
Modulation of Existent Obstetrics EHRs to the openEHR Specification
Jo
˜
ao Carlos Menezes de Magalh
˜
aes
1
and Ricardo Jo
˜
ao Cruz Correia
2,3
1
Mestrado Integrado em Medicina, Faculdade de Medicina da Universidade do Porto, Porto, Portugal
2
CINTESIS, Faculdade de Medicina da Universidade do Porto, Porto, Portugal
3
Department of Health Information and Decision Sciences, Faculdade de Medicina da Universidade do Porto,
Keywords:
Interoperability, Semantic Interoperability, openEHR, e-Health.
Abstract:
Objective: Create templates in OpenEHR through the modulation of existing electronic health records defined
in OpenObsCare platform. Materials and Methods: Apply a 4 step process: select data fields already existent
in OpenObscare; search both in openEHR and NEHTA clinical knowledge manager (CKM) for the archetypes
that contain these data fields; create new archetypes when a data field doesn’t have an existent one in both
CKM’s; develop templates from all the information gathered in the previous steps. Results: Development of 6
templates available online via http://joaomagalhaes.me/admission templates and 1 archetype (openEHR-EHR-
CLUSTER.exam-vagina.v1). Discussion: The process of modulation from existent EHR to the openEHR was
possible since the standardization of clinical concepts allowed the re-utilization of a lot of already existent
archetypes. This speeds up the development process by defining earlier the domain knowledge necessary
for the HIS. Some hurdles faced in the process were due to the necessity of translation of all the archetypes
to use at a national level and also due to the lack of national wide accepted terminologies. As this process is
eased by the robustness of existent archetypes, the creation of default obstetric templates validated by a special
commission, would probably be advantageous since the interoperability and semantics standardization would
allow effective transmission of information between all the health care agents. Conclusion: The modulation
of admission data existent in the HIS OpenObsCare to openEHR was easier than the ”traditional” way of doing
it which is by specifying requirements. This is due to the fact that a lot of the existent archetypes are already
robust enough and the number of them is enough to represent several clinical concepts contained in the created
templates.
1 INTRODUCTION
The widespread use of electronic health records de-
mands the need of a electronic health record (EHR)
that can resist during a patient entire lifetime. The
quality of the EHR can enhance the health care qual-
ity(Delpierre et al., 2004) and can also facilitate
the research for academic purposes contributing for
a more evidence based medical practice(Zeng and
Cimino, 1999). There is a consensus about the need of
a system that is designed to allow maintainability and
interoperability of this records(Hovenga, 2010)(Beale
and Heard, 2007)(Xiao et al., 2011). The interoper-
ability is the ability of different software systems to
interpret clinical information in the same way. For
this to be achieved the advantages of standardized
clinical concepts and reference models comes as a
need (Hovenga, 2010). This is the goal that OpenEHR
foundation and others such as HL7(Dolin et al., 2001)
proposed to reach.
The openEHR architecture is a two level mod-
elling approach for EHRs. The first level is the
reference model which is a relatively small set of
classes used to support the medico-legal requirements
and record management functions (Beale and Heard,
2007). The first level stands for functional inter-
operability. It provides the communication between
different HIS (Health Informatic Systems).The sec-
ond level represents the openEHR archetype method-
ology. Archetypes map clinical knowledge, there-
fore each archetype represents one clinical concept
by constraining instances of the openEHR reference
model. This dual approach allows a fundamental ab-
stract concept which is the independence of the devel-
opment of domain knowledge (clinical content) which
is delegated to medical specialists and technical im-
plementation which is a concern for the software de-
velopment team. This has an enormous advantage
since there is no need to transmit clinical require-
ments to non specialized people.
OpenEHR Templates(Leslie, 2008) are created by
the clinicians and are used to create definitions of con-
439
Carlos Menezes de Magalhães J. and João Cruz Correia R..
Modulation of Existent Obstetrics EHRs to the openEHR Specification.
DOI: 10.5220/0005220804390445
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2015), pages 439-445
ISBN: 978-989-758-068-0
Copyright
c
2015 SCITEPRESS (Science and Technology Publications, Lda.)

tent such as a particular document or message, re-
quired for specific use cases, such as specific screen
forms, message types or reports. They contain dif-
ferent archetypes that have meaning all together (e.g.
obstetrics hospitalization entrance note, obstetrics ul-
trasound report) and that can be assigned to the same
template or to different templates several times mak-
ing it re-usable.
In an effort to implement this change of paradigm
in the Obstetrics department at Hospital de S
˜
ao Jo
˜
ao,
Porto, we propose the creation of templates to be
used by an experimental version of the OpenObsCare
health information system (HIS) that is currently be-
ing used in this department. Since there are differ-
ent ways of collecting data for an obstetrics EHR the
analysis and comparison of this data between differ-
ent institutions an countries is hard.
In this work we aim at creating openEHR tem-
plates for a pregnant woman hospitalization admis-
sion in an obstetrics department. We also want to
document the process in order to evaluate its advan-
tages and disadvantages compared to a more tradi-
tional way of creating HIS.
2 MATERIALS AND METHODS
As data source for the templates’ creation we used the
current HIS implemented in the obstetrics department
at Hospital de S
˜
ao Jo
˜
ao - OpenObscare. To create
openEHR templates 4 stages were defined:
1. Select data fields already existent in OpenObscare
2. Search both in openEHR and NEHTA clinical
knowledge manager (CKM) for the archetypes
that contained those data fields
3. Create new archetypes for data that doesn’t have
a corresponding archetype in the openEHR and
National E-Health Transition Authority (NEHTA)
clinical knowledge managers (CKM).
4. Create Templates
This similar process has already been used by oth-
ers (G.M. Bacelar-Silva, 2012).
2.1 Select Data Fields from
OpenObsCare
OpenObsCare (Figure 1) is an opehEHR solution still
in development that derives from the already existent
ObsCare. Obscare is a software that was designed
to be used by OB/GYN doctors, anesthesiologists,
nurses and administrative staff and is used to regis-
ter patient admission and discharge, as well as child-
birth and newborn data. It is also used to register sur-
gical and anesthetic procedures, nursing records, as
well as gynecological interventions. It is currently
in use at Hospital de S.Jo
˜
ao and will soon be in-
stalled in several other hospitals in northern Portugal.
These fields were extracted from the hospitalization
admission section of this HIS which is composed of
several main tabs. We only included the Admission
Note, General information and Ultrasound Exams for
this modulation. The General Information contains
5 more sub-tabs which were each counted as main
tabs. For each of these tabs a google spreadsheet was
created to describe the different forms they contain.
The spreadsheet information was gathered regarding
the following parameters: Data fields, Description,
OpenEHR archetype corresponding field, Archetype
ID and Note.
2.2 Search for Archetypes
OpenEHR maps the clinical statements using specific
types of Entries (Administrative, Observation, Evalu-
ation, Instruction and Action) according to the nature
of the statement. Archetypes were chosen according
to the clinical concept the data field was part of. As
an example, the pattern of uterine contraction data
field present in OpenObsCare could be represented
by the field Pattern of the archetype openEHR-EHR-
Observation.uterine contractions.v1. Preference was
given to the openEHR CKM and only when a clin-
ical concept wasn’t found on it, the NEHTA reposi-
tory was used. This archetypes were found in both the
referred CKM’s by submitting a ”Complete search”,
which searches ”inside” resources, including all meta-
data, and for archetypes, archetype definition, and the
archetype ontologies. The last search was performed
on August 27th.
2.3 Create New Archetypes for Data
that doesn’t have a Corresponding
Archetype in the openEHR and
NEHTA Clinical CKM’s
If after searching on the referred repositories no avail-
able archetype could be found to represent a clinical
statement, the creation of a new archetype would be
considered. For this purpose the Ocean Archetype
Editor, a tool to support the authoring of archetypes
was used.
HEALTHINF2015-InternationalConferenceonHealthInformatics
440
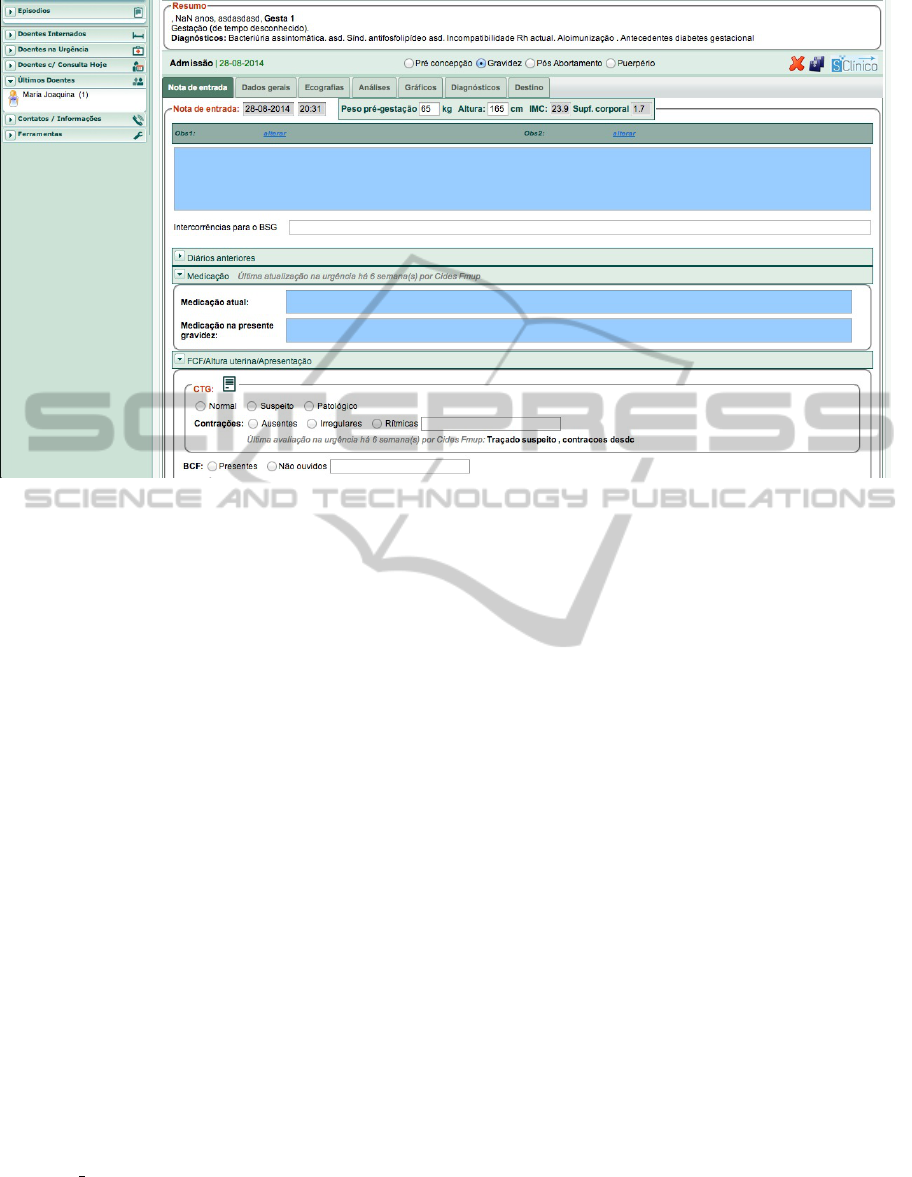
Figure 1: OpenObsCare platform.
2.4 Create Templates
The structured spreadsheets created helped in creat-
ing the framework for the development of the tem-
plate, where the archetypes will be arranged. This
was made using Ocean Template Designer – software
that allows composing a set of archetypes into a tem-
plate.
3 RESULTS
From the modulation of OpenObsCare IHS, spread-
sheets with the specifications necessary for the devel-
opment of templates were created (Fig.3). From this
framework 6 templates were developed:
• Admission Note(Fig.3)
• Ultrasounds
• Current Pregnancy
• Obstetric history
• Family history
• Personal history
They are all available for download in
the following url http://joaomagalhaes.me/
admission templates.
The archetypes used for creating the mentioned
templates are presented in Table 1. Only 1 of the con-
cepts used is taken from the NEHTA repository and
also only 1 was created (Fig. 4). The reason for this
has to do with the fact that no archetype could define
with clinical rigor the concept of the pelvic examina-
tion.
4 DISCUSSION
The process of creating templates for an obstetrics
pregnancy hospitalization admission was possible by
mostly using archetypes already defined in OpenEHR
and NEHTA CKM’s. This is an advantage compared
to the process of creating new ones from scratch since
those already available to be shared have been val-
idated by a group of specialists and so its robust-
ness is inevitable. One archetype was created be-
ing derived from a pre-existent cluster - openEHR-
EHR-CLUSTER.exam-vagina.v1. This was neces-
sary since there wasn’t an already available archetype
to represent the findings of a speculum examination
performed on a pregnant woman. This archetype can
also be used in a more general context e.g. in a gy-
necology routine consult. However it still lacks the
analysis of obstetrics specialists by being submitted
to validation in openEHR CKM. Another limitation
has to do with the fact that the archetypes and their
fields were chosen according to the pre-existent spec-
ifications of ObsCare platform.
This migration from traditional HIS to a more
standardized and consistent OpenEHR specification
ModulationofExistentObstetricsEHRstotheopenEHRSpecification
441
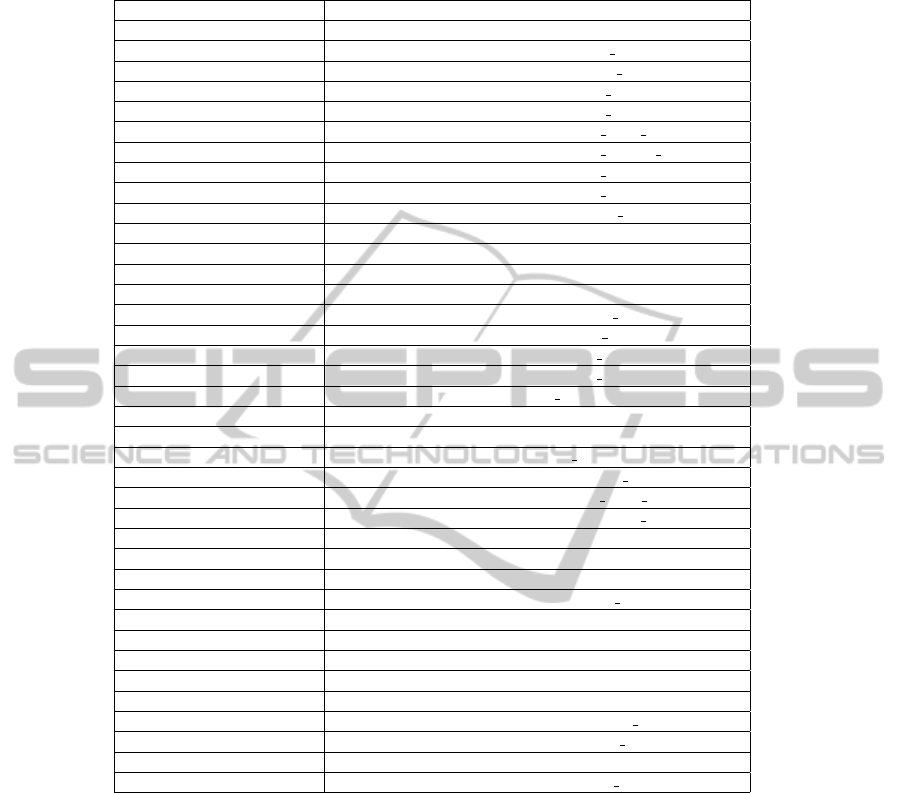
Table 1: List of archetypes used - all taken from the openEHR CKM except for the Pregnancy Summary which was taken
from NEHTA CKM and Examination of the vulva which was newly created.
Name ID
Adhoc heading openEHR-EHR-SECTION.adhoc.v1
Adverse Reaction openEHR-EHR-EVALUATION.adverse reaction.v1
Alcohol Use openEHR-EHR-OBSERVATION.alcohol use.v1
Blood Matching openEHR-EHR-OBSERVATION.blood match.v1
Blood Pressure openEHR-EHR-OBSERVATION.blood pressure.v1
Body Mass Index openEHR-EHR-OBSERVATION.body mass index.v1
Body Surface Area openEHR-EHR-OBSERVATION.body surface area.v1
Body Temperature openEHR-EHR-OBSERVATION.body temperature.v1
Body Weight openEHR-EHR-OBSERVATION.body weight.v1
Examination of the cervix openEHR-EHR-CLUSTER.exam-uterine cervix.v1
Examination of the fetus openEHR-EHR-CLUSTER.exam-fetus.v1
Examination of the uterus openEHR-EHR-CLUSTER.exam-uterus.v1
Examination of the vulva openEHR-EHR-CLUSTER.exam-vagina.v1
Examination openEHR-EHR-CLUSTER.exam.v1
Family History openEHR-EHR-COMPOSITION.family history.v1
Family History openEHR-EHR-EVALUATION.family history.v1
Fetal Heart Monitoring openEHR-EHR-OBSERVATION.fetal heart-monitoring.v1
Fetal Movement openEHR-EHR-OBSERVATION.fetal movement.v1
Free text openEHR-EHR-CLUSTER.free text.v1
Gestation openEHR-EHR-OBSERVATION.gestation.v1
Height/Length openEHR-EHR-OBSERVATION.height.v1
Imaging examination openEHR-EHR-ACTION.imaging exam.v1
Imaging examination result openEHR-EHR-OBSERVATION.imaging exam.v1
Medication Order List openEHR-EHR-SECTION.medication order list.v1
Medication Order openEHR-EHR-INSTRUCTION.medication order.v1
Oedema openEHR-EHR-CLUSTER.oedema.v1
Physical Examination openEHR-EHR-OBSERVATION.exam.v1
Pregnancy Summary openEHR-EHR-EVALUATION.pregnancy.v1
Problem/Diagnosis openEHR-EHR-EVALUATION.problem diagnosis.v1
Procedure Report openEHR-EHR-COMPOSITION.report-procedure.v1
Procedure undertaken openEHR-EHR-ACTION.procedure
.v1 Report openEHR-EHR-COMPOSITION.report.v1
Review openEHR-EHR-COMPOSITION.review.v1
Story/History openEHR-EHR-OBSERVATION.story.v1
Substance Use openEHR-EHR-OBSERVATION.substance use.v1
Tobacco Use openEHR-EHR-OBSERVATION.tobacco use.v1
Urinalysis openEHR-EHR-OBSERVATION.urinalysis.v1
Uterine contractions openEHR-EHR-OBSERVATION.uterine contractions.v1
has already been performed by others (Bernstein
et al., 2009)(Tapuria et al., 2013). As in the current
paper the advantages of using pre-existent archetypes
was valued and the biggest disadvantage resides in the
translation of the concepts when creating templates.
Other common problem noticed was the difference
between terminologies (Bernstein et al., 2009) (e.g.
degree and extent of oedema and fetal contractions)
which can indicate the need for a national or interna-
tional level standardization.
As the modulation of an existent EHR was pos-
sible and bearing in mind the advantages of using
openEHR to achieve national interoperability we can
see the enormous advantages of creating a national
level comission to create obstetrics templates. They
would have the minimal acceptable content. The ad-
vantages of this approach would be a common lan-
guage spoken by all HIS in the country, a consensus
on what is essential for an obstetrics EHR and the
flexibility to allow different regions or locals to add
more archetypes since the database schema doesn’t
have to suffer big changes thus also being very well
supported economically. The local archetype addi-
tion could be useful in cases where a specific detail
of the obstetric history that isn’t contained in one the
national accepted templates is necessary for academic
purposes.
Since the templates were created but not translated
to HTML and implemented in the OpenObscare ver-
sion that was built with a database schema that adapts
to OpenEHR specification, there is no information
about the possible easiness or difficulty in perform-
ing this process.
HEALTHINF2015-InternationalConferenceonHealthInformatics
442
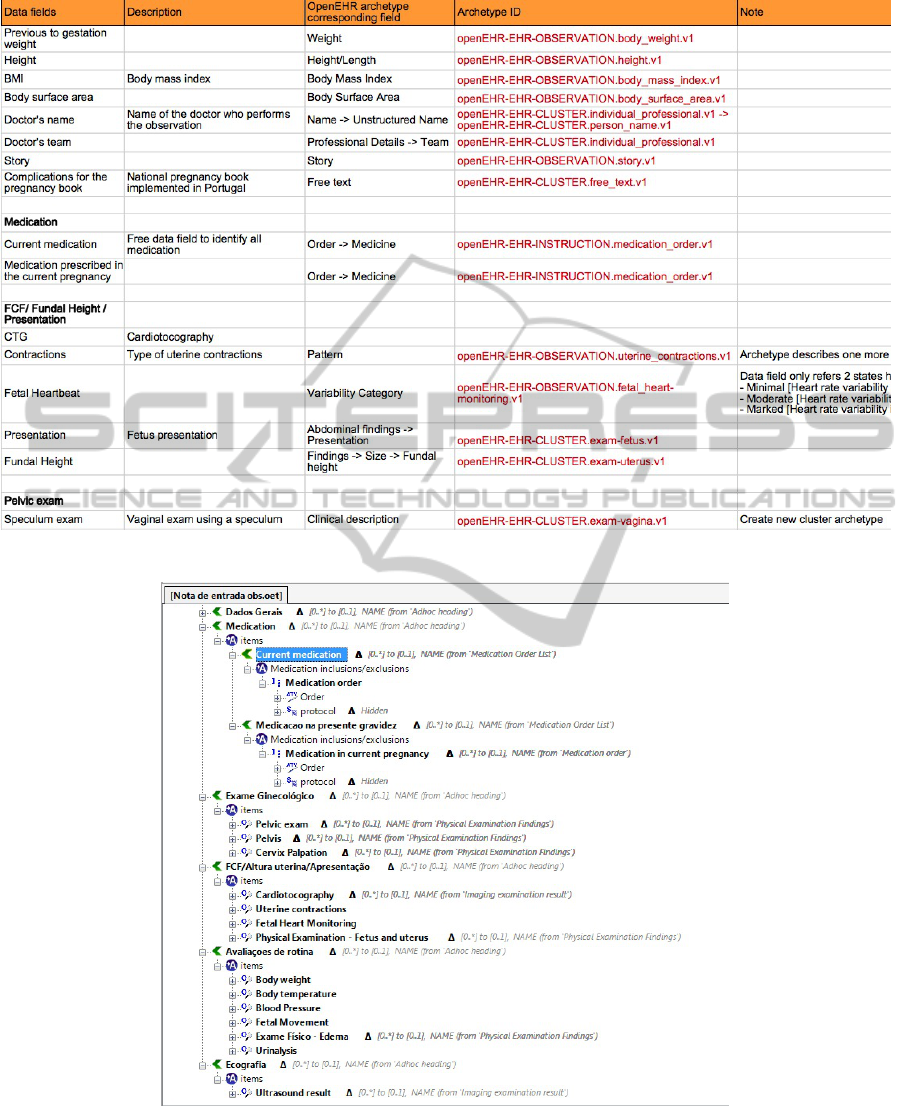
Figure 2: OpenObsCare form modulation spreadsheet for the Admission note.
Figure 3: Admission Template.
ModulationofExistentObstetricsEHRstotheopenEHRSpecification
443
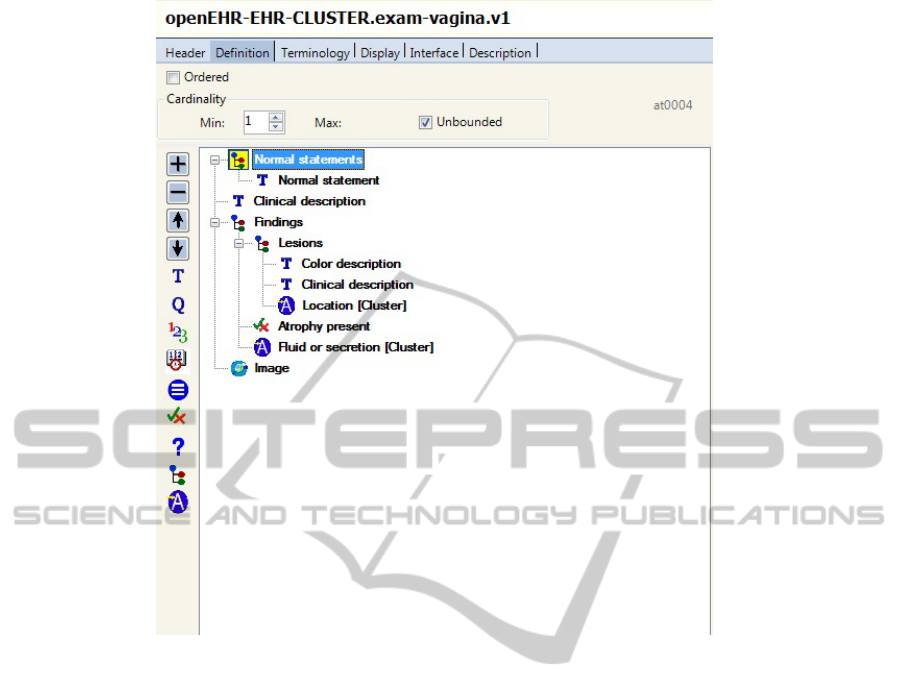
Figure 4: Vulva examination archetype.
5 CONCLUSION
In the current paper the modulation of clinical hos-
pitalization data existent in an obstetrics HIS to the
OpenEHR specification was performed. The process
was easier than the ”classic” one by which medical
specialists transmit the requirements of the system
and then these data models are created from scratch
since it can be easily achieved by reusing existent
validated archetypes. Both OpenEHR and NEHTA
CKM’s contain good solid archetypes with a com-
munity of medical specialists reviewing them in an
iterative process that aims to achieve an EHR stan-
dardization that allows interoperability between dif-
ferent systems. There was only the need to create 1
new archetype and to edit other. Using the method
described here in this paper the transition process to
an interoperable and semantics standardized EHR can
start. However there are still more steps ahead and the
process of application and maintainability of this type
of EHR must be ascertained. Furthermore this is an
effort that we would expect to be more effective if
there were nationwide standard templates defined by
a special comission of specialists.
REFERENCES
Beale, T. and Heard, S. (2007). openEHR - Architecture
Overview. Technical report.
Bernstein, K., Tvede, I., Petersen, J., and Bredegaard,
K. (2009). Can openEHR archetypes be used in a
national context? The Danish archetype proof-of-
concept project. Studies in health technology and in-
formatics, 150:147–51.
Delpierre, C., Cuzin, L., Fillaux, J., Alvarez, M., Mas-
sip, P., and Lang, T. (2004). A systematic review of
computer-based patient record systems and quality of
care: more randomized clinical trials or a broader ap-
proach? International journal for quality in health
care : journal of the International Society for Quality
in Health Care / ISQua, 16:407–416.
Dolin, R. H., Alschuler, L., Beebe, C., Biron, P. V., Boyer,
S. L., Essin, D., Kimber, E., Lincoln, T., and Matti-
son, J. E. (2001). The HL7 Clinical Document Archi-
tecture. Journal of the American Medical Informatics
Association, 8:552–569.
G.M. Bacelar-Silva, R. Chen, R. C.-C. (2012). From Clin-
ical Guideline to openEHR: Converting JNC7 into
Archetypes and Template. CBIS.
Hovenga, E. J. S. (2010). National standards in health infor-
HEALTHINF2015-InternationalConferenceonHealthInformatics
444

matics. Studies in health technology and informatics,
151:133–55.
Leslie, H. (2008). International developments in openEHR
archetypes and templates. Health Information Man-
agement Journal, 37(1):38–40.
Tapuria, A., Kalra, D., and Kobayashi, S. (2013). Contri-
bution of Clinical Archetypes, and the Challenges, to-
wards Achieving Semantic Interoperability for EHRs.
Healthcare informatics research, 19(4):286–92.
Xiao, L., Cousins, G., Courtney, B., Hederman, L., Fahey,
T., and Dimitrov, B. D. (2011). Developing an elec-
tronic health record (EHR) for methadone treatment
recording and decision support. BMC medical infor-
matics and decision making, 11(1):5.
Zeng, Q. and Cimino, J. J. (1999). Evaluation of a system
to identify relevant patient information and its impact
on clinical information retrieval. Proceedings / AMIA
... Annual Symposium. AMIA Symposium, pages 642–
646.
ModulationofExistentObstetricsEHRstotheopenEHRSpecification
445
