
MyHealthFrame
Design and Evaluation of a Minimally Invasive Communication Platform for
Telemedicine Services Aimed at Older Adults
Mohammad Hossein Nassabi
1
, Harm op den Akker
1,2
, Marian Bittner
1
, Coen Kemerink
2
,
Bert-Jan van Beijnum
1
, Hermie Hermens
1,2
and Miriam Vollenbroek
1,2
1
Telemedicine Group, University of Twente, Enschede, The Netherlands
2
Telemedicine Group, Roessingh Research and Development, Enschede, The Netherlands
Keywords:
Telemedicine, Persuasive Technology, Adherence, Physical Activity.
Abstract:
MyHealthFrame is a communication platform that telemedicine (and well-being) services can leverage to
deliver motivational messages and notifications to their end-users. Instead of being a telemedicine service in
itself, MyHealthFrame is a channel through which external services can reach their users to provide reminders
or deliver simple information such as number of steps. To its end-users, MyHealthFrame is a tablet device
which is designed to be perceived as a photoframe and can be immersed in the users’ living environment. In
this paper, we describe the design and the preliminary assessment of the platform. The results of the feasibility
study with five older adults (65+) are promising.
1 INTRODUCTION
Patient participation is essential to successfully move
care from hospitals to homes. However, the uptake
and adherence to telemedicine systems targeting the
home environment remains poor (McGee-Lennon and
Brewster, 2011). To address this gap, special attention
must be paid to the characteristics of the end-users.
Especially in the case of older adults, not only should
researchers consider the cognitive and physical im-
pairments, but technological literacy and ease of use
also play significant roles in accepting a home-based
system.
Some telemedicine systems support the elderly
in establishing a healthy behavior in order to re-
duce future health complications. Researchers have
been using persuasive technology to promote such
changes to daily living. Virtual activity coaches are
the prime example of systems in which techniques
such as goal-setting, increasing self-awareness and re-
inforcing proper attitudes are used to increase levels
of physical activity. Although the older adults’ atti-
tude towards technology is not uniform, it has been re-
ported that they have greater fear and anxiety of using
computers comparing to other age groups (Barnard
et al., 2013). This can lead to the elderly not being
keen on using technology. In addition, some barriers
can further demotivate the older adult end-user from
accessing the health service. Consider the example of
a web-based rehabilitation service: The elderly has to
turn on his computer, log into the Operating System
(OS), open up the browser and log into the website to
access the rehabilitation service. In a more dramatic
scenario, changes to the elderly’s computer setting
(e.g., software updates) can result in the user becom-
ing discouraged and not using the service at all. This
example can become more complicated if the elderly
has to use more telemedicine systems (and well-being
services) to address the health needs in different do-
mains. Each of these services may also use persuasive
technology to motivate their end-users. However, the
end-users will never receive the persuasive elements
if they stop referring to the corresponding websites or
devices.
The MyHealthFrame platform is designed to facil-
itate long-term communication between telemedicine
systems and end-users who will benefit from the ser-
vices offered by such systems. Therefore, MyHealth-
Frame in itself is not a telemedicine system. How-
ever, it is an always-available communication chan-
nel through which a simplified subset of function-
ality from a telemedicine system is delivered in the
home environment. As such, it can be viewed as a
proxy to the older adults’ daily living. Moreover,
322
Nassabi, M., Akker, H., Bittner, M., Kemerink, C., Beijnum, B-J., Hermens, H. and Vollenbroek, M.
MyHealthFrame - Design and Evaluation of a Minimally Invasive Communication Platform for Telemedicine Services Aimed at Older Adults.
DOI: 10.5220/0005705703220329
In Proceedings of the 9th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2016) - Volume 5: HEALTHINF, pages 322-329
ISBN: 978-989-758-170-0
Copyright
c
2016 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

the platform can be employed as a hub for collect-
ing sensor data and passing this data to suitable ex-
ternal services. MyHealthFrame, with its ubiquitous
front-end, attempts to overcome barriers to initiating
service use by: (1) Reminding the user about the ex-
istence of the external services by delivering the per-
suasive elements generated by them and (2) Present-
ing simple information originating from the external
services. Consequently, MyHealthFrame has the po-
tential to yield higher user engagement and possibly
long-term adherence to the offered services.
In this paper, we discuss the design, develop-
ment and preliminary assessment of MyHealthFrame.
The assessment will be done for services targeting
the physical domain with which the older adults can
achieve a physically active lifestyle.
2 BACKGROUND
To the best knowledge of the authors, no ICT sys-
tem similar to MyHealthFrame—as a channel to de-
liver persuasive elements from external health ser-
vices to older adult end-users—exists. The type of in-
formation delivered via MyHealthFrame is mainly re-
lated to health persuasion. Therefore, in this section,
we briefly describe persuasive technology and sub-
sequently present several systems that promote self-
management and harness persuasive elements to es-
tablish healthy behavior change. These systems have
been evaluated by either patients or healthy subjects.
Our main interest here is to explore the opportunities
for the delivery of persuasive content to older-adult
end-users.
2.1 Persuasive Technology
Persuasive technology is defined as the study of inter-
active systems designed to deliver attitude or behav-
ior change. Studies regarding the technology have al-
ready been performed in various domains such as ed-
ucation, marketing, safety, entertainment and health,
where the latter has attracted most contributions.
(Oinas-Kukkonen and Harjumaa, 2009) present
a Persuasive System Design (PSD) model in which
persuasive techniques are classified into four cate-
gories: (1) Primary Task Support, which are tech-
niques that help users perform the main activity and
achieve their goals; examples include personaliza-
tion and self-monitoring; (2) Dialogue Support, ad-
dressing computer-human interaction bearing in mind
similarities to human interactions such as reminders,
praise, feedback and rewards; (3) Credibility Support
to promote the user’s trust in the system for exam-
ple, verifiability and trustworthiness; and finally (4)
Social Support Techniques, leveraging the social fac-
tors to increase system’s persuasiveness by compe-
tition, recognition and normative influence (namely,
peer pressure).
2.2 Self-management Promoting
Systems
A well-known category of persuasive systems are vir-
tual activity coaches in which a pedometer or an ac-
celerometer sensor is used to measure physical ac-
tivity so that the intervention can be adjusted ac-
cordingly. For example, in Fish’n’steps (Lin et al.,
2006), a virtual pet is presented on a fixed LCD dis-
play whose life state is dependent on the user’s ac-
tivity. In Ubifit Garden (Consolvo et al., 2008), the
authors use a PDA mobile device to depict a garden
metaphor in which the number of flowers increases
as a result of achieving activity goals. In Flowie (Al-
baina et al., 2009), a flower metaphor representing the
end-user’s physical performance is provided through
a photoframe device. Extra user interfaces have also
been introduced for goal-setting. The authors evalu-
ated the prototype in a panel consisting of two older
adults (aged 65+). The results showed that the panel
had a positive attitude toward adopting the system.
Some systems have used the TV as their ser-
vice delivery medium. In (Giordano et al., 2009), the
Philips Motiva system was connected to patients’ TV
through which the educational videos were shown.
The authors in (Stojmenova et al., 2013) used an in-
teractive TV to increase adherence to medication by
sending reminders. However, an intrinsic problem
with systems employing TV as their medium is the
communication loss when the TV is off.
Beside the more conventional modalities, re-
searchers have also used robots to provide health ser-
vices. For example, in (Johnson et al., 2014), a so-
cially assistive robot was integrated into a smart home
to support the elderly’s independent living. However,
the long-term acceptance of such robots has scarcely
been studied (de Graaf et al., 2015).
The above-mentioned studies show the range of
different options that can be chosen as delivery de-
vice in telemedicine systems. We can consider multi-
ple criteria to compare various options and choose the
most suitable device for a given application. Portabil-
ity, Affordability, Availability, Information Richness
(op den Akker et al., 2014), Computation Power, Re-
quired Infrastructure, Learning Curve and Interaction
Type can be named as some criteria for consideration.
MyHealthFrame - Design and Evaluation of a Minimally Invasive Communication Platform for Telemedicine Services Aimed at Older
Adults
323
3 CONCEPT OVERVIEW
Our aim in this research was to design an afford-
able interaction device that could be immersed in the
home. This led on from previous research indicating
that the homes of the elderly can be an ideal loca-
tion for providing persuasive elements (Cabrita et al.,
2015). We ruled out mobile devices as we could not
find strong evidence of elderly preference for such de-
vices in home-based systems (McGee-Lennon et al.,
2012). Moreover, we selected a photoframe represen-
tation for the end-user device as it seems to easily be-
come a natural part of the existing living environment.
This kind of end-user device has already been inves-
tigated with older adults (or with their caregivers) in
(Mynatt et al., 2001), (Dadlani et al., 2010) and (Al-
baina et al., 2009).
MyHealthFrame provides a single point of refer-
ence for the older adult end-users via which motiva-
tional messages, reminders and feedback are commu-
nicated.
Fitbit server
0
MyHealthFrame
Server
Reminders and
motivational
content
Reminders and
motivational
content
Physical
activity data
GNPT
cognitive trainer
Reminders,
feedback,
images,
notifications
MyHealthFrame
Tablet
Pre-frail elderly
CoCo
physical trainer
Figure 1: MyHealthFrame presents the motivational mes-
sages to the older adult end-user.
To its end-users, MyHealthFrame is a tablet de-
vice, designed to be perceived as a digital photoframe.
The tablet requires minimal explicit user interaction
and is placed at a location that is easily accessible
by the elderly end-user. When idle, it can show im-
ages of family members or delightful scenery to im-
prove the the elderly’s mood and mental state. Exter-
nal telemedicine systems can trigger the tablet to con-
vey persuasive elements to the elderly. In addition, the
tablet can transmit sensor data to the relevant external
systems.
The first major exploitation of the platform will
be in the PERSSILAA project in which multiple
electronic health services in the domains of phys-
ical, cognitive and healthy nutrition are offered to
pre-frail community dwelling older adults. Partici-
pants in PERSSILAA use their personal computers
to access electronic health services (some of which
are shown in Figure 1) to train and thereby improve
their health. For example, PERSSILAA users follow a
12-week physical exercise program on the Condition
Coach (CoCo) system: a web-based physical trainer
allowing the elderly to perform exercises in their
home setting (Tabak et al., 2014). Moreover, cognitive
exercises are provided through the Guttmann Neurop-
ersonal Trainer (GNPT) which is a Java-based desk-
top application (Solana et al., 2015). The users are
also provided with Fitbit sensors to track their physi-
cal activity.
4 REQUIREMENT ELICITATION
The main functional requirements considered for the
MyHealthFrame platform are listed below. Not all
the functional requirements have been implemented
in the first prototype.
1. An external telemedicine (or well-being) service
can register itself with the platform.
2. The end-users can register themselves with the
platform by providing the credentials for the ex-
ternal services.
3. An external service can send motivational items
via the platform to registered end-users.
4. The platform queues messages based on their pri-
ority.
5. The end-user tablet filters the received messages
based on their validity period.
6. The platform collects sensor data and sends it to
the corresponding services.
7. The platform can update parts of the user interface
in the tablet to present simple information such as
step count originating from the external services.
We took a user-centered approach while design-
ing the first prototype of the system for requirements
related to end-users. Initially, we presented the con-
cept and ideas regarding to MyHealthFrame to a focus
group consisting of four older adults aged between
65 and 75. Subsequently, the participants were asked
several questions about the concept and the features
they would like to see included in the prototype. All
participants mentioned that they would place such a
solution in the living room for example, next to the
TV, and some mentioned that they would favor the in-
clusion of a clock and an overview of their physical
activity. The focus group was also asked to give their
preferences for the activity sensor and all stated that
they would like to use it to record their daily move-
ment level.
HEALTHINF 2016 - 9th International Conference on Health Informatics
324
5 PROTOTYPE DESIGN AND
IMPLEMENTATION
The first prototype was built to assess the feasibility
and potential uptake of the solution by older adults.
5.1 System Architecture
The architecture used in the prototype is shown in
Figure 2. The user can interact with external ser-
vices via their proprietary browser-based applica-
tions. The Java programming language is used to de-
velop the required JSON-RPC 2.0 web-services ex-
posed by MyHealthFrame server. Since the CoCo
physical trainer’s functionality to generate motiva-
tional messages is under development, we created a
back-end control panel (i.e., caregiver user interface)
that allows an experiment conductor to inject motiva-
tional items into the system.
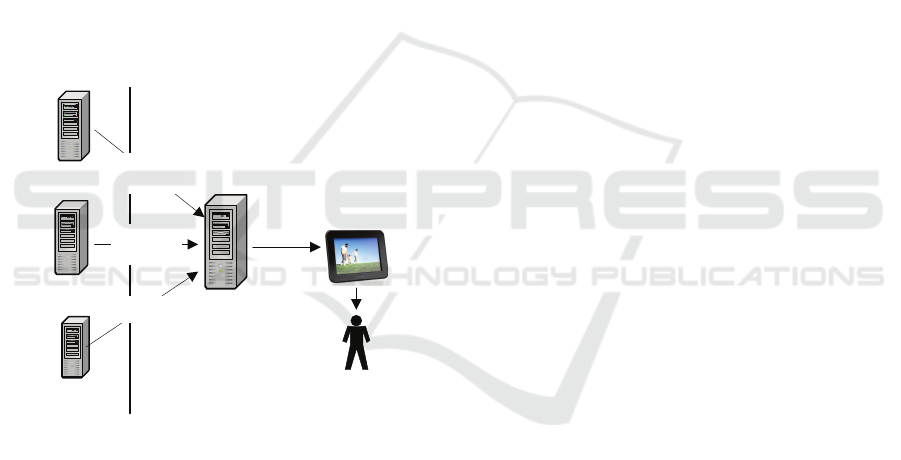
Figure 2: The push mechanism is used to communicate per-
suasive elements to the MyHealthFrame tablet.
In the prototype implementation, we have used
the Google Cloud Messaging (GCM) service to push
items to the tablet. The decision was made to accel-
erate the development process. Moreover, the tablet
is set to pull sensor data (i.e., step count) every 15
minutes using the Bluetooth protocol. However, the
successful synchronization of the accelerometer data
depends on: (1) the proximity of the sensor and the
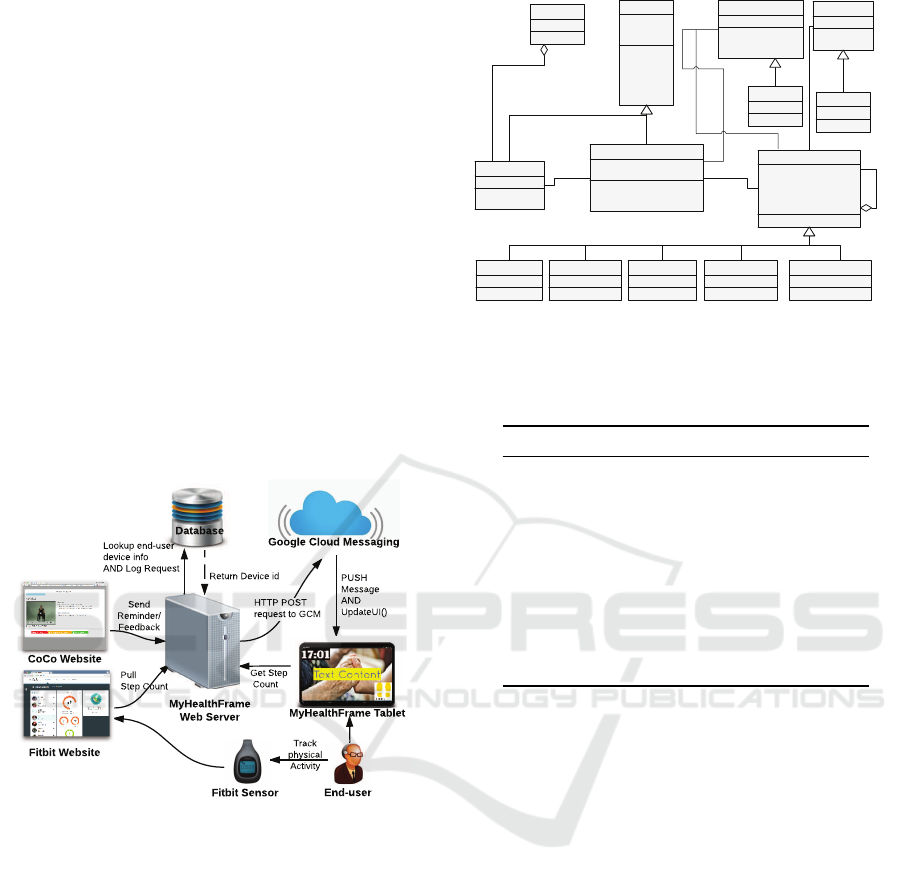
tablet; and (2) the sensor not being idle. The classes
in the back-end that are defined for communicating
with the tablet are shown in Figure 3. Despite consid-
ering a single device per user for our first prototype,
the software architecture allows for multiple user de-
vices.
Each message sent to the tablet is defined as an
ActionMessage object containing a pair of action type
(e.g., image) and content (i.e.,parameters). After ver-
+getAge()
+getEmail()
+getGender()
+setAge()
+setEmail()
+setGender()
-age
-gender
-email
Person
+getReceivers()
+sendAction()
-receivers : Receiver
Sender
+executeActions()
+setDevices()
+addAction()
-devices : IDevice
-actionMessages : ActionMessage
Receiver
+handle()
-externService : IExternService
-successor : ActionMessage
-targetDevice : IDevice
-requestedAction : string
-requestedContent : string
ActionMessage
*
1
DialogActionHandlerTextActionHandler MarqueeActionHandler
+addContent()
+sendAllActions()
IExternService
1
-successor
0..1
-sender1
1
+isActionAllowed() : bool
+getId()
+setId()
-Id
IDevice
AndroidDevice
1
*
GoogleCloud
1
0..*
+sendAction()
HFService
*
AlertActionHandlerImageActionHandler
Figure 3: Extensibility and multiple end-user devices were
considered when designing the system.
Table 1: The various types of messages that can be sent to
the MyHealthFrame tablet.
Type Parameters
Image imageAddress, playMusic?
Text messageText, position
fontSize, fontType
fore/background colour
MarqueeText Same as a text message plus
numberOfRepititions
Dialog messageText, dialogDuration
Voice messageText, voiceGender
voiceSpeed
GetDisplayedData No Parameters
ResetFrame No Parameters
ifying that the end-user’s device is capable of exe-
cuting the requested ActionMessage, the message is
transmitted via the GCM service.
5.2 Communicated Items
A communicated item can be an image, a textual item,
a marquee text, a voice message and a dialog item. In
case of the later, a user dialog is shown on the tablet
that requires the user to press a button.
Each item can be parametrized according to its
type, thereby allowing for some levels of customiza-
tion. For example, if a text message is sent, beside
the content, the text location, size and color can be
adjusted. As another example, each image can be ac-
companied by a random music sample 10 seconds
long.
Table 1 lists the message types implemented in the
first prototype. The last two types were added to help
the experiment conductor to verify that the tablet is
always in a consistent state.
MyHealthFrame - Design and Evaluation of a Minimally Invasive Communication Platform for Telemedicine Services Aimed at Older
Adults
325
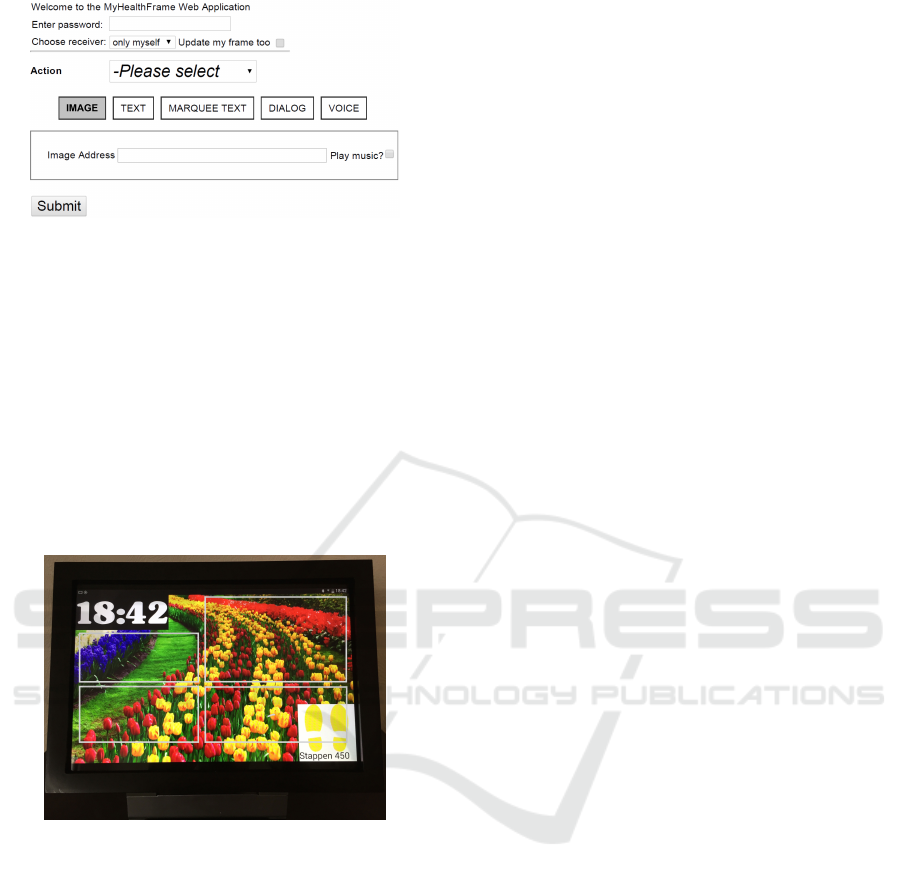
Figure 4: Message parameters can be set via the caregiver
user interface.
5.3 User Interfaces
Two user interfaces (UI) were designed for the first
prototype. The caregiver UI shown in Figure 4 is a
secure website that the authenticated study conductor
can use to send items to the elderly’s tablet. Following
the successful transmission, a notification is provided.
The care receiver UI is the interface designed for
older adults. This interface is integrated in an Android
application. The application cannot be closed unless
the tablet is out of power.
Figure 5: The implemented Android app on MyHealth-
Frame tablet is always running and cannot be closed.
Textual messages can be rendered in either of the
four boxes shown in Figure 5. The strong contrast
between the white number and the black background
makes it easy to read the time. The step counter in the
lower right corner shows the latest received number
of steps for the Fitbit sensor. The shoe color changes
from yellow to green if the step count is higher than a
pre-defined threshold.
6 EVALUATION
We investigated the feasibility of MyHealthFrame
in a small exploratory study. The only external
telemedicine system based on which motivational
content was communicated was the browser-based
CoCo physical exercise trainer. This system provides
a set of exercises in the form of narrated videos ac-
companied by textual descriptions. Each exercise set
consists of a warm-up, main phase and cool-down
stage containing four, nine and four exercises respec-
tively. The participants had to use their own comput-
ers to access the physical trainer. Step counts were
collected using the Fitbit Zip sensor given to each par-
ticipant.
CoCo’s motivational message-generator service is
currently under development. Therefore, this study
was done as a Wizard of Oz experiment: the partic-
ipants were told that an intelligent system communi-
cates with them through the tablet, although in real-
ity, a nursing student was sending messages based on
participant’s activity levels and their progress in the
physical trainer.
6.1 Study Protocol
The goal of the study was to evaluate the feasibility
of MyHealthframe with a group of older adults and to
collect their feedback about the system. The study du-
ration was three weeks and consisted of two phases.
The data collected during the initial phase (first two-
weeks) was used as a baseline for sending persuasive
elements in the the second phase (last week) of the
study. During the registration meeting, the research
conductor explained the goal of the research and col-
lected the signed informed consent form. Moreover,
the participants filled in a short questionnaire about
their physical activity levels and were given access
to the CoCo physical trainer. The participants were
asked to perform the exercises on the trainer three
times per week using their notebook computers. The
Fitbit sensors were given to participants in the same
day. In the third week, the participants were provided
with the tablets for a one week period.
At the end of the study, the nursing student held
an interview with the participants asking them to
fill in the Computer System Usability Questionnaire
(CSUQ) (Lewis, 1995) containing 19 items on over-
all system usability (OVERALL), system usefulness
(SYSUSE), information quality (INFOQUAL) and
interface equality (INTERQUAL). The items can be
answered using 7-point Likert scales, ranging from
”Strongly agree” with one point to ”Strongly dis-
agree” with seven points, and an additional Not Ap-
plicable (N/A) point. Moreover, to collect further in-
formation regarding user acceptance, the six extra
questions listed below were asked during the inter-
view of which some focused on the feedback given
and future potential improvements to the system.
1. How was your experience with the system and
HEALTHINF 2016 - 9th International Conference on Health Informatics
326

the provided feedback?
2. What did you learn from the given feedback?
3. What could be improved when giving feedback?
4. Have you benefited from the feedback or
reminders? Please elaborate on your answer.
5. What would you like to change in the system?
6. Would you recommend MyHealthFrame to a
friend? Please elaborate on your answer.
6.2 Participants
Five participants aged between 65-68 were recruited
for the pilot consisting of two couples (Subjects 1 & 2
and Subjects 3 & 4) and a single male subject (Sub-
ject 5). Only four tablets were distributed amongst
the participants resulting in Subjects 1 & 2 receiving
a single tablet.
All of the participants mentioned that they cycled
every day. Three participants mentioned exercising at
a gym or a sport center for a minimum of once per
week e.g., playing tennis. All participants were able
to do daily activities such as shopping and performing
household tasks.
6.3 Communication Timing and
Content
Motivational messages were sent to the tablet both at
fixed and time-varying moments. Based on the time
of the day (morning, noon, evening), three generic im-
ages accompanied by a text were communicated to the
participants e.g., the “Good Morning” message was
sent at 9:00 am. In addition, after performing six (out
of nine) exercises on the CoCo system, positive feed-
back in the form of an image would be sent. More-
over, a motivational message was sent if the number
of steps was more than the average step count for a
specific person (based on two weeks collected data).
If the participant had not been exercising on the
physical trainer and the step count was lower than
5000 steps on a given day, a reminder was sent to the
user to perform physical activity e.g., a textual mes-
sage containing “It is a great day to exercise”.
6.4 Results
The number of steps measured during the study is
shown in Figure 6. The average number of steps in
some cases (e.g., subject 1) is significantly higher than
the recommended 7000-8000 steps for the 65+ age
group. The step counts supports the finding that the
studied participants, other than subject 5, are more ac-
tive than the general population.
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
20000
Subject1 Subject2 Subject3 Subject4 Subject5
Average number of daily steps
With
System
Without System
Figure 6: The average number of daily steps collected from
participants in during the study.
Table 2: Four scores are calculated based on the answers to
the CSUQ usability questionnaire.
Based Average Missing
Score on questions responses value ratio
OVERALL 1 to 19 3.04 0.31
SYSUSE 1 to 8 2.74 0.11
INFOQUAL 9 to 15 3.5 0.56
INTERQUAL 16 to 18 4 0.4
Only one couple (Subject 1 and Subject 2) regu-
larly exercised using the CoCo physical trainer sys-
tem. The other users stated that they were already
physically active which was confirmed by sensor data.
The participants could not provide answers to all
19 questions of the CSUQ questionnaire. Following
the guidelines of (Lewis, 1995), the questionnaire can
be summarized into the four scores listed in Table 2.
This table also contains the ratio for missing values
per score defined using Equation 1:
Missing value ratio=
∑
N/A Answers
#Questions ×#Participants
(1)
Unfortunately questions regarding information
and interface quality seemed ambiguous or not appli-
cable to most participants. However, the SYSUSE
score suggested that the participants were satisfied
with the system.
All participants were satisfied with using the Fit-
bit Zip sensor; indeed, Subject 5 mentioned that he
became more active because of the sensor. Subjects
3 and 4 also stated that presenting the step counts on
the tablet motivated them to compete with each other.
Subjects 1, 2 and 3 mentioned that they liked the
received feedback shown on the tablet. The most ac-
tive participant, Subject 4, did not notice any feed-
back as she was mainly outside doing voluntary work.
Subject 5, the least active participant, could not under-
stand how MyHealthFrame could help him.
MyHealthFrame - Design and Evaluation of a Minimally Invasive Communication Platform for Telemedicine Services Aimed at Older
Adults
327

7 DISCUSSION AND FUTURE
WORK
The acceptance of a computer system is influenced
by multiple factors including user satisfaction, system
usability, perceived ease of use and perceived useful-
ness (Acton et al., 2004). In this feasibility study, we
attempted to collect subjective measurements related
to the usability and usefulness of the MyHealthFrame
platform with a limited number of participants. Even
though the qualitative results regarding system useful-
ness are limited, still they indicate a positive attitude
towards accepting the system.
The low value for information and interface qual-
ity and the corresponding high missing value ratios
in Table 2 suggest that better explanations should be
given about the system and its intended role. Al-
though the participants were given a one-page de-
scription of the overall system at the beginning of the
study, their answers to the extra questions about the
system suggested some levels of confusion. For ex-
ample, one participant suggested improvements to the
CoCo physical trainer despite the fact that the ques-
tion concerned MyHealthFrame. Another reason for
such confusion can be the introduction of CoCo and
Fitbit without taking into account the differences in
the learning abilities of the participants. Therefore,
one inclusion criteria for future studies can be the par-
ticipant’s prior acquaintance with web-based systems
and his or her computer literacy.
The most important consideration for future stud-
ies is the inclusion of participants who benefit most
from the platform. All participants in this study were
moderately to highly active in comparison with peo-
ple in the same age group. Consequently, there was
no need for them to follow the online physical exer-
cises. This inevitably led to fewer feedback moments
related to their progress.
An interesting extension to the platform would
be the addition of competition features for older
adult couples. As stated by two participants, such
functionality could have motivated them to become
more physically active. However, the competition fea-
tures would not need to be limited to physical ac-
tivity and could be generalized to make use of any
health/service information. For example, the user
progress in GNPT cognitive trainer can also be con-
sidered as the competition information source. In this
case, a total score could be aggregated based on scores
in each health domain. Inclusion of such features in a
future prototype would require implementing a light
computation engine in the back-end. Moreover, the
user interface would need to be modified to present
the couple progress in a single tablet.
The calculated total scores can also be used to
implement other game mechanics than (intra-couple)
competition such as leaderboards, challenges, social
networking and awarding points amongst all partici-
pants. For example, a reward scheme can be defined
for end-users motivating them to become more en-
gaged with the external telemedicine systems. The
scheme can reward users in terms of prizes in the form
of electronic badges as done in Fitocracy (Hamari
and Koivisto, 2013) to promote individuals’ achieve-
ments.
Our main focus for next prototypes will be on im-
proving the user interface for participants belonging
to the target group (pre-frail end-users). Specifically,
we plan to perform a task-oriented user study. Par-
ticipants will be asked to perform a pre-defined set of
tasks using MyHealthFrame tablet and will be subse-
quently interviewed and asked to fill in the User Expe-
rience Questionnaire (Laugwitz et al., 2008). Setting
up the study in this way will allow us to compare and
improve various design elements in the system which
can eventually lead to a more effective solution.
The architecture of the platform allows users to
use multiple Android devices. Consequently, it is
possible not only to send messages to the devices at
home but also to communicate with the mobile de-
vices that the user carries. Therefore, as a future ex-
tension, we would like to assess the effectiveness of
cross-platform electronic health content delivery.
After analyzing the log files from the study, some
end-user mistakes when sending messages based on
time of the day were detected (made by the experi-
ment conductor). Therefore, to minimize the human
error in future studies, a scheduler component will be
included in the platform that can be used for fixed
time/rule-based messages.
8 CONCLUSION
In this paper, we have presented MyHealthFrame,
a communication platform that third-party electronic
health service providers can exploit to deliver persua-
sive elements such as motivational messages and re-
minders. The platform can also gather sensor data and
send it to the relevant external services.
The preliminary results from the feasibility study
yielded small yet positive indications. In addition, the
study highlighted essential improvement points for
future evaluations such as a more strict inclusion cri-
teria for participants. The focus of the next study will
be on improvements to usability and collecting more
credible evidence about the platform’s effectiveness.
HEALTHINF 2016 - 9th International Conference on Health Informatics
328

ACKNOWLEDGEMENTS
The authors would like to thank the European Com-
mission for providing the funding of this research
through the PERSSILAA FP7 project. Moreover, the
authors thank Sanne Frazer for her contributions to
the study.
REFERENCES
Acton, T., Golden, W., Gudea, S., and Scott, M. (2004).
Usability and acceptance in small-screen information
systems. In Proceedings of 9th European Collabora-
tive Electronic Commerce Technology and Research
Conference.
Albaina, I. M., Visser, T., van der Mast, C. A., and Vas-
tenburg, M. H. (2009). Flowie: A persuasive virtual
coach to motivate elderly individuals to walk. In Per-
vasive Computing Technologies for Healthcare, 2009.
PervasiveHealth 2009. 3rd International Conference
on, pages 1–7. IEEE.
Barnard, Y., Bradley, M. D., Hodgson, F., and Lloyd,
A. D. (2013). Learning to use new technologies by
older adults: Perceived difficulties, experimentation
behaviour and usability. Computers in Human Behav-
ior, 29(4):1715–1724.
Cabrita, M., Nassabi, M. H., op den Akker, H., Tabak, M.,
Hermens, H., and Vollenbroek, M. (2015). An unob-
trusive system to monitor physical functioning of the
older adults: Results of a pilot study. In International
Workshop on Personalisation and Adaptation in Tech-
nology for Health.
Consolvo, S., McDonald, D. W., Toscos, T., Chen, M. Y.,
Froehlich, J., Harrison, B., Klasnja, P., LaMarca, A.,
LeGrand, L., Libby, R., et al. (2008). Activity sensing
in the wild: a field trial of ubifit garden. In Proceed-
ings of the SIGCHI Conference on Human Factors in
Computing Systems, pages 1797–1806. ACM.
Dadlani, P., Sinitsyn, A., Fontijn, W., and Markopoulos, P.
(2010). Aurama: caregiver awareness for living inde-
pendently with an augmented picture frame display.
Ai & Society, 25(2):233–245.
de Graaf, M. M., Allouch, S. B., and Klamer, T. (2015).
Sharing a life with harvey: Exploring the acceptance
of and relationship-building with a social robot. Com-
puters in human behavior, 43:1–14.
Giordano, A., Scalvini, S., Zanelli, E., Corr
`
a, U., Longob-
ardi, G., Ricci, V., Baiardi, P., and Glisenti, F. (2009).
Multicenter randomised trial on home-based teleman-
agement to prevent hospital readmission of patients
with chronic heart failure. International journal of
cardiology, 131(2):192–199.
Hamari, J. and Koivisto, J. (2013). Social motivations to use
gamification: An empirical study of gamifying exer-
cise. In ECIS, page 105.
Johnson, D. O., Cuijpers, R. H., Juola, J. F., Torta, E., Si-
monov, M., Frisiello, A., Bazzani, M., Yan, W., We-
ber, C., Wermter, S., et al. (2014). Socially assis-
tive robots: A comprehensive approach to extending
independent living. International Journal of Social
Robotics, 6(2):195–211.
Laugwitz, B., Held, T., and Schrepp, M. (2008). Con-
struction and evaluation of a user experience ques-
tionnaire. Springer.
Lewis, J. R. (1995). Ibm computer usability satisfac-
tion questionnaires: psychometric evaluation and in-
structions for use. International Journal of Human-
Computer Interaction, 7(1):57–78.
Lin, J. J., Mamykina, L., Lindtner, S., Delajoux, G., and
Strub, H. B. (2006). Fish’n’steps: Encouraging phys-
ical activity with an interactive computer game. In
Proceedings of the 8th International Conference on
Ubiquitous Computing, UbiComp’06, pages 261–278,
Berlin, Heidelberg. Springer-Verlag.
McGee-Lennon, M., Smeaton, A., and Brewster, S. (2012).
Designing home care reminder systems: lessons
learned through co-design with older users. In Per-
vasive Computing Technologies for Healthcare (Per-
vasiveHealth), 2012 6th International Conference on,
pages 49–56. IEEE.
McGee-Lennon, M. R. and Brewster, S. (2011). Reminders
that make sense: Designing multimodal notifications
for the home. In Pervasive Computing Technologies
for Healthcare (PervasiveHealth), 2011 5th Interna-
tional Conference on, pages 495–501. IEEE.
Mynatt, E. D., Rowan, J., Craighill, S., and Jacobs, A.
(2001). Digital family portraits: supporting peace of
mind for extended family members. In Proceedings of
the SIGCHI conference on Human factors in comput-
ing systems, pages 333–340. ACM.
Oinas-Kukkonen, H. and Harjumaa, M. (2009). Persuasive
systems design: Key issues, process model, and sys-
tem features. Communications of the Association for
Information Systems, 24(1):28.
op den Akker, H., Jones, V. M., and Hermens, H. J.
(2014). Tailoring real-time physical activity coaching
systems: a literature survey and model. User model-
ing and user-adapted interaction, 24(5):351–392.
Solana, J., C
´
aceres, C., Garc
´
ıa-Molina, A., Opisso, E.,
Roig, T., Tormos, J. M., and Gomez, E. J. (2015). Im-
proving brain injury cognitive rehabilitation by per-
sonalized telerehabilitation services: Guttmann neu-
ropersonal trainer. Biomedical and Health Informat-
ics, IEEE Journal of, 19(1):124–131.
Stojmenova, E., Debevc, M., Zebec, L., and Imperl, B.
(2013). Assisted living solutions for the elderly
through interactive tv. Multimedia tools and appli-
cations, 66(1):115–129.
Tabak, M., Brusse-Keizer, M., van der Valk, P., Hermens,
H., and Vollenbroek-Hutten, M. (2014). A telehealth
program for self-management of copd exacerbations
and promotion of an active lifestyle: a pilot random-
ized controlled trial. International journal of chronic
obstructive pulmonary disease, 9:935.
MyHealthFrame - Design and Evaluation of a Minimally Invasive Communication Platform for Telemedicine Services Aimed at Older
Adults
329
