
Physiological-based Dynamic Difficulty Adaptation in a Theragame
for Children with Cerebral Palsy
Adrien Verhulst
1
, Takehiko Yamaguchi
2
and Paul Richard
1
1
LARIS Laboratory, University of Angers, Angers, France
2
Harada Laboratory, Tokyo University of Science, Tokyo, Japan
Keywords: Dynamic Difficulty Adaptation, Physiological Signal, Emotion Recognition, Theragame, Cerebral Palsy.
Abstract: The purpose of this research is to provide a physiological-based Dynamic Difficulty Adaptation (DDA) for
rehabilitation of children with Cerebral Palsy (CP). In this paper, we present all the steps of the DDA devel-
opment by going through (1) the acquisition of physiological signals, (2) the extraction of the physiological
signals’ features, (3) the training of a learning classifier of physiological signals' features, and (4) the im-
plementation of the DDA in a game-based rehabilitation system. As a result, we successfully implement a
physiological-based DDA based on the user affective state (anxiety and boredom).
1 INTRODUCTION
Research and development in game-based stroke
rehabilitation (theragame) spreads increasingly. The
main advantages of the gaming approach are: (1) a
more effective rehabilitation through an increase of
the motivation (Hocine and Gouaich, 2011), (2) an
access to quantified data, (3) the possibility to repeat
and to adapt the exercises, and (4) the possibility to
scale the rehabilitation (McCue et al., 2010).
Children are most likely to lose motivation in
front of a repetitive exercise than adults (Liebert et
al., 2006). Since the repetition is necessary in the
rehabilitation process, it is important to keep them
motivated. A way to do it is by keeping them in the
flow state (Huang et al., 2010).
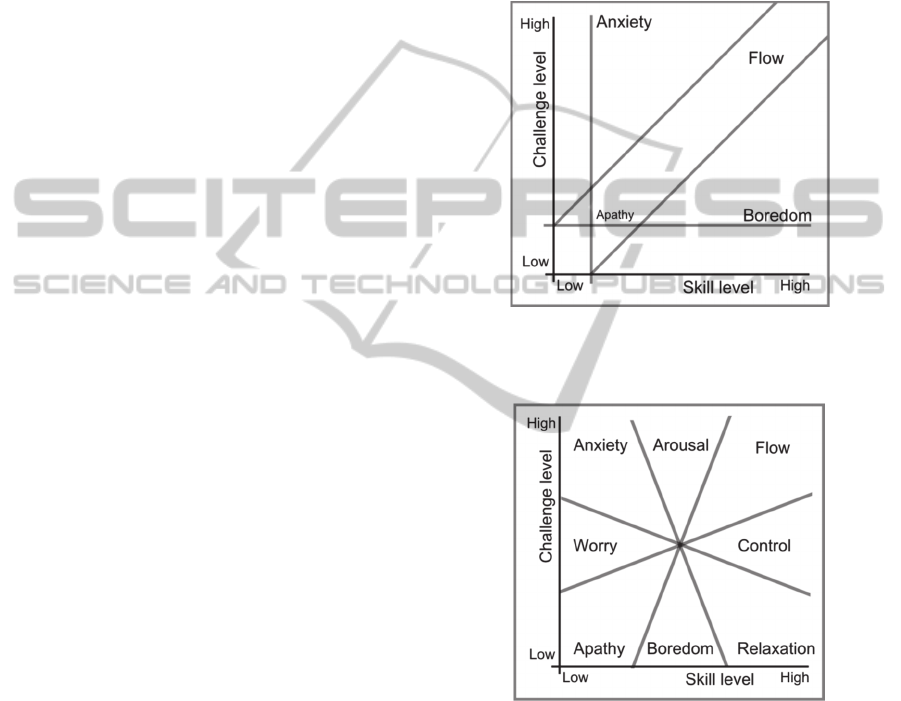
The flow (refer Figs. 1 and 2) is “a state in which
people are so involved in their activity that nothing
else seems to matter; the experience itself is so
enjoyable that people will do it even at great cost,
for the sheer sake of doing it” (Csikszentmihalyi,
1990).
The flow has been used in several researches to
measure the enjoyment of a user in interactive
applications. The idea behind the flow theory can be
summarized as follows: (1) the user is more
susceptible to be in the flow state when the
challenge equals the skill, (2) if the challenge is less
important than the skill, the user is bored (too easy
for him/her), and (3) if the challenge is more
important than the skill, the user is frustrated (too
hard for him/her).
There are several reasons of why a simple
selection of the level of difficulty (easy-medium-
hard), at the beginning of the application, may not be
sufficient: (1) there is a limited difficulty variation,
(2) there is a difficulty gap between levels, (3) it is
not enough responsive to player learning, (4) it is
time-consuming to implement those variations and
(5), the user has to «guess» his/her level regarding
the levels of difficulty. The DDA’s main advantage
over non-dynamic difficulty adaptation is the
possibility to automatically adapt itself from the user
actual performance.
In this context, we are developing the Children
Rehabilitation Project (CRP) which is based on a
new modular adaptive system dedicated to
rehabilitation of children having CP. The system has
been designed as a framework permitting to easily
implement rehabilitation applications. The first
theragame developed in the context of the CRP is
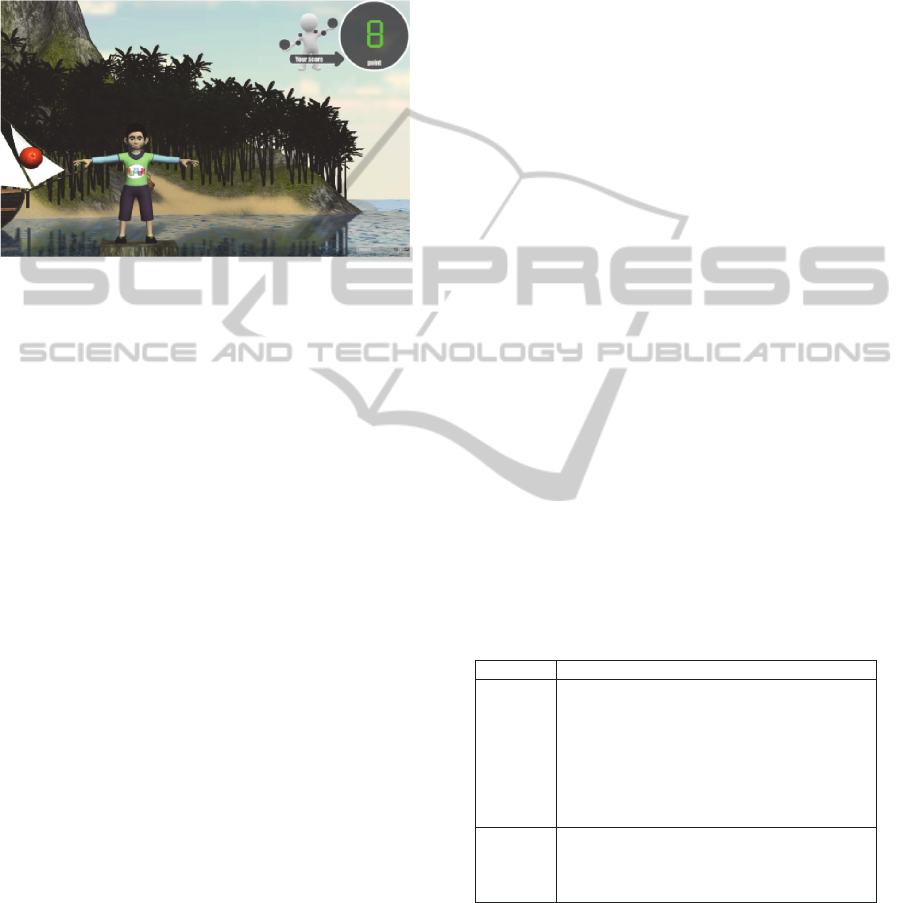
the Rehab-Island theragame (Fig. 3). In this
application, the user controls the avatar through a
Kinect
TM
, and must touch objects by moving his/her
left arm. The application parameters (such as
objects’ velocity, size, etc.) are decided by the
therapist. In the next section, we survey the state of
the art concerning Dynamic Difficulty Adaptation
(DDA). In section 3, we present the proposed
approach. Section 4 is dedicated to the software
implementation of our system. In section 5 we
164
Verhulst A., Yamaguchi T. and Richard P..
Physiological-based Dynamic Difficulty Adaptation in a Theragame for Children with Cerebral Palsy.
DOI: 10.5220/0005271501640171
In Proceedings of the 2nd International Conference on Physiological Computing Systems (PhyCS-2015), pages 164-171
ISBN: 978-989-758-085-7
Copyright
c
2015 SCITEPRESS (Science and Technology Publications, Lda.)
describe the feature extraction protocol. Section 6
presents the training of the classifier. Section 7
presents the implementation of the DDA. Section 8
provides a short discussion of our method. The paper
ends by a conclusion and gives some tracks for
future works.
2 STATE OF THE ART
Cerebral Palsy (CP) refers to various motor impair-
ments caused by damage to the motor control center
of the developing brain, and can occurs during preg-
nancy, during childbirth, or after birth up to about
age three (Aisen et al., 2011). Children having im-
paired motor movements after CP need physical
therapy, which can be enhance by rehabilitation
applications (Parsons et al., 2009).
There are only a few papers presenting a
Dynamic Difficulty Adaptation (DDA) for stroke or
CP rehabilitation systems. Moreover, in all those
papers, DDA is only based on user’s performance
(mainly score). For example, Parnandi et al., (2013)
proposed an approach based on control theory’s
principles. They used variation of actual and desired
arousal of the user as the variation error to minimize.
Huang et al., (2010), following the work of Hao
et al., (2010); and Li et al., (2010), presented Real
Time Computational Intelligence (RTCI) and
Adaptive ANN Computational Intelligence
(ANNCI) approaches for NPC, both being based on
Monte-Carlo Tree Search (MCTS).
Wong (2008) also presented an ANNCI
approach, but not based on MCTS. Hocine and
Gouaich (2011) described an approach based on
prior assessments of the capability of the user. The
adaptation is done through an ability zone, which
contains information on the difficulty to do a given
task at given position. They conducted an
experiment on 8 subjects through a reaching-task
application.
Gouaïch et al., (2012), following the work of
Hocine, proposed a digital pheromone approach
based on the ant algorithm introduced by Dorigo and
Stützle (2004). The adaptation is done through an
ability zone updated regarding user’s performance.
They conducted an experiment on 10 subjects
through a reaching-task application.
Arulraj (2010) proposed a differential learning
approach for NPC. The agent learning-rate reduces
with time, while being impacted by user’s
performance. The approach feasibility has been
tested using the Minigate game. Andrade and
Ramalho (2005) and Tan et al., (2011) both proposed
a Reinforcement Learning (RL) approach for NPC.
G. Andrade implemented it by using the Q-learning
algorithm, the adaptation being done by choosing
the action-value which fit the level of the user. C.
Tan implemented it by using Adaptive Uni-
Chromosome Controller (AUC) and Adaptive Duo-
Chromosome Controller (ADC) algorithms, the
adaptation being done by activating controller’s
behaviour which fit the level of the user.
Figure 1: Out-dated version of the flow theory. Researches
on affect-based DDA mainly use it, since it is easier to
apply than the updated version of the flow theory.
Figure 2: Updated version of the flow theory. apathy,
anxiety and boredom are still used.
Regarding physiological based DDA, the DDA is
usually handled through the flow theory, where the
emotional states captured orient the DDA to move
the challenge to emotional state.
Liu (2009), showed that a player's affective state
can be deciphered from his physiological state
during gaming, and that a DDA can be based on the
affective state. They conducted an experiment on 9
subjects, and investigate several classification
algorithms to test the affective models (Regression
Tree, K Nearest Neighbours, Bayesian Network
Physiological-basedDynamicDifficultyAdaptationinaTheragameforChildrenwithCerebralPalsy
165
Technique, and Support Vector Machines (SVM)).
They showed that the majority of the participants
improved during the affect-based DDA session, and
that they perceived the game more challenging with
an affect-based DDA than a performance based
DDA.
Figure 3: Illustration of the Rehab-Island application. The
avatar's arms follow the user's arms through the Kinect
TM
.
Chanel and Rebetez (2011) developed a DDA to
maintain player in flow through an affective model
based on EEG signals. They showed that the
affective state was changing when playing Tetris.
They then trained a classifier to recognize the
affective state in order to adapt Tetris.
Guillaume et al., (2012) proposed a method to
implement an affect-DDA in games. They recorded
the player's physiological signals and then extracted
the signals' features when the player was (1) playing
the game and was (2) in a given affective state (such
as boredom). They then trained a learning classifier
to recognize the affective state from the
physiological features. Finally, they used the
learning classifier to know the affective state of the
player (boredom or not) and use that information to
adapt the game in real-time.
Parnandi and Ahmed (2014) presented Chill-Out,
an adaptive biofeedback game monitoring the
breathing rate of the player and adapting the game in
a way that encourages relaxing behaviours. They
showed that such an adaptation led to improved
performances.
3 APPROACH
We decided to use a simple approach to do our
DDA. Based on the user's physiological state a
learning classifier identifies the user's affective state.
This affective state is then passed to our DDA algo-
rithm (refer Figs. 4 and 5) which adapts accordingly
the level of difficulty of the theragame. This ap-
proach allows us to use the flow theory, which de-
pends of the user's affective state.
The flow theory uses several affective states. The
out-dated flow theory use anxiety, boredom and
flow, while the updated flow theory uses apathy,
worry, anxiety, boredom, arousal, relaxation, control
and flow. In our work, we decided to use only
anxiety and boredom, since (1) they are very
relevant to the flow theory (already present in the
out-dated version), (2) they have already been used
in physiological-based DDA (Liu et al., 2009),
(Giakoumis et al., ).
In previous works anxiety and boredom have
been already classified using (1) ICG, BVP, EMG,
ECG, EDA (or GSR) and heart sound features (Liu
et al., 2009); (2) ECG and EDA (or GSR) features
for boredom (Giakoumis et al., 2011).
Since anxiety is closely related to the stress
affective state, which can be detected from ECG and
EDA features, we decided to only use ECG and
EDA. It allow us (1) to have less constraint in our
material choice (since it is then supposed to be used
with children having CP in rehabilitation, we had to
limit the captors), (2) to use the same signals for
both the anxiety and boredom.
In summary, from the choice of detecting anxiety
and boredom, we decided to use ECG and EDA
signals. We decided to use BITalino
TM
in order to
record them. Concerning the features choice and
extraction, we based our work on the previous work
done by Lieu C. et al and Giakoumis D. et al. We
selected 14 different features, based on ECG and
EDA signals (see table 1).
Table 1: Features extracted from EDA and ECG.
Signals Features
EDA
EDA Mean;
EDA SD;
EDA 1 derivation average;
EDA 1 derivation RMS;
EDA SCR;
EDA 1 difference raw data;
EDA 1 difference normalized data;
EDA 2 difference normalized data.
ECG
IBI RMSSD;
IBI Pnn50;
IBI 1 difference raw data;
IBI 1 difference normalized data.
We then used those features to train a SVM.
While others learning classifier (such as Regression
Tree) may give better results, we felt more confident
about the SVM, which usually gives good result in
emotion classification (Yoo et al., 2007).
We decided to train 2 SVM, one trained to
recognized anxiety, and the other one to recognized
PhyCS2015-2ndInternationalConferenceonPhysiologicalComputingSystems
166
boredom. Since, to the best of our knowledge, no
method exists to recognize flow, we thought that
detecting the absence of anxiety or the absence of
boredom would indicate that the user was in flow.
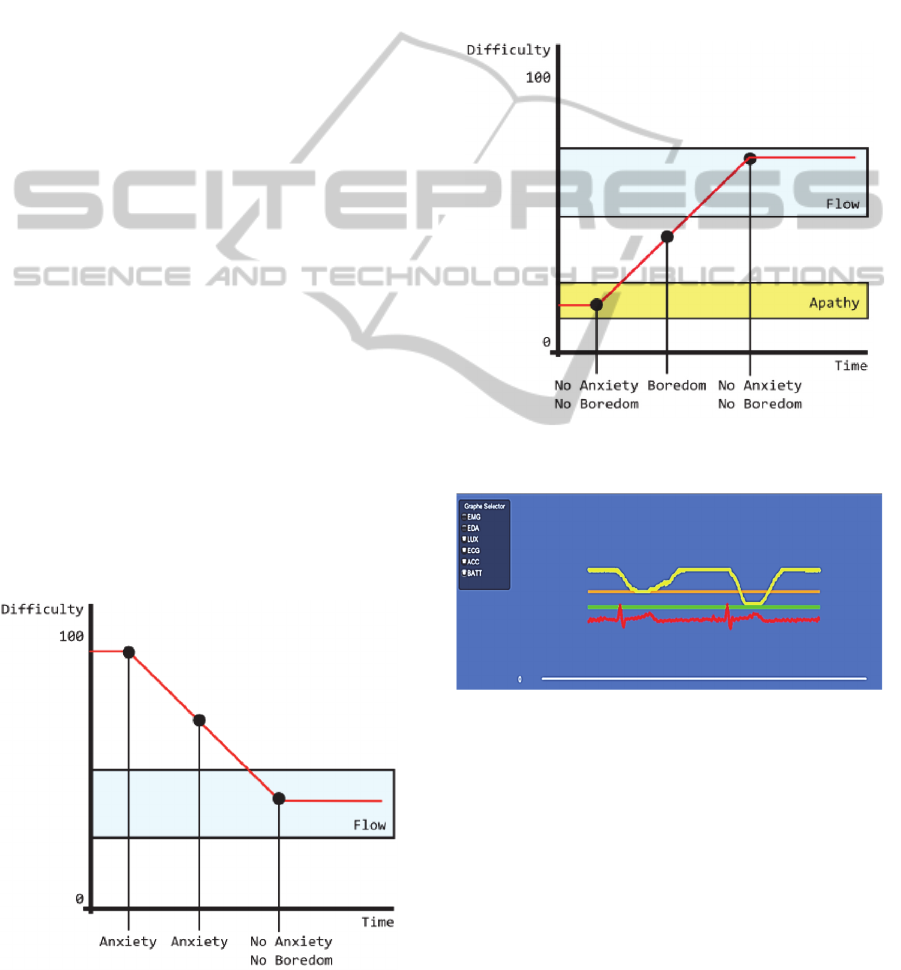
We decided that if there was no anxiety and
boredom detected, and that if the level of difficulty
was above or equal to 10%, the user was in flow. If
there was no anxiety and no boredom detected, and
that if the level of difficulty was below 10%, the
user was in apathy. If the user was in flow, then the
difficulty will not change. If the user was in apathy,
then the difficulty will increase (to stimulate the
user). If there was anxiety and no boredom, then the
difficulty will decrease. If there was no anxiety and
boredom, then the difficulty will increase. If there
was anxiety and boredom, then the difficulty will not
change, since it may be an error in the signals
reading. The figures 4 and 5 summarize the idea.
The DDA algorithm can be explained in those
few lines: the application change the difficulty until
anxiety/boredom is not detected and the difficulty is
above a given threshold.
4 IMPLEMENTATION
We used the BITalino Board Kit
TM
, a low cost de-
vice able to record EMG, ECG, EDA (Guerreiro and
Martins, 2013) in order to record ECG and EDA.
While fairly new, it is already world-wide used.We
decided to use it since it was: (1) Cheap, others ma-
terials commonly used in research (such as Pro-
comp5) are above the thousands of €; (2) Described
in the literature; (3) Delivered with a SDK and (4)
Wearable.
Figure 4: When anxiety is detected, the level of difficulty
decreases over time, until it reaches another affective state.
We developed a BITalino C# SDK (.NET 2.0)
based on the BITalino Java SDK in order to
implement BITalino in Unity3D (v4.5x).
By doing so, we successfully implemented
BITalino in Unity3D (see Fig. 6). It allowed us to
record in real-time ECG and EDA signals.
We also developed several Unity scripts to allow
us to set the BITalinoTM parameters from the
application (such as the frequency). The BITalino C#
SDK as well as our Unity's scripts is available online
in the API section of the BITalino official website
.
Figure 5: If the level of difficulty is to low (< 10%), we
consider that the user is in the apathy state.
Figure 6: BITalino
TM
working inside Unity3D. We can see
in red the ECG signal. In the left panel, we can select
which signals to display.
5 FEATURES EXTRACTION
BITalino
TM
did not provide software to extract phys-
iological features. Therefore we had to implement a
feature extraction system ourselves. While the calcu-
lations were fairly easy to do, we decided to do it
using a MATLAB C-shared DLL, to be able to use
some built-in MATLAB functions. We did it in order
to be able to easily change and adapt the algorithms.
Physiological-basedDynamicDifficultyAdaptationinaTheragameforChildrenwithCerebralPalsy
167
It could however also have been done directly in C#
through mathematical libraries. We developed sever-
al MATLAB scripts able to extract the features we
were interested in (see table 1). We then exported the
scripts through a C-shared DLL, to be able to call
them from Unity3D.
Concerning the features extraction calculation,
we followed the work previously done by
Giakoumis, D. et al. The scripts were able, from the
ECG and EDA raw data, to automatically extract the
features of the table 1. The raw data were sampled
(at 255 Hz, from the 1000 Hz raw data), then
normalized and smoothed with a local regression
filter.
The ECG signal was measured using three
electrodes placed in lead II (negative electrode on
the right arm, positive electrode on the left leg). This
placement allowed the subjects' arms to move freely.
The EDA signal was measured using two electrodes
in bipolar placement on the left (or right) hand
(index and middle finger). Even if it was as less
restrictive as possible, this placement requires the
subjects' left (or right) arm to not move. By doing
so, we successfully managed to extract the features
within Unity3D, from the signals recorded by
BITalino, in real-time.
6 CLASSIFIER TRAINING
We integrated LibSVM (Chang and Lin, 2013) in
Unity3D; through one of its open-source implemen-
tation available in C# (We slightly modified it to be
able to use it in .NET 2.0). To train the SVM, we
developed an application (ProvokeAffect) able to put
the user in boredom affective state and anxiety affec-
tive state.
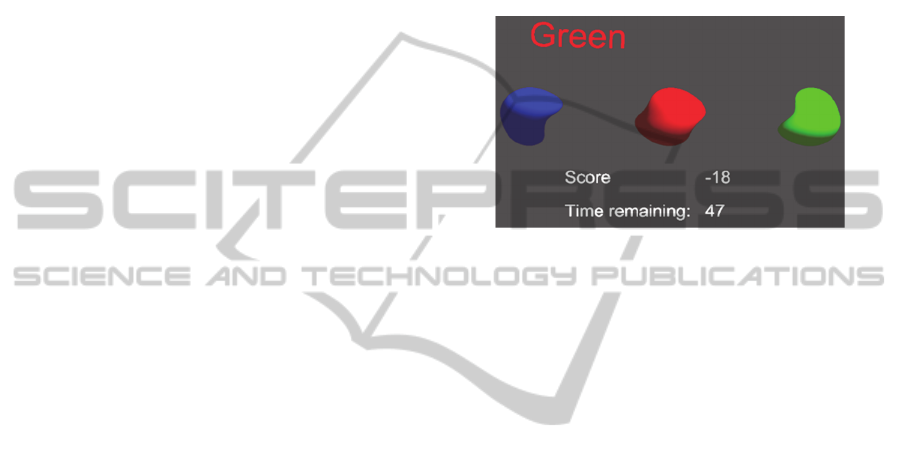
We developed three scenes in ProvokeAffect: (1)
boredom scene, (2) anxiety scene, (3) excitement
scene. Each of those scenes follows the same rules:
A message displays the name of a colour (Red; Blue;
Green). The subject have to click (one time) on the
sphere having the named colour. After few seconds
(or milliseconds) the colour’s name changes. If the
subject clicks on the sphere before the time limit, he
gains 1 point. If he does not click on the sphere
before the time limit, or if he misses, he loses 1
point. The differences between each scene depend of
the: (1) overall difficulty, (2) environment (sounds,
background). To provoke boredom, the interval of
time between each message change is set to 4
seconds, without difference between (1) colour’s
spheres, (2) colour’s message. Moreover, the
sphere’s number is 2.
To provoke anxiety, the interval of time between
each message changes is set to 0.85 seconds, with a
difference between (1) colour’s spheres, (2) colour’s
message. Moreover, the sphere’s number is 3. In top
of that, the anxiety scene has a score-DDA to
increase difficulty if the user is doing too well. The
DDA (1) changes the interval of time between each
message (minimum: 0.5s; maximum: 0.85s), (2)
changes the shape of the sphere, (3) changes the
background colour, (4) produces heart-beat sound.
Figure 7: Anxiety scene. We can see that the message is
coloured in a different way from what is intuitively sup-
posed to be (red instead of green).
To provoke excitement, the interval of time
between each message changes is set to 1.5 seconds,
with a difference between (1) colour’s spheres, (2)
colour’s message. Moreover, the sphere’s number is
3. In top of that, the excitement scene has a score-
DDA to increase difficulty if the user is doing too
well. The DDA changes the interval of time between
each message (minimum: 0.75s; maximum: 1.5s).
Finally, it is possible to do several series of combo.
Successful combo produces (1) score increase, (2)
sounds effects. Note that we did not use the
excitement scene to train a SVM dedicated to
excitement (the preliminary results did not show a
great difference between anxiety and excitement, so
we preferred to not use it), unlike the anxiety and
boredom scene.
Having the ProvokeAffect application, we did a
preliminary test to see if there were noticeable
differences between anxiety and boredom scene
when looking at the physiological signals.
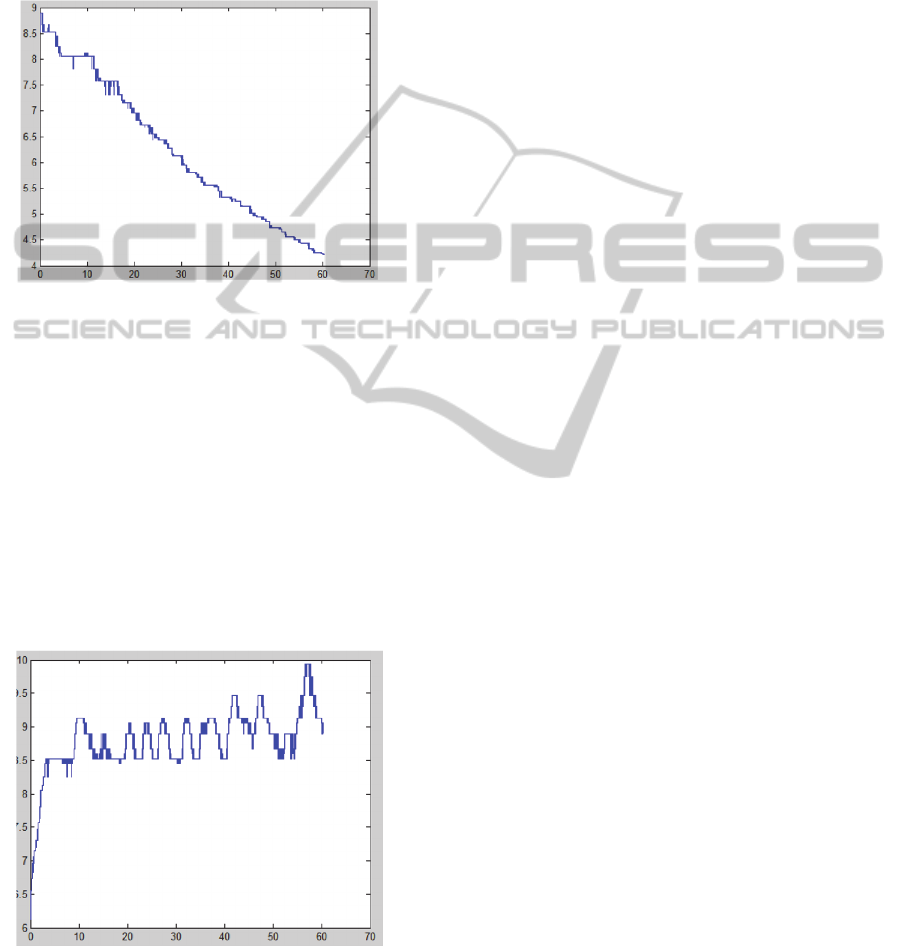
We can see that, even without looking at the
features, there are important differences between
“EDA boredom” and “EDA anxiety” signals (see
Figs 8 and 9). Concerning the experimentation
relative to the training of the learning classifier, we
used all three scenes of ProvokeAffect. All the
experimentation (including the Likert-scale test) was
automatized, in order to not induce change(s) in the
affective state of the user. The experiment was 15
minutes long. After an explanation of the rules
PhyCS2015-2ndInternationalConferenceonPhysiologicalComputingSystems
168
(automated), the user had to pass 3 trials of the
boredom scene, then 3 trials of the anxiety scene,
then 3 trials of the excitement scene. The change
between the scenes was automated. Between each
trials, there was a one minute during which the
subject had to fill a 5 Likert-scale self-report (still
automated).
Figure 8: EDA when doing the Boredom scene of Pro-
vokeAffect.
The Likert-scale comported several non-relevant
questions to our experiment in order to not orient the
subject in his answers. As relevant questions, we
asked if he was bored (1-5) or if he was anxious (1-
5). After the experiment, we labelled the results as
anxiety / boredom if the user answered 4 or 5 and
not anxiety / boredom if it was 1 or 2. If it was 3,
then we did not include the result. Finally, we had 10
subjects who did the experiment (and therefore a
total 90 trials). From those labelled features, we
trained the two learning classifier (one for anxiety
recognition and one for boredom recognition).
Figure 9: EDA when doing the Anxiety scene. We can
clearly see that there are a lot more of SCR than with the
Boredom scene of ProvokeAffect.
By training our SVMs (after grid-search) we
obtained a cross-validation result up to 75% for both
anxiety and boredom SVM. While this result is
below other studies (probably because there was not
enough trials), it was enough to continue our work
on our affect-DDA.
7 IMPLEMENTATION OF THE
DDA
Since the DDA is supposed to be used by different
theragames, it was important to decouple it from the
theragames into a DDA module. The DDA module
comports the reading of physiological signals, the
features extraction, the SVM classifiers and the
implementation of the DDA algorithm. The DDA
module gives to the theragames a difficulty level
between 0-100, which may change over time (unless
the user is in flow). 0% correspond to the easiest
difficulty while 100% correspond to the hardest
difficulty.
It is then up to the developer of each theragame,
according to a value of difficulty in percentage
(which may change over time) to implement the
“meaning” of such difficulty. For example, in our
Rehab-Island theragame, we observed that the
difficulty was mainly dependant of 4 main different
variables. We gave to each of those variables a
minimum and maximum value, which follow a
linear, exponential or logarithmic curve. By doing
so, when the difficulty is updated, each of our
difficulty variables is automatically updated.
However, this is a pretty straightforward example.
There are others ways to implement the difficulty,
which depend mainly of the kind of game
developed.
8 DISCUSSION
By decoupling our DDA from our theragame, we
successfully managed to implement it in the CRP. In
summary, we implemented a physiological-based
DDA, which, through the affective-state (boredom
and anxiety states) of the user, adapts the difficulty.
At the best of our knowledge, there is non-yet a
physiological-based DDA using boredom and anxie-
ty state together. There is non-yet either a physiolog-
ical-based DDA in a theragame.
Even if our work present a working solution to a
physiological-based DDA implementation in an
adaptive interface, its purpose was to be the base of
researches in rehabilitation using DDA. We would
Physiological-basedDynamicDifficultyAdaptationinaTheragameforChildrenwithCerebralPalsy
169

like to see if a physiological-based DDA is more
effective than score-based DDA in CP's
rehabilitation, and in what ways it is more effective.
We would also like to try others devices than
BITalino (such as the Kinect 2, able to track the
blood flow of the user). Eventually, we would also
like to improve the existing system, by training a
more accurate classifier (Liu et al., suggested to use
a Regression Tree classifier).
9 CONCLUSION AND FUTURE
WORK
We successfully managed to implement a philologi-
cal-based DDA in an adaptive interface (the CRP).
This DDA uses the EDA and ECG signals of the
user. From those signals, it extract its important
features (such as GSR and HR), in order to accurate-
ly classify user's affective state. Using 2 trained
SVM (one for boredom affect state, one for anxiety
affect state), the DDA is able to know if the user is
bored, anxious or likely to be in the flow affect state,
and therefore to increase, decrease, or not change the
difficulty. By providing such a DDA, we would like
to propose a more effective DDA in order (1) to
improve rehabilitation, (2), to allow the patient to be
less dependent of the patrician.
In our future study, we will see if the
physiological-based DDA presented in this work is
more effective than a straightforward score-based
DDA in CP's rehabilitation. To do so, it will be
necessary to retrain the SVMs, since the SVMs data
in our experiment came from adults, and CP
rehabilitation is for children. During the training, it
will be also necessary to propose a “boring”
application and an “anxious” application which ask
the user to perform a physical effort on his upper-
body. Luckily enough, Rehab-Island seem adapted
to propose such applications.
REFERENCES
Aisen, M. L. et al., 2011. Cerebral palsy : clinical care and
neurological rehabilitation. The Lancet Neurology,
10(9), pp.844–852.
Andrade, G., Ramalho, G., and Coruble, V., 2005. Chal-
lenge-sensitive action selection: an application to
game balancing, International Conference on Intelli-
gent Agent Technology, pp. 194-200.
Arulraj, J. J. P., 2010. Adaptive agent generation using
machine learning for dynamic difficulty adjustment.
International Conference on Computer and Communi
cation Technology (ICCCT), pp. 746 - 751.
Chanel, G. & Rebetez, C., 2011. Emotion assessment from
physiological signals for adaptation of game difficulty.
Systems, Man and Cybernetics, 41(6), pp.1052–1063.
Chang, C. & Lin, C., 2011. LIBSVM : A Library for Sup-
port Vector Machines. ACM Trans. Intelligent Systems
and Technology, (2), pp. 1-27.
Csikszentmihalyi, M., 1990. Flow : The Psychology of
Optimal Experience, Harper and Row, New York.
Dorigo, M. & Stützle, T., 2004. Ant Colony Optimization,
Giakoumis, D. et al., 2011. Automatic Recognition of
Boredom in Video Games Using Novel Biosignals
Moment-Based Features. IEEE Transactions on Affec-
tive Computing, 2(3), pp.119–133.
Gouaïch, A. et al., 2012. Digital-pheromone based diffi-
culty adaptation in post-stroke therapeutic games. Pro-
ceedings of the 2
nd
ACM SIGHIT symposium on In-
ternational health informatics – IHI’12, p.5.
Guerreiro, J., Martins, R., Silva, H., Lourenço, A., and
Fred A., 2013, “BITalino: A Multimodal Platform for
Physiological Computing” International Conference
on Informatics in Control, Automation and Robotics
(ICINCO) (1), pp.500-506.
Guillaume, C., Konstantina, K. & Thierry, P., 2012. Ga-
mEMO: how physiological signals show your emo-
tions and enhance your game experience. Proceedings
of the 14
th
ACM, pp. 1–3.
Hao, Y. H. Y. et al., 2010. Dynamic Difficulty Adjustment
of Game AI by MCTS for the game Pac-Man. Sixth
International Conference on Natural Computation
(ICNC), 8, pp. 3918-3922.
Hocine, N. & Gouaich, A., 2011. Motivation based diffi-
culty adaptation for therapeutic games. Serious
Games.
Huang, W. et al., 2010. Dynamic difficulty adjustment
realization based on adaptive neuro-controlled game
opponent. Intelligence (IWACI), 2010.
Li, X. et al., 2010. To create DDA by the approach of
ANN from UCT-created data. International Confer-
ence on Computer Application and System Modeling
(ICCASM), pp.475–478.
Liebert, M. A. et al., 2006. Feasibility, Motivation, and
Selective Motor Control : Virtual Reality Compared to
Conventional Home Exercise in Children with Cere-
bral Palsy., 9(2), pp.123–129.
Liu, C. et al., 2009. Dynamic Difficulty Adjustment in
Computer Games Through Real-Time Anxiety-Based
Affective Feedback. International Journal of Human-
Computer Interaction, 25(6), pp. 506–529.
McCue, M., Fairman, A. & Pramuka, M., 2010. Enhancing
quality of life through telerehabilitation. Physical med-
icine and rehabilitation clinics of North America,
21(1), pp.195–205.
Parnandi, A. & Ahmed, B., 2014. Chill-Out: Relaxation
Training through Respiratory Biofeedback in a Mobile
Casual Game. Mobile Computing, pp.252–260.
Parnandi, A., Son, Y. and Gutierrez-Osuna, R., 2013. A
Control-Theoretic Approach to Adaptive Physiological
Games. Humaine Association Conference on Affective
Computing and Intelligent Interaction, pp.7–12.
PhyCS2015-2ndInternationalConferenceonPhysiologicalComputingSystems
170

Parsons, T. D. et al., 2009. Virtual reality in paediatric
rehabilitation : A review. , 12(August), pp.224–238.
Tan, C., Tan, K. & Tay, A., 2011. Dynamic game difficulty
scaling using adaptive behavior-based AI. IEEE
Transactions on AI in Games, 3(4), pp.289–301.
Wong, K., 2008. Adaptive computer game system using
artificial neural networks. Neural Information Pro-
cessing, pp.675–682.
Yoo, S., Lee, C. & Park, Y., 2007. Determination of Bio-
logical Signal for Emotion Identification. World Con-
gress on Medical Physics, 14, pp.4047–4049.
Physiological-basedDynamicDifficultyAdaptationinaTheragameforChildrenwithCerebralPalsy
171
