘mhealth’ or
‘assisted living’ were presented in the title or
abstract; and ii) all the reviews where any the
keywords ‘technology-based’, ‘information
technology’, ‘information and communication’,
‘internet-based’, ‘web-based’, ‘on-line’,
‘smartphones’, ‘mobile apps’, ‘mobile phone’,
‘monitoring devices’ or ‘consumer health
information’ were presented in the title or abstract
together with any of the keywords ‘healthcare’,
‘health care’, ‘patient’, ‘chronic disease’, ‘older’ or
‘elderly’.
The search was limited to articles in English, but
conducted in any country, and performed on 30 of
April of 2016, to include reviews published during
the preceding 10 years.
2.1 Inclusion and Exclusion Criteria
The study reported in the present article included
reviews and meta-analysis related to technological
solutions that can be used to support home
monitoring of older adults living with a chronic
disease. Chronic disease is defined as an illness that
is prolonged in duration, has a non-self-limited
nature, is rarely cured completely and is associated
with persistent and recurring health problems
(Thrall, 2005; Australian Institute of Health and
Welfare, 2006).
Since the scientific literature presents a large
number of articles that report studies related to home
monitoring, it was planned to include systematic
reviews or meta-analysis only.
The authors excluded all the articles not
published in English or that report systematic
reviews of reviews. Furthermore, the authors also
excluded all the reviews and meta-analysis reporting
solutions that: i) are not focused on the monitoring
of health conditions; ii) target more than one chronic
condition (e.g. diabetes together with congestive
heart failure); iii) target long-term health condition
not related to older patients (e.g. paediatric
conditions); iv) do not target the patients (i.e. studies
that were clinicians focused or were intended
primary to deal with the problems of caregivers
rather than the patients); and v) were designed to be
used in an institutional environment and not in the
domicile of the patients.
2.2 Review Selection
After the removal of duplicates and articles not
published in English, the selection of the remainder
articles was performed by two authors in three steps:
First, the authors assessed all titles for
relevance and those clearly not meeting the
inclusion criteria were removed.
Technologies for Ageing in Place to Support Home Monitoring of Patients with Chronic Diseases
67
Afterwards the abstracts of the retrieved
articles were assessed against the inclusion
and exclusion criteria.
Finally, authors assessed the full text of the
articles according to the outlined inclusion and
exclusion criteria.
In all these three steps any disagreement between
the two authors was discussed and resolved by
consensus.
2.3 Data Extraction
The following characteristics of the retrieved articles
were extracted: i) authors, title and year of
publication; ii) aims of the review or meta-analysis;
iii) target chronic disease; iv) technologies being
used; v) search strategy; vi) inclusion and exclusion
criteria; vii) quality assessment; viii) data extraction
procedure; ix) total number of primary studies; x)
total number of random clinical trials (RCT); xi)
total number of participants; xii) primary outcomes;
xiii) secondary outcomes; xiv) author’s
interpretations; and xv) author’s conclusions.
The relevant data were extracted and recorded
independently by two authors. Once more, any
disagreement between the two authors was discussed
and resolved by consensus.
3 RESULTS
The present study comprises a narrative synthesis of
the retrieved systematic reviews and meta-analyses
and followed the guidelines of the Preferred
Reporting Items for Systematic Reviews and Meta-
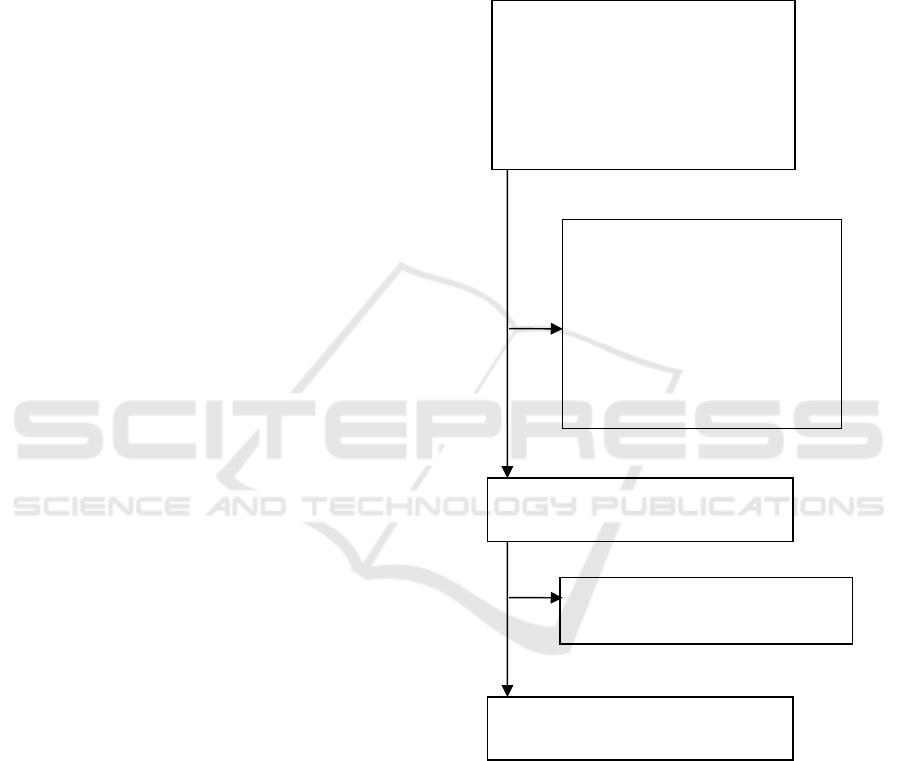
Analyses (PRISMA) (Moher, 2009). Figure 1
presents the respective flowchart.
A total of 2681 articles were retrieved from the
initial searches on PubMed (822 articles), Web of
Science (1263 articles), Scopus (550 articles) and
IEEE Explorer (46 articles). The initial screening
yielded 1429 articles by removing the duplicates
(1210 articles) or the articles without abstracts or
without the names of the authors (42 articles). After
exclusions based on title alone 563 articles were
retrieved. Additionally, 315 articles were eliminated
based upon review of their abstracts.
The full texts of the 248 remaining articles were
assessed and 213 articles were eliminated, due to the
following reasons: i) the studies target multiple
chronic diseases - 102 articles; ii) the main goals of
the studies are health promotion related to general
population - 48 articles; iii) the studies are not
focused on home monitoring of patients with chronic
diseases - 31 articles; iv) the studies are not
systematic literature reviews or meta-analysis - 12
articles - or are reviews of reviews - 3 articles; v) the
target users are not the patients but the caregivers - 8
articles; vi) the reported solutions are to be used in
an institutional environment or are related to acute
conditions - 4 articles; vi) the studies were not
reported in English - 5 articles.
Figure 1: PRISMA Flowchart.
3.1 Characteristics of the Studies
The 35 resulting articles from the filtered queries
synthesize evidence of home monitoring to support
patients with chronic diseases. After an analysis of
the full text of the retrieved articles, they were
categorized into 4 clinical domains: i) diabetes - 20
articles; ii) congestive heart failure - 9 articles; iii)
chronic obstructive pulmonary disease - 5 articles;
and iv) hypertension - 1 article. The following
Articles found (n=2681):
Web Of Science (n=1263);
Scopus (n=550);
PubMed (n=822);
IEEE Explorer (n=46).
Articles underwent full review (n=248).
Articles excluded by preliminary
screening (n=2079):
Duplicate articles (n=1210);
Articles without abstracts (n=42);
Excluded based on titles (n=512);
Excluded based on abstracts
(n=315).
Excluded based on the full review
(n=213).
Total number of articles (n=35).
HEALTHINF 2017 - 10th International Conference on Health Informatics
68

subsections present the results of these 4 categories.
3.2 Diabetes
Of the 35 retrieved articles, 20 dealt with home
monitoring of patients with diabetes. A significant
number of articles focuses both type 1 and type 2
diabetes (Jaana and Paré, 2007; Verhoeven et al.,
2007; Baron, McBain and Newman, 2012; El-Gayar,
2013; van Vugt et al., 2013; Or and Tao, 2014;
Huang et al., 2015; Tildesley, Po and Ross, 2015;
Riazi et al., 2015; Garabedian, Ross-Degnan and
Wharam, 2015). Others articles focus type 2 diabetes
(Jackson, 2006; Ramadas et al., 2011; Frazetta,
Willet and Fairchild, 2012; Cassimatis and
Kavanagh, 2012; Tao and Or, 2013; Huang et al.,
2015; Hunt, 2015; Ortiz, Felix and Sosa, 2015;
Arambepola, 2016). Only one of the retrieved
studies focuses exclusively on type 1 diabetes
(Peterson, 2014).
By principle, the articles of the diabetes category
include primary studies with high quality scientific
evidence. All the 20 retrieved articles considered
RCT primary studies and 11 of them considered
RCT as one of the inclusion criteria (Jaana and Paré,
2007; Verhoeven et al., 2007; Cassimatis and
Kavanagh, 2012; Baron, McBain and Newman,
2012; Pal et al., 2013; Tao and Or, 2013; van Vugt
et al., 2013; Or and Tao, 2014; Huang et al., 2015;
Tildesley, Po and Ross, 2015; Arambepola, 2016).
On the other hand, aggregating all the primary
studies included in the 20 studies of the diabetes
category it is evident that the number of the involved
patients is relatively significant (e.g. 1 article reports
the involvement of 3578 patients (Pal et al., 2013)
and other reports the involvement of 3798 patients
(Huang et al., 2015)).
In technological terms, several articles (Ramadas
et al., 2011; Frazetta, Willet and Fairchild, 2012; El-
Gayar, 2013; Pal et al.; Tao and Or, 2013; van Vugt
et al., 2013; Huang et al., 2015; Tildesley, Po and
Ross, 2015; Riazi et al., 2015; Hunt, 2015) refer
web-based applications (Table 1). In general, these
applications allow synchronous (e.g. instant
messaging or chat) and asynchronous (e.g. electronic
mail or bulletin board) communications together
with web pages to register clinical parameters (e.g.
weight or blood pressure) and medication.
Besides web-based applications, there are other
technological solutions reported in different articles:
Computer-assisted applications integrating the
management of clinical data with electronic
practice guidelines, reminder systems, and
feedback to the patients (Jackson, 2006; El-
Gayar, 2013).
Smartphones (i.e. standalone smartphones and
smartphones integrating specific devices such
as glucometers for automatic glucose level
upload) (Frazetta, Willet and Fairchild, 2012;
Cassimatis and Kavanagh, 2012; Baron,
McBain and Newman, 2012; El-Gayar, 2013;
Pal et al., 2013; Peterson, 2014; Tildesley, Po
and Ross, 2015; Garabedian, Ross-Degnan
and Wharam, 2015; Hunt, 2015; Ortiz, Felix
and Sosa, 2015; Arambepola, 2016).
Automatic patient data transmission by means
of monitoring devices (i.e. devices to monitor
vital signals or devices to monitor behaviour
outcomes such as pedometers or
accelerometers connected by wireless
communications to monitor physical activity
(Jaana and Paré, 2007)).
Video-conference (Verhoeven et al., 2007; El-
Gayar et al., 2013).
Telephone calls (Riazi et al., 2015).
The main outcome of most of the articles
included in the diabetes category is the control of
glycaemia by using glycosylated haemoglobin
(HbA1c) as a proxy. However, in all the studies, this
aim is complemented with other health related
outcomes (e.g. health related quality of life
(Verhoeven et al., 2007; Ramadas et al., 2011; Pal et
al., 2013; van Vugt et al., 2013), weight (Ramadas et
al., 2011; Pal et al., 2013; Huang et al., 2015;
Garabedian, Ross-Degnan and Wharam, 2015),
depression (Pal et al., 2013), blood pressure
(Verhoeven et al., 2007; Or and Tao, 2014; Riazi et
al., 2015; Garabedian, Ross-Degnan and Wharam,
2015), cholesterol level (Ramadas et al., 2011; Or
and Tao, 2014), triglycemius level (Or and Tao,
2014), fluctuation index (Ramadas et al., 2011)),
behaviour outcomes (e.g. physical activity)
(Jackson, 2006; Verhoeven et al., 2007; Ramadas et
al., 2011; Cassimatis and Kavanagh, 2012; van Vugt
et al., 2013; Riazi et al., 2015; Garabedian, Ross-
Degnan and Wharam, 2015; Hunt, 2015;
Arambepola, 2016), patient self-motivation
(Tildesley, Po and Ross, 2015), patient-clinician
communication (Tildesley, Po and Ross, 2015),
medication adherence (Cassimatis and Kavanagh,
2012; Hunt, 2015) ), and structural outcomes related
to care coordination (Jaana and Paré, 2007;
Verhoeven et al., 2007).
Technologies for Ageing in Place to Support Home Monitoring of Patients with Chronic Diseases
69

Table 1: Articles that focus diabetes.
Study Technology
(*)
Jackson et
al., 2006
Web-based applications,
computer assisted applications
and standard telephone calls
26/14
Jaana et al.,
2007
Automatic patient data
transmission by means of
monitoring devices
17/17
Verhoeven
et al., 2007
Video-conference 39/39
Ramadas et
al., 2011
Web-based applications 13/8
Frazettaet
al., 2012
Smartphones 7/7
Cassimatis
et al., 2012
Smartphones 13/13
Baron, et
al., 2012
Smartphones 24/24
El-Gayar et
al., 2013
Web-based applications,
smartphones, computer assisted
applications and video-
conference
104/60
Pal et al.,
2013
Web-based applications and
smartphones
16/16
Tao et al.,
2013
Web-based applications 43/43
van Vugt et
al., 2013
Web-based applications 13/13
Or et al.,
2014
Web-based applications 67/67
Peterson Smartphones 14/1
Huang et
al., 2015
Web-based applications and
standard telephone calls
18/18
Tildesley et
al., 2015
Web-based applications and
smartphones
22/22
Riazi et al.,
2015
Web-based applications and
standard telephone calls
67/52
Garabedian
et al., 2015
Smartphones 1479
Hunt, 2015
Web-based applications and
smartphones
14/9
Ortiz et al.,
2015
Smartphones 8/4
Arambepola
et al., 2016
Smartphones 13/13
(*) Number of RCT included in the review / Number of
primary studies include in the review.
Most of the articles of the diabetes category
report moderate to large significant reduction of
HbA1c when compared with usual care (Jackson,
2006; Jaana and Paré, 2007; Frazetta, Willet and
Fairchild, 2012; Cassimatis and Kavanagh, 2012;
Tao and Or, 2013; Or and Tao, 2014; Peterson,
2014; Huang et al., 2015; Tildesley, Po and Ross,
2015; Riazi et al., 2015; Garabedian, Ross-Degnan
and Wharam, 2015; Hunt, 2015; Ortiz, Felix and
Sosa, 2015; Arambepola, 2016). However, several
studies are not conclusive about the reduction of
HbA1c (Verhoeven et al., 2007; Ramadas et al.,
2011; Baron, McBain and Newman, 2012; Pal et al.,
2013). In particular, computer-based diabetes self-
management interventions (Pal et al., 2013) and
consultations supported by video-conference
(Verhoeven et al., 2007) appear to have a small
beneficial effect on glycaemia control.
An article (El-Gayar et al., 2013) reporting
research gaps of the technological approaches
identifies the need to improve the usability of the
applications as well the need for more
comprehensive solutions, including real-time
feedback to the patients and the integration of
electronic health records systems supporting the
service providers.
3.3 Congestive Heart Failure
The number of RCT and non-RCT primary studies
included in the 9 articles dealing with congestive
heart failure varies from 9 to 42 (Table 2). The
majority of the articles (i.e. 6 articles (Chaudhry et
al., 2007; Dang, Dimmick and Kelkar, 2009;
Polisena et al., 2010a; Ciere, Cartwright and
Newman, 2012; Conway, Inglis and Clark, 2014;
Nakamura, Koga and Iseki, 2014)) considered RCT
as one of the inclusion criteria.
Considering the supporting technologies (Table
2), automatic patient data transmission by means of
monitoring devices is being used together with
video-conference and standard telephone calls to
allow the assessment of symptoms and vital signs, as
well as the transmission of automatic alarms.
In terms of clinical outcomes, the main concerns
are the impacts of home monitoring in heart failure-
related hospitalizations and all-cause mortality
(Conway, Inglis and Clark, 2014) when compared
with usual care. However, several secondary
outcomes are also considered such as self-care
behaviour (e.g. adherence to prescribed medication,
daily weighing or adherence to exercise
recommendations (Ciere, Cartwright and Newman,
2012)).
HEALTHINF 2017 - 10th International Conference on Health Informatics
70
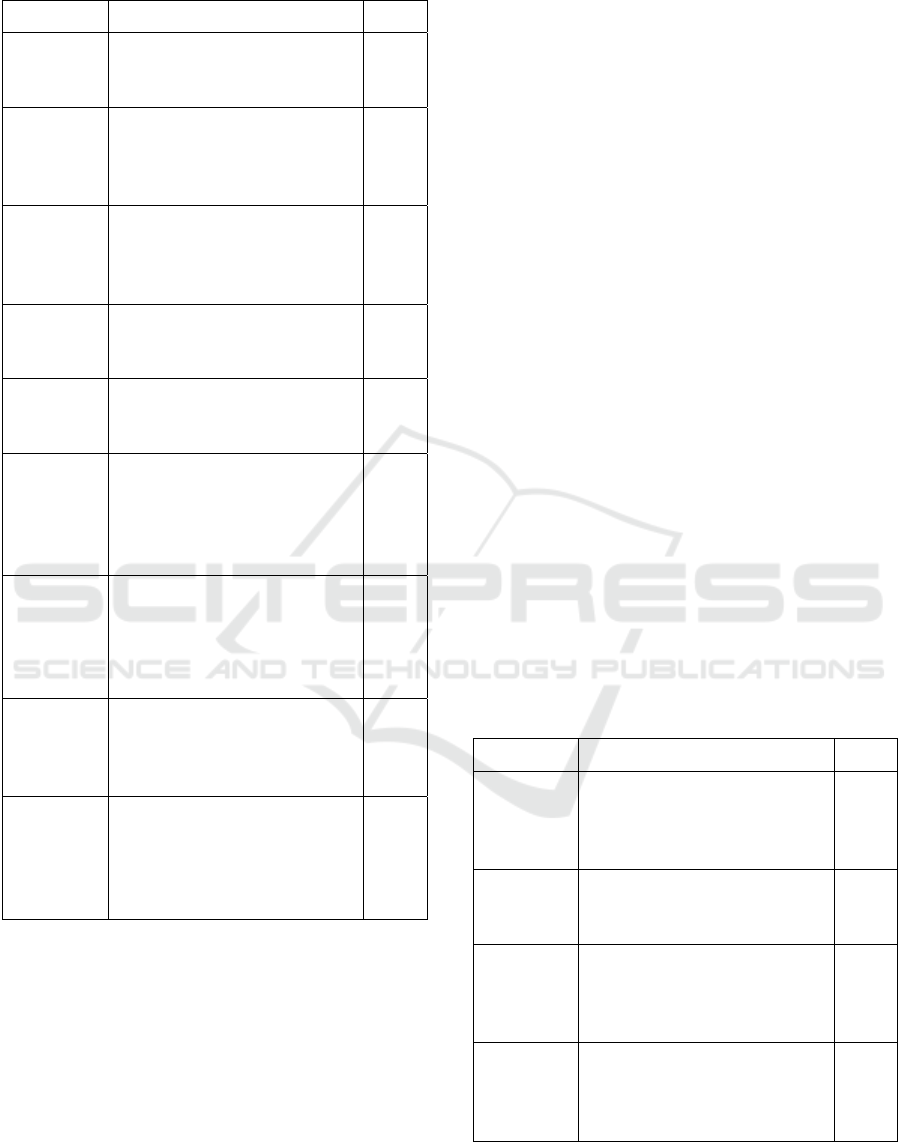
Table 2: Articles that focus congestive heart failure.
Study Technology
(*)
Martínez et
al., 2006
Automatic patient data
transmission by means of
monitoring devices
42/13
Chaudhry et
al., 2007
Automatic patient data
transmission by means of
monitoring devices and standard
telephone calls
9/9
Clark et al.,
2007
Automatic patient data
transmission by means of
monitoring devices and standard
telephone calls
14/14
Dang et al.,
2009
Automatic patient data
transmission by means of
monitoring devices
9/9
Polisena et
al., 2010a
Automatic patient data
transmission by means of
monitoring devices
9/9
Ciere et al.,
2012
Automatic patient data
transmission by means of
monitoring devices and standard
telephone calls and video-
conference
12/7
Grustam et
al., 2014
Automatic patient data
transmission by means of
monitoring devices and standard
telephone calls and video-
conference
32/21
Conway et
al.
Automatic patient data
transmission by means of
monitoring devices and standard
telephone calls
25/25
Nakamura
et al., 2014
Automatic patient data
transmission by means of
monitoring devices, including
external, wearable, or
implantable electronic devices
13/13
(*) Number of RCT included in the review / Number of
primary studies include in the review.
Accordingly the reviewed articles home
monitoring has a positive effect on clinical outcomes
in community dwelling patients with congestive
heart failure. Home monitoring reduces mortality
when compared with usual care and it also helps to
lower both the number of hospitalizations and the
use of other health care services (Dang, Dimmick
and Kelkar, 2009; Polisena et al., 2010a; Conway,
Inglis and Clark, 2014; Nakamura, Koga and Iseki,
2014).
However, there is a need for high-quality trials
(Chaudhry et al., 2007). Additionally, Grustam et al.
(2014) state that evidence from the scientific
literature related to home monitoring to support
congestive heart failure patients is still insufficient.
Also, more full economic analyses are needed to
reach a sound conclusion. This means that further
research is required in terms of comparisons of
home monitoring with usual care of patients with
congestive heart failure.
3.4 Chronic Obstructive Pulmonary
Disease
All the retrieved articles dealing with chronic
obstructive pulmonary disease analyse RCT primary
studies (Table 3). In particular, 3 of them considered
RCT as one of the inclusion criteria (Polisena et al.,
2010b; Pedone and Lelli, 2015; Lundell et al., 2015).
Home monitoring is supported by commercially
available devices to measure and transmit different
types of information (e.g. weight, temperature, blood
pressure, oxygen saturation, spirometry parameters,
symptoms, medication usage or steps in 6-minutes
walking distance). In some cases the automatic data
acquisition is complemented by clinical staff using
questionnaires in telephone interviews (Polisena et
al., 2010b; Pedone and Lelli, 2015). Video-
conference can also be used to provide feedback to
the patients (Lundell et al., 2015).
Table 3: Articles that focus chronic obstructive pulmonary
disease.
Study Technology
(*)
Polisena et
al., 2010b
Automatic patient data
transmission by means of
monitoring devices and standard
telephone calls
10/10
Bolton et al.
2011
Automatic patient data
transmission by means of
monitoring devices
6/2
Pedone et
al., 2015
Automatic patient data
transmission by means of
monitoring devices and standard
telephone calls
12/12
Lundell et
al., 2015
Automatic patient data
transmission by means of
monitoring devices and video-
conference
9/9
(*) Number of RCT included in the review / Number of
primary studies include in the review.
Technologies for Ageing in Place to Support Home Monitoring of Patients with Chronic Diseases
71

In what concerns the primary and secondary
outcomes, 3 studies (Polisena et al., 2010b; Bolton et
al. 2011; Pedone and Lelli, 2015) compare home
monitoring with usual care of patients with chronic
obstructive pulmonary disease, considering
mortality, admissions to hospital or other health care
utilization as primary outcomes. Secondary
outcomes include, among others, health related
quality of life, patient satisfaction, physical capacity
and dyspnea.
Home monitoring was found to reduce rates of
hospitalization and emergency department visits,
while the findings related to hospital bed days of
care varied between studies (Polisena et al., 2010b;
Pedone and Lelli, 2015). However, 1 study (Polisena
et al., 2010b) reports a greater mortality in a
telephone-support group compared with usual care.
Additionally, there is evidence that home monitoring
has a positive effect on physical capacity and
dyspnea (Lundell et al., 2015) and it is similar or
better than usual care in terms of quality of life and
patient satisfaction outcomes (Polisena et al.,
2010b).
The evidence systematized by the articles of the
category related to chronic obstructive pulmonary
disease does not allow drawing definite conclusions,
as the studies are small. The benefit of home
monitoring of patients with chronic obstructive
pulmonary disease is not yet proven and further
research is required before wide-scale
implementation be supported.
3.5 Hypertension
Finally, concerning patients with hypertension 1
article systematizes the results of 12 RCT using
devices with automated data transmission, and
video-conference.
The article reports improvements in the
proportion of participants with controlled blood
pressure compared to those who received usual care,
but the authors conclude that more interventions are
required and cost-effectiveness of the intervention
should also be assessed (Chandak and Joshi, 2015).
4 DISCUSSION
According to the findings of the systematic review
reported in the present article, diabetes, congestive
heart failure, chronic obstructive pulmonary disease
and hypertension are the most relevant chronic
diseases in terms of the use of technologies for
ageing in place to support home monitoring (i.e. the
first research question of the present study).
Type 1 and type 2 diabetes stand out from other
chronic conditions with a total of 20 studies, which
constitute 57.1% of the articles that were retrieved.
In order of relevance, the second chronic condition
is congestive heart failure (i.e. 28.6% of the articles
that were retrieved), which was followed by chronic
obstructive pulmonary disease (i.e. 11.4% of the
articles that were retrieved). Furthermore, one article
reporting a systematic review related to home
monitoring of patients with hypertension was also
included in the present systematic review.
Self-management of diabetes requires patient
adherence to best practice recommendations (e.g.
glucose monitoring, dietary management or physical
activity) (Or and Tao, 2014), congestive heart failure
has a high rate of hospital readmission (Bonow,
2005; Joe and Demiris, 2013) and key aspects of the
natural history of the chronic obstructive pulmonary
disease are episodes of acute exacerbations, which
are considered related to a faster disease
progression, presence of comorbidities, and worse
functional prognosis (Calvo, 2014). Therefore, the
results of the present systematic review are in line
with the current strong motivation for using
technological solutions as a way to monitor patients
with chronic diseases at home and to promote an
increasing compliance of self-care.
In terms of types, outcomes, and impacts of
technologies supporting home monitoring of patients
with chronic diseases (i.e. the second research
question of the study reported in the present article),
the results show that:
The technological solutions being used
include web-based applications, computer
assisted applications, smartphones, automatic
patient data transmission by means of
monitoring devices, video-conference and
standard telephone calls (Tables 1-3).
In general, the systematic reviews compare
home monitoring with usual care and the
primary outcomes depend of the type of the
patients being considered (e.g. glycaemia
control for patients with diabetes, patient’s
readmissions and mortality for patients with
congestive heart failure and patients with
chronic obstructive pulmonary disease, or
control of the blood pressure of patients with
hypertension).
Secondary outcomes are quite diverse and
include health related quality of life, weight,
depression, blood pressure, behaviour
outcomes, self-management, care knowledge,
medication adherence, patient-clinician
HEALTHINF 2017 - 10th International Conference on Health Informatics
72

communication, or structural outcomes related
to care coordination.
The analysis of the retrieved articles suggest
that home monitoring has positive effects with
a moderate to large improvements of different
outcomes when compared with usual care of
patients with diabetes, congestive heart
failure, chronic obstructive pulmonary disease
and hypertension (although in this case the
evidence is not as robust – only 1 article – as it
is in the other 3 chronic diseases). However,
some studies are not conclusive about this
positive impact and only report small
beneficial effects.
Despite a high level of technological innovation
and implementation, one of the findings is that
telephone calls are still an important channel for the
communication between patients and care providers.
Furthermore, it seems that important aspects are
neglected during the technological developments,
since there are reports of usability drawbacks as well
as reports of the need for more comprehensive
solutions, including provision of real-time feedback
and the integration of the electronic health records
systems being used by the care providers (El-Gayar
et al., 2013).
Therefore, the results show that not only
disruptive technological solutions have a key role
when dealing with home monitoring, since practical
and robust solutions are required, which means that
the integration and the interoperability of existing
technologies assume a great importance.
In general, the retrieved studies suggest positive
effects of home monitoring, but evidence provided
for the real benefit of home monitoring in some
aspects was not totally convincing. Further research,
including large scale RCT trials with consistent
primary and secondary outcomes, and robust
analysis about long-term sustainability, is required to
allow the full incorporation of home monitoring in
the clinical practice.
5 CONCLUSION
Considering the large amount of articles that report
studies related to home monitoring of patients with
chronic diseases, the authors decided to perform a
review of reviews and meta-analysis.
Although the authors tried to be as elaborate as
possible in methodological terms to guarantee that
the review selection and the data extraction were
rigorous, it should be acknowledged that this study
has limitations, namely the weaknesses inherent to
secondary analyses (i.e. review of reviews and meta-
analysis), the limitations related to the dependency
on the keywords and the databases selected, or the
assumption that the retrieved articles have a
homogeneous quality, which was not verified.
Despite these possible biases, the authors believe
that the systematically collected evidence
contributes to the understanding of the use of
technologies for ageing in place to support home
monitoring of patients with chronic diseases.
In parallel with this study, the authors have used
similar methods to analyse the role of technologies
for ageing in place to empower patients with chronic
diseases. However, due to several limitations, the
authors decide not to report the results in this article.
Therefore, these results will be the object of a future
publication. Also, as a future work, further studies
will be implemented, namely to analyse how
technologies for ageing in place are being used to
support daily activities and promote the participation
in social, economic, cultural, civil or spiritual
matters of older adults.
ACKNOWLEDGEMENTS
This work was partially supported by COMPETE -
Programa Operacional Competitividade e
Internacionalização (COMPETE 2020), Sistema de
Incentivos à Investigação e Desenvolvimento
Tecnológico (SI I&DT), under the project Social
Cooperation for Integrated Assisted Living
(SOCIAL).
REFERENCES
Arambepola, C., Ricci-Cabello, I., Manikavasagam, P.,
Roberts, N., French, D.P. and Farmer, A., 2016. The
impact of automated brief messages promoting
lifestyle changes delivered via mobile devices to
people with type 2 diabetes: a systematic literature
review and meta-analysis of controlled trials. Journal
of medical Internet research, 18(4).
Australian Institute of Health and Welfare, 2006. Chronic
Diseases and Associated Risk Factors in Australia,
2006. Australian Institute of Health and Welfare.
Baron, J., McBain, H. and Newman, S., 2012. The impact
of mobile monitoring technologies on glycosylated
hemoglobin in diabetes: a systematic review. Journal
of diabetes science and technology, 6(5), pp.1185-
1196.
Bolton, C.E., Waters, C.S., Peirce, S. and Elwyn, G.,
2011. Insufficient evidence of benefit: a systematic
Technologies for Ageing in Place to Support Home Monitoring of Patients with Chronic Diseases
73

review of home telemonitoring for COPD. Journal of
evaluation in clinical practice, 17(6), pp.1216-1222.
Bonow, R.O., Bennett, S., Casey, D.E., Ganiats, T.G.,
Hlatky, M.A., Konstam, M.A., Lambrew, C.T.,
Normand, S.L.T., Pina, I.L., Radford, M.J. and Smith,
A.L., 2005. ACC/AHA clinical performance measures
for adults with chronic heart failure: a report of the
American College of Cardiology/American Heart
Association task force on performance measures
(writing committee to develop heart failure clinical
performance measures) endorsed by the Heart Failure
Society of America. Journal of the American College
of Cardiology, 46(6), pp.1144-1178.
Calvo, G.S., Gómez-Suárez, C., Soriano, J.B., Zamora, E.,
Gónzalez-Gamarra, A., González-Béjar, M., Jordán,
A., Tadeo, E., Sebastián, A., Fernández, G. and
Ancochea, J., 2014. A home telehealth program for
patients with severe COPD: the PROMETE study.
Respiratory medicine, 108(3), pp.453-462.
Cassimatis, M. and Kavanagh, D.J., 2012. Effects of type
2 diabetes behavioural telehealth interventions on
glycaemic control and adherence: a systematic review.
Journal of telemedicine and telecare, 18(8), pp.447-
450.
Chandak, A. and Joshi, A., 2015. Self-management of
hypertension using technology enabled interventions
in primary care settings. Technology and Health Care,
23(2), pp.119-128.
Chaudhry, S.I., Phillips, C.O., Stewart, S.S., Riegel, B.,
Mattera, J.A., Jerant, A.F. and Krumholz, H.M., 2007.
Telemonitoring for patients with chronic heart failure:
a systematic review. Journal of cardiac failure, 13(1),
pp.56-62.
Ciere, Y., Cartwright, M. and Newman, S.P., 2012. A
systematic review of the mediating role of knowledge,
self-efficacy and self-care behaviour in telehealth
patients with heart failure. Journal of telemedicine and
telecare, 18(7), pp.384-391.
Clark, R.A., Inglis, S.C., McAlister, F.A., Cleland, J.G.
and Stewart, S., 2007. Telemonitoring or structured
telephone support programmes for patients with
chronic heart failure: systematic review and meta-
analysis. Bmj, 334(7600), p.942.
Connelly, K., Mokhtari, M. and Falk, T.H., 2014.
Approaches to Understanding the impact of
technologies for aging in place: a mini-review.
Gerontology, 60(3), pp.282-288.
Conway, A., Inglis, S.C. and Clark, R.A., 2014. Effective
technologies for noninvasive remote monitoring in
heart failure. Telemedicine and e-Health, 20(6),
pp.531-538.
Cruz, V.T., Pais, J., Bento, V., Mateus, C., Colunas, M.,
Alves, I., Coutinho, P. and Rocha, N.P., 2013. A
rehabilitation tool designed for intensive web-based
cognitive training: Description and usability study.
Journal of Medical Internet Research, 15 (12), p. e59.
Doi: 10.2196/resprot.2899.
Cruz, V.T., Pais, J., Alves, I., Ruano, L., Mateus, C.,
Barreto, R., Bento, V., Colunas, M., Rocha, N. and
Coutinho, P., 2014. Web-based cognitive training:
patient adherence and intensity of treatment in an
outpatient memory clinic. Journal of medical Internet
research, 16(5), p. e122. Doi: 10.2196/jmir.3377.
Dang, S., Dimmick, S. and Kelkar, G., 2009. Evaluating
the evidence base for the use of home telehealth
remote monitoring in elderly with heart failure.
Telemedicine and e-Health, 15(8), pp.783-796.
El-Gayar, O., Timsina, P., Nawar, N. and Eid, W., 2013. A
systematic review of IT for diabetes self-management:
are we there yet?. International journal of medical
informatics, 82(8), pp.637-652.
Eysenbach, G., 2008. Medicine 2.0: social networking,
collaboration, participation, apomediation, and
openness. Journal of medical Internet research, 10(3),
p.e22.
Frazetta, D., Willet, K. and Fairchild, R., 2012. A
systematic review of smartphone application use for
type 2 diabetic patients. Online Journal of Nursing
Informatics (OJNI), 16(3).
Garabedian, L.F., Ross-Degnan, D. and Wharam, J.F.,
2015. Mobile phone and smartphone technologies for
diabetes care and self-management. Current diabetes
reports, 15(12), pp.1-9.
Genet, N., Boerma, W.G., Kringos, D.S., Bouman, A.,
Francke, A.L., Fagerström, C., Melchiorre, M.G.,
Greco, C. and Devillé, W., 2011. Home care in
Europe: a systematic literature review. BMC health
services research, 11(1), p.1.
Grustam, A.S., Severens, J.L., van Nijnatten, J., Koymans,
R. and Vrijhoef, H.J., 2014. Cost-effectiveness of
telehealth interventions for chronic heart failure
patients: a literature review. International journal of
technology assessment in health care, 30(01), pp.59-
68.
Househ, M., 2014. The role of short messaging service in
supporting the delivery of healthcare: An umbrella
systematic review. Health informatics journal,
p.1460458214540908.
Huang, Z., Tao, H., Meng, Q. and Jing, L., 2015.
MANAGEMENT OF ENDOCRINE DISEASE:
Effects of telecare intervention on glycemic control in
type 2 diabetes: a systematic review and meta-analysis
of randomized controlled trials. European Journal of
Endocrinology, 172(3), pp.R93-R101.
Hunt, C.W., 2015. Technology and diabetes self-
management: An integrative review. World journal of
diabetes, 6(2), pp.225-233.
Jaana, M. and Paré, G., 2007. Home telemonitoring of
patients with diabetes: a systematic assessment of
observed effects. Journal of evaluation in clinical
practice, 13(2), pp.242-253.
Jackson, C.L., Bolen, S., Brancati, F.L., Batts?Turner,
M.L. and Gary, T.L., 2006. A systematic review of
interactive computer?assisted technology in diabetes
care. Journal of general internal medicine, 21(2),
pp.105-
Joe, J. and Demiris, G., 2013. Older adults and mobile
phones for health: A review. Journal of biomedical
informatics, 46(5), pp.947-954.
HEALTHINF 2017 - 10th International Conference on Health Informatics
74

Kickbusch, I. and Nutbeam, D., 1998. Health promotion
glossary. Geneva: World Health Organization.
Kitsiou, S., Paré, G. and Jaana, M., 2015. Effects of home
telemonitoring interventions on patients with chronic
heart failure: an overview of systematic reviews.
Journal of medical Internet research, 17(3), p.e63.
Koch, S., 2013. Achieving holistic health for the
individual through person-centered collaborative care
supported by informatics. Healthcare informatics
research, 19(1), pp.3-8.
Kvedar, J., Coye, M.J. and Everett, W., 2014. Connected
health: a review of technologies and strategies to
improve patient care with telemedicine and telehealth.
Health Affairs, 33(2), pp.194-199.
Lundell, S., Holmner, Å., Rehn, B., Nyberg, A. and
Wadell, K., 2015. Telehealthcare in COPD: a
systematic review and meta-analysis on physical
outcomes and dyspnea. Respiratory medicine, 109(1),
pp.11-26.
Martínez, A., Everss, E., Rojo-Álvarez, J.L., Figal, D.P.
and García-Alberola, A., 2006. A systematic review of
the literature on home monitoring for patients with
heart failure. Journal of telemedicine and telecare,
12(5), pp.234-241.
McBain, H., Shipley, M. and Newman, S., 2015. The
impact of self-monitoring in chronic illness on
healthcare utilisation: a systematic review of reviews.
BMC health services research, 15(1), p.1.
Moher, D., Liberati, A., Tetzlaff, J. and Altman, D.G.,
2009. Preferred reporting items for systematic reviews
and meta-analyses: the PRISMA statement. Annals of
internal medicine, 151(4), pp.264-269.
Mori, A.R., Mazzeo, M., Mercurio, G. and Verbicaro, R.,
2013. Holistic health: predicting our data future (from
inter-operability among systems to co-operability
among people). International journal of medical
informatics, 82(4), pp.e14-e28.
Nakamura, N., Koga, T. and Iseki, H., 2014. A meta-
analysis of remote patient monitoring for chronic heart
failure patients. Journal of telemedicine and telecare,
20(1), pp.11-17.
Or, C.K. and Tao, D., 2014. Does the use of consumer
health information technology improve outcomes in
the patient self-management of diabetes? A meta-
analysis and narrative review of randomized controlled
trials. International journal of medical informatics,
83(5), pp.320-329.
Ortiz, P.M.V., Felix, P.M. and Sosa, E.S.G., 2015. Text
messaging interventions to glycemic control in type 2
diabetes adults: systematic review/Mensajes de texto
para el control glucémico en adultos con diabetes tipo
2: revisión sistemática. Enfermería Global, 14(1),
p.445.
Pal, K., Eastwood, S.V., Michie, S., Farmer, A.J., Barnard,
M.L., Peacock, R., Wood, B., Inniss, J.D. and Murray,
E., 2013. Computerbased diabetes selfmanagement
interventions for adults with type 2 diabetes mellitus.
The Cochrane Library.
Pastalan, L.A., 1990. Aging in place: The role of housing
and social supports (Vol. 6, No. 1-2). Psychology
Press.
Pedone, C. and Lelli, D., 2015. Systematic review of
telemonitoring in COPD: an update. Pneumonol
Alergol Pol, 83, pp.476-8484.
Peterson, A. (2014). Improving Type 1 Diabetes
Management With Mobile Tools A Systematic
Review. Journal of diabetes science and technology,
8(4), 859-864.
Polisena, J., Tran, K., Cimon, K., Hutton, B., McGill, S.,
Palmer, K. and Scott, R.E., 2010. Home
telemonitoring for congestive heart failure: a
systematic review and meta-analysis. Journal of
Telemedicine and Telecare, 16(2), pp.68-76.
Polisena, J., Tran, K., Cimon, K., Hutton, B., McGill, S.,
Palmer, K. and Scott, R.E., 2010. Home telehealth for
chronic obstructive pulmonary disease: a systematic
review and meta-analysis. Journal of telemedicine and
telecare, 16(3), pp.120-127.
Queirós, A., Carvalho, S., Pavão, J. and da Rocha, N.P.,
2013. AAL Information based Services and Care
Integration. In HEALTHINF 2013 - Proceedings of
the International Conference on Health Informatics,
pp. 403-406.
Queirós, A., Silva, A., Alvarelhão, J., Rocha, N.P. and
Teixeira, A., 2015. Usability, accessibility and
ambient-assisted living: a systematic literature review.
Universal Access in the Information Society, 14(1),
pp.57-66. Doi: 10.1007/s10209-013-0328-x.
Ramadas, A., Quek, K.F., Chan, C.K.Y. and Oldenburg,
B., 2011. Web-based interventions for the
management of type 2 diabetes mellitus: a systematic
review of recent evidence. International Journal of
Medical Informatics, 80(6), pp.389-405.
Riazi, H., Larijani, B., Langarizadeh, M. and Shahmoradi,
L., 2015. Managing diabetes mellitus using
information technology: a systematic review. Journal
of Diabetes & Metabolic Disorders, 14(1), p.1.
Slev, V.N., Mistiaen, P., Pasman, H.R.W., Verdonck-de
Leeuw, I.M., van Uden-Kraan, C.F. and Francke, A.L.,
2016. Effects of eHealth for patients and informal
caregivers confronted with cancer: A meta-review.
International journal of medical informatics, 87,
pp.54-67.
Tao, D. and Or, C.K., 2013. Effects of self-management
health information technology on glycaemic control
for patients with diabetes: a meta-analysis of
randomized controlled trials. Journal of telemedicine
and telecare, 19(3), pp.133-143.
Teixeira, A., Pereira, C., e Silva, M.O., Alvarelhão, J.,
Silva, A.G., Cerqueira, M., Martins, A.I., Pacheco, O.,
Almeida, N., Oliveira, C. and Costa, R., 2013. New
telerehabilitation services for the elderly. I. Miranda,
M. Cruz-Cunha, Handbook of Research on ICTs and
Management Systems for Improving Efficiency in
Healthcare and Social Care, IGI Global, pp.109-132.
Doi: 10.4018/978-1-4666-3990-4.ch006.
Thrall, J.H., 2005. Prevalence and Costs of Chronic
Disease in a Health Care System Structured for
Technologies for Ageing in Place to Support Home Monitoring of Patients with Chronic Diseases
75

Treatment of Acute Illness 1. Radiology, 235(1), pp.9-
12.
Tildesley, H.D., Po, M.D. and Ross, S.A., 2015. Internet
Blood Glucose Monitoring Systems Provide Lasting
Glycemic Benefit in Type 1 and 2 Diabetes: A
Systematic Review. Medical Clinics of North
America, 99(1), pp.17-33.
van Vugt, M., de Wit, M., Cleijne, W.H. and Snoek, F.J.,
2013. Use of behavioral change techniques in web-
based self-management programs for type 2 diabetes
patients: systematic review. Journal of medical
Internet research, 15(12), p.e279.
Verhoeven, F., van Gemert-Pijnen, L., Dijkstra, K.,
Nijland, N., Seydel, E. and Steehouder, M., 2007. The
contribution of teleconsultation and videoconferencing
to diabetes care: a systematic literature review. J Med
Internet Res, 9(5), p.e37.
World Health Organization, 2002. Active ageing: a policy
framework: a contribution of the World Health
Organization to the Second United Nations World
Assembly on Ageing. Madrid (ES): World Health
Organization.
HEALTHINF 2017 - 10th International Conference on Health Informatics
76
