
Preliminary Design of Bilio-digestive Anastomosis by Magnetic
Compression
M
´
elanie Courtaudi
`
ere
1
, Nicolas Andreff
2
and St
´
ephane Koch
3
1
ISIFC, Universit
´
e de Franche-Comt
´
e, Besanc¸on, France
2
Femto ST Institute, UFC/CNRS/ENSMM/UTBM, Besanc¸on, France
3
CHU J. Minjoz, Besanc¸on, France
Keywords:
Magnetic Compression, Bile Duct, Duodenum, Ferrofluid, Obstruction, Jaundice.
Abstract:
Some experiments have been realized to determine the characteristics of magnets allowing for bilio-digestive
anastomosis by magnetic compression using a ferromagnetic gel and a magnet. The attraction distance be-
tween the ferromagnetic gel and the magnet was determined experimentally, under several configurations:
magnet shape, strength, number and arrangements. Two magnets with a strength of 14,000 Gauss and a di-
ameter of 12.7mm were necessary to attract 0.353mL of ferrofluid contained in a plastic sheath placed at 1cm
of the magnet. So the magnet is able to attract the ferrofluid. However, this procedure needs a large powerful
magnet which is not compatible for an immediate use in the human body. Nevertheless, this preliminary result
opens promising investigation paths.
1 INTRODUCTION
Currently two treatments are available to treat a bil-
iary obstruction (Figure 1). The first one is a non-
invasive treatment: the ERCP (endoscopic retrograde
cholangio pancreatography) using a duodenoscope
and a guide wire through the obstruction allows to in-
sert a biliary stent and thus to treat the obstruction
However if the guide wire can’t be inserted through
the tumor, the biliary stent cannot be placed and a
cholangitis occurs and kills the patient. The second
method is the invasive surgery to skirt the obstruc-
tion. For instance, duct-to-duct anastomosis by in-
Figure 1: Anatomic diagram of the gallbladder and the duo-
denum.
vasive surgery are performed. As a promising al-
ternative to surgery, anastomosis by magnetic com-
pression is currently practiced for intestinal anasto-
mosis (Cope, 1995; Myers et al., 2010; Uygun et al.,
2012; Pichakron et al., 2011; Gonzales et al., 2012;
Mimuro et al., 2003; Itoi et al., 2010). However, the
reported magnetic duct-to-duct compressions seem to
require surgical insertion of the magnet placed up-
stream the obstruction (and may be also a surgical re-
moval) (Fan et al., 2011).
To avoid invasive surgery, the creation of an
anastomosis by magnetic compression between the
blocked bile duct and the duodenum could be the so-
lution. However, the question of inserting a magnet in
the bile duct upstream the obstruction without surgery
is left unanswered yet.
Our proposal is to investigate the injection of a
biocompatible ferromagnetic gel in the biliary duct
and then study its attraction by the magnet placed in
the duodenum.
2 METHOD
2.1 A Novel Clinical Procedure
More precisely, the novel clinical protocol we foresee
218
Courtaudière M., Andreff N. and Koch S..
Preliminary Design of Bilio-digestive Anastomosis by Magnetic Compression.
DOI: 10.5220/0004903902180223
In Proceedings of the International Conference on Biomedical Electronics and Devices (BIODEVICES-2014), pages 218-223
ISBN: 978-989-758-013-0
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)
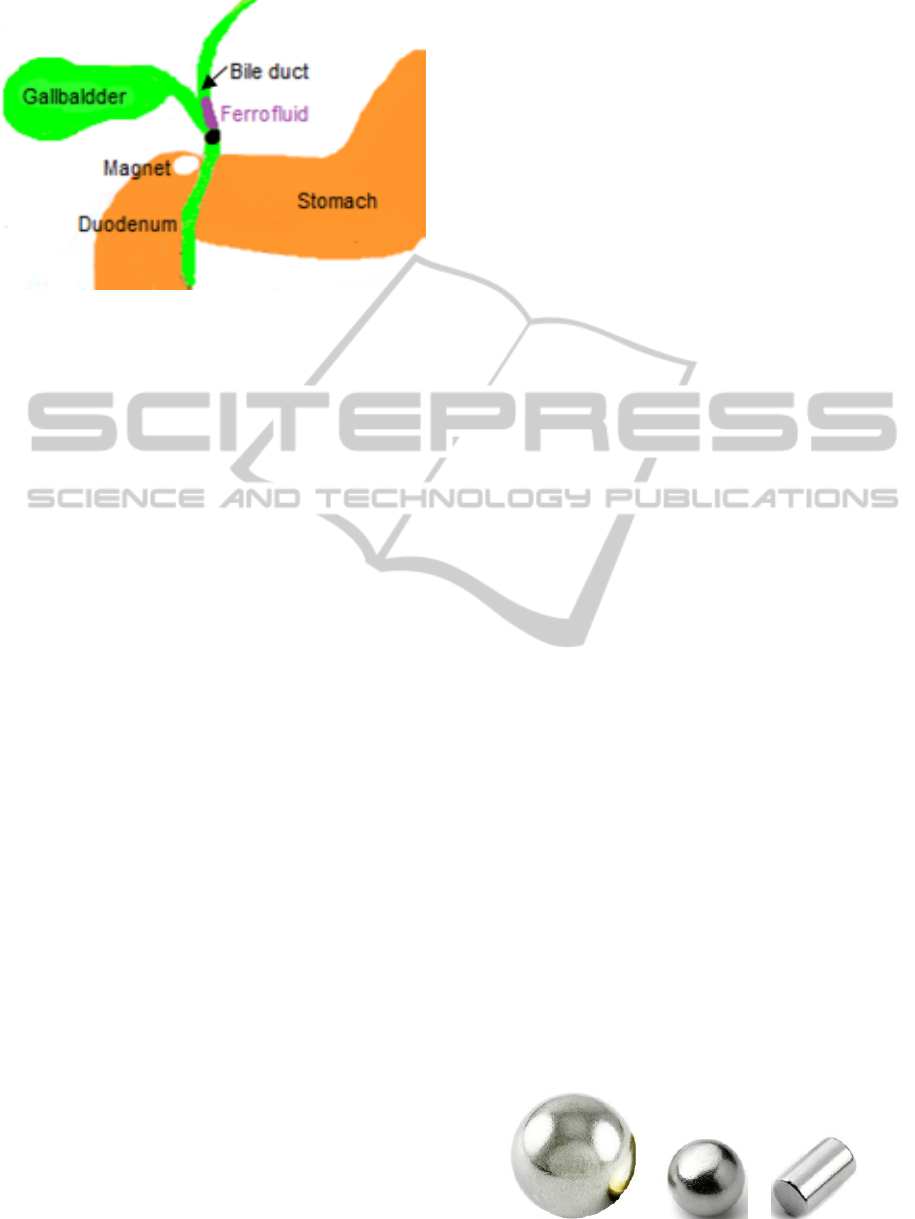
Figure 2: Anatomic diagram of the biliary duct and the duo-
denum + obstruction and considered treatment.
consists of the injection under EUS (endosonography)
of a biocompatible ferromagnetic gel by a FN with
a diameter of 0.9mm (19G) above the obstruction of
the bile duct. It thus will stay there until anastomo-
sis is done and will be removed or eliminated by the
new natural channel. Then a magnet would be placed
in the duodenum with a video endoscope. Removal
of the magnet and gel would occur by simple natural
elimination in the feces.
2.2 Anatomical Constraints
Before this protocol can be tested, the choice of ma-
terials must be tested in accordance to the anatomi-
cal constraints. Ideally, the magnet would be placed
through the operator channel, thus limiting the diam-
eter of the magnet to some 4.2 mm. Nevertheless, us-
ing a magnet with a somewhat larger diameter could
be enabled by holding over the scope with a nylon
wire.
The common bile duct has an internal diameter
included between 3mm and 8 mm in normal state
(>10mm after cholecystectomy or in case of obstruc-
tion). The volume of ferromagnetic gel that needs to
be considered must cope with the bile duct lumen.
The bile duct measures about 10cm (hepatic duct
and common duct) and the anastomosis can be located
only in front of the first duodenum. So the distance
between the gel and the duodenum magnet will be less
than 1cm. Therefore, we need to determine the attrac-
tion strength of the magnets which are necessary to
the attraction of a ferromagnetic gel localized at 1cm.
This is coherent with all the published studies,
where the magnets were placed very close from one to
another, with a maximal attraction distance between
the magnets lower than 20mm. Moreover, the diame-
ter of the different magnets varied between 2mm and
5mm. However, this does not tell much on how this
would extend to bilio-digestive anastomosis. Indeed,
replacing one magnet by ferromagnetic gel in order to
avoid a surgical insertion in the bile duct completely
changes the magnetic characteristics of the set-up.
The use of two kinds of magnets is reported:
• magnets in Samarium-Cobalt;
• magnets in Neodymium-Iron-Bore.
Both kinds are rare-earth magnets, identical in
term of magnetic flow density. Each of them is ap-
propriated for the anastomosis by magnetic compres-
sion but the obstructive strength of the magnets in
Samarium-Cobalt is higher and so better. The mag-
nets used in previous studies had a strength included
between 3000 Gauss (≈0.3 Tesla) and 3700 Gauss
(≈0.37 Tesla). Furthermore, to ensure their biocom-
patibility, many covering materials can be used, such
as chromium, titanium nitride or polycarbonate. Dif-
ferent magnets shapes were used: spherical, cylindri-
cal and ring-shaped. The spherical magnets show a
smooth and round surface, thus they can move and
roll up.
2.3 Experimental Set-up and Method
The experiments that were set-up consists of the
use of off-the-shelf ferrofluid and magnets in vari-
ous shapes, strengths and configurations. A ferrofluid
is a colloidal solution of ferromagnetic nanoparti-
cles, having a size of 10nm, put in solution in a
solvent or in water. The liquid becomes magnetic
when an external magnetic field is applied. However,
it keeps its colloidal stability. The ferrofluids have
the strange property that, when the magnetic field is
strong enough, the ferrofluid topology changes and
weakly rigid peaks appear on the surface. Ferroflu-
ids are, most frequently, composed of nanoparticles of
magnetite (Fe3O4) or of magnesite (γ-Fe2O3), which
are both iron oxide. Ferrofluids have an application in
many fields especially in medicine and biology (test-
ing of biological groups, contrast substance, cancerol-
ogy, to name a few).
The magnets used (Figure 3) were made in
neodymium iron bore and had the characteristics
given in Table 1, determined thanks to the state of art.
The magnets were placed in 3 different configu-
rations: horizontal (Figure 4), vertical (Figure 5) and
Sphere 1 Sphere 2 Cylinder 1
Figure 3: The different magnets used in the experiments.
PreliminaryDesignofBilio-digestiveAnastomosisbyMagneticCompression
219
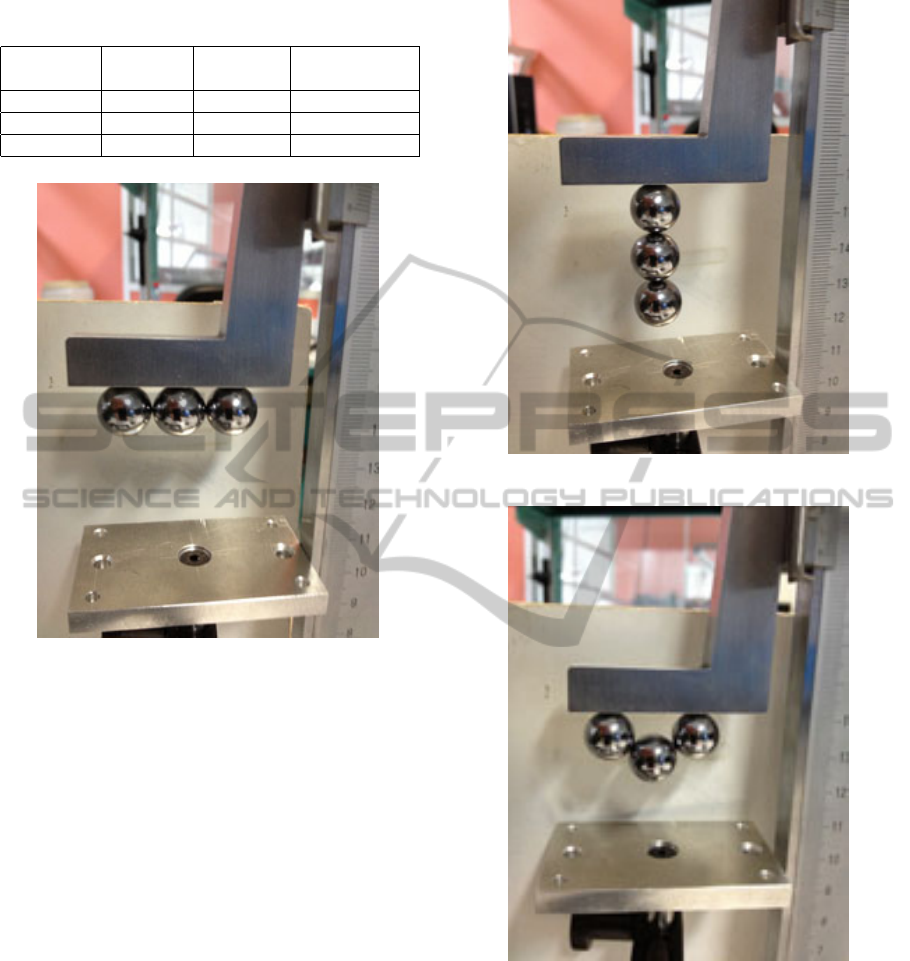
Table 1: Characteristics of the different magnets used in the
experiments.
Magnet Diameter Afterglow Magnetization
(mm) (Gauss)
Sphere 1 12.7 14,000 N42
Sphere 2 8 12,400 N38
Cylinder 1 5 13,500 N45
Figure 4: The 3 magnets in horizontal configuration.
“loop” when it was possible (Figure 6).
The magnets were used alone, by two or by three.
Their simultaneous utilization was always made with
magnets which had the same characteristics (there
was no mix between the different types of magnets).
To measure the necessary distance for the attrac-
tion between the ferrofluid and the magnet, the fol-
lowing assembly was realized thanks to a gauge (Fig-
ure 7). The gauge has a magnetic fixation system so
the magnet(s) were simply fixed by magnetization.
To represent the bile duct of the patient it was nec-
essary to use a material which had the same charac-
teristics as the human body. A plastic sheath (Fig-
ure 8) possessed the matching properties. The ferro-
magnetic liquid was inserted with a syringe B-D Plas-
tipak (capacity of 1mL) and a needle with a diameter
of 0.45mm. The plastic sheath had a diameter of 3mm
and a length of 5cm. The quantity of ferrofluid in-
serted was:
V = πr
2
h = π ∗ 0.15cm
2
∗ 5cm = 0.353mL (1)
The needle was made of stainless steel which was
not magnetic so there was not interaction with the fer-
rofluid.
Figure 5: The 3 magnets in vertical configuration.
Figure 6: The 3 magnets in the “loop” configuration.
The experimental protocol was to place the sheath
on the gauge base with the magnets far enough from
it. Then, the magnets were slowly descended until
the sheath was lifted up in the air by the magnetic
attraction.
The acquisition of the movement was made by a
camera Mikrotron EoSens 4 CXP with a 25mm Com-
putar objective. When the acquisition was finished,
the attraction distance could be calculated. It cor-
responded at the distance between the base and the
BIODEVICES2014-InternationalConferenceonBiomedicalElectronicsandDevices
220
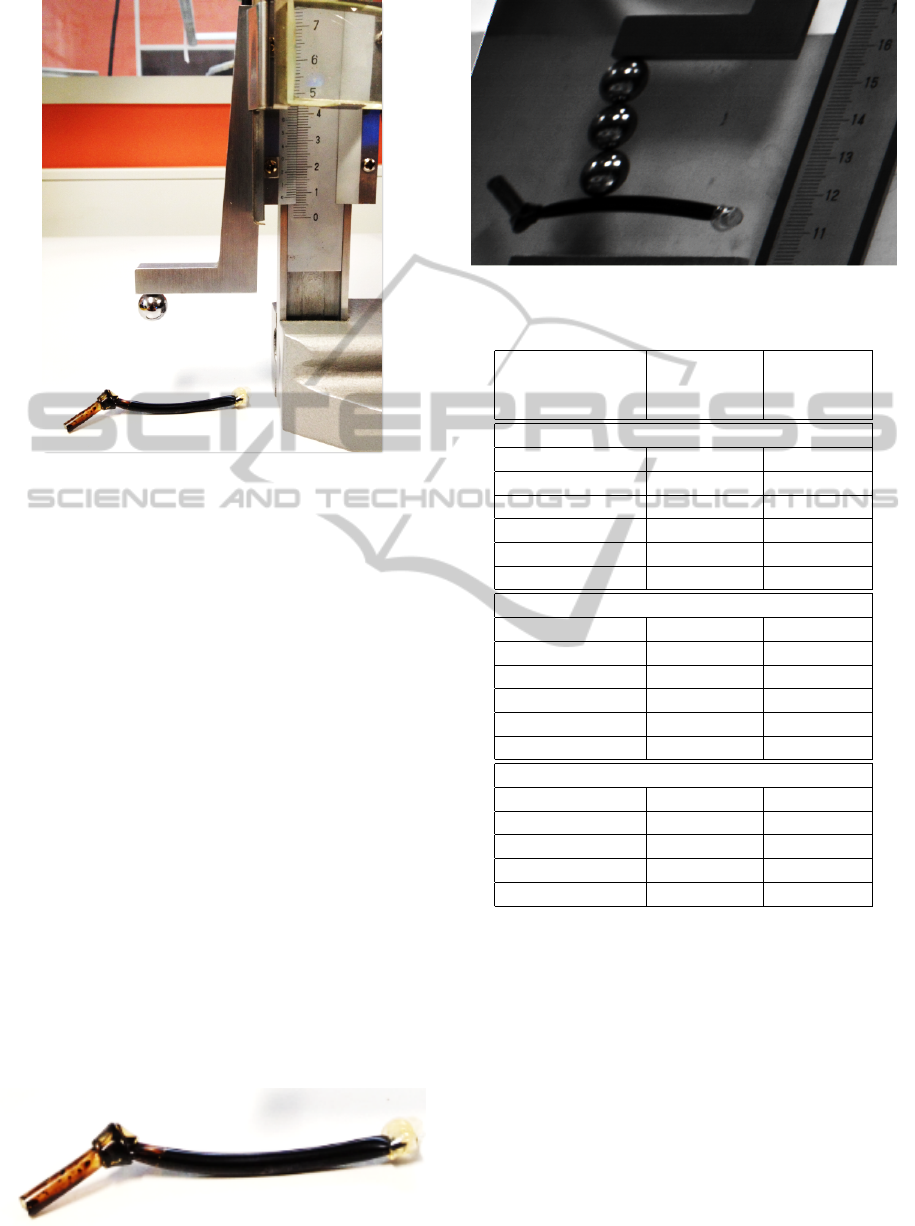
Figure 7: Experimental set-up.
end of the plastic sheath, once it had been attracted
by the magnet. The distance was directly legible on
the screen thanks to the graduation of the gauge (Fig-
ure 9).
To increase the reliability of the measures, each
were realized 5 times, then the mean of the results
was calculated.
3 RESULTS
The results are assembled in Table 2.
For a single spherical magnet, the horizontal and
the vertical measure with one magnet is the same, so it
appears only once in the table. The measures with the
cylindrical magnets have been realized on the “short
side” (Figure 10). The difference of attraction be-
tween the horizontal and the vertical position for the
same number of magnets was very low.
With the “loop” configuration the attraction dis-
tance decreased by 50%. This configuration was not
efficient, so it will be important to avoid this position-
ing for the magnets when they will be inserted in the
human body. For the same type of magnet, the attrac-
Figure 8: Plastic sheath of 3mm filled with ferrofluid.
Figure 9: Result of an acquisition.
Table 2: The results of the experiments with the 3 magnets.
Configurations Number of
magnets
Attraction
distance
(cm)
Spherical 1 (diameter 12,7mm)
Horizontal 1 magnet 0,98
2 magnets 0,98
3 magnets 1,08
Vertical 2 magnets 1,04
3 magnets 1
“loop” 3 magnets 0,56
Spherical 2 (diameter 8 mm)
Horizontal 1 magnet 0,64
2 magnets 0,44
3 magnets 0,6
Vertical 2 magnets 0,6
3 magnets 0,58
“loop” 3 magnets 0,28
Cylindrical 1 (diameter 5mm)
Horizontal 1 magnet 0,36
2 magnets 0,46
3 magnets 0,48
Vertical 2 magnets 0,44
3 magnets 0,46
tion distance fluctuated in function of the number of
magnets, sometimes the attraction distance is higher
with 2 magnets than with 3. This fluctuation was
caused by the positioning of the magnets one over the
other. Indeed the magnetization between them could
be in different directions, thus it influenced the total
properties of the magnet. These results showed the
variability of the attraction as a function of the posi-
tioning of the magnets. When they will be inserted
in the body it will be necessary to take care of their
orientation. The utilization of several magnets in-
creased the attraction distance. This increasing stays
low. Moreover for the patient, the utilization of many
magnets is not recommended for safety reasons (e.g.
PreliminaryDesignofBilio-digestiveAnastomosisbyMagneticCompression
221
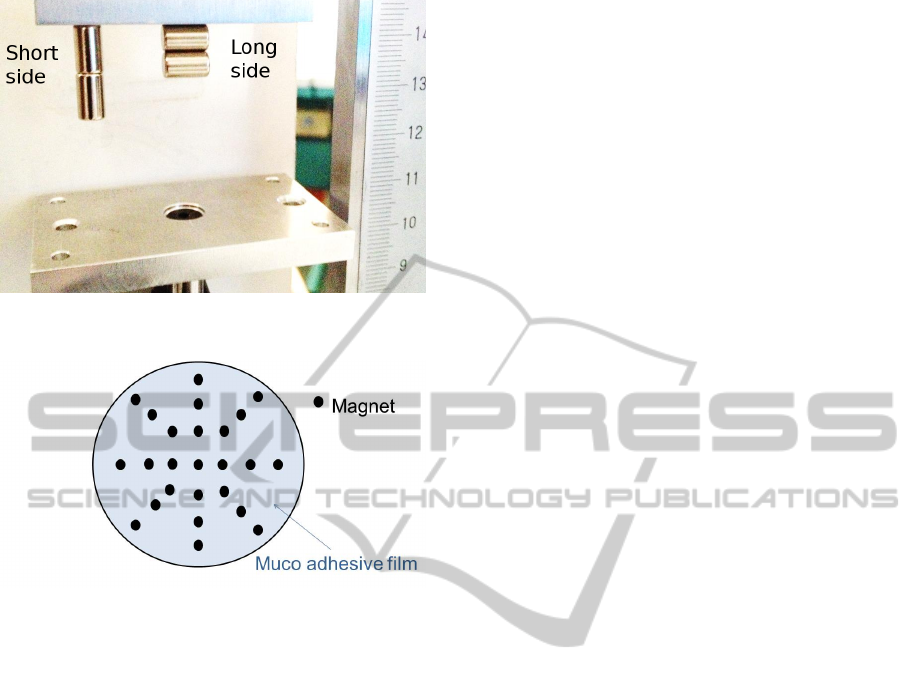
Figure 10: The two possible positions for the cylindrical
magnets.
Figure 11: The future configuration.
undesired magnetic compression in the small bowel),
unless a specific device allows to keep them together.
4 DISCUSSION
The bile duct and the duodenum are separated by a
distance of 1cm, so an attraction distance higher or
equal is necessary. However, the weight of the sheath
was measured to 1g, which means that the attraction
force is only 10mN at 1cm distance. This might not be
enough for starting the compression. Moreover, only
the utilization of many spherical magnets with a di-
ameter of 12.7mm and an afterglow of 14,000 Gauss
(≈1.4 Tesla) allows to achieve this value. The diame-
ter of such a magnet is not perfectly adapted for being
used in the body because it is both heavy and yet still
small enough to pass into the small bowel. The mi-
gration of this magnet should be avoided.
The alternative we will study now it the use of a set
of weaker magnets (Figure 11), attached together onto
a muco-adhesive patch, in order to increase both the
biocompatibility and efficiency of the device. Indeed,
this patch would cover a larger surface and hence the
set of magnets is expected to yield a stronger attrac-
tion force than a single one. Moreover, such a patch
is expected to have a stronger adhesion to the mu-
cosa and to less encumber the duodenum than a single
spherical magnet.
The patch would be inserted in the duodenum
thanks to the operator channel of the endoscope, then
it would be placed on the duodenum wall thanks to a
self-expandable fully covered metallic stent. To avoid
the attraction of the magnets when the patch is in the
operator canal and to allow its extension, the magnets
should be oriented in the same direction of polarity
(all the north faces are on the same side). To permit
the adhesion of the patch on the duodenum wall, the
patch could be covered with a muco-adhesive film.
Finally, the ferrofluid could be replaced by a
magneto-rheologic fluid. Such fluids are made of
lager ferromagnetic particles and thus have better
magnetic properties. They are considered to have
the drawback of sedimenting, contrary to ferrofluids
where nanoparticles stay apart. Nevertheless, this
might not necessarily be a concern in our case, if
properly handled, because it would improve the re-
moval of all magnetic material from the body at the
end of the treatment.
ACKNOWLEDGEMENTS
This work was partly supported by the French ANR
Labex ACTION (contract ”ANR-11-LABX-01-01”).
REFERENCES
Cope, C. (1995). Creation of compression gastroenteros-
tomy by means of the oral, percutaneous, or surgical
introduction of magnets: feasibility study in swine. J
Vasc Interv Radiol., 6(4):539–45.
Fan, C., Ma, J., Zhang, H.-k., Gao, R., Li, J.-h., Yu, L.,
Wu, Z., and Lv, Y. (2011). Sutureless intestinal anas-
tomosis with a novel device of magnetic compres-
sion anastomosis. Chinese Medical Sciences Journal,
26(3):182–189.
Gonzales, K. D., Douglas, G., Pichakron, K. O., Kwiat,
D. A., Gallardo, S. G., Encinas, J. L., Hirose, S., and
Harrison, M. R. (2012). Magnamosis iii: delivery of a
magnetic compression anastomosis device using min-
imally invasive endoscopic techniques. Journal of Pe-
diatric Surgery, 47(6):1291–1295.
Itoi, T., Yamanouchi, E., Ikeuchi, N., Kasuya, K., Iwamoto,
H., and Tsuchida, A. (2010). Magnetic compression
duct-to-duct anastomosis for biliary obstruction in a
patient with living donor liver transplantation. Gut
and liver, 4(Suppl 1):S96–S98.
Mimuro, A., Tsuchida, A., Yamanouchi, E., Itoi, T., Ozawa,
T., Ikeda, T., Nakamura, R., Koyanagi, Y., and Naka-
mura, K. (2003). A novel technique of magnetic com-
BIODEVICES2014-InternationalConferenceonBiomedicalElectronicsandDevices
222

pression anastomosis for severe biliary stenosis. Gas-
trointest Endosc., 58(2):283–7.
Myers, C., Yellen, B., Evans, J., DeMaria, E., and Pryor,
A. (2010). Using external magnet guidance and endo-
scopically placed magnets to create suture-free gastro-
enteral anastomoses. Surg Endosc., 24(5):1104–9.
Pichakron, K., Jelin, E., Hirose, S., Curran, P., Jamshidi,
R., Stephenson, J., Fechter, R., Strange, M., and Har-
rison, M. (2011). Magnamosis ii: Magnetic com-
pression anastomosis for minimally invasive gastroje-
junostomy and jejunojejunostomy. J Am Coll Surg.,
212(1):42–9.
Uygun, I., Okur, M., Cimen, H., Keles, A., Yalcin, O., Oz-
turk, H., and Otcu, S. (2012). Magnetic compression
gastrostomy in the rat. Pediatr Surg Int., 28(5):529–
32.
PreliminaryDesignofBilio-digestiveAnastomosisbyMagneticCompression
223
