
Generalizing the Detection of Internal and External
Interactions in Clinical Guidelines
Veruska Zamborlini
1,2
, Rinke Hoekstra
1,3
, Marcos da Silveira
2
, Cedric Pruski
2
, Annette ten Teije
1
and Frank van Harmelen
1
1
Dept. of Computer Science, VU University Amsterdam, Amsterdam, The Netherlands
2
LIST Luxembourg Institute of Science and Technology, Esch-sur-Alzette, Luxembourg
3
Faculty of Law, University of Amsterdam, Amsterdam, The Netherlands
Keywords:
Clinical Guidelines, Semantic Web, Knowledge Representation, Ontologies.
Abstract:
This paper presents a method for formally representing Computer-Interpretable Guidelines to deal with mul-
timorbidity. Although some approaches for merging guidelines exist, improvements are still required for
combining several sources of information and coping with possibly conflicting pieces of evidence coming
from clinical studies. Our main contribution is twofold: (i) we provide general models and rules for represent-
ing guidelines that expresses evidence as causation beliefs; (ii) we introduce a mechanism to exploit external
medical knowledge acquired from Linked Open Data (Drugbank, Sider, DIKB) to detect potential interactions
between recommendations. We apply this framework to merge three guidelines (Osteoarthritis, Diabetes, and
Hypertension) in order to illustrate the capability of this approach for detecting potential conflicts between
guidelines and eventually propose alternatives.
1 INTRODUCTION
Clinical Guidelines (CG) are developed for support-
ing physicians decision, e.g. specifying what treat-
ment work best in what situation (Peleg, 2013).
When possible, the recommendations provided by
CGs are based on evidence from clinical researches.
In this case, there is a direct mapping to the clini-
cal evidence that describes the effects (transitions)
of certain care action (e.g. do not administer aspirin
because of an increased risk of gastrointestinal bleed-
ing). Since an evidence is not a fact, a multitude of
evidence rating systems (Lohr, 2003) are adopted by
CGs authors. Epistemologically, an evidence reflects
a belief in the existence of a causal relation between
e.g. administering aspirin and gastrointestinal bleed-
ing. Furthermore, CGs are targeted to the treatment of
a specific illness. However, it is quite common to have
patients with multiple diseases (multi-morbidity) that
need to be addressed according to different CGs. For
example, according to (Barnett et al., 2012), around
40% of 55 years old patients suffer from at least 2 dis-
eases, and 20% of 70 years old patients suffer from
at least 4 diseases in Scotland. As with any large
volume of regulations, combined guidelines almost
inevitably involve intricate interactions between the
recommendations they describe. Finding interactions
(like potential conflicts) requires intensive collabora-
tion in multidisciplinary teams.
Computational support can be of great value for
supporting physicians to handle all this complexity.
Many languages have been proposed for representing
“computer interpretable” guidelines (CIG) and rea-
soning about it (Peleg, 2013). However, the con-
cepts here discussed are poorly or not addressed by
those approaches. The main reason is because much
has been devoted to executing guidelines within treat-
ments rather than other purposes such as combining
and updating CGs. In particular, regarding the issue
of multimorbidity, existing approaches for combin-
ing CGs are limited in their ability to automatically
detect the interactions, propose alternatives or com-
bining more than two guidelines (Zamborlini et al.,
2015b).
This work follows an incremental methodology.
We start by addressing realistic but simplified case
studies, and add more complexity according to the
lessons learned in each iteration. Therefore, this paper
is the continuation of earlier work reported in (Zam-
Zamborlini, V., Hoekstra, R., Silveira, M., Pruski, C., Teije, A. and Harmelen, F.
Generalizing the Detection of Internal and External Interactions in Clinical Guidelines.
DOI: 10.5220/0005704101050116
In Proceedings of the 9th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2016) - Volume 5: HEALTHINF, pages 105-116
ISBN: 978-989-758-170-0
Copyright
c
2016 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
105

borlini et al., 2014a; Zamborlini et al., 2014b; Zam-
borlini et al., 2015b; Zamborlini et al., 2015a). In this
series of work, we investigated (i) what knowledge
is required to represent and reason about CGs (rather
than how to acquire such knowledge), particularly for
supporting the multimorbidity issue; (ii) how it can
be formalized; (iii) how it can be implemented using
Semantic Web technologies, so that (iv) we can ex-
ploit the medical knowledge available as Linked Open
Data (LOD). As a consequence, the results we obtain
are limited to the current expressiveness of the model,
e.g. temporal aspects and related interactions will be
addressed in future iterations.
This paper reports on improvements to both the
models and the implementation to better address the
issue of multimorbidity. The contributions are (C1)
a more generic version of the models with respect to
recommendations, beliefs and event types. This in-
cludes (C2) a formalization of the improved models
and rules in FOL; and (C3) a Semantic Web frame-
work for representing and reasoning about recom-
mendations and beliefs using standard vocabularies.
This provides (C4) a flexible mechanism for reusing
external knowledge bases to extend our ability to
detect interactions (showcased using DrugBank and
Sider).
The remainder of this paper is as follows: Sect. 2
presents a case study to illustrate the main concepts,
which are further defined in the models and rules, fol-
lowed by their implementation. An experimental as-
sessment shows the results obtained for the referred
case study in Sect. 3. The related work is discussed
in Sect. 4 and the main contributions and future work
are discussed in Sect. 5.
2 THE MODELS & FRAMEWORK
This section describes our case study, as well as
the adapted version of the TMR (Transition-based
Medical Recommendation) models and their semantic
web-based implementation as a framework for repre-
senting norms (recommendations) in the clinical do-
main and reasoning about interactions among them.
2.1 Case Study
This case study is meant for illustrating the concepts
previously mentioned and further defined in the next
section. It concerns the combination of three guide-
lines, namely Osteoarthritis (OA), Diabetes (DB) and
Hypertension (HT), and the detection of interactions
among them (adapted from (Jafarpour, 2013)). The
recommendations, depicted in Fig. 1, are:
Diabetes (DB)
1. Should adm. NSAID to reduce blood coagulation
2. Should adm. Tramadol to reduce blood coagulation
3. Should adm. Insulin to reduce blood sugar level
Osteoarthritis (OA)
1. Should NOT administer Aspirin to avoid increasing
the risk of gastrointestinal bleeding
2. Should administer Ibuprofen to reduce pain
Hypertension (HT)
1. Should adm. Thiazide to reduce the blood pressure
Among them some interactions can be identified:
Internal Interactions:
1. DB.1 and DB.2 are alternative recommendations
meant for promoting the same effect.
2. DB.1 and OA.1 are contradictory recommendations
since the first might lead to the prescription of As-
pirin which is non-recommended by the later.
External Interactions (from external knowledge sources):
1. DB.1 and DB.2 both have as external alternative Ad-
minister Epoprostenol to achieve the desired effect
according to DrugBank.
2. DB.2 and OA.2 recommend incompatible actions ac-
cording to Drugbank
3. DB.3 and HT.1 interact since the latter might lead to
prescription of bendroflumethiazide, which has high
blood sugar level as side effect according to Sider,
as opposed to goal in the former.
4. HT.1 and OA.2 interact since the latter has high
blood pressure as side effect according to Sider, as
opposed to goal in the former.
5. (others)
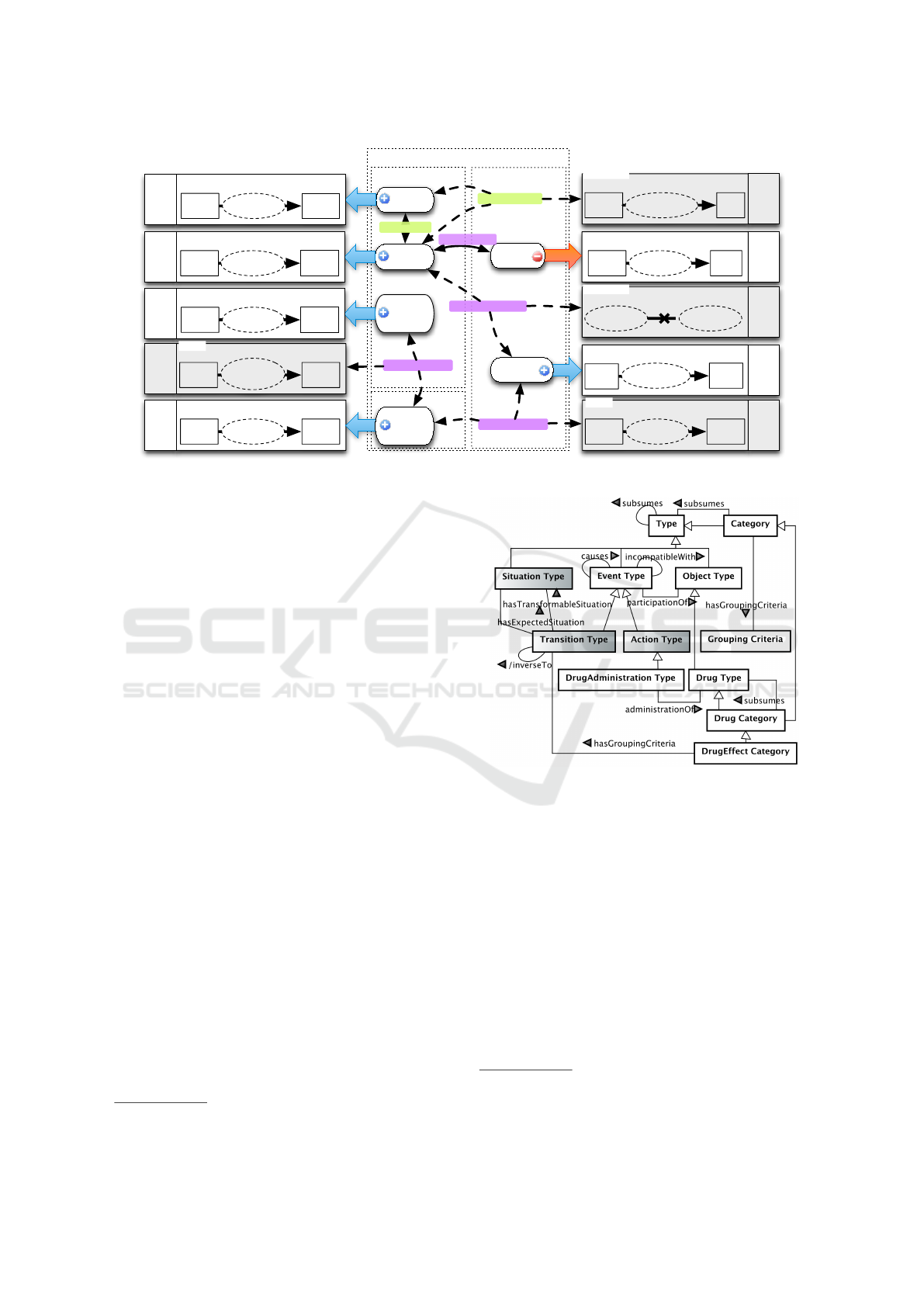
In Fig. 1 the big rectangles in both left and right
sides represent beliefs regarding the care actions (ad-
ministering tramadol). The latter is represented as
dotted ellipses inside the beliefs. The causation be-
liefs are about a transition between situations (blood
coagulation goes from normal to low) that are be-
lieved to be promoted by executing a care action
type). The causation belief has a frequency e.g. ad-
miniter tramadol always reduce the blood coagula-
tion. For sake of simplicity, we consider in this work
only always as frequency for all causation beliefs.
They also have a strength associated, which corre-
sponds to the evidence level (e.g. high level), accord-
ing to the quality attributed to the sources (or stud-
ies) that provide such knowledge. The beliefs in gray
shade represent the knowledge imported from an ex-
ternal source described in the top left (e.g. Drug-
Bank). The strength in this case will depend on the
reliability of each data source. The external sources
here considered describe two types of beliefs: causa-
tion belief or incompatibility belief. The latter repre-
sents action types that should not be recommended to-
gether, e.g. Administer Aspirin is incompatible with
HEALTHINF 2016 - 9th International Conference on Health Informatics
106
HT
DB
OA+HT+DB Guideline Transitions by Care Actions
Avoid
Thrombi
should
Blood Coagulation
low
Administer
NSAID
normal
Reduce
Blood
Sugar Level
should
Blood Sugar Level
normal
Administer
Insulin
high
OA
Pain
no
pain
Administer
Ibuprofen
pain
should
Heal Pain
Avoid
Thrombi
should
Blood Coagulation
low
Administer
Tramadol
normal
Transitions by Care Actions
alternative
extIncompEffect
extIncompEffect
extAlternative
Blood Coagulation
low
Administer
Epoprostenol
normal
Blood Pressure
high
Administer
Ibuprofen
??
Incompatibility
Administer
Aspirin
Administer
Ibuprofen
extIncompActions
[DrugBank]
[DrugBank]
[Sider]
Blood Sugar Level
high
Administer
bendroflume
thiazide
??
[Sider]
Blood Pressure
low
Administer
Thiziade
high
should
Reduce
Blood
Pressure
Gastrointestinal Bleeding
high
risk
Administer
Aspirin
low
risk
shouldn't
Avoid
Bleeding
contradiction
high
level
med.
level
med.
level
med.
level
high
level
low
level
always
low
level
med.
level
med.
level
low
level
Figure 1: Case study on combining guidelines for OA+HT+DB.
Administer Ibuprofen (the reason is not provided in
structured way from the sources).
The dotted rectangles in the middle represent the
guidelines. The more external one is the merge of
the three guidelines for OA+HT+DB. They comprise
both the recommendations (e.g. avoid thrombi) and
the interactions alternative among them. The former
is represented as rounded rectangles, and the latter is
depicted by labelled thin arrows connecting the inter-
acting recommendations and beliefs. Solid arrows are
for internal interactions and dotted arrows for exter-
nal ones. A positive (or negative) recommendation is
indicated by a thick arrow labeled with “should” (or
“should not”).
2.2 Conceptual Model & Rules
Figure 2 presents a UML class diagram for the
T MR
Event
model describing some relevant concepts
and relations regarding event types in the scope of
this work. The concepts introduced in previous ver-
sions of the models are depicted in gray-shade (same
for the next diagrams). This model is inspired in UFO
(Unified Foundational Ontology) (Guizzardi et al.,
2013) that is a formal theory describing some of the
general concepts used here, namely Type (Universal)
and Category, as well as Object, Event, Action and
Situation Types. The model regards mostly types of
things
1
since it is meant for modeling, for example,
the type of event that is expected as consequence of
another one, rather then the particular event that was
the consequence of another particular one. In other
words, we do not want to say that John’s pain was re-
1
For sake of simplicity we can omit the word ‘type’.
Figure 2: UML class diagram for the T MR
Event
Model.
lieved due to the administration of aspirin, but that ad-
ministering aspirin often relieves the pain of patients
2
.
While action types concern event types to be per-
formed by an intentional agent (omitted in the model),
transition types concern (deterministic) event types
for which pre and post situation types can be de-
fined
3
. In other words, it represents the transforma-
tion of a situation type into another (transformable
& expected situations). An event type can be de-
fined as the participation of a certain object type,
e.g. a DrugAdministration type is the administration
of (participation of) a Drug type. An event type can
cause another event type to happen (occurrence of
one causes the occurrence of the other). Moreover,
2
For a deeper explanation see (Zamborlini et al., 2014a).
3
We do consider some event types are non-deterministic
or non-intentional, but this is out of scope of this work.
Generalizing the Detection of Internal and External Interactions in Clinical Guidelines
107

an event type can also be incompatible with another
one when they can not or should not occur together.
In other words, either happening together is not pos-
sible or would bring about results/transitions that are
not the expected ones.
A category is a type that (transitively) subsumes
(or regroups) other types according to a grouping cri-
teria, e.g. ThiazideDrug is a category of drugs that
contains the molecule thiazide, e.g. bendroflumethi-
azide. In this case the grouping criteria regards a
structural property. However, it can also concern the
effect expected to be promoted, e.g. NSAID is the cat-
egory for the (non-steroidal) drugs expected to pro-
mote the transition reduce inflammation, e.g. Aspirin.
FOL rules are provided for deriving relations rel-
evant in the context of this work. Some relations
are defined in terms of other relations, for example,
inverseTo between transition types is one transition
that ‘undo’ the effect of the other. These relations
are preceded by a slash in the models (previous and
forthcoming). Other relations can be propagated, e.g.
the grouping criteria of an object category (Analgesic
Drug) is the grouping criteria of the event category
of administering such object (Adm. Analgesic) and
vice-versa.
Inverse Transitions: one transition type t1 trans-
forms situation s1 into s2 while another transition
t2 transforms s2 into s1.
R.1 ∀t1, t2, s1, s2 TransitionType(t1)∧ TransitionType(t2)
∧ SituationType(s1) ∧ SituationType(s2) ∧ s1 6= s2
∧ hasTransformableSituation(t1,s1)
∧ hasExpectedSituation(t1,s2)
∧ hasTransformableSituation(t2,s2)
∧ hasExpectedSituation(t2,s1))
→ inverseTo(t1,t2)
Propagating grouping criteria via administra-
tionOf: if an action type a1 is the administration
of a drug type d1, a transition type t1 is the group-
ing criteria for d1 iff it is also for a1.
R.2 ∀a1, d1, t1 (ActionType(a1) ∧ DrugType(d1)
∧ TransitionType(t1) ∧ administrationOf(a1,d1))
→ ( hasGroupingCriteria(d1, t1)
↔ hasGroupingCriteria(a1, t1))
Other relations can be difficult to be precisely de-
fined either for epistemic or ontological issues. For
instance, some event types might not have a precise
definition of their consequences, e.g. administering
aspirin sometimes relieves the pain, sometimes it does
not. We address this issue in the T MR
Belie f
model
by representing those relations through beliefs, pre-
sented in a UML class diagram in Fig. 3. In this
work, beliefs allow to represent a ‘degree of truth’ for
assertions about things/entities according to a source.
Figure 3: UML class diagram for the T MR
Belie f
Model.
‘M1’ is used as short reference for T MR
Event
.
It allows for complementary beliefs, e.g. aspirin re-
lieves the pain in 80% of the cases (therefore it does
not in 20%), but also for inconsistent ones, e.g, ad-
ministering aspirin always relieves the pain and it
never relieves the pain. This is a desired feature since
for some assertions there can be no common agree-
ment from different sources (see (Zamborlini et al.,
2015a)). However, we consider that one (merged)
guideline that rely on incompatible beliefs is then in-
consistent. We also account for the certainty/quality
of the belief as its strength, such as the evidence level
classification in clinical guidelines.
We are particularly interested in beliefs about
the relations causes, subsumes and incompatibleWith
between event types, for which we provide ‘epis-
temic/doxastic’ versions (represented as dotted lines
in the model). In other words, they are relations de-
pendent on the existence of a belief to ground their
truthfulness (in practice they have a belief as a third
argument). Therefore, they are not the same as the
ones in Fig. 2.
The causation belief between event types reflects
the likelihood/frequency (probability) of one causing
the another according to a source. In this work we fo-
cus on beliefs about action (hasAsCause Action Type)
causing transitions (hasAsEffect Transition Type) as
justification for the clinical recommendations. More-
over, for the interaction rules we consider only the
positive causation beliefs, i.e., an action type always
cause a transition, since it is not on the scope of this
work both (i) the negative causation, which only ap-
pears as sub-justifications of recommendation (dis-
cussed in (Zamborlini et al., 2015a)) and (ii) the in-
termediate frequency values (often, rarely, etc)
4
. In its
turn, the incompatibility between event types is con-
sidered in this work to be given as an assertion. There-
fore it is represented as a belief, although it could be
explained/derived at a certain level of granularity. Fi-
4
This approach exclude endless assertions about all the
effects an event is not expected to produce since the beliefs
are defined in CGs or scientific papers by a community of
experts, e.g. cancer is not an effect of a certain drug.
HEALTHINF 2016 - 9th International Conference on Health Informatics
108
nally the subsumption of event types due to expected
effect also relies on beliefs, namely the causation one.
Causation - an event type e1 causes another one e2
with a certain frequency f according to a belief cb:
R.3 ∀e1, e2, cb, f (EventType(e1) ∧ EventType(e2)
∧ CausationBelief(cb) ∧ hasAsCause(cb, e1)
∧ hasAsEffect(cb, e2)) ∧ frequency(cb, f)
→ causes(e1,e2, f, cb)
Similar Causation Beliefs: two beliefs cb1, cb2
about different event types e1, e2 promoting with
same frequency f another event type e3.
R.4 ∀cb1, cb2, e1, e2, e3, f causes(e1, e3, f, cb1)
∧ causes(e2, e3, f, cb2) ∧ cb1 6= cb2 ∧ e1 6= e2
→ similarTo(cb1,cb2)
Propagating causation via hasGroupingCriteria:
If an event type e1 has as grouping criteria a tran-
sition type t1 then e1 must cause t1
R.5 ∀e1, t1 (EventType(e1) ∧ TransitionType(t1)
∧ hasGroupingCriteria(e1, t1))
→ ∃cb causes(e1, t1, ‘always’, cb)
Deriving Subsumption via causation and group-
ing criteria: if an event type e1 causes a transi-
tion t1 that is the grouping criteria of another event
type e2 then e2 subsumes e1 according to the cau-
sation belief.
R.6 ∀e1, e2, t, cb1 (EventType(e1) ∧ EventType(e2)
∧ TransitionType(t) ∧ causes(e1, t, ‘always’, cb1)
∧ hasGroupingCriteria(e2, t) ∧ e1 6= e2)
→ ∃cb subsumes(e2, e1, cb1)
Incompatible Event Types: event type e1 is be-
lieved be incompatible with another one e2.
R.7 ∀e1, e2, ib (EventType(e1) ∧ EventType(e2)
∧ IncompatibilityBelief(ib) ∧ about(ib,e1)
∧ about(ib,e2))
→ incompatibleWith(e1, e2, ib)
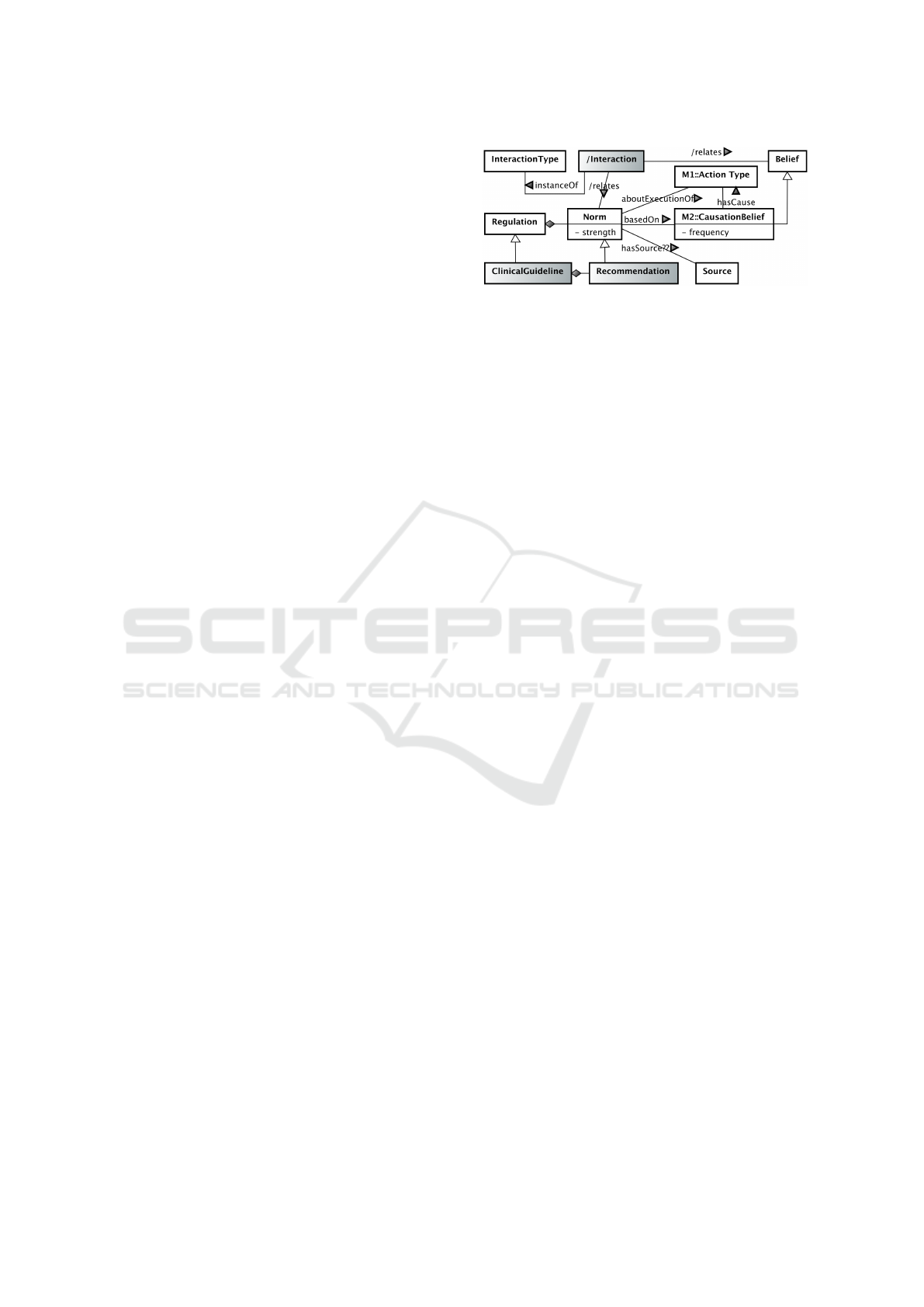
In more general terms, a Regulation is composed
of a set of Norms, given by a source, about the ex-
ecution of action types based on a causation belief.
The norm strength can vary from obligation to prohi-
bition. For the specific case of clinical domain, norms
are specialized as Recommendations and regulations
as Clinical Guidelines. Since the clinical guidelines
are mostly considered a reference for best practices,
the strength of recommendations in this work will
be considered as ‘should’ (positive) and ‘should-not’
(negative), any other variation of strength is out of
scope. Finally, among norms there can be Interac-
tions of different types. In this work we formalize
internal interactions discussed in (Zamborlini et al.,
2015a) and we extend and formalize external inter-
actions (introduced in (Zamborlini et al., 2015b)).
Figure 4: UML class diagram for the T MR
Norm
Model.
‘M1’ and ‘M2’ are used as short references for T MR
Event
and T MR
Belie f
respectively.
Figure 4 presents the UML class diagram for the
T MR
Norm
model.
The following FOL rule defines the derivable re-
lation regulates while the interactions are defined in
the next subsections. Some interaction types have
a cumulative behavior, like Repeated Action and Al-
ternative Actions (introduced in (Zamborlini et al.,
2014b)). For example, if three norms recommend
the administration of aspirin, there should be one sin-
gle interaction of type Repeated Action among them,
rather than three different interactions among pairs
of them. External interactions also accumulate, like
External-Alternative Action. Although the subsump-
tion relation in these rules can be also the epistemic
one, derivable through causation beliefs, we adopt the
simplified notation subsumes(a1, a2) since it does not
change the meaning of the rules.
Regulation - a norm n from a regulation r over an
action type a has strength st based on a causation
belief cb:
R.8 ∀r, n, a, st, cb (Regulation(r) ∧ Norm(n)
∧ partOf(n, r) ∧ ActionType(a) ∧ CausationBelief(cb)
∧ aboutExecutionOf(n, a) ∧ strength(n, st)
∧ basedOn(n, cb))
→ regulates(r, n, a, st, cb)
With respect to previous work, this section present
more generic version of the models with respect to
norms, beliefs and event types, (mentioned contribu-
tion C1). It allows, for instance, to better handle the
hierarchies of action types (or event types) possibly
deriving them from hierarchies of drug types, which
is commonly found in the existent datesets and ter-
minologies. Particularly the hierarchies concerning
effects believed to be promoted (e.g. Adm. Aspirin
specializes Adm. AntiInflammatory) are handled as
beliefs. This is indeed compatible with the discourse
of not of having certainty about causation relations.
FOL formulas are adapted/introduced for the deriv-
able relations. Furthermore, the incompatibility belief
is introduced in the T MR
Belie f
model, as well as the
strength of beliefs and causation frequency. Finally,
the recommendations strength is also introduced in
Generalizing the Detection of Internal and External Interactions in Clinical Guidelines
109

the T MR
Norm
model.
2.2.1 Internal Interaction Rules
Considering the modifications in the model, we pro-
pose in this section the corresponding adaptation of
the internal interaction rules presented in (Zambor-
lini et al., 2015a) (contribution C2). The following
types of interactions are defined:
Repeated Action: two positive norms about the
same action or about actions in a subsuming re-
lation. The second rule is for the cumulative be-
havior, i.e. when two different interactions of this
type relate the same norm (n2) then those interac-
tions are the same.
(I.1.1) ∀r, n1, n2, a1, a2, cb1, cb2(
regulates(r, n1, a1, ’should’, cb1)
∧ regulates(r, n2, a2, ’should’, cb2)
∧ (a1 = a2 ∨ subsumes(a1,a2) ∨ subsumes(a2,a1)))
→ ∃i(RepeatedAction(i) ∧ relates(i,n1)
∧ relates(i,n2))
(I.1.2) ∀i1, i2, n1, n2, n3( RepeatedAction(i1)
∧ RepeatedAction(i2) ∧ relates(i1,n1)
∧ relates(i1,n2) ∧ relates(i2,n2) ∧ relates(i2,n3)
∧ r1 6= n3 ∧ n1 6= n2 ∧ n2 6= n3 )
→ i1 = i2
Alternative Actions: two positive norms about dif-
ferent actions for achieving the same transition,
i.e. they are based on similar causation beliefs for
different actions. The second rule is for the cumu-
lative behavior
(I.2.1) ∀r, n1, n2, a1, a2, cb1, cb2(
regulates(r, n1, a1, ’should’, cb1)
∧ regulates(r, n2, a2, ’should’, cb2)
∧ similarTo(cb1, cb2) ∧ a1 6= a2 )
→ ∃i(AlternativeActions(i) ∧ relates(i,n1)
∧ relates(i,n2) )
(I.2.2) ∀i1, i2, n1, n2, n3( AlternativeActions(i1)
∧ AlternativeActions(i2) ∧ relates(i1,n1)
∧ relates(i1,n2) ∧ relates(i2,n2) ∧ relates(i2,n3)
∧ n1 6= n3 ∧ n1 6= n2 ∧ n2 6= n3 )
→ i1 = i2
Contradictory Norms: (i) two norms, positive and
negative, about the execution of same action (or
actions in a subsuming relationship) or (ii) two
norms, positive and negative, about different ac-
tions promoting the same transition or (iii) two
positive regulations about different actions for
achieving inverse transitions.
(I.3) ∀r, n1, n2, a1, a2, cb1, cb2, t1, t2(
regulates(r, n1, a1, ’should’, cb1)
∧ regulates(r, n2, a2, str, cb2)
∧ causes(a1,t1,’always’,cb1)
∧ causes(a2,t2,’always’,cb2)
∧ (( str = ’should-not’
∧ (a1 = a2 ∨ subsumes(a1,a2) ∨ subsumes(a2,a1))
∨ (str = ’should-not’ ∧ a1 6= a2 ∧ t1 = t2 )
∨ (str = ’should’ ∧ a1 6= a2 ∧ inverseTo(t1, t2))))
→ ∃i(Contradiction(i) ∧ relates(i,n1) ∧ relates(i,n2) )
Repairable Transition: two norms, positive and
negative, about different actions that are believed
to cause inverse transitions, i.e. if the undesired
effect cannot be avoided, it can be repaired by an-
other action.
(I.4) ∀r, n1, n2, a1, a2, cb1, cb2, t1, t2(
regulates(r, n1, a1, ’should’, cb1)
∧ regulates(r, n2, a2, ’should-not’, cb2)
∧ causes(a1,t1,’always’,cb1)
∧ causes(a2,t2,’always’,cb2)
∧ a1 6= a2 ∧ inverseTo(t1, t2) )
→ ∃i(RepairableAction(i) ∧ relates(i,n1)
∧ relates(i,n2))
2.2.2 External Interaction Rules
Beliefs from other sources provide interesting infor-
mation to enrich the system, allowing for detection of
external interactionsdefined as:
External-Alternative Actions: actions of which the
regulation system is not aware that might promote
a desired effect according to external sources. The
second rule is for the cumulative behavior, i.e. two
different interactions of this type relating the same
external causation belief are the same.
(E.1.1) ∀r, n1, a1, a2, cb1, cb2(
regulates(r, n1, a1, ’should’, cb1)
∧ similarTo(cb1, cb2) ∧ hasAsCause(cb2,a2)
∧ ¬(∃n2 regulates(r, n2, a2, ’should’, cb2))
∧ ¬ subsumes(a1, a2))
→ ∃i( ExternalAlternativeAction(i)
∧ relates(i,n1) ∧ relates(i,cb2) ∧ relates(i,a2) )
(E.1.2) ∀i1, i2, r, n1, n2, cb (ExternalAlternativeAction(i1)
∧ ExternalAlternativeAction(i2) ∧ CausationBelief(cb)
∧ relates(i1,cb) ∧ relates(i1,n1)
∧ relates(i2,cb) ∧ relates(i2,n2)
∧ Regulation(r) ∧ partOf(n1,r) ∧ partOf(n2,r))
→ i1 = i2
External-Incompatible Actions: two positive
norms about actions that the regulation system
is not aware of them being incompatible to each
other (or to a subsumed action), according to ex-
ternal sources.
(E.2) ∀r, n1, n2, a, a1, a2, cb1, cb2, ib1(
regulates(r, n1, a1, ’should’, cb1)
∧ regulates(r, n2, a2, ’should’, cb2)
∧ incompatibleWith(a, a2, ib1)
∧ (a1 = a ∨ subsumes(a1,a) ∨ subsumes(a,a1)))
HEALTHINF 2016 - 9th International Conference on Health Informatics
110

→ ∃i(ExternalIncompatibleActions(i)
∧ relates(i,n1) ∧ relates(i,n2) ∧ relates(i,ib11) )
External-Incompatible Effects: effects (situations)
recommended to be either avoided or changed, but
which are believed to be promoted by other rec-
ommended actions, according to external sources,
while the regulation system is not aware of it.
(E.3) ∀r, n1, n2, a, a1, a2, cb, cb1, cb2, s1(
regulates(r, n1, a1, st, cb1)
∧ causes(a1, t1, ’always’, cb1)
∧ ((st= ‘should’) ∧ hasTransformableSituation(t1,s1))
∨ (st= ‘should-not’) ∧ hasExpectedSituation(t1,s1)))
∧ causes(a, t, ’always’, cb) ∧ a 6= a1
∧ hasExpectedSituation(t, s1)
∧ regulates(r, n2, a2, ’should’, cb2) ∧ cb 6= cb2
∧ (a2 = a ∨ subsumes(a,a2) ∨ subsumes(a2,a)))
→ ∃i(ExternalIncompatibleEffects(i) ∧ relates(i,n1)
∧ relates(i, n2) ∧ relates(i,s1) ∧ relates(i,cb2) )
This section concludes the contribution C2 by pro-
viding generic rules for detecting external interac-
tions. In (Zamborlini et al., 2015b) the rules were
specific for a dataset (namely DrugBank). Now the
generic rules apply to beliefs imported from any
dataset. At this point its also important to observe
that both models and rules are defined in a domain-
independent way. A SemWeb-based implementation
is provided in the next section.
2.3 SemWeb Implementation
This section presents a SemWeb implementation
5
for
the proposed approach. The proposed models have
a straighforward mapping to OWL2 (ommited in the
paper). However, for instantiating the models with the
clinical knowledge, we propose the use of a frame-
work as RDF graph structure based on the open for-
mats Nanopublication, Provenance and Open Anno-
tation (see section 4). It is applied for representing
the recommendations (norms) and beliefs as asser-
tions connected to their sources, besides other meta-
information. In the sequence, the implementation of
the FOL rules using SWI-Prolog is exemplified, to-
gether with a procedure adopted to import clinical
knowledge from LOD (e.g. DrugBank and Sider) as
assertions via generic predicates (beliefs).
2.3.1 Framework
The framework, illustrated in Fig. 5, follows the
Nanopublication structure, which presupposes the use
of Prov vocabulary, and is enriched with (optional)
Open Annotation vocabulary. The latter is meant for
5
Accessible at http://rapgmsbgym.github.io.
Nanopublication
Assertion
nanopub:hasAssertion
nanopub:hasProvenance
Provenance
prov:wasDerivedFrom
a
oa:hasBody
oa:hasTarget
oa:hasSource
source
oa:Annotation
_
PublicationInfo
dateTime
prov:generatedAtTime
x
prov:wasAttributedTo
nanopub:hasPublicationInfo
Figure 5: Nanopublication Schema proposed for represent-
ing Beliefs & Recommendations.
representing assertions that are (somehow) extracted
from textual documents.
Rounded-dotted boxes represent named graphs
containing triples, which in turn are represented as
directed-named arrows among resources. The black
circles represent the named graphs themselves as sub-
ject/object, while the other resources are represented
as ellipses with a description inside (where underline
stands for blank nodes) or as an expected data-value
(e.g. source or date).
The more external named graph, called Nanopub-
lication, connects the following three named graphs:
The assertion is a named graph where some knowl-
edge is described using suitable vocabularies, in our
case the TMR models. The other named graphs are
meant to provide the meta-information about both
the assertion and its publication as rdf-data: (i) the
provenance graph can contain information such as
the source (prov:wasDerivedFrom) of the assertion
(e.g. clinical guideline, study or dataset), and text-
annotations (oa:Annotation) when the assertion is ex-
tracted from a piece of text; and (ii) the publication-
Info graph provides meta-information such as when
the publication was created and by whom. For sake of
readability, henceforth we omit from the figures part
of the framework that is not relevant for the discussion
here conducted.
Figure 6 illustrates the representation of both a
causation belief (at the top) and a recommendation
(at the bottom). The Assertion1 is a CausationBe-
lief with high strength level, about the action type
that Adm. Ibuprofen always causes the transition type
Pain relief according to OA-CIG-Description. The
Assertion2 is a Norm, part of OA-GIC that states
Adm. Ibuprofen should be executed based on the
evidence stated in Assertion1 according to OA-CIG-
Description. Beliefs taken from external sources are
similarly represented (see Fig. 7).
The framework favor data reusability as LOD,
Generalizing the Detection of Internal and External Interactions in Clinical Guidelines
111

Provenance1
prov:wasDerivedFrom
a
oa:hasBody
oa:hasTarget
oa:hasSource
OA-CIG-Descr.
oa:Annotation
_
Provenance2
prov:wasDerivedFrom
a
oa:hasBody
oa:hasTarget
oa:hasSource
OA-CIG-Descr
oa:Annotation
_
Assertion2
m3:Norm
a
"should"
m3:strength
Adm.
Ibuprofen
m3:aboutExecOf
m3:basedOn
OA-CIG
m3:partOf
Assertion1
m2:CausationBelief
a
"always"
m2:frequency
Adm.
Ibuprofen
Pain Relief
m2:causes
m2:strength"high"
Figure 6: Nanopublication Schema for Causation Beliefs &
Norms extracted from Guidelines. ‘M2’ and ‘M3’ are used
as prefixes for T MR
Belie f
and T MR
Norm
respectively.
since it is compatible with SemWeb standards pro-
posed for expressing and annotating knowledge ex-
tracted from (scientific) publications. It comprises
part of contribution C3 (SemWeb implementation of
model and rules).
2.3.2 Rules
The proposed FOL rules have the typical format of
Prolog rules, what makes its implementation very
straightforward. The implemented rules are here il-
lustrated as: function F.1 implements R.8 while func-
tions F.2.1, F.2.2 implement the rules I.1.1 and I.1.2
for interaction RepeatedAction. For the purpose of
this application, the existential quantifier in the conse-
quent of interaction rules is implemented as a Prolog
function called existsInteraction. This function uses
the rdf
assertion built-in-function to insert the respec-
tive interaction in the dataset in case it does not exist.
(F.1) regulates(Reg, Norm, ActT, Str, CBelief) :-
instanceOf(Norm, m3:’Norm’),
rdf(Norm, m3:‘partOf’, Reg),
rdf(Norm, m3:‘aboutExecutionOf’, ActT),
rdf(Norm, m3:‘strength’, literal(type(xsd:string,Str))),
rdf(Norm, m3:‘basedOn’, Belief, Norm).
(F.2.1) forall( (regulation(Reg),
regulates(Reg, N1, ActionT1, ’should’, ),
regulates(Reg, N2, ActionT2, ‘should’, ),
different(N1,N2),
( same(ActionT1, ActionT2)
; subsumes(ActionT1, ActionT2)
; subsumes(ActionT2, ActionT1) )),
existsInteraction(‘RepeatedAction’, N1, N2)).
(F.2.2) forall( (interacts(‘RepeatedAction’, N1, N2, I1),
interacts(‘RepeatedAction’, N2, N3, I2),
different(N1,N3), different(I1, I2)),
rdf assert(I1, owl:sameAs, I2)).
This section comprises part of contribution C4
(flexible mechanism for reusing LOD to detect in-
teractions) and together with the framework, it con-
cludes contribution C3.
Assertion4
m2:CausationBelief
a
"always"
m2:frequency
Adm.
Ibuprofen
Tr. High Blood
Pressure
m2:causes
m2:strength"low"
Assertion3
m2:CausationBelief
a
"always"
m2:frequency
Adm.
Epoprostenol
Tr. LowerBlood
Coagulation
m2:causes
m2:strength"medium"
Assertion5
m2:IncompatibilityBelief
a
Adm.
Ibuprofen
Adm. Aspirin
m2:incompatibleWith
"medium"
m2:strength
Provenance3
prov:wasDerivedFrom
Drugbank
db:Epopros.
db:catAC
_
prov:used
prov:was
GeneratedBy
prov:Activity
a
prov:used
Provenance4
prov:wasDerivedFrom
Sider
sd:Ibuprofen
sd:HighBP
_
prov:used
prov:was
GeneratedBy
prov:Activity
a
prov:used
Provenance
prov:wasDerivedFrom
Drugbank
db:DDI-A-I
_
prov:used
prov:was
GeneratedBy
prov:Activity
a
Figure 7: Nanopublication schema for representing beliefs
extracted from external knowledge sources. ‘M2’ is used as
prefix for T MR
Belie f
.
2.3.3 Using External Knowledge - LOD
For some external knowledge-bases available as
LOD, a procedure is adopted for importing the knowl-
edge as new beliefs. For example, knowledge about
the (side) effects of administering a certain drug can
be imported from Sider. Each LOD requires a proce-
dure of reinterpreting the original knowledge into the
format here proposed. Once it is done, the rules can
derive external interactions regardless to the source
6
.
The following SWI-Prolog rule is used for importing
causation beliefs from drugbank (other rules can be
found online, also comprising sider and dikb).
Drug Alternatives for all drugs belonging to a
drugCategory regarding an effect, the causa-
tion beliefs are asserted about the actions of
administering those drugs promoting the referred
effect/transition.
forall( rdf(DrugCat, model:’hasGroupingCriteria’,
Trans1),
same(DrugCat, DrugCatDB),
rdf(DrugDB, drugcategory:’category’, DrugCatDB),
rdf(Act1, model:’administrationOf’, DrugType),
same(DrugType, DrugDB))),
(assertCausation(Act1, Trans1, ‘always’, ‘drugbank’,
6
The Drug and Situation Types are mirrored and mapped
to the to the external knowledge sources via owl:sameAs.
HEALTHINF 2016 - 9th International Conference on Health Informatics
112

NanopubURI),
assertProvResourceUsed(NanopubURI, DrugDB),
assertProvResourceUsed(NanopubURI, DrugCatDB))).
Figure 7 depicts the representation of beliefs ex-
tracted from both Drugbank and Sider. The Asser-
tion3 at the top is a CausationBelief with medium
strength level, stating that the action type Adm.
Epoprostenol always causes the transition type Lower
Blood Coagulation according to Drugbank. The As-
sertion4 in the middle is another CausationBelief
with low strength level, stating that Adm. Ibuprofen
always causes to Higher Blood Pressure according to
Sider. Finally, Assertion5 is a IncompatibilityBelief
with medium strength level, stating that Adm. Ibupro-
fen and Adm. Aspirin are incompatible according to
Drugbank. For all of them, the provenance graphs
contain, besides the source dataset, the external re-
sources based on which the assertions were generated.
This section concludes contribution C4 together
with the formalisation and implementation of rules
for external interactions. Medical guidelines as well
as external clinical knowledge can be expressed by
means of the conceptual model and can be imple-
mented in a SemWeb-based Framework for automat-
ically detecting interactions. In the next section we
provide an experimental assessment by discussing the
implementation a case study on detecting recommen-
dations interactions enriched by external knowledge
sources.
3 EXPERIMENTAL
ASSESSMENT
This section presents the results obtained by imple-
menting the case study on combining OA+HT+DB
guidelines (Sect. 2.1). The following activities where
performed in the experiment: (i) the guideline knowl-
edge was (manually) introduced in a RDF dataset ac-
cording to the implementation here proposed; (ii) the
rules for importing LOD were fired; (iii) the rules for
inferring relations and interactions were fired. An ‘in-
teractive’ documentation describing the experiment
and the prolog code is available online
7
. Figure 8
summarize the obtained results. It describes the type
of interaction, the interaction and its source (derived
from internal or external knowledge). The first six
lines are the interactions described in Sect. 2.1. The
last two lines illustrates that more external interac-
tions can be detected, actually much more given the
large volume of clinical LOD. However, since excess
of information can become a disadvantage, we intend
7
http://rapgmsbgym.github.io
to provide filters, such as the causation frequency or
the strength of the evidence.
Comparing to the previous implementation (Zam-
borlini et al., 2015b), the following explicit improve-
ments are observed: (i) reasoning over action type
hierarchy allows for detecting non-straightforward
interactions (e.g. DO administer NSAID and DO
NOT administer Aspirin are in contradiction because
Aspirin specializes NSAID); (ii) new datasets (e.g.
Sider) are added without need for writing specific
rules for detecting external interactions; and (iii) cau-
sation frequency, belief strength (evidence level) and
recommendation strength can be represented. Im-
plicit improvement are: (i) a more maintainable and
reusable implementation that will favor new features
and datasets to be introduced in future work; (ii) the
more reliable and/or relevant information can be se-
lect.
4 RELATED WORK
Formal languages proposed for representing clini-
cal guidelines as “computer interpretable” ones (An-
nette ten Teije, 2008; Peleg, 2013) were not designed
to handle the combination of multiple CIGs (Zam-
borlini et al., 2014a). An alternative solution is the
development of alert systems that are independent of
the CGs. Such Computerized Physician Order Entry
systems (CPOE), are used to alert physicians about
drug interactions (Ammenwerth et al., 2008). De-
spite the usefulness of these systems, a lot can be
gained by tackling interactions between general rec-
ommendations on the outset, rather than employing
drug-interaction alerts on the hospital floor.
We have investigated this issue in a series of work.
In (Zamborlini et al., 2014a) we analyzed related
work that addresses recommendation interactions in
different levels. Our research focuses on what we
called the CIG level, i.e. it accounts for the need
to combine guidelines and handle interactions be-
fore applying them to a specific patient. This is the
case when common co-occurring diseases are consid-
ered during guideline development, but could also be
needed for uncommon co-occurring diseases in the
practice setting. The related work (Jafarpour, 2013;
L
´
opez-Vallverd
´
u et al., 2013; Wilk and Michalowski,
2014) has as their main drawback the need for defin-
ing specific rules for each interaction, e.g. give as-
pirin & don’t give aspirin requires a specific rule
and give ibuprofen & don’t give ibuprofen requires
another rule (a more detailed analysis in (Zambor-
lini et al., 2015b)). As a consequence, they do not
provide ‘scalabe’ support for combining guidelines,
particularly more than two. Piovesan et al. (Pi-
Generalizing the Detection of Internal and External Interactions in Clinical Guidelines
113

Interactions
Interaction Type
Interacting Recommendations/Beliefs
Source
AlternativeActions
['Avoid thrombi - by should Administer NSAID', 'Avoid thrombi - by should Administer
Tramadol']
Internal
Contradiction
['Avoid gastrointestinal bleeding - by should-not Administer Aspirin', 'Avoid thrombi - by should
Administer NSAID']
Internal
ExternalAlternativeAction
['Administer Epoprostenol always causes Low Blood Coagulation', 'Avoid thrombi - by should
Administer NSAID', 'Avoid thrombi - by should Administer Tramadol']
DrugBank
ExternalIncompatibleActions
['Administer Aspirin incompatible with Administer Ibuprofen', 'Avoid thrombi - by should
Administer NSAID', 'Reduce pain - by should Administer Ibuprofen']
DrugBank
ExternalIncompatibleEffects
['Administer Bendroflumethiazide always causes High Level Blood Sugar', 'Reduce blood pressure
- by should Administer Thiazide', 'Reduce blood sugar level - by should Administer Insulin']
Sider
ExternalIncompatibleEffects
['Administer Ibuprofen always causes High Blood Pressure', 'Reduce blood pressure - by should
Administer Thiazide', 'Reduce pain - by should Administer Ibuprofen']
Sider
ExternalAlternativeAction
['Administer Dipyridamole always causes Low Blood Coagulation', 'Avoid thrombi - by should
Administer NSAID', 'Avoid thrombi - by should Administer Tramadol']
DrugBank
ExternalIncompatibleEffects
['Administer Ibuprofen always causes High Level Blood Sugar', 'Avoid thrombi - by should
Administer NSAID', 'Reduce blood sugar level - by should Administer Insulin']
Sider
Figure 8: Case study on combining guidelines for OA+HT+DB.
ovesan et al., 2014) propose guideline-independent
algorithms based on ontologies for detecting interac-
tions, restricted to types “concordance” and “discor-
dance”. The use of intentions associated to recom-
mendations for detecting “intention interactions” is
close to our approach on verifying transitions related
to recommendations. To the best of our knowledge,
none of the related work provides means to express
negative norms, nor negative causation beliefs. More-
over, they do not explore action type hierarchies, nor
reuse clinical knowledge available online in order to
enrich the detection of interactions. However, they do
address other aspects that we do not address yet, such
as intentions, temporal aspects and qualitative transi-
tions.
Our earlier work highlighted the importance of
having the recommendations formally represented
with a high level of detail. Explicit description of
local constraints and impact of recommendations is
considered an important source of information for in-
creased reasoning capabilities and improved explana-
tion of conflicts in (Bonacin et al., 2013). The model
described in (Zamborlini et al., 2014a) introduced
clinical recommendations as governing care actions
that cause state transitions; an extended version of this
model presented in (Zamborlini et al., 2014b) defines
different ways in which recommendation can inter-
act according to the referred actions and transitions.
The implementation and evaluation of the model us-
ing Semantic Web languages was proposed by us in
(Zamborlini et al., 2015b). We argued that the detec-
tion of interactions using external knowledge sources
(in our case drug interactions modeled in the Linked
Data version of DrugBank (Law et al., 2014)) can pro-
vide more precise information. A Web-based applica-
tion for browsing the guideline interactions was made
available online
8
. Extending this model to introduce
the notion of causation beliefs (for evidence) and the
8
See http://guidelines.hoekstra.ops.few.vu.nl
subsumption relations among actions was presented
in (Zamborlini et al., 2015a). It was a first formal ex-
ercise with the goal of providing a systematic view
on possible internal interactions among recommenda-
tions.
The emphasis on evidence means that care rec-
ommendations are ultimately grounded in domain
knowledge (generalizations over facts). The evidence
that underlies the recommendations is weighed de-
pending on the quality, depth and breadth of the study:
guidelines are part of a larger network of hypotheses,
claims and pieces of evidence that span across mul-
tiple publications (de Waard et al., 2009). However,
only few CIG languages offer means to link to evi-
dence (Peleg, 2013), and they generally are targeted
to very concrete and procedural guidelines, akin to
medical protocols. In (Hoekstra et al., 2012), the
authors describe a lightweight ontology that repre-
sents the relations between a guideline, its recom-
mendations, and underlying evidence, as annotations
on the guideline and evidence texts using a combina-
tion of the Open Annotation
9
and PROV
10
formats.
Huang et al. (Huang et al., 2014) propose an even
more lightweight semantic representation of evidence
based clinical guidelines, but automatically extract it
from guideline texts. It includes UMLS identifiers for
medical terms appearing in the text and use proximity,
and the types of terms to infer the type and strength
of the evidence that underlies recommendations. The
Nanopublication model (Mons et al., 2011) seems to
be a natural fit to modeling the evidence that under-
lies guidelines. It represents a publication as three
RDF graphs, that respectively capture an assertion
(the finding or evidence), the provenance of the as-
sertion (e.g. an experiment) and publication informa-
tion about the nanopublication (when was the asser-
tion published and by whom).
9
See http://www.openannotation.org.
10
See http://www.w3.org/TR/prov-o.
HEALTHINF 2016 - 9th International Conference on Health Informatics
114

The work presented here combines the pragmatic
approaches of (Hoekstra et al., 2012; Huang et al.,
2014) and (Mons et al., 2011) in a model that takes the
epistemological stance that the evidence underlying a
recommendation expresses a belief that a care action
causes a certain state transition. This strategy allows
for using classical logic-based languages for handling
inconsistent knowledge, such as conflicting findings
published in different clinical studies.
5 DISCUSSION & CONCLUSION
The work reported on in this paper improves over our
previous work by offering a more generic and scal-
able way to represent clinical guidelines and detect-
ing interactions. This is done by adapting and ex-
tending both the conceptual model and the Semantic
Web-based implementation. The TMR models and
rules are made more generic so that they can be more
easily extended to incorporate new features such as
hierarchies of transition types and causal chains. In-
corporating the epistemological nuance of beliefs in
the Semantic Web representation, improves the abil-
ity to (i) handle knowledge from different sources and
(ii) select the reliable ones; (iii) to allow different, in-
compatible beliefs about the same event to co-exist;
and (iv) to provide reusable formal rules that are ap-
plicable regardless of specific regulations, guidelines
or external sources. This has a favorable effect on
reusability, maintainability, and scalability beyond the
guidelines we currently covered.
We furthermore show the power of using the ex-
tensive domain knowledge available on the Semantic
Web for enhancing the ability to automatically per-
form new tasks, such as suggesting alternative drugs.
Our use of open standards and vocabularies, such as
the nanopublicaiton format, makes that the knowl-
edge accumulated in our own models is shareable and
reusable in a similar fashion. We implement inferenc-
ing using expressive SWI-Prolog rules that execute
over RDF graphs. The adoption of SWI-Prolog was
an improvement over the implementation in (Zam-
borlini et al., 2015b), as it gave us a single environ-
ment for expressing our inference rules benefiting un-
derstandability and maintainability. This, of course,
at the cost of Semantic Web standards compliance
for that specific part of our model. In (Zamborlini
et al., 2015b) the limitations of OWL2 for detecting
the interactions, forced the use of multiple knowl-
edge representation languages. We had to resort to a
combination of expressive OWL2 inferencing, Star-
dog SPARQL rules (a SWRL dialect) and custom
SPARQL update queries to perform reasoning.
The experimental assessment shows that inter-
actions can be automatically detected among three
guidelines and enriched by knowledge from Drug-
Bank and Sider, from each of which the relevant
knowledge was imported as beliefs. Although the
case study comprises only drug administration as ac-
tion types, the approach is designed to address inter-
actions among other types of interventions, such as
surgeries and exercise therapy. More complex case
studies will be addressed in future work. We faced
some issues regarding the integration with these ex-
ternal knowledge sources, particularly on deciding
which identity criteria we should use to map to the
external datasets. For example, we could choose be-
tween PubChem ID, UMLS code, dbpedia and so on,
where each choice would bring about different cover-
age and reliability.
Although this work is applied to clinical guide-
lines, its potentially of more general application, since
both the model and the rules are defined indepen-
dently of a particular domain. We plan to investi-
gate the applicability of the models and rules to other
domains such as disaster management. As ongoing
work, we plan to address four limitations: (i) tem-
poral validity for the assertions; (ii) quantification of
beliefs and norms (i.e., frequency and strength); (iii)
qualification of transitions (e.g. increasing or decreas-
ing a property value); and (iv) considering goals and
intentions;
ACKNOWLEDGEMENTS
The first author would like to thank colleagues from
NEMO-UFES/Brazil for fruitful discussions about
transitions, causation beliefs and regulations, and also
prof. md. Saulo Bortolon for the nice discussions
about medical domain; Jan Wielemaker and Wouter
Beek from VU for helping with SWI-Prolog imple-
mentation; Wytze Vliestra (former VU) for fruitful
discussions about the biomedical domain; and Paul
Groth from Elsevier for fruitful discussions about
the potential generality of the model and the use of
nanopublications, This work was partially funded by
the Dutch National Programme COMMIT.
REFERENCES
Ammenwerth, E., Schnell-Inderst, P., Machan, C., and
Siebert, U. (2008). The effect of electronic prescrib-
ing on medication errors and adverse drug events: a
systematic review. Journal of the American Medical
Informatics Association, 15(5):585–600.
Generalizing the Detection of Internal and External Interactions in Clinical Guidelines
115

Annette ten Teije, Silvia Miksch, P. L., editor (2008).
Computer-based Medical Guidelines and Protocols:
A Primer and Current Trends, volume 139 of Tech-
nology and Informatics.
Barnett, K., Mercer, S., Norbury, M., and Watt, G. (2012).
Epidemiology of multimorbidity and implications for
health care, research, and medical education: a cross-
sectional study. The Lancet.
Bonacin, R., Pruski, C., and Da Silveira, M. (2013). Ar-
chitecture and services for formalising and evaluating
care actions from computer-interpretable guidelines.
IJMEI International Journal of Medical Engineering
and Informatics, 5:253–268.
de Waard, A., Shum, S. B., Carusi, A., Park, J., Samwald,
M., and S
´
andor,
´
A. (2009). Hypotheses, evidence
and relationships: The hyper approach for represent-
ing scientific knowledge claims. In Proceedings of the
8th ISWC, Workshop on Semantic Web Applications in
Scientific Discourse, Berlin. Springer.
Guizzardi, G., Wagner, G., de Almeida Falbo, R., Guiz-
zardi, R. S. S., and Almeida, J. P. A. (2013). Towards
Ontological Foundations for the Conceptual Model-
ing of Events. In Conceptual Modeling, 32th Interna-
tional Conference, ER 2013, pages 327–341, Hong-
Kong. Springer Berlin Heidelberg.
Hoekstra, R., de Waard, A., and Vdovjak, R. (2012).
Annotating evidence based clinical guidelines - A
lightweight ontology. In Paschke, A., Burger, A., Ro-
mano, P., Marshall, M. S., and Splendiani, A., editors,
Proceedings of the 5th International Workshop on Se-
mantic Web Applications and Tools for Life Sciences,
Paris, France, November 28-30, 2012, volume 952 of
CEUR Workshop Proceedings. CEUR-WS.org.
Huang, Z., ten Teije, A., van Harmelen, F., and Ait-
Mokhtar, S. (2014). Semantic Representation of
Evidence-based Clinical Guidelines. In 6th Inter-
national Workshop on Knowledge Representation for
Health Care (KR4HC2014), volume 8903 of LNCS.
Jafarpour, B. (2013). Ontology Merging using
Semantically-defined Merge Criteria and OWL
Reasoning Services: Towards Execution-time
Merging of Multiple Clinical Workflows to Handle
Comorbidity. PhD thesis, Dalhousie University.
Law, V., Knox, C., Djoumbou, Y., Jewison, T., Guo, A. C.,
Liu, Y., MacIejewski, A., Arndt, D., Wilson, M.,
Neveu, V., Tang, A., Gabriel, G., Ly, C., Adamjee,
S., Dame, Z. T., Han, B., Zhou, Y., and Wishart, D. S.
(2014). DrugBank 4.0: Shedding new light on drug
metabolism. Nucleic Acids Research, 42(D1):1091–
1097. D1091-7, PubMed ID: 24203711.
Lohr, K. N. (2003). Rating the strength of scientific evi-
dence: relevance for quality improvement programs.
International Journal for Quality in Health Care,
16(1):9–18.
L
´
opez-Vallverd
´
u, J. A., Ria
˜
no, D., and Collado, A. (2013).
Rule-based combination of comorbid treatments for
chronic diseases applied to hypertension, diabetes
mellitus and heart failure. In LNCS, volume 7738
LNAI, pages 30–41.
Mons, B., van Haagen, H., Chichester, C., Hoen, P.-B.,
den Dunnen, J., van Ommen, G., van Mulligen, E.,
Singh, B., Hooft, R., Roos, M., Hammond, J., Kiesel,
B., Giardine, B., Velterop, J., Groth, P., and Schultes,
E. (2011). The value of data. Nature Genetics,
43(4):281–283.
Peleg, M. (2013). Computer-interpretable clinical guide-
lines: a methodological review. Journal of biomedical
informatics, 46(4):744–63.
Piovesan, L., Molino, G., and Terenziani, P. (2014). An
ontological knowledge and multiple abstraction level
decision support system in healthcare. Decision Ana-
lytics, 1(1):8.
Wilk, S. and Michalowski, M. (2014). Using First-Order
Logic to Represent Clinical Practice Guidelines and to
Mitigate Adverse Interactions. In Knowledge Repre-
sentation for Health-Care (KR4HC). LNCS, vol. 8903,
Berlin Heidelberg. Springer.
Zamborlini, V., da Silveira, M., Pruski, C., ten Teije,
A., and van Harmelen, F. (2014a). Towards a
Conceptual Model for Enhancing Reasoning about
Clinical Guidelines: A case-study on Comorbid-
ity. In Knowledge Representation for Health-Care
(KR4HC). LNCS, vol. 8903, Vienna, Austria. Springer
Berlin Heidelberg.
Zamborlini, V., da Silveira, M., Pruski, C., ten Teije, A.,
and van Harmelen, F. (2015a). Analyzing Recommen-
dations Interactions in Clinical Guidelines: Impact of
action type hierarchies and causation beliefs. In Artifi-
cial Inteligence in Medicine (AIME). LNCS,. Springer.
Zamborlini, V., Hoekstra, R., da Silveira, M., Pruski, C.,
ten Teije, A., and van Harmelen, F. (2014b). A
Conceptual Model for Detecting Interactions among
Medical Recommendations in Clinical Guidelines. In
Knowledge Engineering and Knowledge Management
(EKAW). LNCS, vol. 8876, pages 591–606. Springer.
Zamborlini, V., Hoekstra, R., da Silveira, M., Pruski, C.,
ten Teije, A., and van Harmelen, F. (2015b). Inferring
Recommendation Interactions in Clinical Guidelines:
Case-studies on Multimorbidity. Semantic Web Jour-
nal, Accepted, Open Acess.
HEALTHINF 2016 - 9th International Conference on Health Informatics
116
