
Sink or Swim: Connected Health Software
Grasping the Innovation Opportunities by Mitigating Risk
Ita Richardson
1
, Ahmed AbuBaker
1
, Patrick O’Connor
2
, Jerry O’Mahony
2
and Pádraig O’Leary
3
1
Lero the Irish Software Research Centre, University of Limerick, Limerick, Ireland
2
ADA-Security Ltd., Rockchapel, Co Cork, Ireland
3
Emergent Research Ltd., Hillcrest, Dromhale, Killarney, Co Kerry, Ireland
Keywords: Connected Health, Innovation, Risks, Mitigation, Malnutrition, Software System.
Abstract: Connected Health innovation can be an opportunity for companies to develop and grow, if they take
opportunity to develop solutions for healthcare. In this paper, we discuss a case study where a very small
company in Ireland developed a connected health solution, but in doing this, discovered a number of risks
which they faced. Working with a research from the University of Limerick (author 1), they developed
mitigation strategies to avoid these risks, and subsequently developed an updated version of their initial
connected health solution. This software, Global-MN, has been implemented by a charity in India, Varanasi
Children’s Hospital. We present information about both the initial and updated product, illustrating how
overcoming the risks has resulted in the company redesigning their product for a global market. Data entered
via this software is now providing Varanasi Children’s Hospital with information and analysis, which, in turn,
is allowing them to provide a better service and improve the nourishment of children in India.
1 INTRODUCTION
The term “Connected Health” describes a new form
of healthcare service that depends on technology
innovation to deliver healthcare. This is defined by
Richardson (2015) as:
Connected Health is where patient-centred care
results from process-driven health care delivery
undertaken by healthcare professionals, patients
and/or carers who are supported by the use of
technology (software and/or hardware).
The development and implementation of
connected health solutions cannot be undertaken by
technologists alone – it must be carried out hand-in-
hand with patients and healthcare professionals
(HCP). For any connected health solution to work
efficiently and effectively, the processes through
which they work must also be developed. Therefore,
while connected health products include software, e-
health (electronic health) and m-health (mobile
health), connected health must be recognised as a
much wider concept.
Furthermore, for companies to move into the
Connected Health market, they need to develop their
products with healthcare in mind. Many innovative
ideas have been proposed. With the global older
population growing dramatically, and the costs of
healthcare rising, connected health is an innovative
marketing opportunity. To support this growth, the
first author is on a Science Foundation Ireland (SFI)
Industry Fellowship, where she has worked for the
past 2 years (part-time) to carry out research within
ADA-Security. She has developed insights into how
connected health innovations should be structured so
that both the healthcare consumer and the company
can benefit. In this research (Richardson et al.,
2016a), we are also interested in understanding how
companies make the transition from one product to
the next. Through the case study presented in this
paper, we have been enabled to investigate how a very
small company can shift extensively to a different
product line through mitigating risk. This paper
discusses these mitigations which ensure that the
company could complete product development. Our
research question is:
What mitigations should a very small enterprise
implement to ensure success in the growing
Connected Health market place?
The remainder of this paper discusses how the
innovation process works for very small enterprises,
presents a case study, outlines the company
products, presents the research method used and
Richardson I., AbuBaker A., O’Connor P., O’Mahony J. and O’Leary P.
Sink or Swim: Connected Health Software - Grasping the Innovation Opportunities by Mitigating Risk.
DOI: 10.5220/0006104102130221
In Proceedings of the 10th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2017), pages 213-221
ISBN: 978-989-758-213-4
Copyright
c
2017 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
213
discusses the risks faced and mitigations
implemented.
2 BACKGROUND
In Ireland, small-to-medium sized enterprises (SMEs)
account for 97% of all enterprises and the most
important contributors to the economy (Forfás, 2007).
The need for SMEs to become more innovative has
probably never been greater given the new
economies, new technologies, and hyper competition
with which they are challenged (Drejer, 2002).
Rogers (2004) regards innovation “as a key
ingredient in business success”.
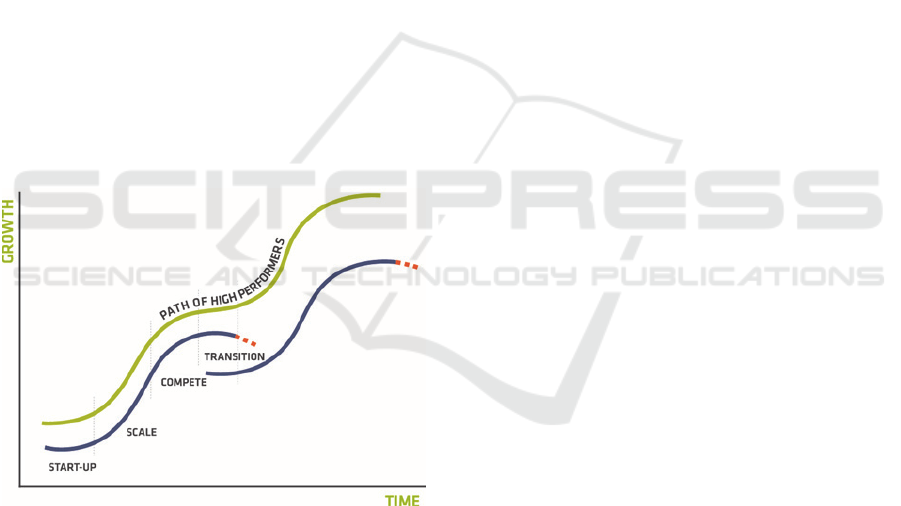
Foster (1986) advocated that the diffusion of
innovation over time follows an S-Curve (Figure 1).
Under the S-Curve paradigm, firms go through
various stages in the diffusion of innovation (Silveria,
2001), namely start-up, scale, maturation (compete)
and decline (transition). Small to medium sized
enterprises (SMEs) experience different market
challenges at each stage ranging from survival and
market validation, transitioning to challenges in
increasing market share, and entering and expanding
into the new markets.
Figure 1: Double S-Curve Model (Squarespace, 2016).
SMEs need to recognise how to operate in markets
with constraints, e.g. regulatory challenges, so as to
retain their competitive advantage as they climb the
S-Curve. Coupled with the diffusion of innovation is
market adaptation, with particular attention being
given to the stage and the focus of the market at each
stage of the S-Curve. Credence must be given to the
market forces at play given the very strong influence
they may assert on the success of innovations in new
targeted markets (Bolton and Thompson, 2013).
3 RESEARCH PROJECT
In her role as an SFI Fellow, the first author of this
paper has spent 2 years part-time as a participant
observer within ADA-Security, a very small
enterprise in rural Ireland. Working closely with the
managing directors (authors 3 and 4), she studied
their connected health software development and
innovation processes. She carried out interviews,
attended meetings, discussed strategy, analysed the
existing product, Local-Health and was involved in
the development of their new product Global-MN.
4 CASE STUDY
ADA-Security is a company, whose focus has been
on installing security systems within homes and
companies nationally. It is a very small enterprise
located in rural Ireland, over 50 miles from the
nearest city. The local area has intermittent access to
broadband, which is not uncommon in rural Ireland
[Irish Farmers’ Association, 2015].
The directors noted an opening in the market for
the installation of home care systems, such as panic
buttons and home monitoring. Innovatively,
company has developed a number of services through
which people can feel more secure and cared for in
their homes. For example, they have developed
activity monitors which can detect inactivity – if an
older person has not risen by a certain time during the
morning, and alarm can be activated. Their service
also includes a friendly-call system which would have
someone ring the older person during the day,
reducing their feeling of social isolation. They now
provide a combination of security, social and
healthcare requirements.
Maintaining the security business and expanding
into home care systems have ensured that the
company has continued to be successful for over 2
decades. Examining the S-Curve in Figure 1, it is
obvious that the company have shifted from one ‘S’
to another – from security to home care systems.
However, as innovators, and to ensure
sustainability and continued growth of the business,
the directors were soon looking at other business
opportunities. They worked with the local
community, investigated requirements from older
persons and established that there is a need for further
healthcare support within their homes, which could
not be provided through hardware products –
software was needed for this purpose. In rural areas,
there is a growing trend towards home monitoring,
HEALTHINF 2017 - 10th International Conference on Health Informatics
214
with many ratified medical devices available for use,
by the older person in the home.
Home monitoring, then, brings with it another
need – that of transmitting biometric data such as
blood pressure measurement and blood sugar levels
to the patient’s health professional. General Practice
has the potential to change – at times, there may not
be a need for the patient, in this case the older person,
to travel to the practice to have these measurements
taken on a sporadic basis. Alternatively, they can take
their own measures and transmit these to medical
care. Consequently, ADA-Security directors, in
conjunction with another company, developed Local-
Health, a prototype for initial testing, with a view to
supplying the connected health market.
4.1 Local-Health: Biometric
Measurement System
Local-Health (described in Richardson et al., 2016b)
allows individuals to text their biometrics from their
mobile phone to the local General Practice. The
information is coded for reading by the bespoke
software where the text is received.
Figure 2: Blood pressure reading text message.
As an example, in Figure 2, the text message
shows a Blood Pressure (BP) reading of 70/120,
which was taken by the patient using a home blood
pressure monitor. The receiving system recognises
the mobile number from whom the text came, and the
data is collected within the General Practice.
The data is compared against an expected reading
for the particular patient. If the actual reading is
abnormal, an alert is sent to that user, asking them to
follow the suggested preventative advice, for example
to seek medical advice. An alert can also be sent to
individual users if they have not sent their results at
the time expected. The General Practitioner can
monitor each patient’s readings on a regular basis,
receive alerts if someone’s readings go out of control,
and conduct up a follow-up if they deem it to be
needed.
Through modifying their healthcare process, the
implementation of this simple connected health
solution has introduced technology for use within the
General Practice,. The patient no longer has to attend
the practice on a regular basis, for example, weekly,
and yet the Doctor and Nurse can effectively monitor
the patient. The consequence of this is that the patient
can be monitored without having to leave their own
home, while the queues and load for the medics in this
rural practice has been alleviated. The General
Practitioner can view their patient’s data as a line
graph e.g. blood pressure over a period of time.
Therefore, a trend is illustrated and support making
medical interventions in a convenient fashion.
4.2 Local-Health: Potential Business
Risks
As time progressed, the company directors
recognised a number of potential business risks which
arose with Local-Health system:
Aimed towards individuals and small healthcare
practices;
Market for Local-Health is national;
ADA-Security expertise is in hardware;
System developed on a known platform;
Regulation required for the system.
Aimed towards individuals and small
healthcare practices: Once patients have mobile-
phone text available they can submit readings, and
they are not required to buy Local-Health software.
Software cost, therefore, is totally borne by the
healthcare practice. The expectation is that this will
become a high-volume, low-cost product. Due to
high software development costs, the business model
is not very cost-efficient.
Market for Local-Health is national: Due to
the nature of its hardware products, which includes
physical installation of security and social systems,
the company has dealt mainly locally and nationally.
The market needs to become international.
However, going global with a low-cost product can
be an expensive undertaking.
Company expertise is in hardware: Those
working in the company have a background and
experience in hardware installation and hardware
attributes. The nature of the new product requires
software engineering expertise. This has not been
readily available, and development to-date has been
sub-contracted. However, without in-house
expertise, other business requirements take priority.
System developed on a known platform:
Local-Health was to be used by older persons within
the local community and it was considered best to
develop the product as a mobile-phone text-based
system integrating with healthcare practice software.
While this works effectively, there is no income due
to selling product to individual patients.
Regulation required for the system: Within
their hardware business in the security industry, ADA
regularly implement regulations. Under European
Council (2007) directive, a medical device means
BP
–
70-120
Sink or Swim: Connected Health Software - Grasping the Innovation Opportunities by Mitigating Risk
215

(amongst other things) “software… intended by the
manufacturer to be used for human beings for the
purpose of diagnosis”, and “software … is a medical
device”. As Local-Health is dealing with the
transmission, collection and diagnosis involving
patient data and HCPs, it is a medical device.
Regulations need to be integrated into the software
which is time-consuming and expensive, thus
pushing up the cost of production.
5 MAKING THE TRANSITION
Reflecting on the S-Curve (Figure 1), the Transition
required for ADA-Security to move from their main
businesses of security and home care systems to
Local-Health is substantial, and the company needs to
find a way to overcome the problems identified. They
had put many resources into the development of
Local-Health to both fulfil a social need and be
profitable. This was an opportunity for them to move
across to yet another ‘S’ curve which is vital for the
survival of any small company - it is the innovative
companies who survive. The leap from security
systems to homecare systems was achievable for the
company. The leap from their current offerings to the
Local-Health software system was difficult.
So how could the company get over this chasm?
How could they mitigate the risks they had identified?
Considering their options, the directors with the first
author of this paper made strategic decisions to
change the direction of the product, allowing the
company to develop a new innovation, while also
presenting opportunities to consider other markets
with which they could be involved. The following
modifications were made to mitigate the difficulties
identified above:
Seek global market opportunities
Develop solution for an organisation
Acquire software engineering skills
Investigate non-regulated possibilities
Investigate mobile solutions
Seek global market opportunities: Global
opportunities present much larger markets than local,
and companies have the ability to expand beyond
their local area. For ADA-Security, the installation of
hardware systems provided the natural consideration
of national solutions. However, moving to a
software-based product provides the potential to
exploit global expanding markets. In particular, the
company recognised that developing countries can
offer large populations, therefore much greater sales
potential.
According to World Food Programme (WFP)
“there are around 800 million people in the world who
are malnourished” (WFP, 2016). This includes 200
million children under the age of five suffering from
undernutrition (USAID, 2016). A quarter of the
world’s malnourished children live in India (WFP,
2016), and there are 473,000 malnourished children
in Kenya (UNICEF, 2016). Charities and Non-
Government Organisations (NGOs) provide health
check-ups to diagnose malnourished children and
nutrition programmes to resolve the problem.
The development of a system, Global-MN, to
support nourishment programs globally has the
potential to provide a large market to ADA-Security’s
software solution.
Develop solution for an organisation: Local-
Health was developed for individual use, but, selling
to an organisation would be more profitable.
Therefore, charities in developing countries were an
opportunity that should be explored further, and the
development of Global-MN was undertaken. This is
an innovative mobile health software application that
can store, track and monitor details of malnourished
children.
NGOs hire Community Health Workers and
health clinics to reach children, test and diagnose
them, enrol them into nutrition programmes, and
schedule further visits to monitor their progress. The
test process normally includes taking the child’s
height, weight, middle-upper arm circumference
(MUAC) and age. To ensure user input to the
product, at development stage, ADA-Security teamed
with an Indian based charity, Varanasi Children’s
Hospital, whose work with these children has been
hampered by the following problems:
The manual process currently used to document
children’s readings is time consuming, thus
decreasing productivity of Community Health
Workers;
Retrieval of paper files when a child returns to
the nutrition clinic is cumbersome and difficult;
Paper-based process does not support efficient
monitoring of children’s progress;
Community Health Workers are unable to
identify previously registered children
As a result, Varanasi were not able to reach and help
as many children as they would like. Additionally,
there are difficulties in developing reasonable
statistics to show how effective the work of the
charity is. Varanasi were unable track how well
individual children are progressing, nor could they
see the success they are having in the field. Having
HEALTHINF 2017 - 10th International Conference on Health Informatics
216

matched this situation with Local-Health, a decision
was made within ADA-Security that Global-MN,
would initially support the nutrition program within
Varanasi Children’s Hospital.
The identified end users are Community Health
Workers, as Global-MN software will be downloaded
into their phones, allowing them to register and
perform screenings on malnourished children. The
second end user group are charity and NGO
management who ensure that their nourishment
programme is effective. Also, to obtain investment
from donors, they must demonstrate the effectiveness
of their program. Therefore, Global-MN will follow
a Business to Business (B2B) commerce model rather
than Business to Consumer (B2C) commerce model.
In the first instance, ADA-Security has developed
the product for Varanasi Children’s Hospital, with
plans to expand in the future to other charities
internationally.
Acquire software engineering skills: This
software-based innovation has potential to open
doors to a global market. While, through their
business and initial software development, they were
in a position to identify the innovation, ADA-
Security directors have recognised that they need to
acquire software engineering skills and make this
product a priority. The skills will ensure that the
product they develop is marketable, secure and
profitable. Therefore, to bring software engineering
to the development process, ADA-Security have
partnered with Emergent Research Ltd. (author 5), a
high performance start-up software company
headquartered locally.
Investigate non-regulated possibilities: While
Global-MN must be secure and private, it is not a
product that needs to be regulated. It is used to input,
track and analyse food-related information – for
example, information regarding children who are
malnourished and amounts of food. Therefore, it is
not a Medical Device and there are no regulations that
need to be considered during its development.
Investigate mobile solutions: Local-Health was
developed as a text-based system for the reasons
stated earlier. However, within the global market for
organisations within which Global-MN is being
targeted, a text-based system would have many
limitations, and a mobile internet-based product is the
better option. We have undertaken research which
demonstrates that there is internet coverage
throughout both India and Kenya, countries where
malnourishment programs with children are being
undertaken, demonstrating sales’ potential.
Additionally, the company needed to understand the
cheapest and most convenient method by which the
data could be transmitted. In rural Ireland, given that
there is often limited and sporadic internet access, the
solution for Local-Health was to text data via mobile
phone. In rural India, internet access is relatively
stable, and cheaper than using a mobile phone.
Therefore, Global-MH used the internet as its
platform. Entering data in this manner means that
once a child is registered with Varanasi Children’s
Hospital, their information is immediately available
to the central office. The effectiveness of the
program can be monitored on a regular basis.
Children who are not progressing as expected can
have their food source changed early on in the
program, and interventions by the central office can
happen quickly. Therefore, infant mortality rates are
affected positively in the long-term.
5.1 Global-MN: A Software Solution
Global-MN system is a web-based system with data
stored on a secure system in Ireland. This research
project was carried out as one action research cycle,
allowing the researchers to understand the difference
that the implementation of the software made in the
field and how the processes could be changed to make
a difference. The charity director was trained in
system use by author 3. He then travelled to India
where he trained the Community Health Workers.
They enter data to the system using software running
on a smart phone. This data can be aggregated and
analysed for Varanasi Children’s Hospital allowing
management to make informed decisions regarding
their malnourishment program..
6 Global-MN: MANAGING
MALNOURISHMENT
Using Global-MN, Community Health Workers add
children’s identification data and a photograph to the
system in the rural villages and collect measures to
determine malnourishment: MUAC, weight, height
and age. Malnourished children are started on a
special food program. They return to the clinic every
two weeks where their signs are re-measured, further
food provided, and updates added to the Global-MN
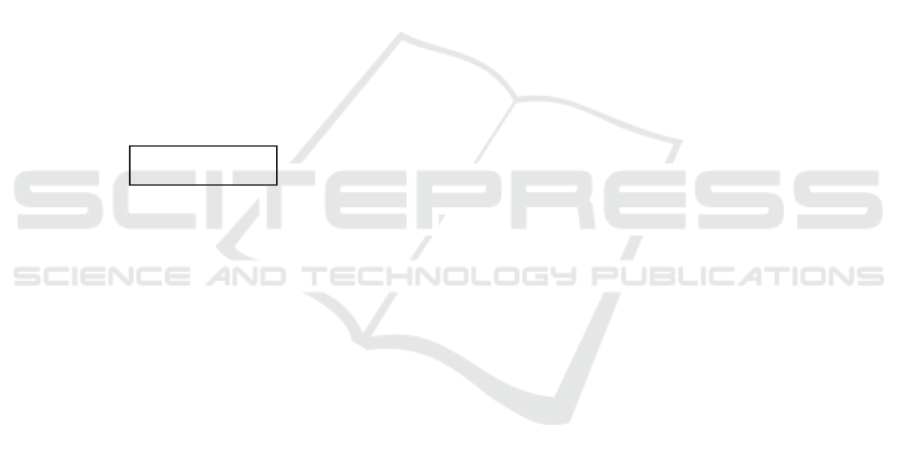
system. Figure 3 shows relevant screen shots from
the system. Once data is uploaded, management are
provided with data analysis, allowing them to observe
progress of children who are on the food program.
Sink or Swim: Connected Health Software - Grasping the Innovation Opportunities by Mitigating Risk
217
6.1 Data Analysis - Individual
Data illustrated is not real data to maintain
confidentiality. However, it illustrates how the
system can be used for the benefit of tracking the food
program for malnourished children.
In Global-MN, data is stored about individual
children, including: child ID, which is created by the
system when child is first entered, child name,
packets given to child per week, start weight, MUAC
and height, weight, MUAC and height at each clinic
visit, healthcare clinic to which the child is registered,
and status, which can be active or discharged. Thus,
the system allows the charity to visualise trends for
individual children.
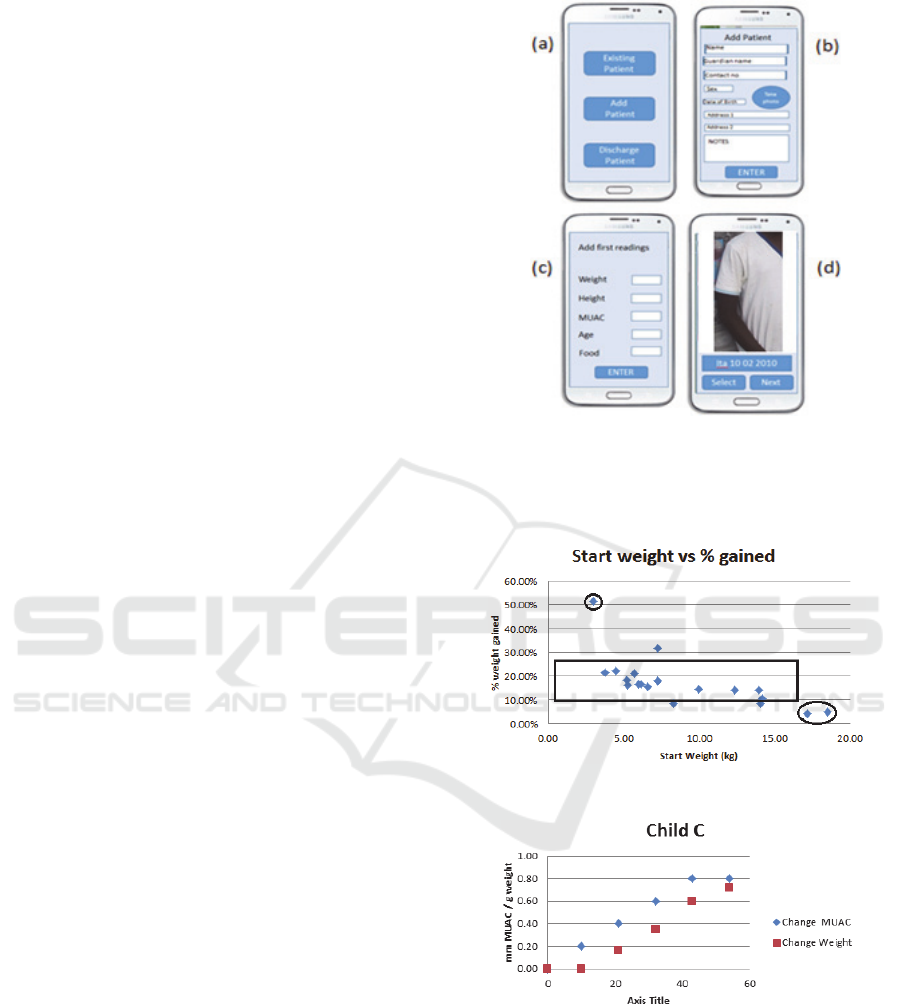
As an example, Figure 4 shows the percentage
weight gained by individual children based on their
start weight. We have highlighted the data for one
child whose start weight was 3kg – this child gained
50% of start weight while on the program. Two
children weighing over 15kg at the start of the
program gained approximately 5% of start weight.
Most children gained between 10-25% of their start
weight, which is what would be expected from the
food program. Figure 5 shows the weight and
MUAC gain for a single child during 6 visits to the
healthcare clinic. As weight increases, so does the
size of the MUAC. This demonstrates that, for this
child, the malnutrition program is having a positive
effect.
Once a child attends the healthcare clinic, a target
weight gain is determined for him / her depending on
starting weight, MUAC and height. For the child
illustrated in Figure 6, it was expected the child would
gain over 4kg in the course of the program. However,
it can be seen here that actual weight gain is much
lower. With access to on-line real-time data, they can
make decisions about this child. It could be, for
example, that the child has an underlying condition,
in which case she / he can now be sent for medical
attention. Prior to Global-MN, this information was
not available, further diagnosis was missing, thus
perpetuating their problem.
Figure 3: (a) Top level menu (b) Adding child’s details (c)
Adding information for a child, including number of food
packets for that child (d) Information about existing patient
including photograph.
Figure 4: % weight gained based on start weight.
Figure 5: Weight (kg) / MUAC (cm) gained by child over 6
clinic visits.
HEALTHINF 2017 - 10th International Conference on Health Informatics
218
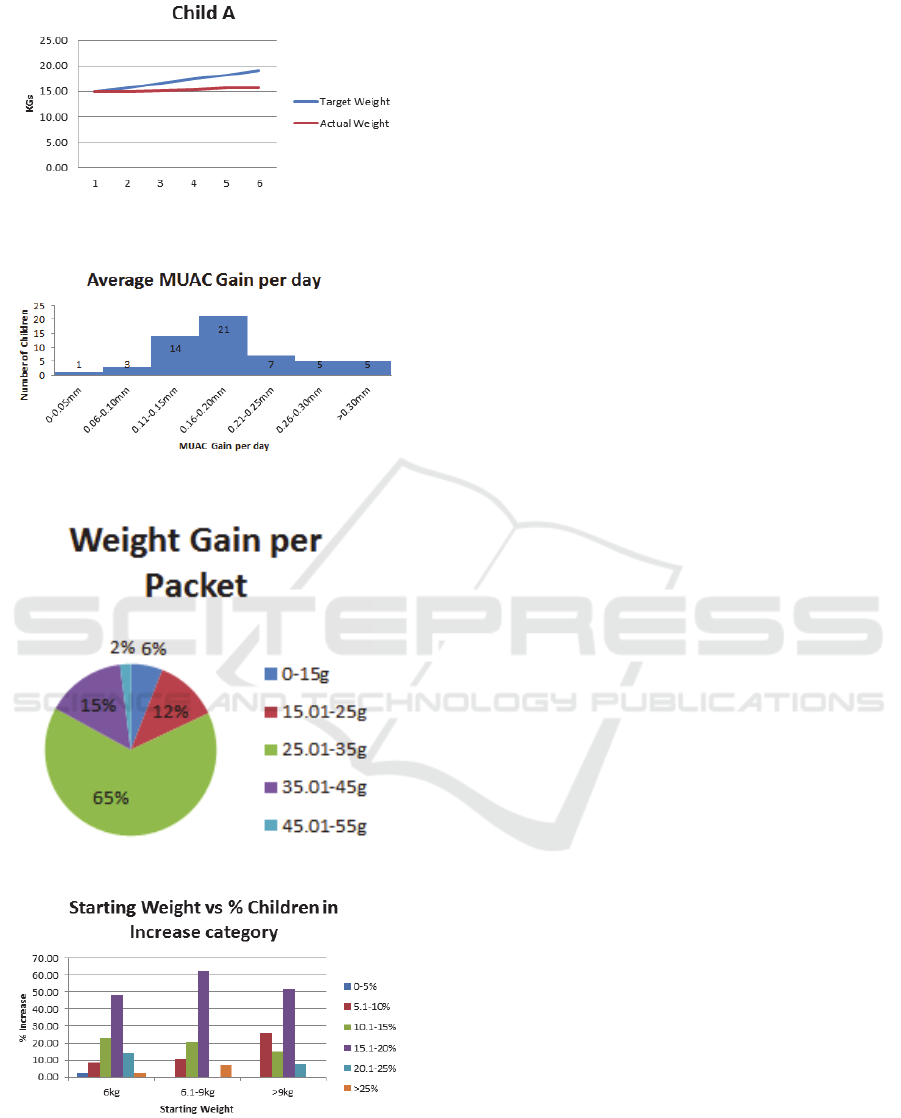
Figure 6: Actual weight gain mapped against Target weight
for a child.
Figure 7: Average MUAC gain per day during program.
Figure 8: Weight gain per packet.
Figure 9: Weight increases mapped against starting
weights.
6.2 Data Analysis - Collective
Data can also be aggregated to determine how well
the food program is working. This information is used
to ensure that children who can benefit are receiving
food and that the investment in food is having the
maximum required effect. In figure 7, the average
MUAC gain per day illustrates that MUAC is
increasing through the food program. Thirty-five
children (out of 56), 62%, gain between 0.11 and
0.20mm per day. Figure 8 illustrates children’s
weight gain per food packet distributed. Sixty-five
percent of children gained between 25-35g in weight
per packet of food. However, six percent of children
gained less than 15g per packet distributed. The
charity can now further investigate as to why
distributed food is not being effective.
Figure 9 shows data for discharged children
categorised by starting weight. The expectation is
that children’s weight would increase by 15-20% of
their starting weight. As can be seen in the graph,
48% of children who start at 6kg or less gain this
amount of weight. Sixty-two percent of children who
are in the 6.1-9kg category gain between 15-20%,
while 51% of those whose starting weight is greater
than 9kg gain similar amounts. Such aggregated data
allows the charity to delve deeper into the success and
difficulties within the program.
6.3 Case Study - Summary
To implement Global-MN within Varanasi
Children’s hospital, Community Care Workers had to
be trained in system usage to ensure that data was
being entered correctly. Initially, all records were
also held on paper, requiring extra work for everyone
involved. Trust in the system needed to be developed.
At this point, we, the researchers, have been enabled
to provide them with both individual and collective
data, allowing them to make changes within the
charity. For example, if a child is observed as not
gaining the expected weight within the program they
can be checked for other health issues. The analysis
regarding weight per packet mapped against start
weight is allowing the charity to consider whether
they give different amounts of food to children who
start with higher weights. They are collating data
which can be used to support arguments for further
funding for the charity.
Following the case study, the software is being
updated to make it more user-friendly and to provide
more on-line and visual reporting that currently exists
within the system. Both Varanasi Children’s Hospital
Sink or Swim: Connected Health Software - Grasping the Innovation Opportunities by Mitigating Risk
219

and ADA-Security are benefitting from the
implementation and analysis of this case study.
7 CONCLUSION
In Ireland and globally, it is recognised that
healthcare is a serious problem that needs fixing -
“healthcare is the greatest immediate threat to the
country” [USA]” (Chase, 2016). Many innovators
see connected health in a variety of forms as a means
to solving that problem. Innovators must decide the
best way to mitigate risks that arise, ensuring that the
return on investment is as expected. For the small to
medium sized enterprise, and certainly for the very
small enterprise, taking risks has a far-reaching effect.
Within ADA-Security, the directors recognised
and mitigated the risks being faced by the company.
Understanding that their business could grow
significantly they sought global market opportunities,
identifying that there was a need for data analysis and
tracking in programs in developing countries. Their
product needed to shift from supporting small to
supporting large and from solutions for individuals to
solutions for organisation. There are many NGOs
working with malnourished children in developing
countries, and, supported by a business plan, ADA-
Security are now marketing internationally. They
recognised that they needed to extend their skill set.
Rather than take on new employees, they have
partnered with Emergent Research to provide
software skills. A further risk was entering the
Medical Device software market which is heavily
regulated. While being cognisant of regulation, they
are developing software without having to obtain
European Union or similar certification. In bringing
in an established software partner, there are
documented software development processes in
place. From a technical perspective, the greatest
change was that of the platform upon which the
product would run - Global-MN is very different to
Local-Health.
Throughout their 25 year history, ADA security
have been an innovative company, expanding their
product base, growing and providing employment in
the local community. They recognised an
opportunity for innovation, and, in exploiting this,
have considered how to overcome the initial risks. In
conclusion, Global-MN has given ADA-Security a
further innovation opportunity. Considering the five
risks and developing mitigation strategies has
allowed them to leap the larger chasm between S-
curves. As they move forward on their innovative
journey, they can take the learnings from Global-MN
development to ensure that they can continue to
innovate and grow.
ACKNOWLEDGEMENTS
This work was supported by Science Foundation
Ireland (SFI) Industry Fellowship Grant Number
14/IF/2530. We would like to thank Pat McMahon,
Varanasi Children’s Hospital for invaluable
discussion.
REFERENCES
Chase, Dave, Why 98% of Digital Health Startups are
Zombies and What They Can Do About it,
http://www.forbes.com/sites/davechase/2016/05/18/w
hy-98-of-digital-health-startups-are-zombies-and-
what-they-can-do-about-it/#1f0ed5bf68f3, Forbes,
22th September, 2016.
Bolton, B., and Thompson, J., (2013) Entrepreneurs Talent,
Temperament and Opportunity, Routledge 3rd Ed.
Drejer, A.(2002) ‘Situations for innovation management:
towards a contingency model’, European Journal of
Innovation Management, 5(1), 4-17.
European Union Council, 2007, EU directive 2007/47/EC.
Irish Farmers Association, Supporting Farms and
Businesses in the Irish Countryside, 2015.
https://www.ifa.ie/wp-
content/uploads/2015/08/150805-IFA-Countyside-
Policy-Document-Final.pdf
Forfás (2007) “Towards developing a policy for
Entrepreneurship in Ireland”, Dublin.
Foster, R.J., (1986) Innovation: The Attackers Advantage.
New York: Summit Books.
Richardson I. (2015). Connected Health: People,
Technology and Processes, Lero-TR-2015-03, Lero
Technical Report Series. University of Limerick.
Richardson, Ita, O’Mahony, Jerry, Howarth, Paul,
O’Connor, Patrick, Glenny, Liam (2016b), Connected
Health: From Rural Ireland to Rural India, Software
Quality in Healthcare Systems, co-located with IEEE
International Conference on Software Engineering,
Austin Texas, May 2016, pp 39-42.
Richardson, Ita, Costin, Yvonne, O’Connor, Patrick,
O’Mahony, Jerry, Glenny, Liam (2016a) Connected
Health Innovation within SMEs: Understanding the
Marketplace, 4th International Conference on
Innovation and Entrepreneurship, Toronto, Canada, 28-
29th April, 2016, pp 63-71.
Rogers, M. (2004), ‘Networks, firm size and innovation’,
Small Business Economics, 22, 141-153
Silveira, G.(2001), ‘Innovation Diffusion: research agenda
for developing economies’, Technovation, 21, 767-773.
HEALTHINF 2017 - 10th International Conference on Health Informatics
220

Squarespace (accessed September 2016) http://static1
.squarespace.com/static/55d244b8e4b0f26e56cd2b32/t
/55e51df8e4b09f6b9550a6d9/1441078778831
WFP (accessed September 2016). World Food Program:
Hunger Statistics. https://www.wfp.org/hunger/stats.
UNICEF (accessed September 2016). UNICEF: Kenya.
http://www.unicef.org/appeals/kenya.html.
USAID, (accessed September 2016). Home: GLOBAL
NUTRITION. https://www.usaid.gov/what-we-do/
agriculture-and-food-security/supporting-global-
nutrition.
Sink or Swim: Connected Health Software - Grasping the Innovation Opportunities by Mitigating Risk
221
