
Industry-oriented Education in eHealth
Janne Lahtiranta
1
and Anne-Maarit Majanoja
2
1
Department of Management and Entrepreneurship, University of Turku, Turku, Finland
2
Department of Information Technology, University of Turku, Turku, Finland
Keywords: Industry-Oriented Education, eHealth, Health Care Information Systems, Health Care Technologies.
Abstract: Technology, or more specifically digitalization, has had a profound effect on industry regardless of the field
of business. It has changed the way individuals interact, work and go about their everyday businesses. This,
still ongoing change, calls for new kind of professionals who can meet the challenges placed by the changing
industry. Health care is one of the areas where digitalization has the most profound effect. It does not only
change the way people work, but it also changes the underlying balance of power between different actors.
The domain is also an inherently hybrid one as the professionals need to understand what is in the crux of
technology and care, between the patient and the professional. In the following, a pilot focused on educating
professionals in the field of eHealth in industry-oriented fashion is described focusing on the process and
people; stages leading to actual lectures. The result of the examination is a process that can be used in
developing industry-oriented education in a domain where expectations are currently high around the globe,
and challenges placed on the educators are in a constant flux.
1 INTRODUCTION
Advanced digitalization, the ongoing industrial
paradigm shift (Lasi et al., 2014) is changing the
world in new and often unanticipated ways. It
changes our behavior, the ways we interact with each
other - how we learn and how we teach - and it even
has an impact on the fundamental notion of what
means to be a human.
Digitalization has already created benefits for
many, and it will continue to do so in the upcoming
years. However, even if it may seem so, digitalization
is not axiomatic nor can be taken for granted; talented
people are needed to see the ongoing shift to come
through.
Universities, especially Humboldtian science
universities, are often blamed for stagnation. They are
regarded as slow to react to the economic
developments in the surrounding worlds (Fathi and
Wilson, 2009; Lozano et al., 2013), and establishing
new courses and degree programs often takes years
(Gerson, 2015). To counter these arguments, and to
develop a sustainable and networked approach for
industry-oriented education, a project called
“Working Life Oriented Open University Education”
was established. In the project, polytechnics,
universities, and industrial partners collaborated in
three distinct fields of 1) health and social services, 2)
bio-based economy, and 3) Information and
Communication Technologies (ICT).
The project, funded by the European Social Fund
(2015-2018) consisted of three pilots, one in each of
the three fields. The pilots were stand-alone pilots. In
other words, they were implemented autonomously in
order to take the distinct characteristics of each field
into account, and to create different practices to be
investigated by an external evaluator later on in the
project. Each pilot was charged with specific tasks of
a) developing a method for industry-oriented
education, and b) testing the method in practice.
In the pilots, the development took the form of
“inspect and adapt” cycles and in concurrent
implementations with a specific focus (Figure 1), in
the spirit of Agile approach (Cohn, 2005). Due to the
differences in the fields, and autonomy of the pilots,
the length and amount of cycles was not predefined
or limited. In some pilots, the most practical solution
was to emphasize the dialogue with the organizations,
focus on business priorities, and to implement a single
cycle in which the defined method was tested.
Lahtiranta, J. and Majanoja, A.
Industry-oriented Education in eHealth.
DOI: 10.5220/0006651504110419
In Proceedings of the 10th International Conference on Computer Supported Education (CSEDU 2018), pages 411-419
ISBN: 978-989-758-291-2
Copyright
c
2019 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
411
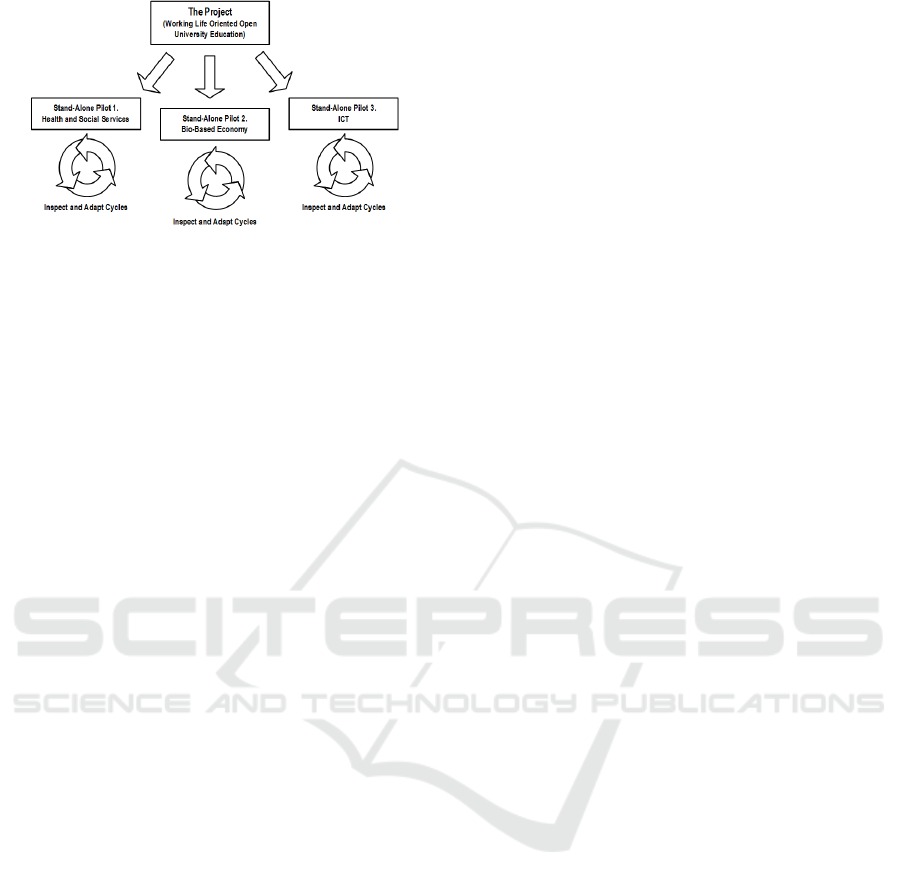
Figure 1: Overall project and pilots.
In the following, the focus is on the ICT pilot (Figure
1, stand-alone pilot 3), and more specifically on one
of its implementations that was carried out during the
first half of the 2016 in the field of health and
wellbeing technologies (eHealth). In the following,
this implementation is referred as the eHealth pilot.
The examination focuses on the process and the
experiences – the way or organizing education in an
industry-oriented fashion. It follows from this that the
end-user experiences, such as statistical analysis of
the student feedback, is omitted from the findings.
2 eHEALTH PILOT
Health care is one of the fields most influences by
digitalization. It does not only change the way of
working in the field, but it also has a tremendous
impact on how responsibilities and duties, even
power, is delegated in the field (Koskinen and
Knaapi-Junnila, 2014; Lahtiranta et al., 2015).
eHealth is also one of the most promising fields in
terms of business growth in Finland. While other
fields have been in decline during the last years,
eHealth has been on the increase. For example, in
2014 health technology export grew to €1.8 billion
with a surplus of €829 million (Kauppalehti, 2015).
By the end of 2014, eHealth alone covered more than
half of the overall high technology export in Finland,
more than telecommunications which has been a
strong field in Finland for a long time (Kauppalehti,
2015).
eHealth is not a new field or a sudden ‘booming
star’ in Finland. The field has been on the rise for the
last eight years and there is no indication that the
situation will change in the near future. One indicator
of this is a survey conducted in the late 2015 amongst
health technology companies in Finland by the
Finnish Health Technology Association (FiHTA) and
Saranen Consulting. According to the survey,
majority of the companies working in the field were
to hire new personnel in 2016 (Saranen Consulting,
2015).
Another indicator of relevance is the changing
health care infrastructure in Finland. At the moment
there are four major health care digitalization projects
in Finland. In two of them, focus on implementing a
new Electronic Health Record (EHR). First one of the
EHR projects, Apotti, focuses on the public health
service providers operating in the metropolitan area
(i.e. greater Capital Region). Apotti is currently in the
early stages of implementation and in early May,
2016 the project recruited approximately 150 health
technology professionals. The latter EHR project,
Una, focuses on providers operating outside the
metropolitan area. The project is currently
(September, 2017) in the early stages of
implementation and it is estimated that the acquisition
of the core components will begin in the fall 2017.
The remaining two health care digitalization
projects, Virtual Hospital and Digital Self-care
Services (ODA), focus on implementing new
electronic services, such as virtual clinics (cd. Krausz,
et al., 2016) in basic health care (ODA), and in
specialized health care (Virtual Hospital). While the
actual costs associated with the projects is still
unclear, it is estimated that the costs of the EHR
projects alone will be in the neighborhood of €1
billion (Helsingin Sanomat, 2015) of which Apotti
alone will cover €575 million (over the timeframe of
10 years) (Apotti, 2017).
The ongoing development in the field has created
an acute demand for technology professionals who
possess a) a domain-specific skill-set from the field
of ICT, and b) at least basic understanding on how the
field of health care operates. In order to understand
what these skills are, and what kind of ‘hybrid
professionals’ the field needs, the first
implementation of the ICT pilot focused on eHealth.
Digitalization does not only create new
opportunities to the field of health care, but to the
field of education as well, as different digital devices,
modalities, and ways of reaching students have
become available (cf. Gárcia-Peñalvo et al., 2014).
However, new tools and ‘gadgets’ alone do not
inspire learning; it is important to focus on the content
and incorporate real-life elements into education. One
well-employed approach is to combine online courses
(El-Bishouty et al., 2014), and mix the course
contents with the challenges emerging in the domain
of application. In this, a constant dialogue with the
domain-experts from the industry-side is of the
essence.
CSEDU 2018 - 10th International Conference on Computer Supported Education
412

2.1 The Framework
On the level of the overall project, the work was
organized in stand-alone pilots focusing on a specific
field. Within the pilot focusing on the field of ICT,
the work was further organized as “inspect and adapt”
cycles and concurrent implementations with a more
refined focus (Figure 1). In the ICT pilot, one of the
implementations focusing on eHealth (i.e. the eHealth
pilot) organized the work even further by employing
a more specific methodological framework.
The employed framework based on the works of
Stewart and Hyysalo (2008), and previous work by
Stewart (2000) on the roles of cybercafés in the
1990s. Their work on intermediary roles in the
development and appropriation of new technologies,
defines intermediaries as individuals who a) facilitate
user innovation, and b) link user innovation into
supply side activities, such as marketing, branding or
product development (Stewart and Hyysalo, 2008).
Using a more down-to-earth, or even a bland
definition, intermediaries can be seen as ‘go-
betweens’; individuals who bring different people
together, and help them in appropriation and
generation of new technologies (or related
innovations). As such, intermediary is not a fixed
concept or a profession, and there are different
intermediaries in different fields of business, and their
alignment in the supply-use axis may wary
(Lahtiranta, 2014.).
The three-tiered framework used by Stewart and
Hyysalo (2008) to categorize primary roles of
intermediaries, consists of the following: 1)
facilitating, 2) configuring, and 3) brokering. In their
framework, facilitating represents providing
opportunities to other, and as such it covers aspects
such as education, setting rules, influencing
regulations, and gathering and distributing resources.
(Stewart and Hyysalo, 2008)
Configuring does not only represent technology-
related configuring (actually technical aspect of
configuring is often present only in a minor way), but
also creation of space that facilitates appropriation.
Configuring also represents influencing individual’s
perceptions and goals (Stewart and Hyysalo, 2008).
A cybercafé is a prime example of configuring; the
space (café) existed before function, and the clientele
brought in their own ideas on how and for what it is
used (Stewart, 2000).
Brokering, as the name suggests, refers to
negotiating on the behalf of represented organizations
and individuals, for example when features of a new
product are discussed. Brokering is one of the most
direct ways of interacting within the framework, as
the intermediaries are often involved with direct
negotiations with different parties, such as sponsors,
suppliers or end-users. (Stewart and Hyysalo, 2008)
2.2 The Framework and the eHealth
Pilot
In the eHealth pilot, the three-tiered framework was
used in a) outlining the needed skill-set, b) organizing
the lectures, and c) setting up the platform used in
education. As such, the role of the intermediary
(Stewart and Hyysalo, 2008) became intertwined with
the concept of a product owner; a key stakeholder in
project implemented in according to the Agile
approach (Cohn, 2005).
Definition of the skill-set, and gaining
understanding on what kind of professionals are
needed in the field, was done personally – brokered
by a domain-specialist. Instead of formal
questionnaires, public seminars or workshops,
representatives working in the organizations were
met face-to-face (when possible). These meetings
were flexible and informal, there was no written
agenda or minutes, and they were organized on the
terms of the representatives (time and place).
The free-spirited meetings gave room for
exploring additional topics in addition to the skill-set
and the expert profile. These included ongoing
projects, potential avenues for future collaboration,
and the organizations themselves. It followed from
this that the meetings were also about facilitating and
brokering, linking organizations together, and not just
about the project.
In relation to the goals of the eHealth pilot, the
primary result of these 18 meetings was a collection
of topics the organizations considered to be of the
relevance in the field (Figure 2).
The topics covered the field of eHealth in a wide
scale. While some of the topics were extremely
specific, related to a single technology or standard,
others were vaguer by nature, reflecting concerns of
the potential employers.
Example: “We have this problem that is not really
related to technology. When a person starts working
in the company, he or she is rather young, typically in
late twenties. Most of them have never been seriously
ill, neither have their parents. A consequence of this
is that they [new employees] do not know how the
field [of health care] works, or how it is organized.
They can’t separate a health center from a university
hospital.” [Lahtiranta, personal communication,
translated]
The topics were also prioritized using a simple
and straightforward method; if the organizations
Industry-oriented Education in eHealth
413
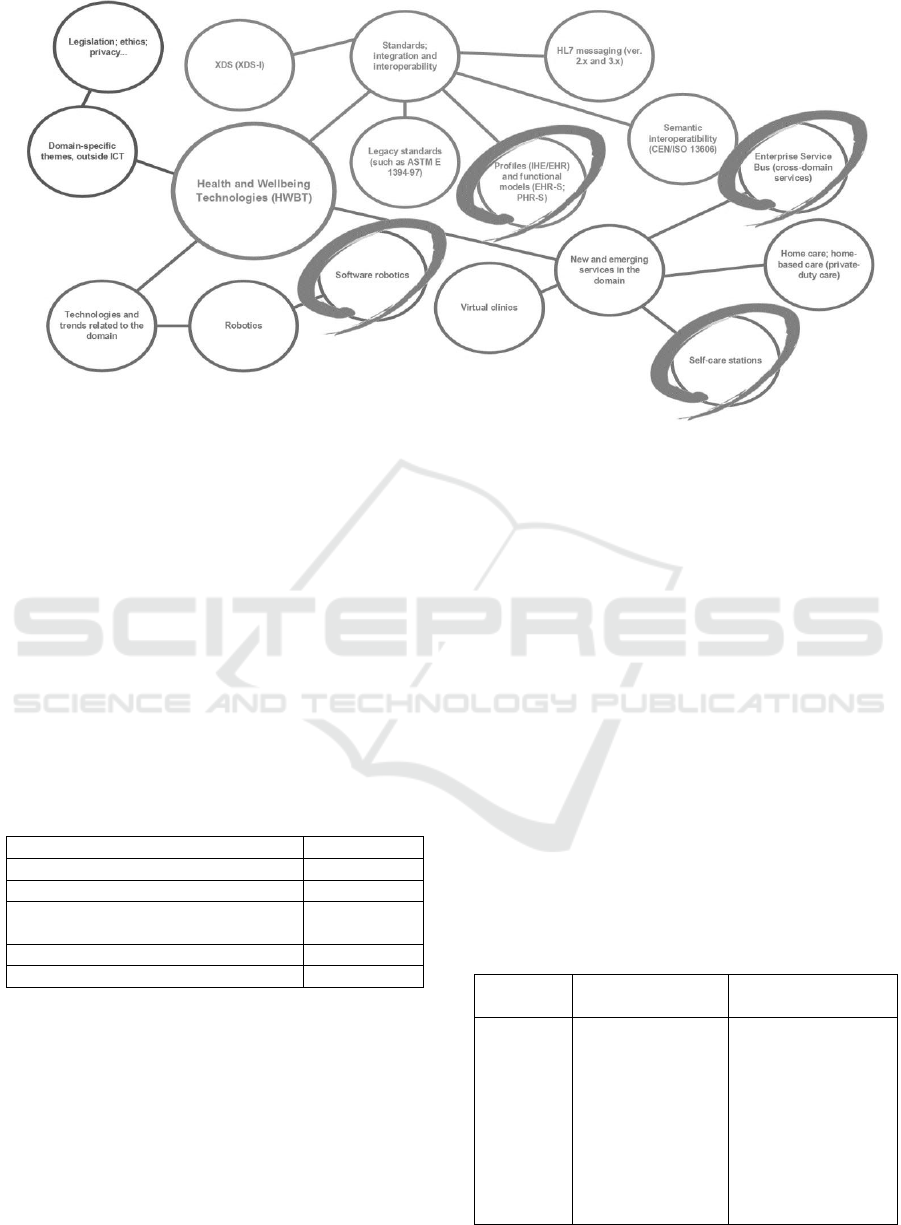
Figure 2: Topics (a sample).
specifically pointed out that certain topic is of the
essence for their business, or if a topic was repeatedly
mentioned in other meetings, it was considered to be
of the essence (indicated by circles in the Figure 2).
Altogether 55 topics of different degrees of
specificity were found out. In order to analyze the
topics in a more detail, they were grouped using the
following categories: a) standards; integration and
interoperability, b) new and emerging services in the
domain, c) technologies and trends related to the
domain, and d) domain-specific themes outside ICT.
Individual topics were distributed according to the
following table (Table 1).
Table 1: Categories and topics.
Category
Distribution
Standards; integration and interoperability
18
New and emerging services in the domain
10
Technologies and trends related to the
domain
18
Domain-specific themes, outside ICT
9
Total
55
In the next phase, the topics were re-grouped into
more concrete groups on the basis of their thematic
and contextual similarities (if there was any). For
example, certain European Union directives
(93/42/EEC, 90/385/EEC and 98/79/EC) formed a
group related to validation and verification. In the
case of messaging, certain standards (ASTM E 1394-
97 and HL7 ver. 2.x) formed a group of their own due
to the similarities in structure and function. These
groups were called thematic groups.
On a more abstract level, thematic groups took the
shape of two distinct collections; introductory and
advanced. The topics that were regarded as
introductory were related to the nature and
organization of health care and social services (e.g.
legislation, funding, etc.). The remaining topics, the
advanced ones, were related to a specific function or
standard, such as the Cross Enterprise Document
Sharing (XDS) standards (Table 2).
As the Table 2 indicates, thematic groups formed
the backbone for the actual lectures. Content and
learning outcomes were defined for each of the
formed group on the basis of literature, domain
knowledge, and earlier discussions with the
companies. In addition, thematic ‘arcs’ were
discussed; how the themes are linked with each other,
what is the actual scope, and how much the themes
overlap (for example, in the case of legislation and
EU directives).
Table 2: Thematic groups (a sample).
Thematic
Group
Content Description
Learning Outcomes
Coding,
classification
and
ontologies
Coding, classification
and ontologies have a
long history in the field
of health care. They
are essential part of
service provisioning
today, and they are
embedded into most
communication
standards in the field.
During the lecture(s), an
introduction to
ontologies is provided,
and some of the most
common coding and
classification systems
(such as SNOMED CT
and ICD-10) are briefly
introduced.
CSEDU 2018 - 10th International Conference on Computer Supported Education
414
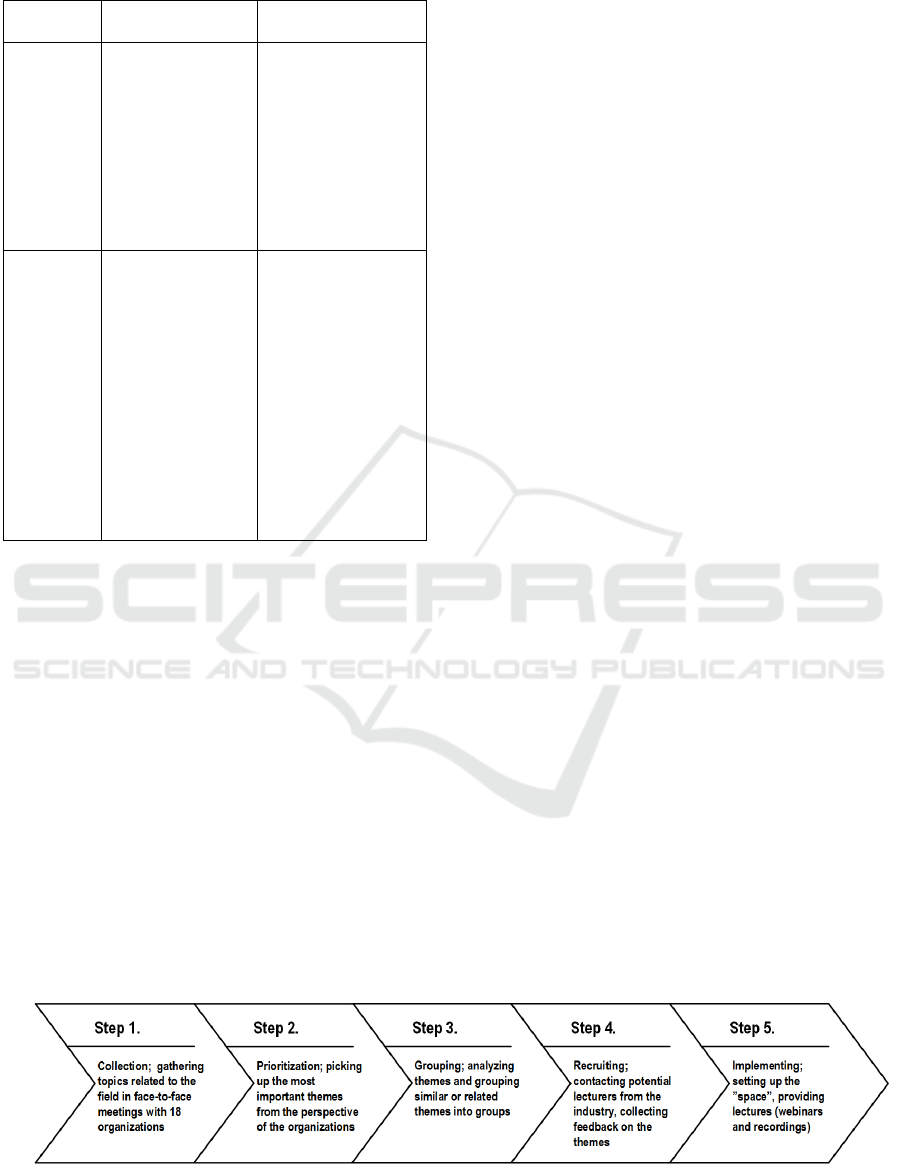
Table 2: Thematic groups (a sample) (cont.).
Thematic
Group
Content Description
Learning Outcomes
Messaging
In the health care
domain, information is
commonly exchanged
in (asynchronous)
messages. Some of
these messages base
on “legacy standards”
were developed in the
1990s but are still in
use.
Starting with ASTM E
1394-97, continuing to
HL7 2.x messaging, and
later on to the up-to-date
HL7 v3 messaging, the
lecture(s) outline the
used standards and
provides practical
examples on their use.
Profiles and
functional
models
Profiles and functional
models provide a
summary of
envisioned functions
for specific information
systems, such as
EHR. Furthermore,
profiles (such as IHE
integration profiles)
define conformance
criteria for such
systems.
The lecture(s) depict the
most relevant functional
models today (such as
PHR-S and EHR-S), and
(localized) integration
profiles used in the field.
In addition the lecture
provides a cursory
glance to IHE Scheduled
Workflow (SWF), and an
introduction to IHE
organization (focusing
on the national special
interest group).
There were no funds reserved for outsourced services,
such as marketing or lectures, in the eHealth pilot.
One consequence of this was that the lecturers had to
be recruited from the industry, domain organizations,
standards development organizations, universities,
and government. All in all, 49 different organizations
were contacted.
As the language of the lectures was English, it was
possible to recruit lecturers internationally. The
recruitment process was also used for collecting
feedback on the original topics, thematic groups, and
on the planned ‘arcs’. As such, the process itself
formed a reflective inspect-and-adapt cycle of its
own, executed in the spirit of Agile development
(Cohn, 2005).
The recruitment process further defined the
thematic groups into actual lectures. While the
original topics (Figure 2) were considered as an
accurate representation of the industry, and needs of
the organizations, the availability and expertise of the
lecturers defined the final content and amount of
lectures (per thematic group). For example, in
addition to giving a generic lecture on trends related
to the field, the lecturers insisted on delving deeper
into specific trends, such as corporate wellness; a
trend that was considered to be of particular
importance.
As the lectures were held in English, and the
recruitment for lecturers was global, the most
practical way of offering lectures was online. Some
of the lectures were webinars with a live audience and
lecturer, while others were recordings made
particularly for the project. The lectures were
recorded using Adobe Connect web conferencing
software service, and they were offered via open-
source learning platform and course management
system known as Moodle.
Employing the taxonomies of the used
methodological framework (Stewart and Hyysalo,
2008), these two (Adobe Connect and Moodle) were
the technical parts of the ‘space’ that was configured
for the purposes of the eHealth pilot, and used for
facilitating expertise and knowledge on eHealth.
In order to summarize the process from definition
to implementation, or from collecting topics to giving
actual lectures, there were 5 steps (Figure 3). First, the
topics were collected in free-form meetings with 1-2
representatives from organizations operating in the
field of eHealth. These included companies,
standards development organizations, universities
and research organizations, and government. The
meetings were held face-to-face when possible. The
collected topics were prioritized and grouped into
thematic groups; assemblages of topics that had
similarities, or were close to each other (context-
wise).
The thematic groups formed the backbone for the
actual lectures, and they were used in recruitment. At
that time, the groups were also subjected for feedback
from potential lectures. The actual lectures were
formed on the basis of the thematic groups and
lecturers’ feedback; their expertise and interests.
Figure 3: Steps 1-5; from definition to implementation.
Industry-oriented Education in eHealth
415

Finally, the lectures were provided via an electronic
teaching platform, or the ‘space’.
Even though the process is depicted as a linear one
in the figure 3, certain steps were repeated. For
example, the composition of thematic groups changed
during the recruitment process, resulting in
regrouping.
The figure 3 can also be used in depicting how
different intermediary roles were aligned during the
overall process. While the content was brokered by a
domain-specialist (steps 1-3) the practical
arrangements (steps 4-5) were primarily – if not
always solely – brokered and configured by the
academic officers. In the following, the challenges
related to the work of the academic officers are
discussed in more detail.
2.3 Practical Arrangement of the
Lectures
Organizing a novel course; especially on a new
domain with tight coupling to industry can be quite
demanding for academic officers working in the Open
University. The practicalities require a lot of
planning, scheduling, brokering, and marketing;
significantly more than in the case of a more typical
or ‘academic’ course.
The lectures and the related materials (handouts,
assignments, etc.) were agreed directly with the
lecturers. During the course of the arranging these
practicalities, it was discovered that sometimes the
language used in the course was a challenge for some
of the lecturers as they were not used to giving
lectures in English. This was considered as too
demanding for some, and in few cases the lecturers
lost their interest.
Another motivational aspect was the
compensation. Some of the lectures refused due to the
small compensations. As discussed earlier, the
eHealth pilot did not have any funding to cover the
lecturing costs. One of the findings of the eHealth
pilot is that investments are needed if experienced
industry specialists are planned to be incorporated
into the education.
Organizing the actual lectures with the potential
lecturers caused some challenges to the Open
University’s academic officers; the lecturers asked
for detailed instructions, for example on the domain-
specific technical aspects of their topic.
Understandably, the officers were not able to answer
to these kinds of questions as they did not possess
sufficient technical know-how on the domain.
It was also identified as a challenge for the Open
University’s academic officers to contact the industry
specialists as they did not have the needed network or
shared the same “language” with them. The academic
officers felt it was quite demanding to call to the
potential lectures and discuss about the practicalities
in-depth.
During the eHealth pilot, four types of challenges
were identified from the perspective of the academic
officers. 1) Scheduling of the lecturers (brokering).
Sometimes it was a challenge to reach lecturers from
the industry-side in order to arrange the schedule of
the lectures. Commonly, the lecturers answered after
the schedule was set. Naturally, this caused changes
to the course setup and structure –eventually, the
effects were evident to the students as well.
As an example, some of the lectures were
originally planned to be available online prior to
assignments, and it was intended that the assignments
base on the contribution. However, the lectures and
the assignments were “out of sync” and this caused
fundamental problems to the organizers, and to the
students.
2) Scheduling of the academic officers
(facilitating). Some of the scheduling problems
originated from the officers, which were a direct
consequence of the somewhat “stop-go” nature of the
course. Planning and practical arrangements (figure
3, steps 4-5) required significantly more time than
was originally estimated – even a partial restructuring
of the timetable required whole working days from
the academic officers. The officers were not solely
assigned to the course, and they had other duties to
attend to.
3) Setting up the online course (configuring). The
original idea was to organize the course as a series of
online lectures, or webinars, into which everyone
interested could attend to. The focus group was not
limited as the course was intended as a low-threshold
introduction to the field, and to the relevant actors
(organizations, companies, researchers, etc.).
However, due to the practical challenges and
problems in scheduling, a decision was made to
implement (to ‘reconfigure’) the course as an online
course with limited access in the Moodle learning
environment. Even though the course was organized
as a closed one (for example, in contrast to a MOOC,
c.f. Baggaley, 2013), the course was successful in
facilitating; in bringing together students from health
care and from the technology side.
4) Student recruitment (brokering). This eHealth-
focused course was a new addition to the course
curricula of the Open University. As such, it needed
new marketing approach. It was not enough just to
add the course to the list of available ones. At first,
the course was marketed using traditional methods,
CSEDU 2018 - 10th International Conference on Computer Supported Education
416

such as via university’s web pages and email
distribution lists. Soon it was realized that in order to
reach the intended audience, potential students
interested in operating in a field that is a mix of
technology and health care, social media channels
had to be utilized as well. In this LinkedIn, Facebook
and Twitter were used as primary channels. In
addition, an interview that focused on the overall
project was published in one of the Finland’s leading
newspapers. This was a real boost in terms of
marketing.
Despite of the practical challenges described
above, the course was successfully carried-out with a
very strong industry connection.
3 RECOMMENDATIONS
Looking back to the eHealth pilot, more precisely into
the 5 steps depicted in the figure 3, the following
recommendations can be made. The
recommendations are not intended as domain or
project specific, and as such they can be applied to the
field of industry-oriented education as a whole.
Use a domain expert as an intermediary (Step 1).
Regardless of the domain, planning industry-oriented
education requires understanding about the industry.
Without a solid understanding about the domain in
question, eliciting information from different sources
(stakeholders, literature, media, etc.) is a challenge.
The domain in itself; its processes, terminology,
hierarchy, etc. may pose a challenge for the
uninitiated. More so if the domain is a hybrid one, as
it is in the case of eHealth. In the case of eHealth,
domain understanding is not just about technology.
Depending on the emphasis, it is also about health
care, social services, and wellbeing.
Domain expertise is related to another important
requirement; networks. Without them, there is a risk
that a certain stakeholder group will go unnoticed, of
its views are not appropriately incorporated in the
planning. For example, in the field of eHealth,
different standards development organizations, such
as the HL7, are of particular importance.
Prefer face-to-face meetings (Step 1). Personal
touch matters. In the eHealth pilot, the representatives
of different organizations appreciated doing things
‘on their terms’ (time, place, etc.). A direct result of
this way of working was a more laid-back
atmosphere, and a possibility to act as an
intermediary. In other words, to bring issues on the
table that would have been otherwise ignored, or left
outside the official agenda.
Meeting face-to-face was also a matter of
efficiency. Instead of communication via email or
phone, in personal meetings it was easier to control
the flow of the meetings; to ensure that everyone was
engaged and participated, and contributed to the
eHealth pilot.
Prioritize! (Step 2). Collecting singular themes
was not enough in the eHealth pilot; they needed
further work and thinning out. Prioritization of the
individual themes on the basis of the corporate needs
was the first step in the right direction. A simple
method that based on the number of occurrences a
theme was brought up, combined with emphasis
brought up in the meetings, was enough.
However, in an afterthought this analysis could
have been strengthened by analyzing future trends
provided by organizations such as Gartner or Forbes
(cf. Forbes, 2017). This kind of analysis would have
given more to the organizations, and even challenged
them to reconsider their current position and future
avenues in the field. The analysis could have even
helped in brokering (Stewart and Hyysalo, 2008), if a
common ground had been found in the fields of
expertise and interest.
Sharpen up and clarify (Step 3). As the process of
planning industry-oriented education moves towards
more practical issues, such as organizing lectures,
structuring content into manageable content is of the
essence. More so, if the lectures are provided by more
than a one person, or with external professionals. In
this, defining content, learning outcomes, and
creating thematic arcs that linked themes together was
a valuable tool in the eHealth pilot.
I&A (Step 4). Inspect and adapt. Reflecting the
current state of the project and comparing the results
on the goals is a basic practice employed in most
project management paradigms. Instead of
performing analysis retrospectively after the project,
iterative and incremental inspect and adapt cycles
were performed during the eHealth pilot in the spirit
of Agile approach (Cohn, 2005).
Each meeting with a company provided a point of
reflection on the themes gathered until that point. The
most natural point of reflection where the ‘whole’
(i.e. thematic groups) could be evaluated for the first
time instead of the ‘parts’ (individual themes) was
during the recruitment. At that point, the actual
lectures, and the emphasis of the whole education,
started to take shape.
Resource adequately (Step 4). Another
recommendation that originates from the generic
project management paradigms is related to adequate
resourcing. There was a single step in the eHealth
pilot during which the resourcing was found
Industry-oriented Education in eHealth
417

insufficient; recruiting. Professional lecturers rarely
come cheaply, or for free, especially if the topic of the
lecture is a current one.
In the eHealth pilot, the whole field is a current
one, especially in Finland, and certain themes even
more so (such as the Fast Healthcare Interoperability
Resource, or FHIR). The lack of resources made
recruiting potential lecturers a challenge.
Another aspect, related to resources and
recruiting, which had an impact on the content of the
lectures was the HL7 membership. Even though the
national organization collaborated and contributed,
the international HL7 organization was
understandably reluctant to contribute as the
organization responsible for the education was not a
member at that time.
Advocate (Step 5). Another old best practice
originating from project management is advocating.
A well-managed project needs a ‘champion’ (Cash.
and Fox, 1992); an unfeigned and authoritative
character who carries the weight of the project. In the
eHealth pilot, this practice should have been put into
a proper use as the project stumbled at a critical point,
during the handover from planning the course to
making the webinars and recordings.
Revalidate (overall process). Industry-oriented
education needs periodic revalidation (unless it is
intended as non-recurring education). More so of the
domain is a rapidly evolving one, as in the case of
eHealth. During the eHealth pilot two basic types of
revalidation were discussed: 1) a calendar-based
revalidation, and 2) a trigger-based revalidation.
A calendar-based revalidation could occur yearly
or bi-yearly depending on the field. During the
process, the education as a whole could be put under
scrutiny. Depending on the implementation of the
education, this could be done at the same time when
the practicalities are organized (time, place, lectures,
etc.), or within a specific frame of time.
A trigger-based revalidation was seen as a more
narrow process. Instead of looking into education as
a whole, single topics or thematic groups could be put
under scrutiny. The trigger, a real-world event, could
be a release of a new standard, law or directive, or
announcement of a project in need of a specific
expertise (such as the Apotti (2017) project discussed
earlier).
While these mechanisms were never put into
actual use due to the nature of the ICT pilot (figure 1),
they were considered as mechanisms that could be
used in maintaining the original connection with the
industry.
4 CONCLUSIONS
Industry-oriented education is a ‘different animal’
when compared to the education Humboldtian
science universities commonly offer. Unlike courses
like ‘discrete mathematics’, where the underlying
paradigms may remain the same for decades,
industry-oriented education may change with every
course iteration.
This difference does not make offering industry-
oriented education impossibility for the science
universities; it just needs a different mind-set and
different practices. Such as the one’s discussed
earlier. As the competition among universities has
become intense and international, and the demand for
research funding has increased globally, industry-
oriented education should be regarded as an opening
and an opportunity for closer cooperation with the
industry. In this, the intermediary roles (Stewart and
Hyysalo, 2008; Lahtiranta, 2014) can be of the
essence.
Understanding a) how universities align on the
supply-use axis from the perspective of the industry,
b) what the expected skill-set and the profile of a
specific domain expert are, and c) how intermediary
roles can be used in interaction with the industry are
steps in the right direction on a grander scheme of
things that is the balance between education and
industry demand.
ACKNOWLEDGEMENTS
The project called “Working Life Oriented Open
University Education (2015-2018) on which the
paper bases on was funded by the European Social
Fund.
REFERENCES
Apotti. 2017. Apotti: usein kysytyt kysymykset, URL=
http:// www.apotti.fi/usein-kysytyt-kysymykset/
(Accessed: 4.10.2017).
Baggaley, J. 2013. MOOC Rampant. Distance Education.
34, 3, pp. 368-378.
Cash, C. and Fox, R 1992. Elements of Successful Project
Management. Journal of Systems Management. 43, 9
(Sep 1992), pp. 10-12.
Cohn, M. 2005. Agile Estimating and Planning. Prentice
Hall, New Jersey, U.S.
El-Bishouty, M. M., Chang, T.-W., Graf, S., and Chen, N.-
S. 2014. Smart e-course recommender based on
CSEDU 2018 - 10th International Conference on Computer Supported Education
418

learning styles. Journal of Computers in Education, 1,
99–111.
Fathi, M. and Wilson, L. 2009. Strategic planning in
colleges and universities. The Business Renaissance
Quarterly: Enhancing the Quality of Life at Work.
Spring 2009, 91-103
Forbes. 2017. Top Five Digital Transformation Trends In
Health Care URL=
https://www.forbes.com/sites/danielnewman/2017/03/
07/top-five-digital-transformation-trends-in-
healthcare/ (Accessed: 4.10.2017).
García-Peñalvo, F. J., Cruz-Benito, J., Griffiths, D.,
Sharples, P., Willson, S., Johnson, M., Papadopoulos,
G., Achilleos, A., Alier, M., Galanis, N., Conde, M.Á.,
Pessot, E., Elerink, R., Veenendaal, E., and Lee, S.
2014. Developing Win-Win Solutions for Virtual
Placements in Informatics: The VALS Case. In F. J.
García-Peñalvo (Ed.), Proceedings of the Second
International Conference on Technological Ecosystems
for Enhancing Multiculturality (TEEM’14) (pp. 733-
738). New York, USA: ACM.
Gerson, E.M. 2015. The interaction of research systems in
the evo-devo juncture. In Conceptual Change in
Biology: Scientific and Philosophical Perspectives on
Evolution and Development. A.C. Love, Ed. Springer,
New York, U.S., 442-458. DOI=
dx.doi.org/10.1007/978-94-017-9412-1
Helsingin Sanomat. 2015. Una avaa yli miljardin euron
pelin. Helsingin Sanomat, September 4, 2015. URL=
http://www. hs.fi/kotimaa/a1441254356635 (Accessed:
20.4.2016).
Kauppalehti. 2015. Terveysteknologian vienti rikkoi ennä-
tyksiä. Kauppalehti, April 9, 2015. URL=http://www.
kauppalehti.fi/uutiset/terveysteknologian-vienti-rikkoi-
ennatyksia/AjFvuGRg (Acccessed: 4.10.2017)
Koskinen, J. and Knaapi-Junnila, S. 2014. Information
technology – the unredeemed opportunity to reduce
cultural and social capital gap between citizens and
professionals in healthcare. In ICT and Society, 11th
IFIP TC 9 International Conference on Human Choice
and Computers HCC11. K. Kimppa, D. Whitehouse, T.
Kuusela, and J. Phahlamohlaka, Eds. Springer, Turku,
July 30 - August 1, 2014, 333-346, DOI=dx.
doi.org/10.1007/978-3-662-44208-1_27
Krausz M., Ward J. & Ramsey D. 2016. From Telehealth to
an Interactive Virtual Clinic. In: Mucic D., Hilty D.
(Eds.) e-Mental Health. Springer
DOI=https://doi.org/10.1007/978-3-319-20852-7_15
Lahtiranta, J. 2014. New and Emerging Challenges of the
ICT-Mediated Health and Well-Being Services.
Doctoral Thesis. Turku Centre for Computer Science.
URL= http:// www.doria.fi/handle/10024/96886
(Accessed: 4.10.2017).
Lahtiranta, J., Koskinen, J.S.S. and Nurminen, M. 2015.
Sensemaking in personal health space, Information
Technology and People, 28, 4, 790-805, DOI=http://dx.
doi.org/ 10.1108/ITP-09-2014-0214
Lasi, H., Fettke, P., Kemper, H., Feld, T., and Hoffman, M.
2014. Industry 4.0. Business & Information Systems.
4,1 (Aug. 2014), 239-242.
DOI=dx.doi.org/10.1007/s12599-014-0334-4
Lozano, R., Lukman, R., Lozano, F.J., Huisingh, D., and
Lambrechts, W. 2013. Declarations for sustainability in
higher education: becoming better leaders, through
addressing the university system. Journal of Cleaner
Production. 48,1, 10-19. DOI=
http://dx.doi.org/10.1016/ j.jclepro.2011.10.006
Saranen Consulting. 2015. Terveysteknologia-alalle tulossa
yli tuhat uutta työpaikkaa ensi vuonna. URL=
http://www.
saranen.fi/uutiset/terveysteknologia_alalle_tuhat_tyop
aikkaa/ (Accessed: 4.10.2015)
Stewart, J. and Hyysalo, S. 2008. Intermediaries, users and
social learning in technological innovation.
International Journal of Innovation Management. 12,
3, pp. 295-325, DOI=
dx.doi.org/10.1142/S1363919608002035
Stewart, J. 2000. Cafematics: the cybercafé and the
community. In Community Informatics. M. Gurstein,
Ed. Idea Group Publishing, 320-338, DOI=
http://dx.doi.org/ 10.4018/978-1-878289-69-8.ch015
Industry-oriented Education in eHealth
419
