The Impact of Diabetes Mellitus on the Physical Health and
Physical Activity
Zivana Gavric
1,2
, Dragana Grujic-Vujmilovic
1,2
and Miodrag Marjanovic
1
1
The Public Health Institute Republic of Srpska, Jovan Ducic 1, Banja Luka, Bosnia and Herzegovina
2
Department of Social Medicine, Faculty of Medicine University Banja Luka, Banja Luka, Bosnia and Herzegovina
Keywords: Diabetes Mellitus, Quality of Life, Physical Health, Physical Activity.
Abstract: Chronic diseases affect the quality of life and all components of the health, and they decrease physical
activity. The aim of the research was to assess how diabetes mellitus affects the physical health component
in relation to sex, age and level of education. For survey research at the Clinical Center of Banja Luka in the
period from October 2011 to June 2012, which included 150 patients with diabetes mellitus, we used a
questionnaire of the World Health Organization (WHOQOL-BREF). The mean score for physical domain
of health were slightly higher in male patients (57.92), but without statistically significant difference (t =
1.256; p >0.05) compared to female respondents. With a statistically significant difference (p <0.01) the
mean scores for the physical domain of health were higher among younger respondents and those with
higher education and those mean scores declines with age and with lower levels of education. Mean score
were highest in unmarried people, followed by married but without statistically significant difference
(p>0.05) compared to divorced and widower. In our patients, diabetes mellitus has an impact on the
physical health component and restrict certain physical activities, especially in patients who are older and
with lower education.
1 INTRODUCTION
Ancient scientific evidence and an increase in
epidemiological facts suggest that “healthy eating
habits and moderate exercise can reduce the
incidence of heart attacks, diabetes and non-
communicable diseases” (WHO, 2002, page 8).
„Physical inactivity is a global health problem that
causes more than two million deaths each year
making it one of the top 10 leading causes of death
and disability“(WHO, 2002, page 2). „The
increasing global problem of NCDs means that
obesity, poor diet and inactivity are increasing
problems for countries in the epidemiological
transition“(Waxman, 2004, page1). “Chronic
diseases are characterized by long duration and slow
progression and they are the leading cause of death
worldwide among which the most important are:
heart diseases, stroke, cancer, chronic respiratory
diseases and diabetes, making 63% of all deaths”
(WHO, 2012, page 6). In 2004, in the world,
diabetes mellitus, in the total burden of disease,
occupied 19 place with a share of 1.3% DALY's, and
it is anticipated that by 2030 the total burden of
disease occupy 10th place with a share of 2.3%
DALY- a " (WHO, 2008, page 22-23). Chronic
diseases affect the quality of life and all components
of the health, and they decrease physical activity.
According to Sigal et all. (2004): Adaptations to
endurance exercise enable the muscle to use O2 and
blood-borne fuels, whereas those for resistance
exercise lead to improved force generation (e.g.,
hypertrophy, contractile properties). Of specific
interest to people with diabetes are those adaptations
that directly affect the metabolism of glucose. (Page
2522) According to Sigal et all. (2004): Before
beginning a program of physical activity more
vigorous than brisk walking, people with diabetes
should be assessed for conditions that might
contraindicate certain types of exercise or predispose
to injury (e.g., severe autonomic neuropathy, severe
peripheral neuropathy, or preproliferative or
proliferative retinopathy), which require treatment
before beginning vigorous exercise, or that may be
associated with increased likelihood of CVD. The
patient’s age and previous physical activity level
should be considered (Page 2523). According to
Guelfi KJ et all. (2005): Exercise in diabetes,
particularly T1DM, can predispose patients to
150
Gavric, Z., Grujic-Vujmilovic, D. and Marjanovic, M..
The Impact of Diabetes Mellitus on the Physical Health and Physical Activity.
In Proceedings of the 3rd International Congress on Sport Sciences Research and Technology Support (icSPORTS 2015), pages 150-155
ISBN: 978-989-758-159-5
Copyright
c
2015 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
hypoglycaemia. The most rapid drop in blood
glucose usually occurs during aerobic or endurance
exercise, when circulating insulin suppresses
metabolic fuel production and increases glucose
uptake into muscles, but an attenuated drop in blood
glucose is also seen with intermittent high-intensity
exercise (which is a mixture of both aerobic and
anaerobic exercise, characteristic of team sports and
children's play) ( Page 1289). “Hypoglycaemia can
also occur after all types of exercise, often
overnight, most likely because of a combination of
increased insulin sensitivity and the need to
replenish depleted energy stores”( McMahon SK,
2007, page 260). Graveling and Frier (2010): An
extreme case is hypoglycaemia-associated
autonomic failure, where a vicious cycle of recurrent
hypoglycaemia develops. This occurs because
exercise blunts the endocrine response to
hypoglycaemia, but hypoglycaemia also blunts the
endocrine response to exercise, and in extreme cases
can result in significant morbidity (Page 587).
According to WHO (1998): Quality of life is defined
by the WHO as “individuals' perceptions of their
position in life in the context of the culture and value
systems in which they live and in relation to their
goals, expectations, standards and concerns”. This
definition reflects the view that quality of life refers to
a subjective evaluation, which is embedded in a
cultural, social and environmental context. The
physical domain of quality of life includes: the
aspect of pain and discomfort, energy and fatigue,
sleep and rest, activities of daily living, dependence
on medication or treatment and work capacity
(Pages 7, 48).
Objective: Assess how diabetes mellitus affects
the component of physical health in relation to sex,
age and level of education.
2 METHODS
With survey research at the Clinical Center of Banja
Luka in the period from October 2011 to June 2012,
we have covered 150 patients with diabetes mellitus.
For the assessment of quality of life, we used a
questionnaire of the World Health Organization
(WHOQOL-BREF). WHOQOL User Manual
(1998): Assessing the quality of life was within the
last 2 weeks. Answers were given on a Likert scale
of 1-5, with 1 being the least and 5 being the highest
agreement, and then the answers were transformed
into points, in two steps, within the 0-100 scale. A
higher score represents greater ("better"), and a
smaller number of points represent a lower
("worse") level of functioning. The questionnaire
contained a number of questions on socio-
demographic condition (age, sex, level of
education).
3 RESULTS
From a total of 150 patients with diabetes mellitus,
58.0% were male and 42.0% female, with average
age of 56 (± 12.4) years, most were aged 30 to 59
years (53.3%) and over 60 years (41.3%). In relation
to the level of education the highest percentage of
respondents had secondary (48%) and primary
(20%) level of education. According to marital
status 2/3 (66.7%) were married, and 1/5 (20%)
were divorced/widower. (Table 1)
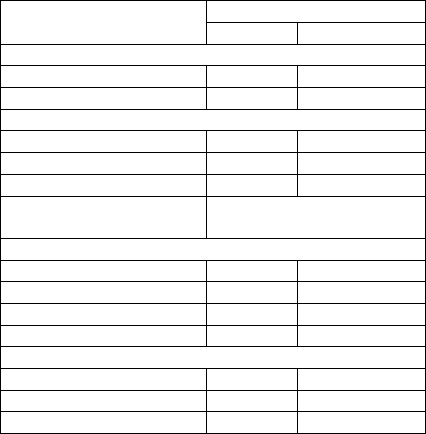
Table 1: Sociodemographic characteristics of the sample.
Variables Respondents (N=150)
n %
Gender
Male 87 58.0
Female 63 42.0
Age
<30 8 5.3
30-59 80 53.3
≥60 62 41.3
Min- Max
Me (±SD)
21-75
55.95±12.4
Level of education
Unfinished primary 20 13.3
Primary 30 20.0
Secondary 72 48.0
High/college 28 18.7
Marital status
Single 20 13.3
Married 100 66.7
Divorced/Widowed 30 20.0
The higher percent of women but without
statistically significant difference compared to male
patients feel that physical pain prevents them from
doing what they need to do; that they need medical
treatment to function in everyday life; that they do
not have enough energy for everyday life; assessed
their ability to get around poor and very poor, and
they were very dissatisfied and dissatisfied with
sleep. Male patients were more satisfied and very
satisfied with their ability to perform daily activities
and very dissatisfied and dissatisfied with their
capacity for work, but without statistically
significant differences compared to female patients.
(Table 2)
The Impact of Diabetes Mellitus on the Physical Health and Physical Activity
151
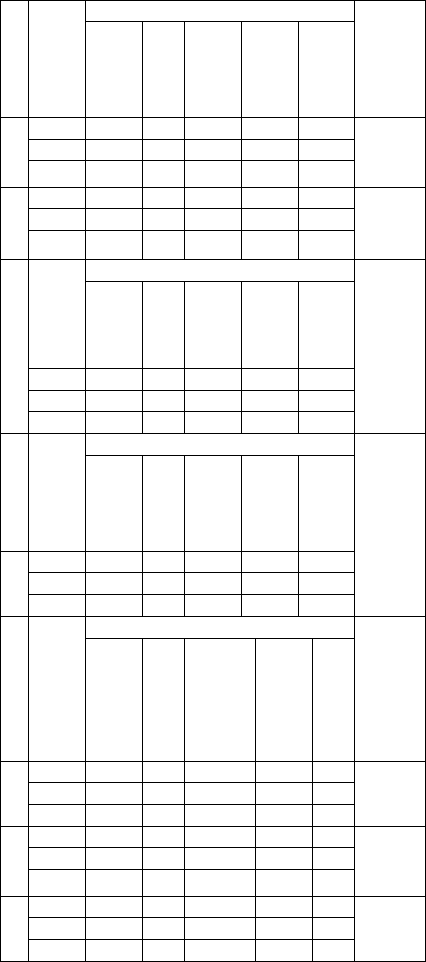
Table 2: Answers of questions* in relation to gender.
Quest
i
o
n
s
Genderº
Answers (%) Kruskal
Wallis
Test*
Not at all
A little
A moderate
amount
Very much
An extreme
amount
1 M 25.3 25.3 28.7 9.2 11.5
2496.6
P=0.34
F 19.0 27.0 27.0 11.1 15.9
T 22.6 26.0 28.0 10.0 13.3
2 M 8.0 9.2 33.3 41.4 8.0
2618.5
P=0.63
F 1.6 17.5 30.2 36.5 14.3
T 5.3 12.7 32.0 39.3 10.7
3
Gende
r
Answers (%)
2527.5
P=0.39
Not at all
A little
Moderately
Mostly
Completely
M 4.6 13.8 19.5 40.2 21.0
F 9.5 12.7 23.8 33.3 20.6
T 6.7 13.3 21.3 37.3 21.3
Gende
r
Answers (%)
2322.0
P=0.09
Very poor
Poor
Neither poor
nor good
Good
Very good
4 M 3.4 13.8 31.0 35.6 16.1
F 3.2 22.2 36.5 27.0 11.1
T 3.2 17.3 33.3 32.0 14.0
Gende
r
Answers (%)
Very dissatisfie
d
Dissatisfie
d
N
either satisfied
nor dissatisfie
d
Satisfie
d
Very satisfie
d
5 M 1.1 31.0 21.8 32.2 13.8
2390.0
P=0.17
F 9.5 27.0 27.0 28.6 7.9
T 4.7 29.3 24.0 30.6 11.3
6 M 2.2 13.8 24.1 50.6 10.3
2584.5
P=0.52
F 3.2 12.7 25.4 54.0 4.8
T 2.0 13.3 24.7 52.0 8.0
7 M 4.6 24.1 26.4 35.6 9.2
2670.0
P=0.78
F 3.2 23.8 20.6 50.8 1.6
T 4.0 24.0 24.0 42.0 6.0
ºM-men; F-females; T-total
*Questions of the physical domain of quality of life:
1. To what extent do you feel that physical pain
prevents you from doing what you need to do?
2. How much do you need any medical treatment to
function in your daily life?
3. Do you have enough energy for everyday life?
4. How well are you able to get around?
5. How satisfied are you with your sleep?
6. How satisfied are you with your ability to perform
your daily living activities?
7. How satisfied are you with your capacity for work?
Without statistically significant differences more
than half of the patients of in all age groups said they
need any medical treatment to function in everyday
life, and that they are satisfied and very satisfied
with the ability to perform daily activities. With a
statistically significant difference with the increase
of age very much and an extreme amount feel that
pain (physical) prevents them to do what they want
to do (p = 0.037); that not at all and a little have
enough energy for daily living (p = 0.005); that their
ability to get around is very poor and poor (p =
0.000); that they are very dissatisfied and
dissatisfied with their sleep (p = 0.025) and that they
were very dissatisfied and dissatisfied with their
capacity for work (p = 0.004). (Table 3)
Half of the respondents (50%) with unfinished
primary school said that physical pain prevents them
from doing what they need to do, but without
statistically significant difference in relation to
persons with secondary (19.4%) and high education
(14.2%). With the increase of the level of education
decreases dissatisfaction among patients, so with
statistically significant difference in higher
percentage patients without primary education said
they very much (20%) and an extreme amount
(30%) need medical treatment to function in
everyday life, and that they not at all (25%) have
enough energy for everyday life, that they have poor
(40%) ability to get around and that they are
dissatisfied with sleep (60%); with ability to perform
daily living activities (30%) and with a capacity for
work (60%) compared to patients with secondary
and higher education. (Table 4)
Mean score for the physical domain of health in
patients with diabetes mellitus were slightly higher
in male patients (57.92), but without statistically
significant difference (t = 1.256; p >0.05) compared
to female respondents. With a statistically significant
difference (p <0.01) the mean scores for the physical
domain of health were higher among younger
respondents and the mean score declines with age.
Mean score with a statistically significant difference
(p <0.01) decrease with decrease of the level of
education so that the highest value is for those with
higher education and the lowest in patients without
primary education. Mean score for the physical
domain of health in patients with diabetes mellitus
were highest in unmarried people followed by
married but without statistically significant
difference (p> 0.05) compared to divorced/widowed.
(Table 5)
icSPORTS 2015 - International Congress on Sport Sciences Research and Technology Support
152
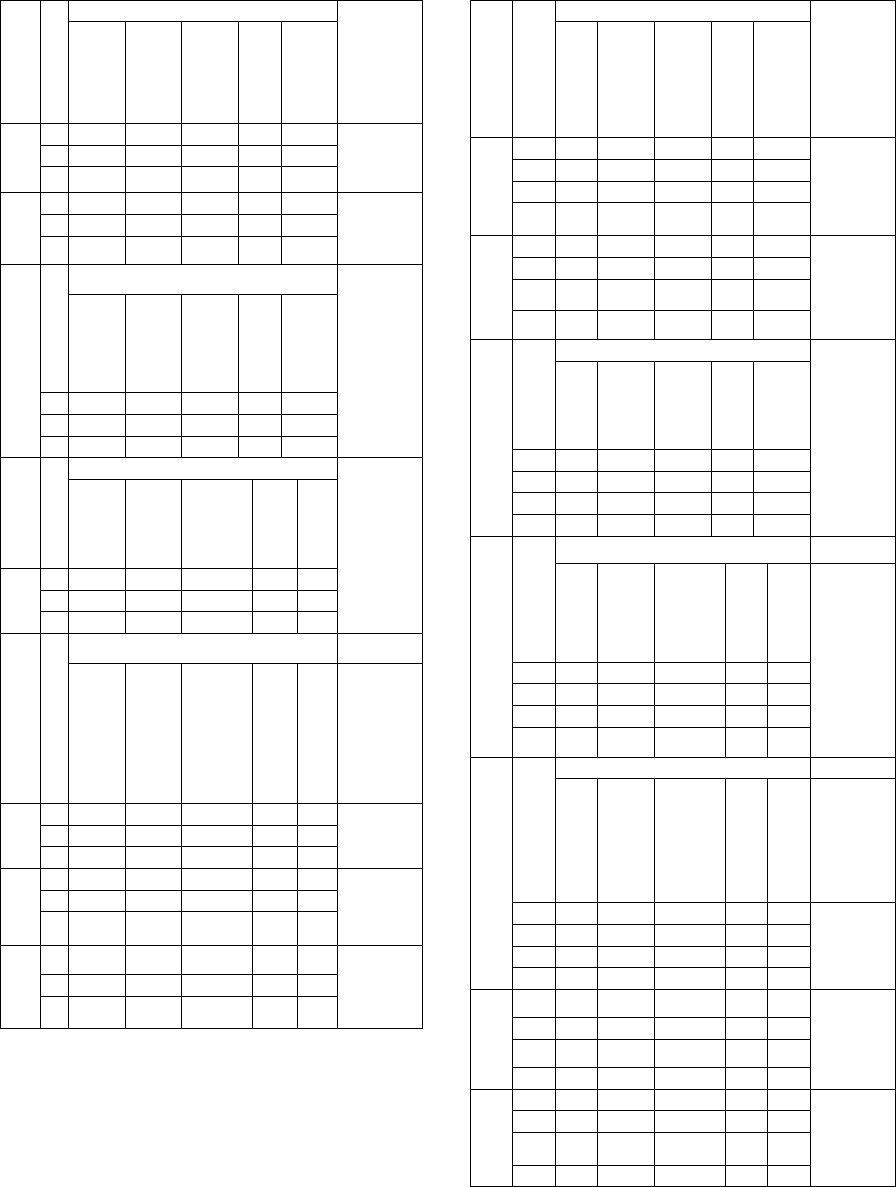
Table 3: Answers of questions* in relation to age.
Questions
A
ge
**
Answers (%) Kruskal
Wallis
test
Not at all
A little
a moderate
amount
Very much
An extreme
amount
1 1 37.5 62.5 0.0 0.0 0.0
10.245
p=0.037
2 17.5 32.5 33.8 6.3 10.0
3 27.4 12.9 24.2 16.1 19.4
2 1 12.5 25.0 12.5 12.5 37.5
8.185
p=0.085
2 5.0 17.5 32.5 33.8 11.3
3 4.8 4.8 33.9 50.0 6.5
3
A
ge
Answers (%)
14.821
p=0.005
Not at all
A little
Moderately
Mostly
Completely
1 0.0 0.0 0.0 50.0 50.0
2 3.8 13.8 21.3 40.0 21.3
3 11.3 14.5 24.2 32.3 17.7
A
ge
Answers (%)
31.821
p=0.000
Very poor
Poor
Neither
poor nor
good
Good
Very good
4 1 0.0 0.0 0.0 37.5 62.5
2 3.8 10.0 32.5 36.3 17.5
3 3.2 29.0 38.7 25.8 3.2
A
ge
Answers (%)
Very dissatisfied
Dissatisfied
Neither satisfied
nor dissatisfied
Satisfied
Very satisfied
5 1 12.5 0.0 12.5 50.0 25.0
11.187
p=0.025
2 1.3 25.0 27.5 32.5 13.8
3 8.1 38.7 21.0 25.8 6.5
6 1 0.0 0.0 12.5 62.5 25.0
7.873
p=0.096
2 1.3 10.0 28.8 48.8 11.3
3 3.2 19.4 21.0 54.8 1.6
7 1 0.0 0.0 0.0 100 0.0
15.099
p=0.004
2 2.5 18.8 26.3 42.5 10.0
3 6.5 33.9 24.2 33.9 1.6
**Age: 1. <30; 2. 30-59; 3. ≥60
Table 4: Answers of questions* in relation to education.
Questions
***Education
Answers (%) Kruskal
Wallis
test
Not at all
A little
A moderate
amount
Very much
An extreme
amount
1 1 20.0 10.0 20.0 20.0 30.0
5.943
p=0.114
2 30.0 26.7 20.0 6.7 16.7
3 19.4 26.4 34.7 9.7 9.7
4 25.0 35.7 25.0 7.1 7.1
2 1 5.0 5.0 0.0 90.0 0.0
12.136
p=0.007
2 0.0 10.0 30.0 40.0 20.0
3 6.9 9.7 43.1 29.2 11.1
4 7.1 28.6 28.6 28.6 7.1
3
Answers (%)
16.295
p=0.001
Not at all
A little
Moderately
Mostly
Completely
1 25.0 25.0 30.0 10.0 10.0
2 6.7 13.3 30.0 30.0 20.0
3 2.8 12.5 20.8 37.5 26.4
4 3.6 7.1 7.1 64.3 17.9
4
Answers (%)
Very poor
Poor
Neithe
r poor
nor
good
Good
Very good
25.669
p=0.000
1 15.0 40.0 30.0 15.0 0.0
2 6.7 20.0 40.0 26.7 6.7
3 0.0 12.5 38.9 31.9 16.7
4 0.0 10.7 14.3 50.0 25.0
5
Answers (%)
Very dissatisfie
d
Dissatisfie
d
Neither
satisfied nor
d
i
ssat
i
s
fi
ed
Satisfie
d
Very satisfie
d
1 5.0 60.0 10.0 25.0 0.0
13.918
p=0.003
2 10.0 36.7 23.3 26.7 3.3
3 4.2 20.8 25.0 29.2 20.8
4 0.0 21.4 32.1 42.9 3.6
6 1 10.0 30.0 25.0 35.0 0.0
10.971
p=0.012
2 0.0 13.3 26.7 60.0 0.0
3 0.0 11.1 27.8 45.8 15.3
4 3.6 7.1 14.3 71.4 3.6
7 1 10.0 60.0 0.0 30.0 0.0
14.266
p=0.003
2 6.7 30.0 23.3 36.7 3.3
3 2.8 15.3 30.6 41.7 9.7
4 0.0 14.3 25.0 57.1 3.6
***Level of education 1-unfinished primary; 2-primary;
3-secondary; 4-high/college
The Impact of Diabetes Mellitus on the Physical Health and Physical Activity
153
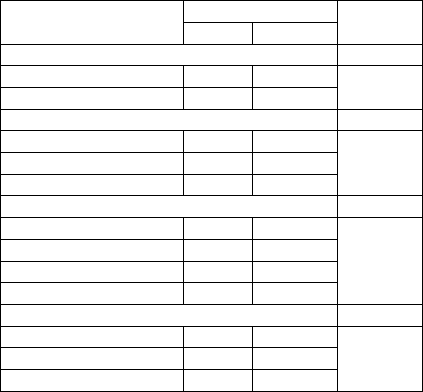
Table 5: Mean scores for the physical domain of health
relation to sociodemographic characteristics.
Variables Physical domain t-test
F-test
Me ±SD
Gender
Male 57.92 19.57 T=1.256
P=0.211
Female 53.85 19.59
Age
<30 75.00 11.29 F=6.306
P=0.000
30-59 62.65 17.65
≥60 49.94 19.84
Level of education
Unfinished primary 38.75 19.84 F=9.397
P=0.000
Primary 51.79 17.91
Secondary 60.02 18.09
High/college 63.63 17.25
Marital status
Single 60.89 19.65 F=0.743
P=0.477
Married 55.89 20.27
Divorced/Widowed 54.17 17.37
4 DISCUSSION
People with diabetes mellitus in our sample had a
mean score for the physical domain of quality of life
(mean score 56.21 ± 19.62) lower than patients with
diabetes mellitus in Denmark (mean score 76.6)
(Nørholm,2001, page 234.), in Iran (mean score
63.75 ± 15.59) (Aghamollaei, 2003, page 56), in
Maryland (mean score 61 ± 29) (Hill-Briggs, 2002,
page 414), in Emirates (mean score 61.8±14.3)
(Bani-Issa,2011, page 827), and higher value in
relation to the mean score (mean score
51.31±19.087) of respondents in the study in Serbia
(Bosić-Živanović, 2012, page 860).
Without statistically significant difference in our
study female had a lower mean score compared to
male patients. In a study in Tokat in Turkey mean
score were significantly lower in women for
physical health domain (Saatcioglu, 2008, page
108), as well as in a study of Bandar Abbas clinic in
Iran (Aghamollaei, 2003, page 56) in study in
Greece (Papadopoulos, 2007, page 4). Statistically
significant lower mean score in the area of physical
functioning in women were in the study conducted
in Estonia (Kalda, 2008, page 24), and in a study in
Japan, women have reported a significantly higher
percentage of problems in the dimension of mobility
than men (Sakamaki, 2006, page 50).
In our study, the mean score statistically
significant declined with age, as well as in a study in
the United States (Glasgow, 1997, page 564). As
well in Study in the Netherlands older age was
associated with statistically significantly greater
frequency of problems in dimension of mobility
(Redekop 2002, page 461). In 240 patients with type
I and type II diabetes mellitus, both groups of
patients had statistically significant worse physical
functioning with increase of age in a study in Boston
(Jacobson, 1994, page 270). People with diabetes
mellitus aged with and over 70 years in study in
Japan reported statistically significantly more
problems in the dimension of mobility and the
dimension of everyday activities than people in other
age groups (Sakamaki, 2006, Page50). There was no
association between age and assessment of quality of
life in the study in Bandar Abbas clinic
(Aghamollaei, 2003, page 56) as well as in study in
Ile -Ifa in Nigeria (Kolawole, 2009, page 163).
The association between level of education and
quality of life assessment was also found in a study
in Bandar Abbas in Iran in which educated patients
had a better quality of life at all scales. Illiterate
patients had poorer estimation of the quality of life
on all scales in relation to patients who were literate
(Aghamollaei, 2003, page 56). Contrary to the
findings of these studies are the findings in Ile-Ifa
(Kolawole, 2009, page 163) and Gaza (Eljedi, 2006,
page 5) in which there was no significant correlation
between the assessment of quality of life and level of
education. Exercise has many health benefits, and
these are important in both T1DM and T2DM.
It is important to be aware that both
hypoglycaemia and hyperglycaemia can occur
during exercise, but strategies are available to deal
with these challenges. (Lumb , 2014, pager 675)
5 CONCLUSION
In our patients, diabetes mellitus has an impact on
the physical health component and restrict certain
physical activities, especially in patients who are
older and with lower education. A more complete
picture would be if we have studied the level of
physical activity that was present before the disease
and restrictions that have resulted from these chronic
diseases, because the physical activity is essential
for the regulation of blood glucose levels as well as
for the functioning of the insulin. What is evident in
our patients is that the level of education affects the
quality of life of the patient in the physical
component of health, and that people with higher
education have better mean score for the physical
component of quality of life.
icSPORTS 2015 - International Congress on Sport Sciences Research and Technology Support
154
REFERENCES
Aghamollaei, T., Eftekhar, H., Shojaeizadeh, D.,
Mohammad, K., Nakhjavani, M., Ghofrani Pour, F.,
2003. Behaviour, Metabolic Control and Health-
related Quality of Life in Diabetic Patients at Bandar
Abbas Diabetic Clinic. Iranian J Publ Health, 32(3):
54-59.
Bani-Issa, W., 2011. Evaluation of the health-related
quality of life of Emirati people with diabetes:
integration of sociodemographic and disease-related
variables. EMHJ,17(11):825-830.
Bosic-Zivanovic, D., Medic-Stojanoska, M., Kovacev-
Zavisic, B., 2012. The quality of life in patients with
diabetes mellitus type 2. Vojnosanit Pregl.,
69(10):858–863.
Eljedi, A., Mikolajczyk, R.T., Kraemer, A., Laaser, U.,
2006. Health-related quality of life in diabetic patients
and controls without diabetes in refugee camps in the
Gaza strip: a cross-sectional study. BMC Public
Health, 6:268.
Glasgow, R.E., Ruggiero, L., Eakin, E.G., Dryfoos, J.,
Chobanian, L., 1997. Quality of Life and Associated
Characteristics in a Large National Sample of Adults
with Diabetes. Diabetes Care, 20(4): 562-567.
Graveling, A.J., Frier, B.M., 2010. Risks of marathon
running and hypoglycaemia in Type 1 diabetes. Diabet
Med, 27:585–8.
Guelfi, K.J., Jones, T.W., Fournier, P.A., 2005. The
decline in blood glucose levels is less with intermittent
high-intensity compared with moderate exercise in
individuals with type 1 diabetes. Diabetes Care,
28:1289–94.
Hill-Briggs, F., Gary, T.L., Hill, M.N., Bone, L.R.,
Brancati, F.L., 2002. Health-related quality of life in
urban African Americans with type 2 diabetes. J Gen
Intern Med., 17(6): 412-9
Jacobson, A.M., de Groot, M., Samson, J.A., 1994. The
Evaluation of Two Measures of Quality of Life in
Patients With Type I and Type II Diabetes. Diabetes
Care, 17(4): 267-274.
Kalda, R., Rätsep, A., Lember, M., 2008. Predictors of
quality of life of patients with type 2 diabetes. Patient
Preferences and Adherence, 2: 21–26.
Kolawole, B.A., Mosaku, S.K., Ikem, R.T., 2009. A
Comparison of two measures of quality of life of
Nigerian clinic patients with type 2 Diabetes Mellitus.
African Health Sciences, 9(3): 161-166.
Lumb, A., 2014. Diabetes and exercise. Clinical
Medicine, Journal of the Royal College of Physicians
of London, 14 (6): 673-676.
McMahon, S.K., Ferreira, L.D., Ratnam, N., et al., 2007.
Glucose requirements to maintain euglycemia after
moderate-intensity afternoon exercise in adolescents
with type 1 diabetes are increased in a biphasic
manner. J Clin Endocrinol Metab, 92:963–8.
Nørholm, V., Bech, P., 2001. The WHO Quality of Life
(WHOQOL) Questionnaire: Danish validation study.
Nord J Psychiatry, 55:229 –235.
Papadopoulos, A.A., Kontodimopoulos, N., Frydas, A.,
Ikonomakis, E., Niakas, D., 2007. Predictors of health-
related quality of life in type II diabetic patients in
Greece. BMC Public Health, 7:186.
Redekop, W.K., Koopmanschap, M.A., Stolk, R.P.,
Rutten, G.E.H., Wolffenbuttel, B.H.R., Niessen, L.W.,
2002. Health-Related Quality of Life and Treatment
Satisfaction in Dutch Patients With Type 2 Diabetes.
Diabetes Care, 25(3): 458-463.
Saatcioğlu, O., Çam Çelikel, F., Kutlutürk, F., Cumurcu
Elbozan, B., Kisacik, B., Yildiz, S., et al., 2008.
Disability and quality of life in patients with type 2
diabetes mellitus. Anatol J Clin Investig, 2(3): 106-
112.
Sakamaki, H., Ikeda, S., Ikegami, N., Uchigata, Y.,
Iwamoto, Y., Origasa, H., et al., 2006. Measurement
of HRQL Using EQ-5D in Patients with Type 2
Diabetes Mellitus in Japan. Value in Health, 9(1): 47-
53.
Sigal, R.J., Kenny, G.P., Wasserman, D.H., Castaneda-
Sceppa, C., 2004. Physical activity/exercise and type
2 diabetes. Diabetes Care, 27:2518–2539.
Waxman, A., 2004. WHO's global strategy on diet,
physical activity and health: response to a worldwide
epidemic of non-communicable diseases.
Scandinavian Journal of Nutrition, 48(2):58-60.
World Health Organization, 2002. Move for health.
Geneva.
World Health Organization, 2012. Chronic disease.
Copenhagen.
World Health Organization, 2008. The global burden of
disease: 2004 update. Geneva.
World Health Organization, 1998. WHOQOL User
Manual. Geneva.
The Impact of Diabetes Mellitus on the Physical Health and Physical Activity
155
