
Extraction of Useful Knowledge for Making Roster by Analyzing
Nurse Scheduling Data and Incident Data
Koichiro Okada
1
, Masanori Akiyoshi
2
, Yukie Majima
1
, Hiroe Takahashi
3
, Sayuri Tanaka
4
,
Misae Tanioka
4
and Miwako Hori
4
1
Department of Computing, Osaka Prefecture University, 1-1 Gakuencho, Naka-ku, 599-8531, Sakai-shi, Osaka, Japan
2
Department of Computing, Kanagawa University, 3-27-1, Rokkakubashi, Kanagawa-ku, 221-8686,
Yokohama-shi, Kanagawa, Japan
3
Department of Planning Management, Japan Community Health care Organization (JCHO), Tokyo, Japan
4
JCHO Osaka Hospital, Osaka, Japan
Keywords: Incident Data, Ladder Level, Nurse Rostering, Nurse Scheduling, Pattern Mining.
Abstract: As described herein, we sought knowledge necessary to make a roster for nurses by analyzing nurse
scheduling data and incident reports on the night shift. Even today, it is difficult to say that computers are
used effectively producing nurse rosters. One reason is that algorithms suggested by researchers are not
practical for nurses working at various sites because they are built without consideration of medical accidents
known as “incidents”. Another reason is that the study of incidents from a team's perspective, which is the
original mode of working as a nurse, is not available. Therefore, this study was conducted for discovery of
knowledge to help produce a nursing roster by analyzing nurse scheduling data and incident data for night
shifts from the viewpoint of teams, which is the original mode of working for nurses.
1 INTRODUCTION
When it is necessary to arrange staff during a day at
institutions such as hospitals, managers usually adopt
a shift-work system to fill a schedule, with shift staff
working days and hours. This system demands a duty
roster to show which duties are covered by which
employee on which time shift. Therefore, this roster
must be produced with consideration of the number
of people needed for duties and various constraints
such as workers’ requests and their respective
capabilities. This scheduling invariably takes much
time. Generally, an experienced expert who is
familiar with the duties and personnel produces this
roster over a long period of time. The problem of
making such a roster entails "the necessity of
assigning work as staff have requested as effectively
as possible." This so-called shift scheduling problem
can be resolved through mathematical programming.
Producing a roster at a medical institution such as a
hospital is a nurse scheduling problem.
Nurse scheduling problems are regarded as a
difficult optimization problem. That is true because
no matter how one might try to resolve the problem,
it is difficult to define an optimum solution for any
reason. If we define such a solution, then it is merely
difficult to obtain the solution. A survey paper
(Smith-Daniels et al., 1988) has presented that
research of nurse scheduling problems began in the
United States in 1976 (Miller et al., 1976). It declined
thereafter, but became popular again from about 1998
(Dowsland, 1998; Miller, Kiragu, 1998). In recent
years, many researchers engaged in the study of this
problem (Burke et al., 2004; Ikegami, 2005; Ikegami,
Tanaka, 2014; Tassopoulos et al., 2015). However, in
spite of the fact that many researchers have developed
the study and have suggested many algorithms for
solving nurse scheduling problems, it remains
difficult to say that computers are used for making
rosters effectively. This fact is apparent from a survey
(Ikegami et al., 1995) that found "the mean time of
making roster is 6.8 hours." Moreover, nurses of a
certain General Hospital, which provided data for our
study, reported long preparation times. Apparently,
hospitals have insufficient cost and technical
knowledge to adopt scheduling software.
Furthermore, the suggested algorithms are not
practical for nurses working at a site because they are
Okada, K., Akiyoshi, M., Majima, Y., Takahashi, H., Tanaka, S., Tanioka, M. and Hori, M.
Extraction of Useful Knowledge for Making Roster by Analyzing Nurse Scheduling Data and Incident Data.
DOI: 10.5220/0005776303830388
In Proceedings of the 9th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2016) - Volume 5: HEALTHINF, pages 383-388
ISBN: 978-989-758-170-0
Copyright
c
2016 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
383

suggested without consideration of medical accidents
known as “incidents.”
Table 1: Number of nurses per level.
Ladder level Number of nurses
1 26
2 16
3 19
4 5
5 6
Temporary (0) 18
Studies of incidents (Bates et al., 1995; Onozawa
et al., 2000) have been conducted by many
researchers along with the nurse scheduling problem.
Most depend on examinations of individual nurses to
examine "What kind of nurses and circumstances
cause incidents and what should we do for preventing
those incidents." Research about incidents from a
team perspective, the original mode of working for
nurses, has not been conducted to date.
Therefore, this study was undertaken for
discovery of knowledge to help produce a nursing
roster by analyzing nurse scheduling data of 2009–
2013 (5 years) and incident reports related to night-
work provided by A General Hospital from the
viewpoint of teams.
2 EXPERIMENTAL DATA
DETAILS
Data we use are nurse scheduling data covering five
years (April 1, 2009 – March 31, 2013 ) and incident
date data on night shifts from the same period of time
provided by A General Hospital (number of hospital
beds, 68; mean number of hospital patients per day,
62; number of nurses, 89). The number of nurses
includes temporary employees. Changing of nurses
occurred during those five years.
Through research collaboration with A General
Hospital, we received consent to use these data.
2.1 Details of Nurse Scheduling Data
These nurse scheduling data (e.g. see Appendix A)
comprise seven items.
Nurse ID
Ladder level (Skill level)
Date
Day of the week
Types of shift work
Shift total of the month for each nurse (e.g. nurse
A [day shift, 10; night shift, 5])
Total number of nurses with each shift (e.g. Day
1 [day shift, 12; night shift, 6])
Nurse ID consists of five digit numbers. The ladder
level has five stages of 1–5 (temporary nurse is 0,
number of nurses per level is shown in Table 1) and
Types of shift work consist of 11 items.
Day shift
Late shift
Night shift
Training
Business trip
Recreation
Public holiday
Holiday
National holiday
Substitute holiday
Absence
2.2 Details of Incident Date Data
These incident date data on the night shift (e.g. see
Appendix B) consist of two items as follows.
Types of incidents
Time and date of occurrence of each incident
Types of incidents consist of three items.
Care: About fall occurrence
Pharmacy: About wrong medication
Tube: About removal of tube
This study was conducted for discovery of the
knowledge to support the production of a nurse roster
by analyzing these data from a team viewpoint.
3 EXPERIMENT
For this study, we conducted three experiments.
Extraction of a shift pattern that all nurses meet
working throughout the year
Correlation of incidents and nurse group in the
night shift
Extraction of nurse pairs with no mutual work on
a day or night shift during five years
Table 2: Time series database (Cited by Zaki, 2001).
SID EID Items
1 10 CD
1 15 ABC
1 20 ABF
1 25 ACDF
HEALTHINF 2016 - 9th International Conference on Health Informatics
384
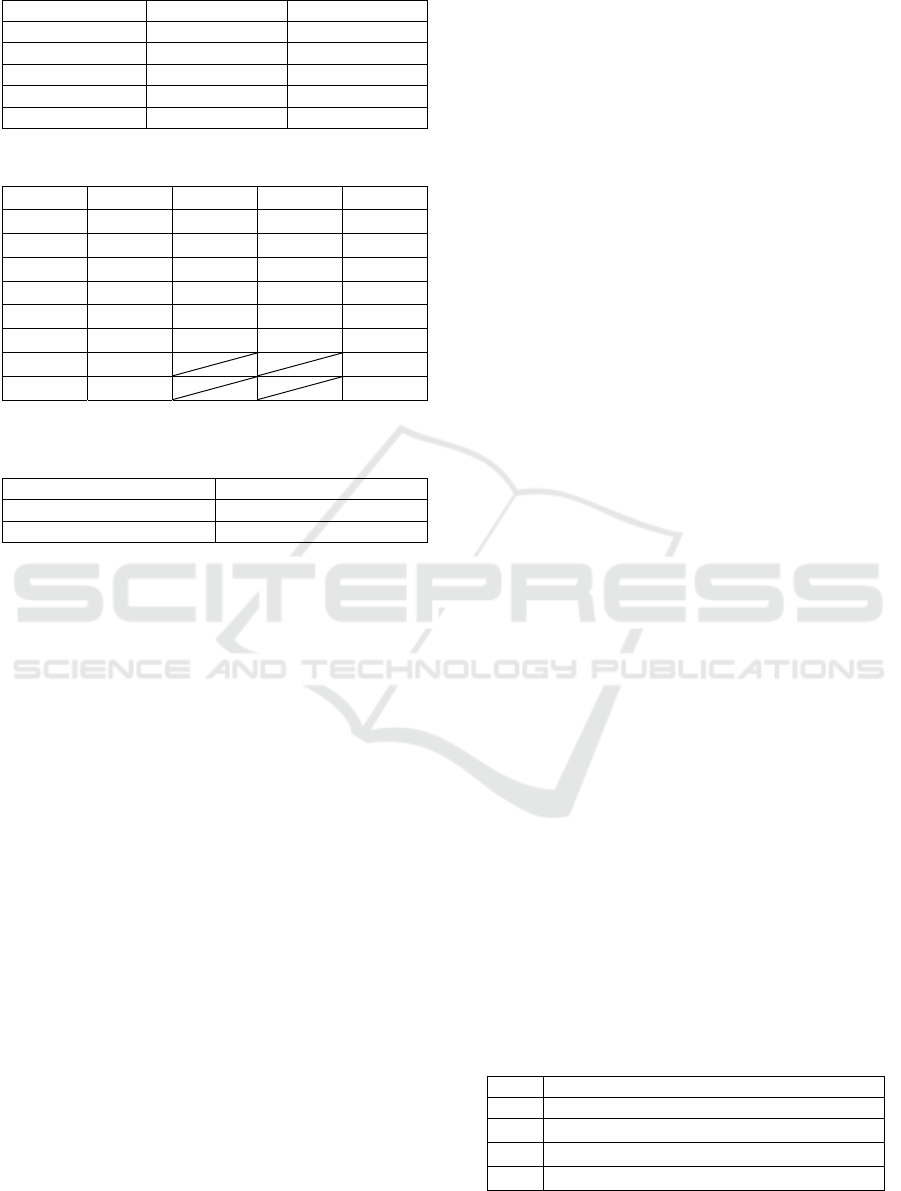
Table 2: Time series database (Cited by Zaki, 2001) (cont.).
2 15 ABF
2 20 E
3 10 ABF
4 10 DGH
4 20 BF
4 25 AGH
Table 3: Part of list coupling SID and TID per item.
A B
…
SID EID SID EID
…
1 15 1 15
…
1 20 1 20
…
1 25 2 15
…
2 15 3 10
…
2 15 4 20
…
3 10
…
4 25
…
Table 4: Lis obtained by combination of item A and B in
Table 3.
A-B
SID EID
1 20
3.1 Extraction of Shift Patterns with
All Nurses Working throughout the
Year
3.1.1 Overview
Nurse replacement occurred in each year, but we
specifically examined nurses who worked throughout
the year and extracted shift patterns such that all
nurses meet using a sequential pattern mining
algorithm called SPADE (Sequential Pattern
Discovery using Equivalence classes) algorithm
(Zaki, 2001). Constraint conditions for making shifts
are likely to be hidden in such shift patterns.
3.1.2 Spade Algorithm
Sequential pattern mining is extraction of pattern
which have ordering. SPADE algorithm is the way of
this mining. SPADE receives a time series database
such as Table 2 as input, and this database consists of
time series data. Time series data has Sequential ID
(SID), Time ID (TID) and Items. SPADE combine
SID and TID into list per item like Table 3 and find a
new time series pattern by coupling these lists like
Table 4.
3.2 Correlation of Incident and Nurse
Groups on the Night Shift
3.2.1 Overview
On the night shift each day, we sorted nurse groups
on shifts according to whether that group is likely to
cause an incident or not based on the following
definition of the group. Then we assess the correlation
of the incident and that group.
Definition: when group work at night shift as
hellows, we regard its group as “Risky group” that is
likely to cause incident and other as “Non-risky
group”.
Group have over 2 nurses whose ladder level is
under 3 and have no nurse whose level is over 3
3.2.2 Procedure
We make an experiment by following the steps
described below.
1. We pick out all nurses as each night shift from
scheduling data. Every nurse work at night shift
are one group.
2. We distinguish these groups “Risky group” form
“Non-risky group” using above definition.
3. We calculate the rate of each incident occurrence
in the case of “Risky group” and “Non-risky
group”.
3.3 Extraction of Nurse Pairs with No
Work Together on Day or Night
Shifts during Five Years
3.3.1 Overview
Nurse work is team work related directly with the life
and death of patients. Therefore, human relations
must be considered, particularly excluding pairs that
are more likely to cause incidents. In addition, human
relations can cause resignation of freshly recruited
nurses (Mizuta et al., 2004). Therefore, it is important
to formalize such pairs without leaving it as tacit
knowledge.
Table 5: Extracted shift pattern that has maximum length in
each year.
Year Extracted shift pattern that has maximum length
2009 <N,N,PH,D,D,N,N,PH,D>
〃
<N,N,PH,PH,D,D,N,N,PH>
〃
<N,N,PH,D,D,D,N,N,PH>
〃
<N,N,PH,D,D,N,N,PH,PH>
Extraction of Useful Knowledge for Making Roster by Analyzing Nurse Scheduling Data and Incident Data
385
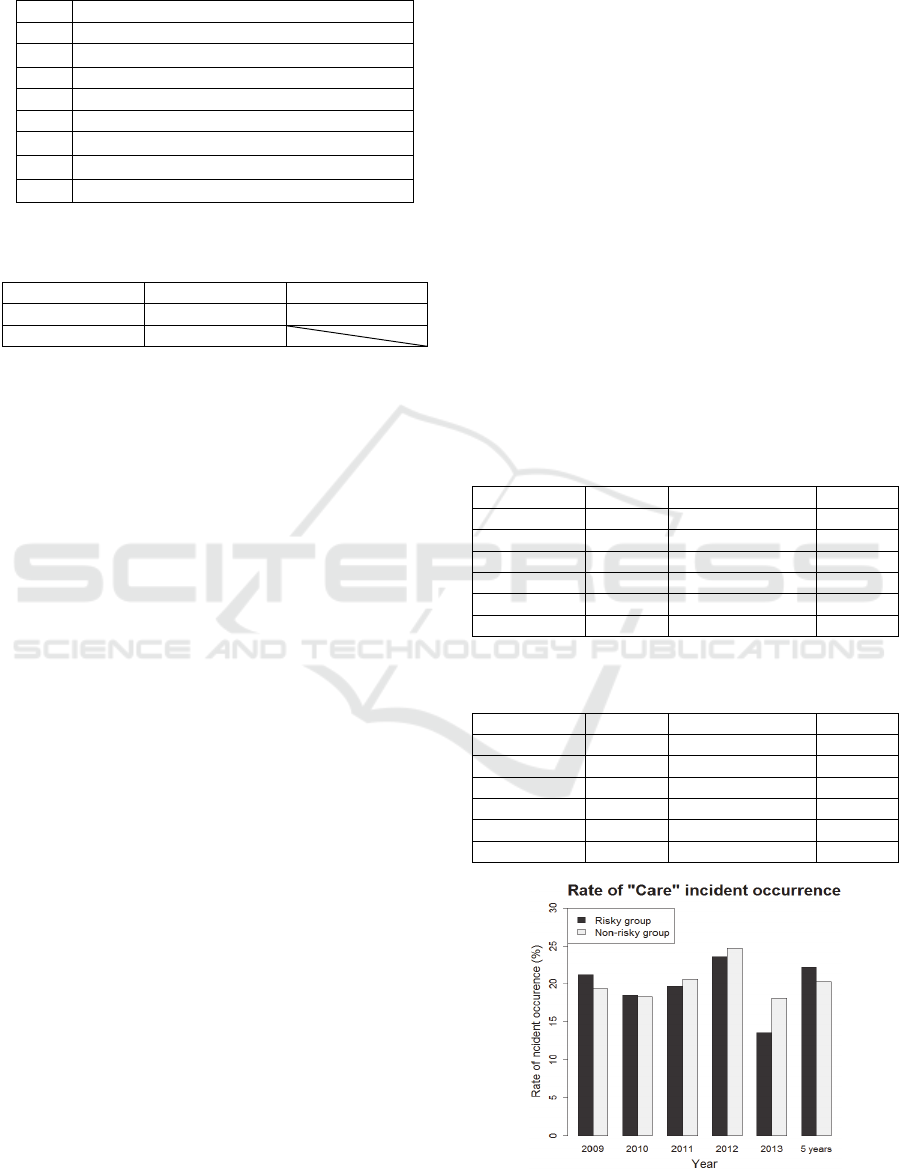
Table 5: Extracted shift pattern that has maximum length in
each year (cont.).
Year Extracted shift pattern that has maximum length
2010 <D,D,N,N,PH,D,D>
〃
<N,N,PH,PH,D,D,D>
2011 <D,N,N,PH,D,D,N,N>
2012 <D,D,N,N,PH,PH,D,D>
2013 <D,D,N,N,PH,PH,D,D>
〃
<D,N,N,PH,PH,D,D,D>
〃
<PH,PH,D,D,D,N,N,PH>
〃
<PH,D,D,D,N,N,PH,PH>
*D: Day Shift, N: Night Shift, PH: Public Holiday
Table 6: Combination of shift patterns of length 3.
<D,D,D> <D,D,N> <D,N,N>
<N,N,PH> <N,PH,D> <N,PH,PH>
<PH,D,D> <PH,PH,D>
*D: Day Shift, N: Night Shift, PH: Public Holiday
3.3.2 Procedure
We make an experiment by following the steps
described below.
1. We acquire all nurse IDs from scheduling data and
make pairs of IDs.
2. We make pairs of IDs at day shift and delete them
form pairs created procedure 1. Similarly, we do
at night shift.
3. After procedure 2, leftover pairs are regarded as
nurse pairs with no work together on day or night
shifts during five years.
4 RESULTS AND DISCUSSION
4.1 Extraction of Shift Patterns with
All Nurses Working throughout a
Year
Table 5 shows the extracted shift pattern that has
maximum length in each year. The maximum lengths
of shift patterns were high values such as 7–9, but a
nurse actually making a roster considered these
longest shift patterns only slightly when producing
the roster. In other words, roster makers consider
shorter shift patterns. Longer shift patterns result
from combined constraints such as "Two consecutive
night shifts are forbidden." Actually, these longer
patterns are explainable by the combination of shift
patterns of length 3, as shown in Table 6. In both
Table 5 and 6, “D”, “N” and “PH” indicate “Day
shift”, “Night shift” and “PH”, respectively. However,
“Night shift” is a set of two “N” like <N,N>. Since,
first “N” indicate “begin working” and second “N”
indicate “finish working”.
4.1 Correlation of Incidents and Nurse
Groups on the Night Shift
Tables 7 and 8 respectively show the rates of incident
occurrence when nurses work in a "Risky group" or
"Non-risky group". Figures 1, 2 and 3 show the rates
of incident occurrence per incident type. According
to Tables 7, 8 and Figures 1, 2 and 3, the rate as a
"Risky group" was slightly higher than that of a "Non-
risky group". Therefore, we investigated them using
a t-test to clarify whether these results had significant
differences. Results show no significant difference in
any of the three kinds of incident. However, these
results are dubious because we only use data for last
5 years. Accordingly, we are set to prepare data for
more than 10 years and do significance test using that
data.
Table 7: Rates of incident occurrence when nurses work in
a "Risky group" (%).
Year Care Pharmacy Tube
2009 21.2 13.6 3.4
2010 18.5 9.2 4.6
2011 19.7 10.6 2.3
2012 23.6 10.8 8.1
2013 13.6 12.6 5.5
Five years 22.2 13.1 5.8
Table 8: Rates of incident occurrence when nurses work in
a "Non-risky group" (%).
Year Care Pharmacy Tube
2009 19.4 10.1 1.6
2010 18.3 7.7 2.6
2011 20.6 9.9 3.0
2012 24.7 6.4 7.8
2013 18.1 18.1 7.8
Five years 20.3 10.0 4.3
Figure 1: Rate of “Care” incident occurrence.
HEALTHINF 2016 - 9th International Conference on Health Informatics
386
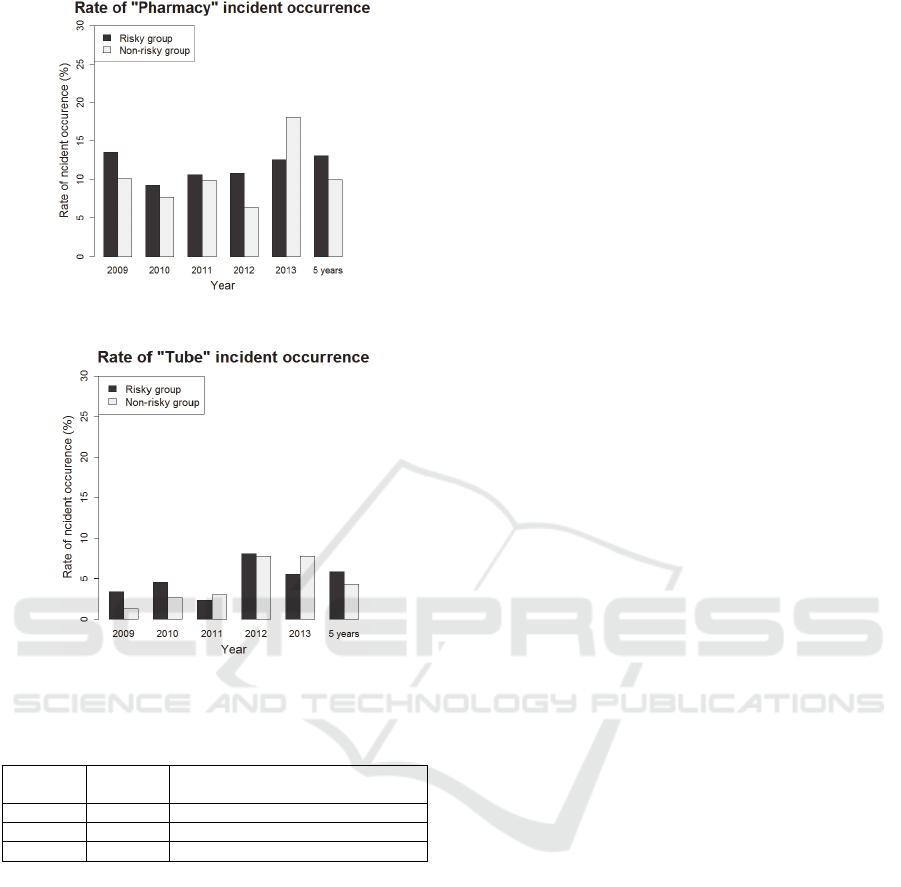
Figure 2: Rate of “Pharmacy” incident occurrence.
Figure 3: Rate of “Tube” incident occurrence.
Table 9: Nurse pairs who did not work together on day and
night shifts during five years.
Type of
shift
Number
of pairs
Number of pairs between the nurses
with ladder level lower than 2
day 117 58
night 34 26
both 24 18
4.2 Extraction of Nurse Pairs Who Did
Not Work Together on Day and
Night Shifts during Five Years
Table 9 shows the results. We gave a breakdown of
the pair between the nurses with ladder level lower
than 2 because the extracted pairs had high
probabilities of causing incidents. We made a roster
devoting attention to these pairs.
5 CONCLUSIONS
As described herein, we sought knowledge to support
production of a nurse roster by analyzing nurse
scheduling data and incident reports from night-work
provided by A General Hospital from a team
viewpoint, reflecting a nurse working style.
Accordingly, we conducted three experiments as
follows from the viewpoint of a team.
Extraction of shift patterns that all nurses meet
working throughout a year
Correlation of incidents and nurse groups on the
night shift
Extraction of nurse pairs with no mutual work on
day and night shifts during five years
In shift pattern extraction, a limitation condition in
roster making and a possible shift pattern were
extracted. The maximum length in each year was
explained using a combination of shift patterns of
length 3. The real incident rate was judged from
viewing 2 in a case of working in the dangerous nurse
group, which was more likely to produce incidents.
Although the rate of the dangerous group was slightly
high, no significant difference was found. Pairs who
did not take day and night duty together during five
years were extracted.
Future studies should examine techniques to
identify shift patterns that are most appropriate as
constraints to roster making by analyzing extracted
shift patterns and correlations with incidents.
REFERENCES
Bates, D. W., Cullen, D. J., Laird, N., Petersen, L. A.,
Small, S. D., Servi, D., Laffel, G., Sweitzer, B. J., Shea,
B. F., Hallisey, R., Vliet, M. V., Nemeskal, R. & Leape,
L. L. 1995. Incidence of adverse drug events and
potential adverse drug events: Implications for
prevention. The Journal of the American Medical
Association, 274, 29-34.
Burke, E. K., Causmaecker, P. D., Berghe, G. V. &
Landeghem, H. V. 2004. The state of the art of nurse
rostering. Journal of Scheduling, 7, 441-499.
Dowsland, K. A. 1998. Nurse scheduling with tabu search
and strategic oscillation. European Journal of
Operational Research, 106, 393-407.
Ikegami, A. 2005 Nurse Scheduling - Site research,
Modeling and Algorithms -. Proceedings of the
Institute of Statistical Mathematics, 53, 231-259.
Ikegami, A., Aizawa, M., Ohkura, M., Wakasa, K.,
Matsudaira, N. & Kosugo, R. 1995. A preliminary study
of the development of a scheduling system for hospital
nurses. Journal of Science of Labour, 71, 413-423.
Ikegami, A., Tanaka, Y. 2014. Re-challenge to the nurse
scheduling problem (in Japanese). The operations
research as a management science, 59, 26-33.
Millar, H. H., Kiragu, M. 1998. Cyclic and noncyclic
scheduling of 12 h shift nurses by network
programming. European Journal of Operational
Extraction of Useful Knowledge for Making Roster by Analyzing Nurse Scheduling Data and Incident Data
387

Research, 104, 582-592.
Miller, H. E., Pierskalla, W. P. & Rath, G. J. 1976. Nurse
scheduling using mathematical programming.
Operations Research, 24, 857-870.
Mizuta, M., Kousaka R., Tsuji, S., Nakano, M. & Inoue, J.
2004. The degree of psychological distress and turnover
wish among new graduate nurses. The bulletin of
Nursing College, Wakayama Medical University, 7, 21-
27.
Onozawa, Y., Yoshioka, N., Kanbayashi, M., Tosaka, K.,
Tamura, T. & Kawaguti H. 2000. A study of incident
on clinical nursing: incident mode and nurses
perceptions. The bulletin of Niigata College of Nursing,
6, 71-90.
Smith-Daniels, V. L., Schweikhart, S. B. & Smith-Daniels,
D. E. 1988. Capacity management in health care
services: Review and future research directions.
Decision Sciences, 19, 889-919.
Tassopoulos, I. X., Solos, I. P. & Beligiannis, G. N. 2015.
A two-phase adaptive variable neighborhood approach
for nurse rostering. Computers and Operations
Research, 60, September 2015, 150-169.
Warner, D. M. 1976. Scheduling nursing personnel
according to nursing preference: A mathematical
programming approach. Operations Research, 24, 842-
856.
Zaki, M. J. 2001. SPADE: an efficient algorithm for
mining frequent sequences. Machine Learning, 42, 31-
60.
APPENDIX
Appendix A: Sample of nurse scheduling data.
2009/04 1 2 3 4 … 30
Shift
total
NurseID -
Ladder
level
Wed. Thurs. Fri. Sat. … Thurs. Day Night … Absence
11111 - 2 PH N N PH … N 10 7 … 0
11122 - 1 N PH D D … PH 12 4 … 0
…
…
…
…
…
…
…
…
…
…
…
…
44111 - 0 D D PH N N PH 7 7 … 0
Shift
total
Day 17 12 15 16 15
Night 7 7 8 6 7
…
…
…
…
…
…
…
Absence 0 0 0 0 0
※ We define Temporary nurse’s ladder level is 0
Appendix B: Sample of incident date data.
2009 Types of incident Date
Care 04/01 04/03 04/10 04/21 05/09 05/13 … 03/12
Pharmacy 05/12 05/27 06/22 06/28 07/05 07/18 … 02/22
Tube 04/21 07/22 08/14 09/04 09/25 10/11 … 02/02
HEALTHINF 2016 - 9th International Conference on Health Informatics
388
