Demonstration of the Anomalous Origin of the Left Coronary Artery
from the Pulmonary Artery in Children using a Multi-Detector CT
Quanli Shen and Xihong Hu
Department of Radiology, Children’s Hospital, Fudan University, 399 Wanyuan Street, Shanghai, China
Keywords: Congenital Anomaly of the Coronary Artery, Computed Tomography, Children.
Abstract: Objective: To explore the value of multi-detector CT coronary angiography (CTCA) in detecting anomalous
origin of the left coronary artery from the pulmonary artery (ALCAPA) in children. Materials and methods:
Seven children aged from 2 months to 4 years who had surgically confirmed ALCAPA were enrolled in this
study. Their CTCA images were retrospectively analyzed. Results: The left coronary arteries were detected
to originate from the left wall of the main pulmonary artery in 2 patients, from the posterior wall of the main
pulmonary artery in 3 patients, and from the left pulmonary sinuse in 2 patients. In a 4-year-old girl, CTCA
showed collateral circulation between the right and the left coronary arteries. Conclusion: CTCA is a
valuable non-invasive method to show the anomalous origin of the coronary artery in small children with
ALCAPA.
1 INTRODUCTION
Anomalous origin of the left coronary artery from
the pulmonary artery (ALCAPA) is a rare congenital
cardiac anomaly. It is important to demonstrate the
anomalous origin of the left coronary artery and its
course before surgery. In this paper, we try to
explore the value of multi-detector CT coronary
angiography (CTCA) in detecting ALCAPA in
children.
2 MATERIALS AND METHODS
Seven children aged from 2 months to 4 years
(median age, 13 months) who had surgically
confirmed ALCAPA were enrolled in this study.
CTCA was performed with a 64-slice multidetector
CT scanner for all patients. Images were
reconstructed from the diastolic phase (75% R-R
interval) for a 4-year-old girl with heart rate 80 beats
per minute. For other patients with heart rates >120
beats per minute, images were reconstructed from
the end-systolic phase (45%~50% of the R-R
interval).
Two pediatric radiologists independently
assessed the image quality according to Paul et al
(Paul, 2011) and the origin of the coronary artery.
3 RESULTS
The result of image quality was summarized in
Table 1. CTCA showed enlargement of the left heart
in all patients. The left coronary arteries were
detected to originate from the main pulmonary artery
(MPA) in all patients (Figs. 1 and 2). The sites of
origin were summarized in Table 2. In a 4-year-old
girl, CTCA showed collateral circulation between
the right and the left coronary arteries (Fig. 3).
Table 1: Result of image quality.
Coronary artery Image quality scale
LMT
4.29±0.95
LAD
4.43±0.53
LCX
3.43±1.81
RCA
4.43±0.79
LMT = left main trunk, LAD = left anterior descending
artery, LCX = left circumflex artery, RCA = right
coronary artery.
Table 2: The origin of the left coronary artery.
Origin Case number
Left wall of the MPA 2
Posterior wall of the MPA 3
Left pulmonary sinuse 2
MPA = main pulmonary artery.
Shen Q. and Hu X..
Demonstration of the Anomalous Origin of the Left Coronary Artery from the Pulmonary Artery in Children using a Multi-Detector CT.
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)
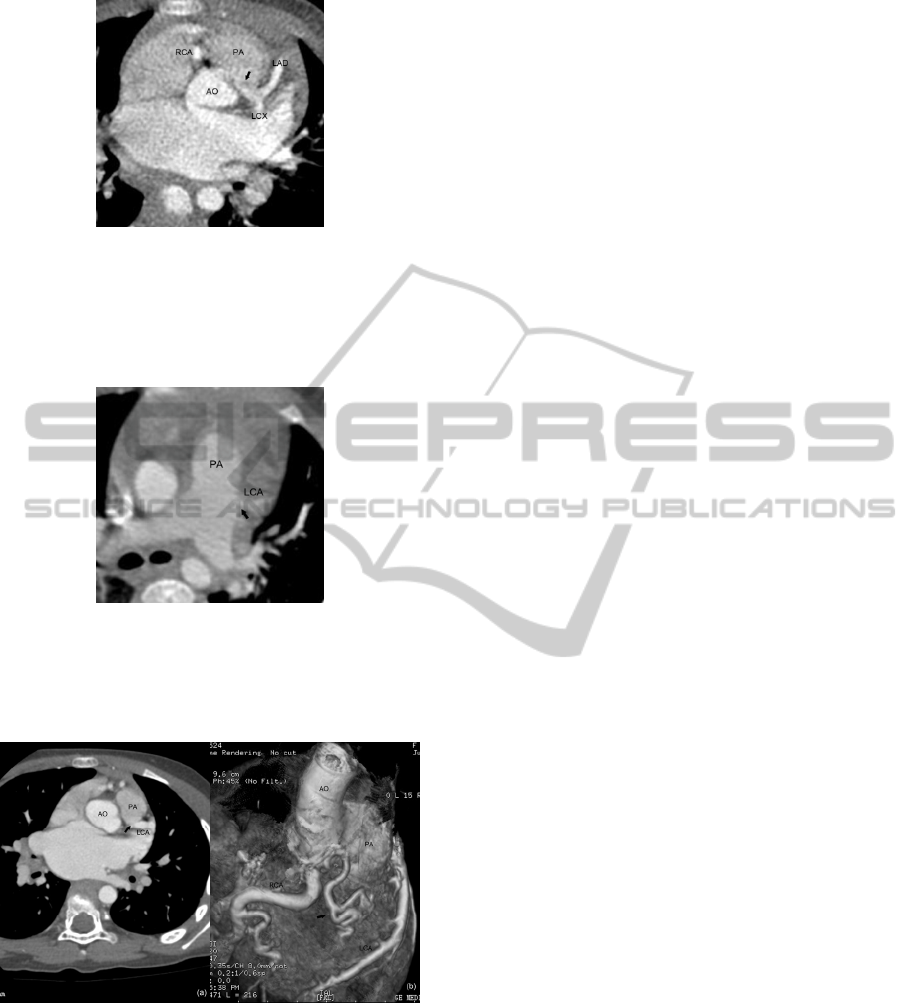
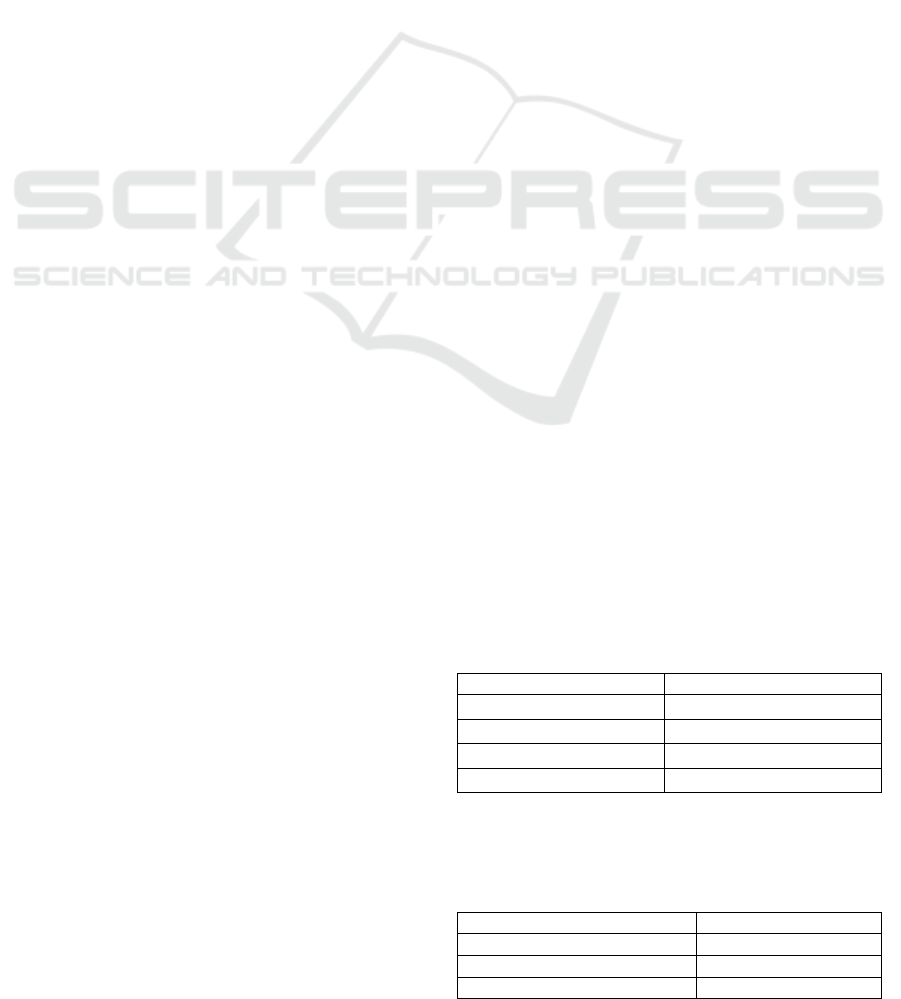
Figure 1: CTCA in a 21-month-old girl with ALCAPA.
Axial CT image demonstrates the left coronary artery
originates from the left pulmonary sinuse (arrow). AO =
aortic artery, PA = pulmonary artery, RCA = right
coronary artery, LAD = left anterior descending coronary
artery, LCX = left circumflex coronary artery.
Figure 2: CTCA in a 5-month-old girl with ALCAPA.
Axial CT image demonstrates the left coronary artery
originates from the left wall of the main pulmonary artery
(arrow). PA = pulmonary artery, LCA = left coronary
artery.
Figure 3: CTCA in a 4-year-old girl with ALCAPA. Axial
CT image (a) demonstrates the left coronary artery
originates from the posterior wall of the main pulmonary
artery (arrow). Volume rendering image (b) shows the
dilated right coronary artery and the tortuous collateral
vessel between the right and the left coronary artery
(arrow). AO = aortic artery, PA = pulmonary artery, LCA
= left coronary artery, RCA = right coronary artery.
4 DISCUSSION
CTCA can provide direct anatomic detail of the
coronary arteries and their origins as well as the
degree of collateralization (Cowles, 2007).
Depending on the acquired raw data, various phases
of the cardiac cycle may be available. In children
with low heart rate, images are usually reconstructed
from the diastolic phase (around 70% of the R-R
interval). But for children with heart rates >80/min,
it has been shown that the end-systolic phase
(between 35% and 45% of the R-R interval)
provides the best sharpness for the coronary arteries.
In case of cardiac motion artefacts, additional sets
may be reconstructed from other available phases of
the cardiac cycle (Lederlin, 2011).
One drawback of CTCA is the ionizing radiation.
Children have unequivocally higher radiosensitivity
and longer life expectancy than the older population
(Goo, 2012). In our study, we lowered the tube
voltage to 80-kV. The tube current was adapted to
the body weight. These settings do not impair image
quality too much and are considered sufficient for
diagnostic evaluation.
5 CONCLUSIONS
In conclusion, CTCA with a low-dose technique is a
valuable non-invasive method to show the
anomalous origin of the coronary artery in small
children with ALCAPA, especially for patients
whose origin of the left artery cannot be detected by
TTE. It is helpful to make a correct diagnosis before
surgery and lower the mortality.
REFERENCES
Paul JF., Rohnean A., Elfassy E., et al., 2011. Radiation
dose for thoracic and coronary step-and-shoot CT
using a 128-slice dual-source machine in infants and
small children with congenital heart disease. Pediatr
Radiol, 41(2):244-249.
Cowles RA., Berdon WE., 2007. Bland-White-Garland
syndrome of anomalous left coronary artery arising
from the pulmonary artery (ALCAPA): a historical
review. Pediatr Radiol, 37(9):890-895.
Lederlin M., Thambo JB., Latrabe V., et al., 2011.
coronary imaging techniques with emphasis on CT
and MRI. Pediatr Radiol, 41(12):1516-1525.
Goo HW., 2012. CT radiation dose optimization and
estimation: an update for radiologists. Korean J Radiol,
13(1):1-11.
