
Are Trustworthy Health Videos Reachable on YouTube?
A Study of YouTube Ranking of Diabetes Health Videos
Randi Karlsen
1
, Jos
´
e Enrique Borr
´
as Morell
1
and Vicente Traver Salcedo
2
1
Department of Computer Science, UiT The Arctic University of Norway, Tromsø, Norway
2
ITACA - Health and Wellbeing Technologies, Universidad Polit
`
ecnica de Val
`
encia, Valencia, Spain
Keywords:
Consumer Health Information, Information Retrieval, Social Networks, YouTube, Health Video Retrieval,
Ranking Evaluation, Diabetes, Personal Health.
Abstract:
While health consumers are increasingly searching health information on the Internet, information overload is
a serious obstacle for finding relevant and good-quality information among inaccurate, obsolete or incorrect
health information. While a lot of information exists, information from credible sources, such as hospitals and
health organisations, may be difficult to find. The aim of this study is to analyse ranking of diabetes health
videos on YouTube over a time period, to learn whether videos from credible sources are ranked sufficiently
high to be reachable to users. 19 diabetes-related queries were issued to YouTube each day over a 1.5-month
period, and in total 2584 videos from credible sources was detected and their ranking position tracked. We
found that only a small number of the tracked videos were in practice available to the user, as most videos
were given a persistent low ranking. Also, since ranking is fairly stable, users cannot expect to find many new
videos (from credible sources) when issuing a query multiple times. We conclude that new tools are needed
that enable health video retrieval based on requirements concerning not only relevance and popularity, but also
credibility of the sources and trustworthiness of the videos.
1 INTRODUCTION
Internet has, during the last years, become a major
source of health information (AlGhamdi and Moussa,
2012; Griffiths et al., 2012; Madathil et al., 2015).
Users are typically searching for information about
specific diseases or symptoms, treatment side effects,
second opinions, complementary or alternative medi-
cines, search for others with similar health concerns
and follow personal health experiences through blogs
(de Boer et al., 2007; Diaz et al., 2002; Fox, 2011b;
Powell et al., 2011). Also, online health information
is used, not only by health consumers to gain know-
ledge about some health issue, but also by physicians,
for clinical decision support and for education purpo-
ses (Hughes et al., 2009).
However, a general problem when searching the
Internet, is the information overload and difficulty of
finding relevant information satisfying the informa-
tion need. Adding to this problem, too many websites
have inaccurate, missing, obsolete, incorrect, biased
or misleading information, and it may be difficult to
distinguish between trustworthy and specious infor-
mation (Briones et al., 2012; Madathil et al., 2015;
Pant et al., 2012; Shabbir et al., 2013; Singh et al.,
2012; Steinberg et al., 2010). When people are re-
lying on online health information to take medical de-
cisions or handle their health issues, it is obviously of
highest importance that the health information provi-
ded to users is not only relevant, but also correct and
trustworthy. Existing search engines select and rank
information based on relevance to a search query and
popularity. Evaluating quality aspects, such as relia-
bility and validity of information, is currently left to
the user. Thus, the overwhelming amount of health
information together with the mixed quality, makes it
difficult for users to identify good-quality health in-
formation on the Internet, especially when users are
not familiar with new technologies or when their he-
alth knowledge is limited. Also, certification appro-
aches, such as the ethical HON code, are not solving
the issue (Diaz et al., 2002).
Health information on the Internet comes from
different sources, including hospitals, health orga-
nisations, government, educational institutions, for-
profit actors and private persons reporting on perso-
nal experiences with some disease. User studies have
shown that the credibility of an information source is
Karlsen R., Borrà ˛as Morell J. and Traver Salcedo V.
Are Trustworthy Health Videos Reachable on YouTube? - A Study of YouTube Ranking of Diabetes Health Videos.
DOI: 10.5220/0006114000170025
In Proceedings of the 10th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2017), pages 17-25
ISBN: 978-989-758-213-4
Copyright
c
2017 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
17

one of the most powerful factors affecting information
credibility (Freeman and Spyridakis, 2009). Users
are for example more likely to trust health informa-
tion published or authored by physicians or major he-
alth institutions than information provided by other
sources (Dutta-Bergman, 2003; Moturu et al., 2008;
Berm
´
udez-Tamayo et al., 2013). Such studies show
that users show greater interest in health information
published by professional sources, such as hospitals
and health organisations, since these are considered
more credible than the average health information on
the Internet.
In our study we focus on health information pro-
vided through videos on YouTube and investigate to
what extent health videos from professional sources,
such as hospitals and health organisations, are availa-
ble to the user. YouTube is today the most important
video-sharing website on the Internet (Cheng et al.,
2008). It has over a billion users (almost one-third of
all people on the Internet) and every day people watch
hundreds of millions of hours on YouTube and gene-
rate billions of views (YouTube, 2016). YouTube so-
cial media tools allow users to easily upload, view and
share videos, and enable interaction by letting users
rate videos and post comments.
YouTube is increasingly being used to share he-
alth information offered by a variety of sources (chan-
nels), including hospitals, organisations, government,
companies and private users (Bennett, 2011). Ho-
wever, it may be difficult to find videos from credi-
ble channels, since YouTube video ranking is known
to favour content from popular channels. This may
cause for instance hospital videos, where social inte-
raction through likes/dislikes and comments are not
so common, to appear low in the ranked list. Also,
YouTube ranking does not focus on trustworthiness,
and both misleading and incorrect videos may well
be popular and may therefore be given a high ranking
(Briones et al., 2012; Shabbir et al., 2013).
A considerable amount of literature has been pu-
blished on YouTube data analysis, such as studying
relations between video ratings and their comments
(Yee et al., 2009) or focusing on the social networ-
king aspect of YouTube and social features (Cheng
et al., 2008; Chelaru et al., 2012). Studies of You-
Tube performance have mainly focused on YouTube
in general, rather than on specific domains, such as
health. However, there have recently been some stu-
dies evaluating YouTube health video content with re-
spect to their quality of information for patient educa-
tion and professional training (Gabarron et al., 2013;
Topps et al., 2013). Such studies, focusing on diffe-
rent areas of medicine, include the work of (Briones
et al., 2012; Singh et al., 2012; Steinberg et al., 2010;
Butler et al., 2013; Schreiber et al., 2013; Murugiah
et al., 2011; Fat et al., 2011; Azer et al., 2013). In
these studies, reviewers evaluate the quality or con-
tent of selected videos, and assess their usefulness as
information source within their respective area.
This paper reports on a study where we tracked
diabetes health videos on YouTube over a period of
1.5 month, to gain knowledge on how videos from
professional channels are ranked on YouTube. The
study was intended to answer the following questions:
“Where are videos from hospitals and health organi-
sations ranked on YouTube?” “Are these videos ran-
ked in positions that make them reachable to users?”
To the best of our knowledge, there has previously not
been conducted a study where the availability of You-
Tube health videos has been tracked over time, as was
done in our work.
The structure of the paper is the following. The
next section presents the methodology used in our
study. Section 3 presents the results of the work,
while findings are discussed in Section 4. Section 5
concludes.
2 METHOD
This study is based on health videos obtained from
YouTube through textual search queries on diabetes-
related issues. We set up a test environment, where 19
diabetes-related queries were issued to YouTube each
day over a period of 1.5 months, from March until
April 2013. During this period, we daily collected
the top 500 YouTube results for each query. Videos
from white-listed (presumably credible) sources were
identified and tracked during each day of the study,
and their ranking position registered.
We implemented a system that for each day au-
tomatically issued the 19 queries and extracted infor-
mation about the top 500 YouTube results. In addition
to ranking position, we collected information such as
video name and identifier, channel identifier, number
of likes, dislikes and comments to the video. All 19
queries included the term “diabetes” and were focu-
sed towards different aspects concerning the disease.
We used queries such as “diabetes a1”, “diabetes glu-
cose”, “diabetes hyperglycemia” and “diabetes lada”,
and issued them as regular search queries on the You-
Tube home page using an anonymous profile (to avoid
any bias) and with language option set to English.
Video ranking was obtained by parsing the html of
the result page, while video and channel information
were collected through YouTube API version 2.0. All
search queries can be seen in Table 1.
Through our study of YouTube health videos, we
HEALTHINF 2017 - 10th International Conference on Health Informatics
18

Table 1: List of You Tube search queries.
diabetes type 1 diabetes hyperglycemia diabetes insulin
diabetes type 2 diabetes hypoglycemia diabetes injection
diabetes a1c diabetes complications diabetes glucose
diabetes food diabetes retinopathy diabetes mellitus
diabetes diet diabetes ketoacidosis diabetes education
diabetes obese diabetes insulin pump
diabetes lada diabetes monitoring
identified a number of (assumed) credible health vi-
deo sources, such as hospitals and health organisa-
tions. We organised these channels into a hospital
white-list and a health organisations white-list, con-
taining channel identifiers for hospitals and health or-
ganisations respectively. In the light of user-interests
in peer-to-peer healthcare (Ziebland and Herxheimer,
2008; Fox, 2011a), we also generated a third white-
list of channels, which includes users that are active
and predominantly publishing diabetes videos. Our
white-lists contained a total of 699 channels, where
651 were hospitals, 30 were organisations and 18
were active users. We used the Health Care Social
Media List started by Ed Bennett (Bennett, 2011) as
an initial white-list, and expanded with more channels
that we identified during our studies (Karlsen et al.,
2013; Morell et al., 2012).
3 RESULTS
Using the 19 search terms shown in Table 1, we trac-
ked the rank position of a total of 2584 YouTube he-
alth videos from white-listed channels during the test
period. The videos were uploaded from 73 hospital
channels, 30 organisation channels and 18 user chan-
nels. Among these, 2372 videos were uploaded to
YouTube before the study began, whereas 212 videos
were uploaded while the study was performed.
For each day of the study, our system detected a
number of new videos from white-listed channels (for
which tracking started and continued to the end of the
study). The number of new videos was large in the
first days of the study, and after some days stabilised
at around 10 new videos each day.
3.1 Ranking of Videos from
White-listed Channels
A goal of this study is to identify the number of vi-
deos from hospitals, health organisations and active
users that are in practice available to users. When a
YouTube search returns over 600.000 ranked videos
(which is the case for the “diabetes type 1” search), it
is obvious that the lowest ranked videos are not very
available. A question is: “How far down in the ran-
ked list of videos is a user willing to browse in order
to find a relevant video?” The answer may to some
extent be a matter of how patient the user is, but tes-
ting several hundred videos are beyond what can be
expected from an average user.
To characterise videos w.r.t availability, we have
grouped the tracked videos using ranking position
intervals that were chosen based on our perception
of how available videos in the different groups are.
We consider videos ranked in position 1-40 as highly
available, position 41-100 as available, position 101-
200 as not very available and position 201-500 as al-
most unavailable. In this work, we assume that videos
ranked lower than position 500, are in practice una-
vailable, and we have therefore tracked only videos
appearing in the top-500 ranking.
To learn where videos from hospitals, health or-
ganisations and active users were ranked, we exami-
ned, for each day, the rank positions for all videos
from our white lists, and determined the number of
videos that were ranked in position intervals (1-40),
(41-100), (101-200), and (201-500). Based on this
study, we found that only a small number of videos
from white-listed channels were in practice available
to the user. When examining the top-40 ranked vi-
deos, we found that on average, only 3.2% were from
hospitals, 10.4% from health organisations and 3.6%
from active users. This means that we on average
will retrieve approximately 7 videos from white-listed
channels among the top-40 ranked videos. In the next
position interval (41-100), the average number of vi-
deos from white-listed channels will be approxima-
tely 6. The results for all rank intervals are seen in
Figure 1. The numbers for the top-500 videos (not gi-
ven in Figure 1) were 2.3% from hospitals, 6.4% from
health organisations and 1.8% from active users.
Figure 1: Average number (in percentage) of videos from
white-listed channels within different rank intervals.
As our white-lists obviously do not contain every
hospital or health organisation available, we took, for
all 19 queries, the top-100 YouTube hits from one
Are Trustworthy Health Videos Reachable on YouTube? - A Study of YouTube Ranking of Diabetes Health Videos
19
Table 2: Classification of the tracked videos from white-listed channels, grouped according to their most frequent ranking
position during the test period. The number of videos in each rank-position group are given (percentage between parentheses).
Group A Group B Group C Group D Group E Total no. of
videos videos videos videos videos videos
(pos. 1-40) (pos. 41-100) (pos. 101-200) (pos. 201-500) (pos. > 500)
Hospitals 26 (1.0%) 27 (1.1%) 52 (2.0%) 99 (3.8%) 334 (12.9%) 538 (20.8%)
Organizations 80 (3.1%) 89 (3.4%) 127 (4.9%) 279(10.8%) 1017 (39.4%) 1592(61.6%)
Active users 30 (1.2%) 33 (1.3%) 33 (1.3%) 55 (2.1%) 303 (11.7%) 454 (17.6%)
Total 136(5.3%) 149(5.8%) 212(8.2%) 433(16.7%) 1654(64.0%) 2584
day’s search and manually checked the channel of
each video. We found 15 new videos from hospitals
not included in the white-list. This addition repre-
sents a modest 0.8% (of the 1900 videos), and does
not significantly improve the amount of hospital vi-
deos given a high ranking.
3.2 Changes in Ranking Position
To investigate variations in video ranking, we first
classified the tracked videos into five rank-position
groups (Group A-E) according to their most frequent
rank position during the test period. Occasional chan-
ges in ranking position were registered by counting
the number of videos from each group that one or
more days had a ranking position associated with a
different group. We also calculated mean position and
standard deviation for videos that were ranked within
a top-500 position the whole period.
Among the 2584 videos from white-listed chan-
nels, we found 136 videos (5.3%) (26 hospital, 80 or-
ganisation and 30 user videos) that most frequently
appeared in the top-40 results, while 1654 videos
(64%) only occasionally appeared among the top-500
results. These were classified as Group A and Group
E videos, respectively. Table 2 shows the number of
videos within each of the five rank-position groups.
Occasional change in ranking is presented in Ta-
ble 3, showing the proportion of videos classified as
Group A-E that occasionally (i.e. one or more days)
appeared in a different rank-position interval. For ex-
ample, 38.2% of Group A videos appeared occasio-
nally in position 41-100, while 14% occasionally ap-
peared in position 101-200. We found that only a
small proportion of videos from Group C, D and E
were occasionally given a high-ranked position within
1 - 40 (11.8%, 2.5% and 4.4% respectively).
These results indicate that most of the videos ap-
pearing in low rank positions, are stuck in low posi-
tions, and will consequently remain (almost) out of
reach to the user.
Mean position and standard deviation (SD) were
calculated for the 175 videos that were ranked within
top-500 the whole test period. Table 4 shows mean
Table 3: Proportion of Group A-E videos (classified accor-
ding to their most frequent ranking position) that occasio-
nally changed ranking position to a different position inter-
val.
Group Group Group Group Group
A B C D E
Occ. pos
1-40 - 35.6% 11.8% 2.5% 4.4%
Occ. pos
41-100 38.2% - 48.6% 11.3% 9.6%
Occ. pos
101-200 14.0% 54.4% - 39.7% 19.6%
Occ. pos
201-500 6.6% 26.8% 59.0% - 81.4%
Occ. pos
> 500 27.9% 63.1% 76.9% 82.7% -
position and standard deviation for videos, grouped
according to their most frequent rank position (i.e.
rank-position group).
Table 4: Mean position and standard deviation for videos
in different rank-position groups. Including the 175 videos
that were ranked within top-500 the whole test period.
No. of Mean Standard
videos position deviation
Group A 71 15.5 7.0
Group B 43 71.0 20.9
Group C 37 145.9 38.2
Group D 24 272.3 48.0
We found that the highest ranked videos (Group
A) had the lowest standard deviation, i.e. 7.0. These
videos seemed to be established in a top-ranked posi-
tion, and had in general less variation in rank-position
than videos from other groups. In fact, stability in
rank position seemed to be the case for all groups,
even though the standard deviation for Group B, C
and D is higher.
SD-values indicate that changes in rank position
in general do not make Group D videos more acces-
sible to users, while Group C and B videos may oc-
casionally be given a more accessible ranking. As an
example, take Group B videos having a mean position
of 71 and an SD value of 20.9. This means that most
HEALTHINF 2017 - 10th International Conference on Health Informatics
20
videos (about 68%, assuming a normal distribution)
were ranked within position 50-92. Approximately
15% of the videos occasionally had a position within
top-40, while approximately 15% were occasionally
not included in the top-100. For Group C videos, less
than 0.5% of the videos would occasionally have a
position within the top-40, while approximately 10%
would occasionally have a position within top-100.
The rank stability observed through these num-
bers, indicates that highly ranked videos remain avai-
lable to users, while low ranked videos will almost
always remain out of reach for the user.
3.3 Relevance of Videos
One could suspect that videos given a low-ranked po-
sition were not relevant to the query. To investigate
this, we selected two queries (“diabetes hyperglyce-
mia” and “diabetes retinopathy”) and determined re-
levance of each tracked video by manually comparing
keywords in the query to video title and description,
and by watching the video to compare video content
to query.
Over the test period, the system tracked 130 vi-
deos for the “diabetes hyperglycemia” query and 64
videos for the “diabetes retinopathy” query. Table
5 shows the number of videos that were i) relevant
to the query, ii) relevant to diabetes in general and
iii) not relevant to diabetes. For example, for Group
E videos of the “diabetes hyperglycemia” query, we
found that 50% were relevant to the query, an addi-
tional 47% were relevant to diabetes, while only 3%
were not relevant to diabetes. For the “diabetes retino-
pathy” query, 55% of Group E videos were relevant to
the query, an additional 18% were relevant to diabe-
tes, while 27% were not relevant. For Group A and B
videos (of both queries), every video was relevant to
the query. In conclusion, we found that a large num-
ber of low-ranked videos were relevant to the query,
implying that lack of relevance could not be the rea-
son for their low ranking.
3.4 Video Properties
To detect possible correlations between video proper-
ties and ranking position, we compared video title and
query terms, investigated social interaction by coun-
ting for each video the number of likes, dislikes, com-
ments and views, and subsequently compared against
the video’s ranking position.
Having a match between query terms and video
title is obviously an important criterion for conside-
ring the video relevant to the query. We found for
Group A videos that 88% (120 of 136 videos) had a
Table 5: The number of videos relevant to i) the search
query and ii) diabetes in general, for the two queries “di-
abetes hyperglycemia” and “diabetes retinopathy”.
Rank relevant Diabetes Diabetes
position to hyperglicemia retinopathy
Group A query 100% 100%
videos diabetes - -
Group B query 100% 100%
videos diabetes - -
Group C query 45% 100%
videos diabetes 55% -
query 41% 72%
Group D diabetes 55% 11%
videos not relev 4% 17%
query 50% 55%
Group E diabetes 47% 18%
videos not relev 3% 27%
perfect match between video title and query (meaning
that all terms in the query were found in the video
title). The proportion of videos with a perfect query-
title match was lower in the other groups, but there
were still a large number of lower ranked videos that
had a perfect query-title match. This shows that such
a match is not sufficient for a high-ranked position.
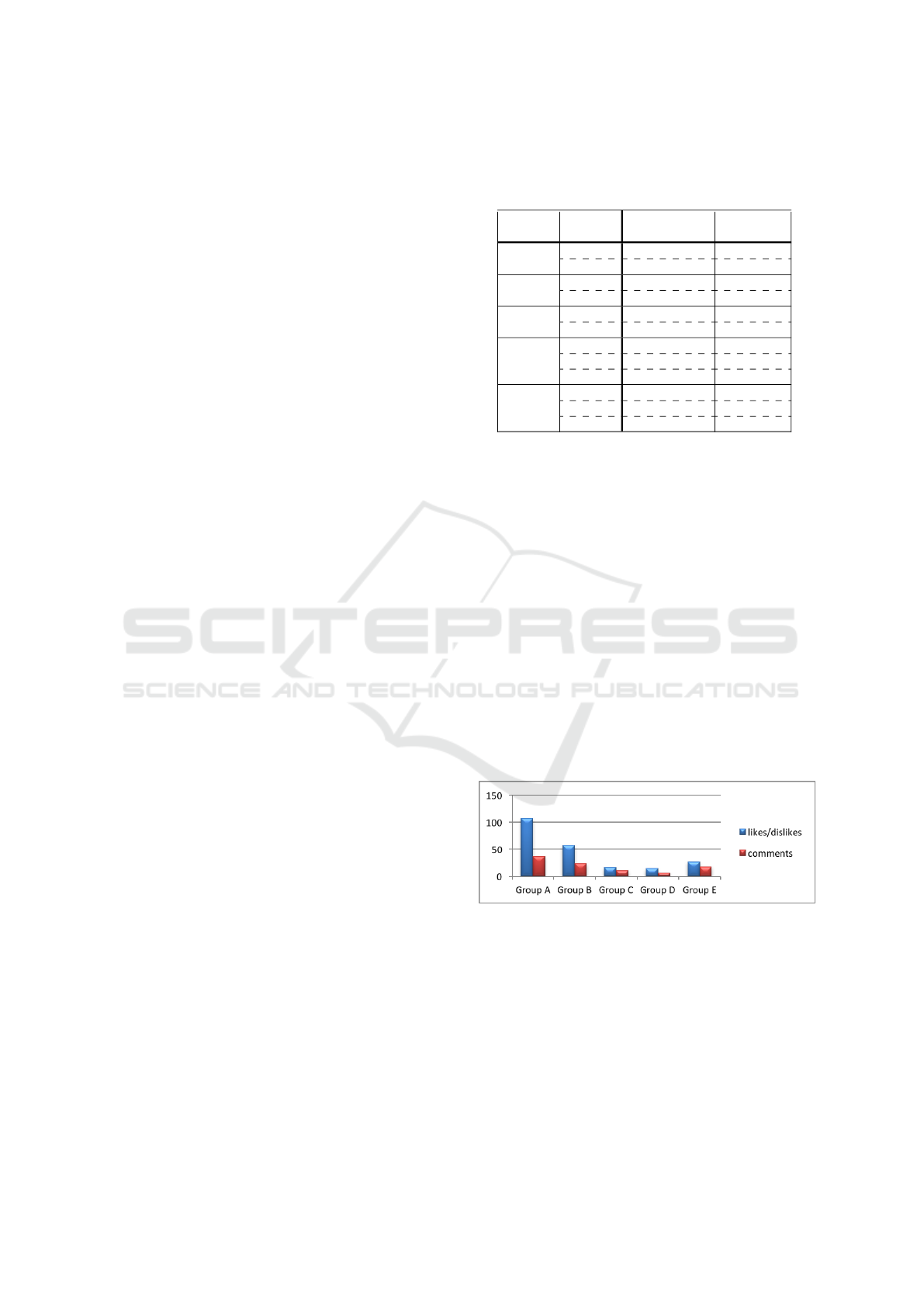
The average number of likes/dislikes and com-
ments for Group A-E videos are displayed in Figure 2.
The general trend was that the highest ranked videos
had the highest number of social interactions. This
coincides well with previous studies, which found
that very few videos get the users’ attention. This
can be explained through the Yule process (or rich-
get-richer principle), as the videos that appear in the
first page are more likely to be viewed and interacted
(Chelaru et al., 2012; Cha et al., 2009).
Figure 2: Average number of likes/dislikes and comments
on videos.
However, when studying individual videos, we
observed huge differences in the number of user in-
teractions. We found for example that a number of vi-
deos without likes/dislikes and comments were highly
ranked despite the lack of user activity. Table 6 shows
the percentage of videos, within each rank-position
group, that had zero likes, dislikes and comments. We
see for example that 20% of Group A videos had no
such social interaction.
Are Trustworthy Health Videos Reachable on YouTube? - A Study of YouTube Ranking of Diabetes Health Videos
21
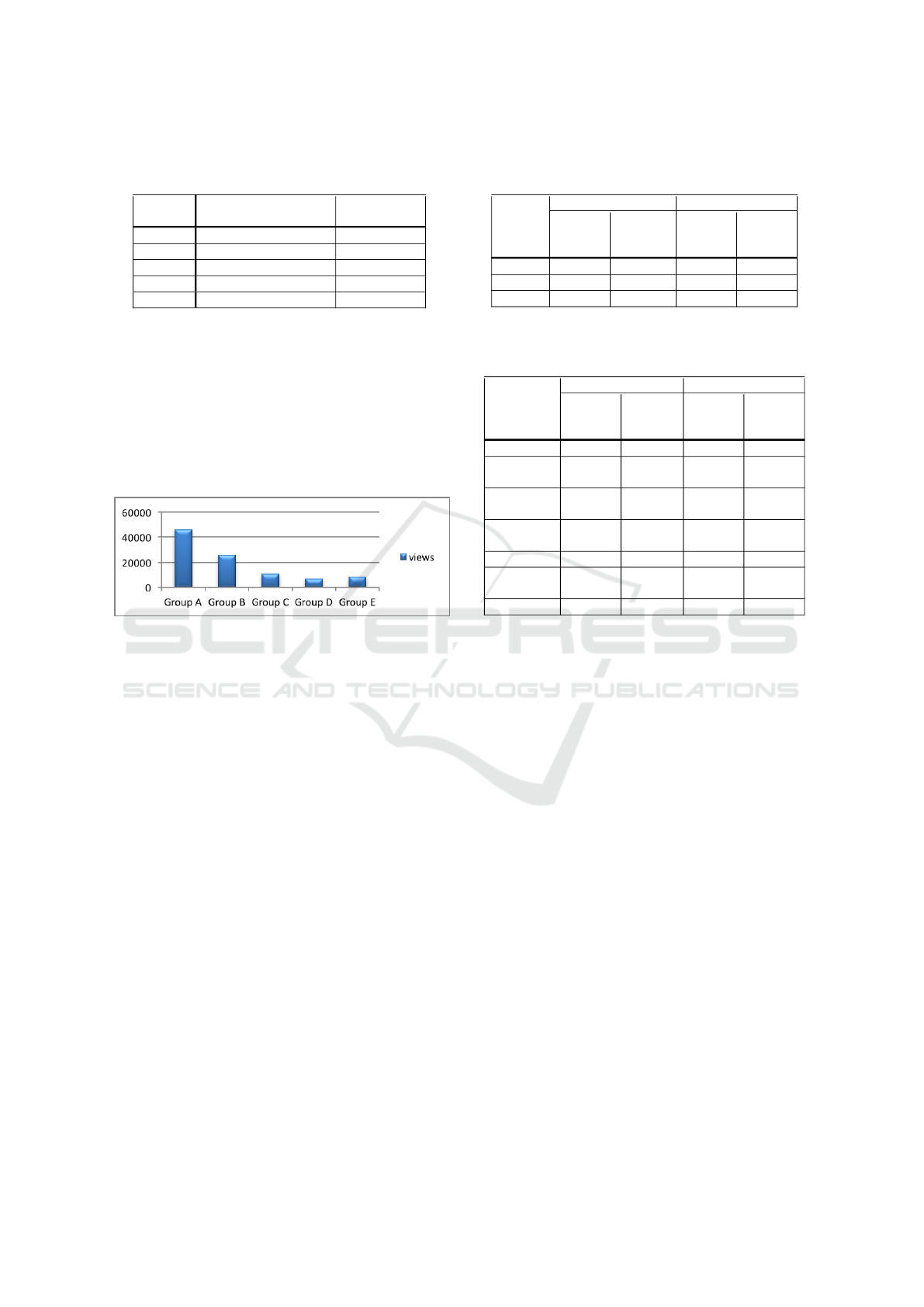
Table 6: Number of videos without user interaction through
likes/dislikes and comments.
Videos tracked All videos
all period (175 videos) (2584 videos)
Group A 21% 20%
Group B 35% 29%
Group C 43% 33%
Group D 33% 39%
Group E - 28%
When examining the number of views for indi-
vidual videos, we found a close correlation between
views and ranking (see Figure 3). This seems obvious
since users can easily find and access highly ranked
videos, which then get a higher number of views com-
pared to low ranked videos. However, there were also
a few exceptions. For instance, one Group A video
had only 18 views, zero likes, dislikes and comments.
Figure 3: Average number of times a video has been vie-
wed.
3.5 Videos From Non-white-listed
Channels
To get an impression of the type of videos not tracked
in our study, we also examined properties of videos
published by non-white-listed channels. Because of
the large number of videos, we restricted this investi-
gation to the top-50 results of two queries: “diabetes
type 1” and “diabetes injection”. For all top-50 vi-
deos we manually examined relevance to query and
channel type.
Relevance and channel type for the examined vi-
deos are shown in Table 7 and Table 8, respectively.
Videos from both white-listed (WL) and non-white-
listed channels are included in the tables. Among
the non-white-listed videos, most came from private
users (47 videos), while only 3 videos were from he-
alth organisations/centres. We further observed that
white-listed channels had the highest proportion of re-
levant videos.
Table 7: Relevance of videos published by non-white-listed
and white-listed channels.
Diabetes type 1 Diabetes injection
Relevant non-WL- WL- non-WL- WL-
to channels channels channels channels
35 videos 13 videos 38 videos 11 videos
query 32 (91%) 13 (100%) 19 (50%) 10 (91%)
diabetes 3 (9%) 0 9 (24%) 1 (9%)
not relev. 0 0 10 (26%) 0
Table 8: Channels of videos published by non-white-listed
and white-listed channels.
Diabetes type 1 Diabetes injection
non-WL- WL- non-WL- WL-
channels channels channels channels
35 videos 13 videos 38 videos 11 videos
Hospital 0 3 (23%) 0 0
Health
organization 1 (3%) 5 (38.5%) 1 (2%) 8 (73%)
Active
users 0 5 (38.5%) 0 3 (27%)
Health
center 1 (3%) - 0 -
Company 8 (23%) - 5 (13%) -
Private
users 24 (68%) - 23 (61%) -
Others 1 (3%) - 9 (24%) -
4 DISCUSSION
The goal of this study was to identify the number of
videos from hospitals, health organisations and active
user channels that are in practice available to users.
On the positive side, the study shows that for each
query, videos from white-listed channels are in fact
available among the top-500 ranked videos. A pro-
blem, however, is that these videos represent a small
proportion of the total number of retrieved videos, and
that many of them are found in low ranked positions
that make them in practice beyond reach for the user
issuing the query. Thus, precision for videos from
white-listed channels is not very good. Among the
top-100 ranked videos for a diabetes related query,
one can on average expect 15% to be from white-
listed channels (2.8% from hospitals, 8.9% from he-
alth organisations and 3.3% from active users).
Of the 2584 tracked videos, 64% were most fre-
quently ranked in a position lower than 500, only oc-
casionally appearing within the top-500 results. This
shows that many relevant videos from credible chan-
nels are in practice unreachable for users. Also, stan-
dard deviation values and observed ranking variations
for individual videos show that the ranking of videos
is fairly stable. This implies that only a small per-
HEALTHINF 2017 - 10th International Conference on Health Informatics
22

centage of low ranked videos improved their ranking
position sufficiently to be available to users and that
users hardly obtain any new videos (from white-listed
channels) by issuing a query multiple times. On the
other hand, ranking stability also guarantees that top-
ranked videos from white-listed channels are availa-
ble to users over a period of time. This benefits new
users that will have access to a few popular and poten-
tially good quality health videos from credible chan-
nels.
One conclusion from our study is therefore that re-
levant diabetes-related health videos are available on
YouTube, but too few are given a ranking that make
them reachable for the user.
The YouTube ranking algorithm is based on video
popularity among users. Previously the algorithm was
based on view count of the video, while the current
version (since 2012) is based on Watch Time, which
is the amount of time on aggregate that viewers watch
a video (Robertson, 2014). Even though Watch Time
is a better measure of success for a video (since it re-
wards engaging videos that keep viewers watching),
it still requires videos to be available to users in order
to get sufficient attention and improve Watch Time.
Also, there is no guarantee that an engaging, much
watched video is trustworthy with respect to the he-
alth information it provides.
In our study, the investigation of correlation bet-
ween ranking position and user attention in the form
of social interactions, gave mixed results. There were
on average a higher number of social interactions (i.e.
likes/dislikes, comments and views) for the highest
ranked videos, but we also saw many examples of vi-
deos that had a high-ranked position with no social
interaction and very few views.
A critical factor in identifying relevant videos ba-
sed on a textual query, is the accuracy of the metadata
with respect to video content. When examining the
correlation between video title and query terms, we
found that a majority (88%) of the highest ranked vi-
deos (Group A videos), but also a large number of
low ranked videos, had a perfect match between vi-
deo title and query terms. However, by inspection,
we also found many video descriptions that were very
short and of such a general nature that they did not
describe the video content. Video titles were also in
many cases inaccurate with respect to video content.
An implication of these findings is that video pu-
blishers should make an effort in providing precise
textual description of videos, where video title and
description matches the video content as accurately
as possible. This is a simple way of improving the
likelihood for being selected as relevant and possi-
bly ranked sufficiently high to be reachable. Allo-
wing and even encouraging social interaction on vi-
deos may also help visibility of the video.
However, an accurate video title/description is
only a step in the right direction for improving video
rank position and precision. We believe there is a need
for new video retrieval tools that not only focus on re-
levance and popularity as it is done today, but also re-
trieves health information based on requirements for
credibility of the sources and trustworthiness of the
videos. This provides topics for future research.
Some limitations to our work should be noted.
Firstly, even though our white-lists of hospitals and
health organisations include a large number of chan-
nels, they cannot include every hospital and health
organisation available. The focus was not to track
every relevant and trustworthy video in the result set
from YouTube, but rather to track videos from speci-
fic channel types that are assumed to be of interest to
health consumers. Also, it should be noted that the
quality of each video was not assessed in this study.
We base the study on the assumption that videos from
hospitals, health organisations and also active users
are of interest and therefore worthwhile investigating.
We are fully aware that videos from other channels
(not tracked in our study) may provide useful and
trustworthy information. Furthermore, for each query
we only examined the top-500 ranked videos from
YouTube. When some queries return over 600.000
videos, this is a small number. However, we believe
that a position over 500 is not significant in terms of
availability to users.
5 CONCLUSION
To gain knowledge about how health videos are ran-
ked on YouTube, we have tracked diabetes health
videos on YouTube every day over a period of 1.5
month. We focused on videos published by credible
channels, such as hospitals, health organisations and
users actively publishing diabetes-related videos. Our
findings show that most videos from these channels
are given a persistent low ranking that makes them
in practice unavailable to users. Additionally, since
ranking position of videos is fairly stable, users re-
ceive the same videos over and over again if issuing
a query multiple times. Thus, users may find it dif-
ficult to obtain new information from YouTube. A
conclusion from this work is that research is needed
to provide users with new tools that enable health vi-
deo retrieval based on requirements concerning not
only relevance and popularity, but also credibility of
the sources and trustworthiness of the videos. Me-
chanisms for alternative ranking or less stable ranking
Are Trustworthy Health Videos Reachable on YouTube? - A Study of YouTube Ranking of Diabetes Health Videos
23

could also be useful for making a larger number of re-
levant videos available to the user.
ACKNOWLEDGEMENTS
The authors appreciate support from UiT The Arctic
University of Troms through funding from Troms Re-
search Foundation, and the important contributions of
the ITACA-TSB Universitat Polit
`
ecnica de Val
`
encia
group.
REFERENCES
AlGhamdi, K. M. and Moussa, N. A. (2012). Internet
use by the public to search for health-related infor-
mation. International journal of medical informatics,
81(6):363–373.
Azer, S. A., AlGrain, H. A., AlKhelaif, R. A., and AlEs-
haiwi, S. M. (2013). Evaluation of the educational va-
lue of youtube videos about physical examination of
the cardiovascular and respiratory systems. Journal of
medical Internet research, 15(11):e241.
Bennett, E. (2011). Social media and hospitals: From
trendy to essential. Futurescan 2001: Healthcare
Trends and Implications 2011-2016, pages 43–48.
Berm
´
udez-Tamayo, C., Alba-Ruiz, R., Jim
´
enez-Pernett,
J., Garc
´
ıa Guti
´
errez, J.-F., Traver-Salcedo, V., and
Yubraham-S
´
anchez, D. (2013). Use of social me-
dia by spanish hospitals: perceptions, difficulties,
and success factors. Telemedicine and e-Health,
19(2):137–145.
Briones, R., Nan, X., Madden, K., and Waks, L. (2012).
When vaccines go viral: an analysis of hpv vac-
cine coverage on youtube. Health communication,
27(5):478–485.
Butler, D. P., Perry, F., Shah, Z., and Leon-Villapalos, J.
(2013). The quality of video information on burn first
aid available on youtube. Burns, 39(5):856–859.
Cha, M., Kwak, H., Rodriguez, P., Ahn, Y.-Y., and Moon,
S. (2009). Analyzing the video popularity charac-
teristics of large-scale user generated content sys-
tems. IEEE/ACM Transactions on Networking (TON),
17(5):1357–1370.
Chelaru, S. V., Orellana-Rodriguez, C., and Altingovde,
I. S. (2012). Can social features help learning to
rank youtube videos? In International Conference
on Web Information Systems Engineering, pages 552–
566. Springer.
Cheng, X., Dale, C., and Liu, J. (2008). Statistics and so-
cial network of youtube videos. In Quality of Service,
2008. IWQoS 2008. 16th International Workshop on,
pages 229–238. IEEE.
de Boer, M. J., Versteegen, G. J., and van Wijhe, M.
(2007). Patients use of the internet for pain-related
medical information. Patient education and counse-
ling, 68(1):86–97.
Diaz, J. A., Griffith, R. A., Ng, J. J., Reinert, S. E., Fried-
mann, P. D., and Moulton, A. W. (2002). Patients’
use of the internet for medical information. Journal of
general internal medicine, 17(3):180–185.
Dutta-Bergman, M. (2003). Trusted online sources of he-
alth information: differences in demographics, health
beliefs, and health-information orientation. Journal of
medical Internet research, 5(3):e21.
Fat, M. J. L., Doja, A., Barrowman, N., and Sell, E. (2011).
Youtube videos as a teaching tool and patient resource
for infantile spasms. Journal of Child Neurology,
26(7):804–809.
Fox, S. (2011a). Peer-to-peer healthcare. Pew Internet &
American Life Project.
Fox, S. (2011b). The social life of health information, 2011.
Pew Internet & American Life Project Washington,
DC.
Freeman, K. S. and Spyridakis, J. H. (2009). Effect of con-
tact information on the credibility of online health in-
formation. IEEE Transactions on Professional Com-
munication, 52(2):152–166.
Gabarron, E., Fernandez-Luque, L., Armayones, M., and
Lau, A. Y. (2013). Identifying measures used for as-
sessing quality of youtube videos with patient health
information: a review of current literature. Interactive
Journal of Medical Research, 2(1):e6.
Griffiths, F., Cave, J., Boardman, F., Ren, J., Pawlikowska,
T., Ball, R., Clarke, A., and Cohen, A. (2012). Social
networks–the future for health care delivery. Social
science & medicine, 75(12):2233–2241.
Hughes, B., Joshi, I., Lemonde, H., and Wareham, J. (2009).
Junior physician’s use of web 2.0 for information see-
king and medical education: a qualitative study. Inter-
national journal of medical informatics, 78(10):645–
655.
Karlsen, R., Morell, J. E. B., Fern
´
andez-Luque, L., and Sal-
cedo, V. T. (2013). A domain-based approach for re-
trieving trustworthy health videos from youtube. In
MedInfo, page 1008.
Madathil, K. C., Rivera-Rodriguez, A. J., Greenstein, J. S.,
and Gramopadhye, A. K. (2015). Healthcare informa-
tion on youtube: a systematic review. Health informa-
tics journal, 21(3):173–194.
Morell, J. E. B., Karlsen, R., Salcedo, V. T., and Luque,
L. F. (2012). Analysis of hospital youtube videos as
health reliable sources. IVWorkshop on on Technology
for Healthcare and Healthy Lifestyle.
Moturu, S. T., Liu, H., and Johnson, W. G. (2008). Trust
evaluation in health information on the world wide
web. In 2008 30th Annual International Conference
of the IEEE Engineering in Medicine and Biology So-
ciety, pages 1525–1528. IEEE.
Murugiah, K., Vallakati, A., Rajput, K., Sood, A., and
Challa, N. R. (2011). Youtube as a source of informa-
tion on cardiopulmonary resuscitation. Resuscitation,
82(3):332–334.
Pant, S., Deshmukh, A., Murugiah, K., Kumar, G., Sa-
chdeva, R., and Mehta, J. L. (2012). Assessing the
credibility of the youtube approach to health informa-
HEALTHINF 2017 - 10th International Conference on Health Informatics
24

tion on acute myocardial infarction. Clinical cardio-
logy, 35(5):281–285.
Powell, J., Inglis, N., Ronnie, J., and Large, S. (2011). The
characteristics and motivations of online health infor-
mation seekers: cross-sectional survey and qualitative
interview study. Journal of Medical Internet Rese-
arch, 13(1):e20.
Robertson, M. R. (2014). Watch time: A guide to youtu-
bes top search ranking factor. Internet: http://www.
reelseo. com/youtube-watch-time/, Einsicht, 8:2015.
Schreiber, J. J., Warren, R. F., Hotchkiss, R. N., and Da-
luiski, A. (2013). An online video investigation into
the mechanism of elbow dislocation. The Journal of
hand surgery, 38(3):488–494.
Shabbir, S. A., Fernandez-Luque, L., Jian, W.-S., Li, Y.-C.,
Crain, S., Hsu, M. H., Wang, Y. C., Khandregzen, D.,
Chuluunbaatar, E., Nguyen, P. A., et al. (2013). Mis-
leading health-related information promoted through
video-based social media. Journal of Medical Inter-
net Research, 15(2).
Singh, A. G., Singh, S., and Singh, P. P. (2012). Youtube
for information on rheumatoid arthritisa wakeup call?
The Journal of rheumatology, 39(5):899–903.
Steinberg, P. L., Wason, S., Stern, J. M., Deters, L., Ko-
wal, B., and Seigne, J. (2010). Youtube as source of
prostate cancer information. Urology, 75(3):619–622.
Topps, D., Helmer, J., and Ellaway, R. (2013). Youtube as a
platform for publishing clinical skills training videos.
Academic Medicine, 88(2):192–197.
Yee, W. G., Yates, A., Liu, S., and Frieder, O. (2009). Are
web user comments useful for search. Proc. LSDS-IR,
pages 63–70.
YouTube (2016). Statistics. https://www.youtube.com/yt/
press/statistics.html, Accessed: 2016-09-26.
Ziebland, S. and Herxheimer, A. (2008). How patients ex-
periences contribute to decision making: illustrations
from dipex (personal experiences of health and ill-
ness). Journal of nursing management, 16(4):433–
439.
Are Trustworthy Health Videos Reachable on YouTube? - A Study of YouTube Ranking of Diabetes Health Videos
25
