
The Current State of EMA and ESM Study Design in
Mood Disorders Research: A Comprehensive
Summary and Analysis
Meredith L. Wallace
1,2
, Molly H. Carter
2,3
and Satish Iyengar
1
1
Department of Statistics, University of Pittsburgh, Pittsburgh, PA 15260, U.S.A.
2
Western Psychiatric Institute and Clinic, University of Pittsburgh, Pittsburgh, PA 15213, U.S.A.
3
Department of Psychology, Xavier University, Cincinati, OH 45207, U.S.A.
Abstract. Ecological momentary assessment (EMA) and experience sampling
methods (ESM) are becoming increasingly prevalent in mood disorders research
due to their potential for capturing underlying dynamic mood processes that can-
not be observed through traditional clinical visits. There have also been recent sta-
tistical developments that allow for innovative EMA/ESM-related research ques-
tions to be answered. However, even the most sophisticated statistical methods
cannot glean accurate representations of underlying mood processes when the
data are sampled inappropriately. Unfortunately, there are few resources investi-
gators can use to make informed decisions about EMA/ESM study design. Thus,
we perform a comprehensive summary of current EMA/ESM study design meth-
ods used in mood disorders research, explore the rationale behind study design
decisions, and investigate the relationship between compliance and various study
design features. Results from these analyses are used to suggest improvements
for designing and reporting future EMA/ESM studies.
1 Introduction
Clinical researchers and psychologists base their patient evaluations and diagnoses
largely on retrospective self-report of experiences. However, this type of information
can be biased by current mood state and day-to-day and even hour-to-hour variability in
experiences and symptoms [1–3]. Because mood disorders such as unipolar depression
(DEP), bipolar spectrum disorders (BD) and disorders of mood dysregulation such as
borderline personality disorder (BPD) are defined by changes in mood state and mood
variability [4], recall bias may be a particularly salient problem in this area. As a result,
information conventionally collected in clinical settings can fail to capture the continu-
ous, dynamic processes underlying mood disorders, thereby hindering researchers’ abil-
ities to characterize disease processes that may lead to specific and effective treatments.
Furthermore, information collected in a clinical setting may not provide a sufficiently
detailed understanding of a patient’s course of illness, potentially contributing to the
high rate of misdiagnosis across mood disorders [5–9].
Ecological momentary assessment (EMA) [1,2] and experience sampling method-
ology (ESM) [10,11] are data collection methods that allow clinical researchers and
L. Wallace M., H. Carter M. and Iyengar S..
The Current State of EMA and ESM Study Design in Mood Disorders Research: A Comprehensive Summary and Analysis.
DOI: 10.5220/0003878400030016
In Proceedings of the 2nd International Workshop on Computing Paradigms for Mental Health (MindCare-2012), pages 3-16
ISBN: 978-989-8425-92-8
Copyright
c
2012 SCITEPRESS (Science and Technology Publications, Lda.)

psychologists to capture a patient’s course of illness with greater frequency and sensi-
tivity through the use of hand-held technological devices. When studying disorders of
mood and mood dysregulation (henceforth, we will refer to them collectively as “mood
disorders”), EMA and ESM are particularly useful for capturing both the mean and in-
stability of mood [12]. EMA accomplishes this through the use of portable technologi-
cal devices, such as hand-held computers and cellular phones, to capture self-reported
measurements as they occur naturally in real time. In this way, EMA allows investiga-
tors to control timing precisely and track compliance [13]. EMA can also be used to
capture behavioral and physiological data; however, the focus herein is on self-reported
EMA. Like EMA, ESM also uses technological devices to capture data in real time;
however, ESM typically uses a digital watch or pager to prompt participants to record
their experiences in a paper-and-pencil diary [10,11]. In this manuscript we focus on
self-reported EMA and ESM, referring to them collectively as EMA.
As with any type of data collection method, EMA study design is of utmost im-
portance. In general, there is consensus that random sampling should be employed and
that the sampling frequency should match the temporal dynamics of the process of in-
terest [11,14,15]. However, there is a paucity of formal empirical evidence regarding
EMA study design methodology and rationale, particularly as it relates to the capture
of underlying mood processes. One important breakthrough study in this area was per-
formed by Ebner-Priemer and Sawitzki [14], who showed that a sampling interval of
less than 30 minutes could optimally capture underlying dynamic processes in BPD,
while intervals greater than 30 minutes could not. However, few research studies (espe-
cially those in clinical populations) are expected to support sampling intervals of less
than 30 minutes due to concerns of participant burden [14].
The field of mental health, and mood disorders in particular, could benefit from
the development of a more standardized set of EMA study design methods so that fu-
ture researchers can make more informed decisions (e.g., consider the stringency with
which clinical trials are designed and reported). As an initial step towards this end goal
we present a comprehensive summary and analysis of study design features in mood
disorders research, focusing on three specific aims:
1. Summarize the current state of EMA study design
2. Explore factors that researchers have considered when making EMA study design
decisions
3. Investigate the relationships among study design features and compliance
Results from these three aims are used to suggest ways that EMA investigators could
improve on the design and reporting of their studies.
2 Methods
To empirically describe and evaluate EMA study design in mood disorders research
it is necessary to use the actual studies, rather than manuscripts generated from these
studies, as the units of analysis. This presents a challenge because manuscripts and
studies are not related on a one-to-one basis. That is, multiple manuscripts may stem
4

from one study or, alternatively, one manuscript may analyze data from multiple stud-
ies. We employed the following strategy to develop a data base with the study as the
unit of analysis. First, we set inclusion and exclusion criteria for the types of studies that
would be considered. Second, we used literature search engines to locate manuscripts
that described studies meeting the inclusion and exclusion criteria. Third, we compared
manuscripts to determine which stemmed from the same studies and which merged data
from multiple studies. We contacted corresponding authors when questions or ambigui-
ties arose. Fourth, we used the manuscripts and additional resources from authors (e.g.,
EMA study questionnaires and protocols) to enter the study-level data. We describe
these steps in further detail below.
2.1 Study Inclusion and Exclusion Criteria
Study inclusion criteria were: 1) at least one subset of participants was clinically diag-
nosed with a mood disorder (BPD, DEP, or BD) and 2) an electronic ambulatory device,
including but not limited to beepers, hand-held computers, cellular phones, and wrist-
watches, was used to capture self-report data at multiple time points. Self-report EMA
may be either event-based (participant enters data before and/or after a prespecified
event occurs), prompt-based (participant enters data when prompted by a technologi-
cal device), or a combination of the two; however, the focus herein lies specifically in
prompt-based EMA because it relies heavily on a priori decisions regarding sampling
frequency. Thus, we excluded studies that did not include some type of prompt-based
EMA. We also excluded EMA case studies because of our specific focus on the use of
EMA to answer empirically-based research questions.
2.2 Search Strategy
We first aimed to identify all manuscripts arising from appropriate EMA studies by
performing literature searches in PubMed, PsycINFO, and ProQuest (Dissertations and
Theses) with the following keywords: ambulatory assessment, ecological momentary
assessment, experience sampling method, electronic diary, computer-assisted diary,
electronic momentary assessment, ecological validity, and hand-held computer. After
removing duplicate references, we performed a computerized search of the resulting
abstracts to narrow them down to those based on populations with mood disorders. Ab-
stract search terms included depression, depressive disorder, borderline, bipolar, mood
disorder, and affective disorder. All remaining abstracts were manually screened to
further identify those which stemmed from studies that fit within our inclusion and ex-
clusion criteria. The full text of each of the remaining manuscripts was then used to
determine whether the study from which it arose would be considered appropriate for
inclusion. Once the final subset of manuscripts was identified, the full text was again
examined to determine which manuscripts stemmed from the same EMA study and
which combined data from multiple EMA studies.
Figure 1 summarizes the search strategy and manuscript selection process. Table 1
lists the final 27 studies selected through this selection process. Because each of these
27 studies could generate multiple manuscripts, we refer to them in Table 1 by the by the
5
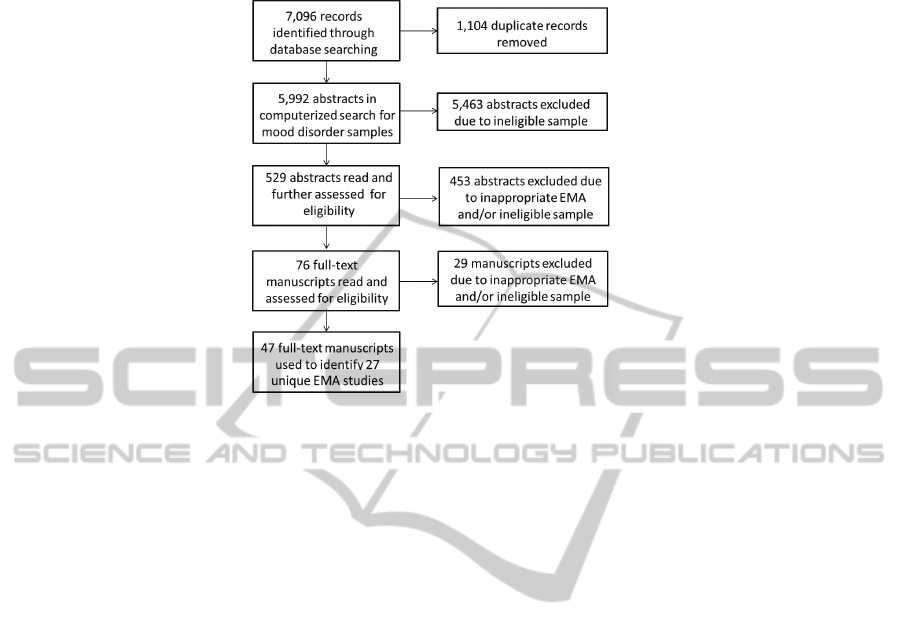
Fig.1. Flow diagram for manuscript and study selection.
first author and year of the earliest manuscript identified through the literature search.
Other related manuscripts are displayed in the “References” column.
2.3 Data Collection
The manuscripts referenced in Table 1 and additional author resources (e.g, EMA ques-
tionnaires and study protocols) were used to develop a data base that included: 1) study
design information, such as the sample size, duration of study, number prompts per day,
number of questions per prompt, and the type of EMA device used, 2) demographic
information for the samples used in each study, such as age and gender, 3) diagnos-
tic groups studied, 4) justification of sampling design, and 5) compliance information,
such as missing data and dropout percentages. When collecting the data from studies
that also included a randomized trial component, we only included EMA data from the
baseline weeks. This was done in an attempt to standardize the studies and also because
treatment assignment may impact measures of compliance.
2.4 Data Analysis
We used descriptive statistics to summarize the 27 EMA studies with respect to sam-
pling design and demographic and clinical characteristics of the participants (Aim 1).
To explore investigators’ rationale behind EMA study design selection (Aim 2) we first
summarized the study design justifications provided in the associated manuscripts. Be-
cause only eight of the 27 studies actually provided this explicit justification (see Table
1), we used our observed data to further explore the rationale behind current EMA study
design. This involved quantifying observed relationships among study design parame-
ters (the number of days of EMA study, the number of prompts per day, and the number
6

Table 1. First author and year of the earliest manuscript identified with each study. All other
related manuscripts are cited in the “References” column.
First Author (Year) References First Author (Year) References
Armistead, M.S. (2010) [16] Husky, M.M. (2010) [43]
Axelson, D.A. (2007)* [17–21] Links, P.S. (2007)* [44–46]
Barge-Schaapveld (1995) [22–25] Mokros, H.B. (1993) [47]
Ben-Zeev, D. (2009) [26] Myin-Germeys, I. (2003) [48–50]
Ben-Zeev, D. (2010) [27] Peeters, F. (2003) [51–54]
Biller, B.A. (2004) [28] Putnam, K.M. (2008) [55]
Bower, B. (2010)* [29,30] Stetler, C. (2004)* [56]
Campbell, J.A. (1998) [31] Stetler, C. (2005)* [57]
Conrad, A. (2008) [32] Stiglmayr, C.E. (2005) [58]
Delespaul, P. (2002) [33] Stiglmayr, C.E. (2008) [59]
Depp, C.A. (2010)* [34] Trull, T.J. (2008) [60,61]
Doyle, P.M. (2009)* [35] Wichers, M. (2010) [62]
Ebner-Priemer, U.W. (2006)* [14,36–40] Wolff, S. (2007) [63]
Glaser, J.P. (2008) [41,42]
*Reported rationale for study design
of questions per prompt) using scatter plots and Pearson product moment correlations.
Because the distributions of these variables were highly skewed, we used the natural
log transformation for all plots and calculations.
To investigate the relationships among study design features and compliance (Aim
3), we first needed to select a single compliance measure. After comparing various pos-
sibilities, we chose the percentage of unanswered prompts because it was frequently
reported and also easily constructed from other types of reported compliance statistics.
We calculated the percentage of unanswered prompts (P ) as the number of unanswered
prompts divided by the total number of possible prompts times 100. Some studies re-
ported only P
1
, the percentage of unanswered prompts based on a subset of N
1
< N
compliant participants with fewer than X% unanswered prompts. Hence, the percent-
age of unanswered prompts for the N
2
= N − N
1
participants, P
2
, was unknown
except for the fact that X % < P
2
≤ 100%. Because N
2
tended to be very small (e.g.,
one or two participants), we assumed that P
2
followed a uniform distribution and let
P
2
= .5 × (100 − X ). P was then calculated as a weighted average of the percentages
of unanswered prompts prompts for the N
1
compliant and N
2
noncompliant partici-
pants, that is, P =
1
N
(P
1
N
1
+ P
2
N
2
).
After calculating the percentage of unanswered prompts (P ), we used scatter plots
and Pearson product moment correlation coefficients to explore its relationships with
various study design features. Specifically, we focused on the number of questions per
prompt, the number of prompts per day, and the number of days of the EMA study.
Because these study design features need to be carefully balanced to reduce participant
burden, we also focused on their interactions: questions per day (questions per prompt
× prompts per day), prompts per study (promptsper day × days of study), and questions
per study (questions per prompt × prompts per day × days of study). Due to the highly
skewed distributions of all variables involved, we used the natural logs of these variables
in our plots and calculations.
7

3 Results
3.1 Aim 1: Summarize the Current State of EMA Research
Study design and demographic characteristics of the of the 27 EMA studies are summa-
rized in Table 2. In general, study participants tended to be female and Caucasian, with
a median age of 31. The study design characteristics selected by investigators (e.g., the
number of questions per prompts, number of prompts per day, and number of days of
EMA) varied widely across the 27 studies, as shown by the minimum and maximum
scores in Table 2.
In addition to selecting the number of questions, prompts, and days of EMA, inves-
tigators must also choose a method for distributing these prompts throughout the study
period. Within each day, the most common method for allocating prompts was random
blocking (e.g., divide waking hours into 6 blocks and randomly sample once during
each block); this method was used in 10 of the 27 studies (37%). Periodic sampling
with random error (e.g., sample every hour plus or minus a ranodmly drawn number of
minutes from a prespecified normal distribution) was the second most common method
for allocating EMA prompts, seen in 8 studies (29.6%). Only five (18.5%) studies used
random sampling (e.g., randomly select 10 times between the hours of 8:00 am to 10:00
pm) and only four (14.8%) studies used fixed time sampling (e.g., sample every hour
on the hour).
The method for distributing prompts throughout the study period must also take into
consideration the fact that participants are not able to answer prompts during sleep. Out
of 26 studies for which this information was known, 70.1% (n=19) set a fixed daily
interval during which prompts could occur (e.g., between the hours of 8:00 am to 10:00
pm for all participants). Other studies set a priori individualized sleep intervals tailed
to each participant’s needs (19.2%, n=5) or requested that the participant turn off the
device during sleep (7.7%, n=2).
Investigators must also determine which technological device (e.g., hand-held com-
puter, cellular phone, pager) to use to deliver each prompt. A hand-held computer, such
as a “personal digital assistant” (PDA) was used in 59.3% of studies (n = 16). The
next most frequently used technological device (37%, n=10) was a pager or wristwatch
along with a paper-and-pencil diary. One study (3.7%) used a cellular phone.
Patients with depression (major depression, minor depression, or dysthymia) were
included in eighteen studies (66.7%), patients with bipolar spectrum disorders were
included in five studies (18.5%), and patients with borderline personality disorder were
included in 9 (33.3%) studies. Other non-affective clinical groups (e.g., schizophrenia,
panic disorder) were included in four (14.8%) studies. Healthy controls were used as a
comparison group in 16 (59.3%) of the studies.
3.2 Aim 2: Explore Investigators’ Rationale behind EMA Study Design
Decisions
We first searched for explicit study design justifications in the manuscripts stemming
from each study. Overall, we identified some type of sampling justification in eight of
the 27 studies (29.64%). Two of these eight studies discussed rationale for the days on
8

Table 2. Demographic, clinical, and study design characteristics from 27 studies.
Characteristic N Observed Mean (SD) Median (Min, Max)
Demographic
Average Age 26 31.69 (11.14) 31.04 (10.01, 62.45)
% Female 24 79.08 (16.54) 78.10 (50, 100)
% Caucasian 12 65.61 (23.72) 64.70 (33.33, 100)
% Higher Education 17* 56.81 (33.39) 64.50 (0, 100)
% Married or Cohabitating 15* 35.34 (32.00) 26.37 (0, 88.24)
% Employed (Full- or Part-Time) 12* 37.40 (17.77) 43.24 (0, 55.73)
Study Design
Sample Size at Study Entry 27 78.67 (43.90) 73 (10, 164)
Days of EMA/ESM 27 9.33 (9.52) 6.79 (1, 42)
Prompts per Day 27 9.16 (9.63) 8 (1, 54)
Questions per Prompt 26 25.58 (16.91) 23 (1, 75)
Percentage of Missed Prompts 22 16.79 (10.40) 12.97 (3, 41.9)
*Among 24 studies with an average participant age > 18
which EMA sampling occurred, citing that “the weekend was chosen because it is the
time when adolescents have the greatest amount of free time and control over activities
and companions” [21] and “the same weekdays (Tuesday-Thursday) were used to have
a homogenous sample of days” [29].
The remaining six of the eight studies provided justification for the timing and/or
frequency of prompts within each day. In two different studies, Stetler et al. [56,57]
sampled cortisol levels at the same time as the self-reported EMA. Specific sampling
time intervals were chosen because they were previously found to “...adequately cap-
ture the diurnal pattern of cortisol secretion without placing undue burden on the par-
ticipants” [56] and because they were able to “...capture the early morning peak that is
part of the diurnal pattern of cortisol secretion” [57]. Ebner-Priemer and Sawitski [14]
emphasized that “the temporal dynamics of emotional-cognitive processes are largely
unknown”, and thus, their study employed multiple sampling frequencies to investi-
gate this question. Depp et al. [34] cited the “need to balance between ‘coverage’ of
affective experiences and subject burden.” Doyle [35] simultaneously employed three
different types of recording procedures “to capture mood ratings in close proximity to
the behaviors and events of interest...”. Links [44] stated that “random times were used
to approximate the daily range of a participant’s affective intensity within the context
and flow of the participant’s daily experience.”
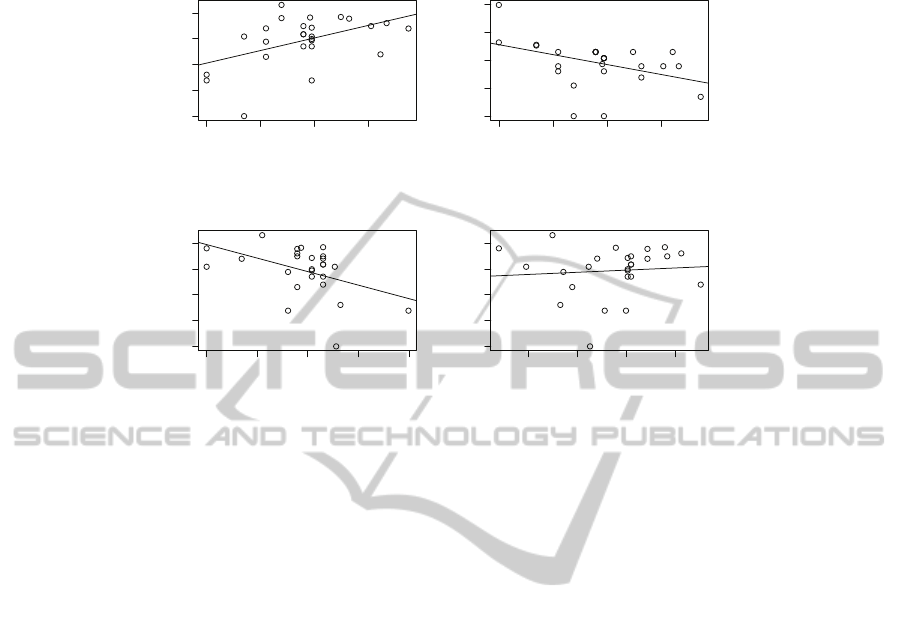
Because there were only eight studies for which an explicit sampling design ratio-
nale was found, we also explored the observed relationships among the number of days
of EMA, the number of prompts per day, and the number of questions per prompt. Be-
cause the study design variables were highly skewed, Figure 2 displays the associations
among the log-transformed study design variables (henceforth, the reader may assume
that all variables discussed are logged transformed). There was a strong negative as-
sociation between the number of questions per prompt and the number of prompts per
day (r = −.45, p = .02). Similarly, there was a strong negative association between the
number of prompts per day and the number of days of EMA (r = −.41, p = .03). There
9
0 1 2 3
0 1 2 3 4
Log of Days of EMA
Log of Questions per Prompt
r = .48; p = .01
0 1 2 3
0 1 2 3 4
Log of Days of EMA
Log of Prompts per Day
r = −.41; p = .03
0 1 2 3 4
0 1 2 3 4
Log of Prompts per Day
Log of Questions per Prompt
r = −.45; p = .02
2 3 4 5
0 1 2 3 4
Log of Total Number of Prompts
Log of Questions per Prompt
r = .08; p = .68
Fig.2. Scatter plots with least-squares regression lines displaying relationships among the log-
transformed number of questions, number of prompts, and number of days of EMA. Pearson
product moment correlation coefficients (r) and associated p-values are also displayed.
was a strong positive association between the number of questions per prompt and the
number of days of EMA (r = .48, p = .01). The positive association may reflect the
fact that more days of EMA leads to fewer prompts per day, which may in turn lead to
more questions asked at each prompt. There was no significant association between the
number of questions per prompt and the total number of prompts over the entire EMA
study.
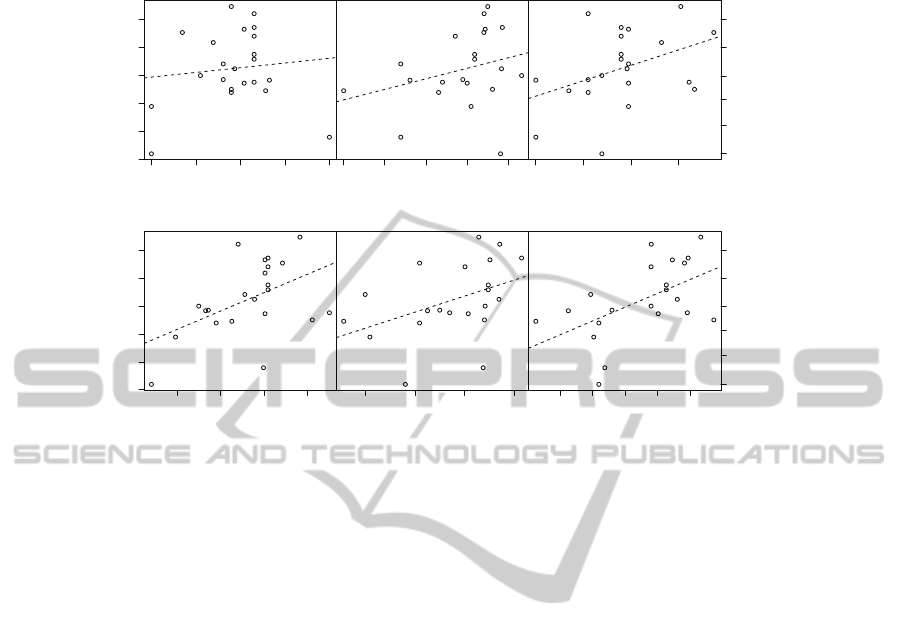
3.3 Aim 3: Investigate Relationships among Study Design Features and
Compliance.
Figure 3 illustrates the relationships among the study design features and the percent-
age of unanswered prompts. The number of questions per prompt and the number of
prompts per day were not significantly associated with the the percentage of unan-
swered prompts. After removing the high but valid outlier in the number of prompts
per day (estimated 54 prompts per day [36]), there was a strong positive relationship
between the percentage of unanswered prompts and the number of prompts per day (r
= .44, p=0.05); however, the removal of this outlier only highlights the potential lever-
age of the low outliers (1 prompt per day [56,57]). There were strong and borderline-
significant positive relationships between the percentage of unanswered prompts and
both the days of EMA and questions per day (questions × prompts). There were strong
and significant positive relationships between the percentage of unanswered prompts
and both the total number of prompts (prompts × days) and the total number of ques-
tions (questions × prompts × days).
10
0 1 2 3 4
Log Prompts per Day
Log % Unanswered Prompts
r = .11, p = .62
1.0 1.5 2.0 2.5 3.0 3.5
0 1 2 3 4
Log Questions per Prompt
r = .29, p = .20
0 1 2 3
Log Days in Study
r = .41, p = .06
3 5 8 12 20 33
% Unanswered Prompts
2 3 4 5
Log % Unanswered Prompts
r = .49, p = .02
Log Prompts in Study
(Prompts*Days)
1.0 1.5 2.0 2.5 3.0 3.5
r = .42, p = .06
3 4 5 6
Log Questions per Day
(Questions*Prompts)
4 5 6 7 8
r = .54, p = .01
Log Questions per Study
(Questions*Prompts*Days)
3 5 8 12 20 33
% Unanswered Prompts
Fig.3. Scatter plots with least-squares regression lines displaying relationships between the log-
transformed study design features and the log percentage of unanswered prompts. Pearson prod-
uct moment correlation coefficients (r) and associated p-values are also displayed.
4 Discussion
The overall goal of this manuscript is to provide researchers with a comprehensive
summary and analysis of current EMA study design methods used in mood disorders
research. To attain this goal, we summarized the current state of EMA study design used
in mood disorders research, explored the rationale behind the selection of EMA study
design features, and investigated the impact of study design on participant compliance.
The results of our comprehensivesummary highlight the wide variety of EMA study
design methods that are currently used in mood disorders research. This is particularly
true regarding to the number of questions per prompt, the number of prompts per day,
and the number of days of EMA. To a large degree, this variability may be explained
by the fact that each study has its own unique goals, participants, and restrictions; thus,
each study’s design must be tailored to meet its specific needs. However, insight into
this process was only provided to the reader in 8 of the 27 studies we investigated. This
lack of detail may pose challenges for newer investigators who may want to enter into
EMA research but do not have the experience to make these decisions on their own.
It may also lead more experienced EMA researchers to use only one familiar study
design, rather than tailoring each study design to match the temporal dynamics of the
underlying process of interest.
The lack of explicit detail regarding study design rationale makes it difficult to ex-
plore which considerations are most important for EMA investigators. However, the
observed negative associations between the number of prompts per day and both the
11

days of EMA and the questions per prompt suggests that investigators do indeed con-
sider the need to balance these study design features, presumably to reduce participant
burden.
Our investigation of the relationships among study design features and participant
compliance showed that the number of study days may havea bigger impact compliance
than either the number of prompts per day or the number of questions per prompt. Not
surprisingly, the strongest observed relationship showed a positive association between
the total number of questions asked during the study (questions × prompts × days)
and the percentage of unanswered prompts. Although these relationships may not be
unexpected, their quantification is an important first step towards developing a set of
study design guidelines for future EMA research.
Although care was taken to avoid potential biases and when developing the data
base, analyzing the data, and interpreting the results, there are limitations that must
be considered. One such limitation stems from the fact that our primary unit of anal-
ysis was the study. As such, features of each study often had to be identified through
manuscripts and by discussion with the actual study investigators. When investigators
could not be reached, the full scope of the original EMA study was not always evident;
this could lead to errors in the data base due to a lack of full study descriptions in these
manuscripts. However, the fact that these study design features were not immediately
evident from the manuscripts highlights the need for a more standardized approach to
developing and reporting EMA studies.
4.1 Future Directions
When designing EMA studies, two critical considerations are to obtain quality EMA
data at the frequency necessary for modeling underlying dynamic processes and to use
a sampling scheme that will not result in undue participant burden [14]. These con-
siderations are often at odds with one another, and thus, pose challenges for EMA re-
searchers. Furthermore, the “underlying temporal dynamics” of mood disorders are still
largely unknown [14], making it difficult to select the appropriate sampling frequency
even without participant constraints.
To overcome these challenges, it will be important to address three areas of EMA
research: 1) monitor and standardize current sampling methods 2) evaluate whether
current EMA sampling methods work actually work as intended (i.e., capture true un-
derlying processes), and 3) develop new EMA sampling methods that can balance the
need to effectively capture these processes while considering participant burden. The
research presented herein is aimed at addressing the first area of research. We are cur-
rently working to address areas two and three so that future EMA investigators can
have the tools they need to answer the critical EMA-related questions, both in the field
of mood disorders specifically and in the broader fields of mental and physical health
research.
References
1. Stone, A. A., Shiffman, S., Ecological Momentary Assessment in Behavioral Medicine. An-
nals of Behavioral Medicine 16 (1994) 199–202.
12

2. Shiffman, S., Stone, A. A., Hufford, M. R.: Ecological momentary assessment. Annual Re-
view of Clinical Psychology 4 (2008) 1–32.
3. Solhan, M. B., Trull, T. J., Jahng, S., Wood, P. K.: Clinical assessment of affective instabil-
ity: comparing EMA indices, questionnaire reports, and retrospective recall. Psychological
Assessment. 21 (2006) 425-436
4. American Psychiatric Association, A. P., Diagnostic and Statistical Manual of Mental Dis-
orders IV. 1994, Washington, D.C.: Author
5. Perlis, R. H.: Misdiagnosis of bipolar disorder. The American Journal of Managed Care 11
(2005) S271–S274
6. Zimmerman, M., Ruggero, C. J., Chelminski, I., Young, D.: Clinical characteristics of de-
pression outpatients previously overdiagnosed with bipolar disorder. Comprehensive Psychi-
atry 51 (2010) 99–105
7. Zimmerman, M., Galione, J. N., Ruggero, C. J., Chelminski, I., Dalrymple, K., Young, D.:
Overdiagnosis of bipolar disorder and disability payments. The Journal of Nervous and Men-
tal Disease 198 (2010) 452–454
8. Hirschfeld, R. M. A., Lewis, L., Vorknik, L.A.: Perceptions and impact of bipolar disorder:
How far have we really come? Results of the national depressive and manic-depressive as-
sociation 2000 survey of individuals with bipolar disorder. Journal of Clinical Psychiatry 64
(2003) 161–174
9. Blacker, D., Tsuang, M. D., Contested boundaries of bipolar disorder and the limits of cate-
gorical diagnosis in psychiatry. American Journal of Psychiatry 149 (1992) 1473–1483
10. Csikszentmihalyi, M., Larson, R.: Validity and Reliability of the Experience-Sampling
Method. Journal of Nervous and Mental Disease 175 (1987) 526–536
11. Bolger, N., Davis, A., Rafaeli, E.: Diary Methods: Capturing Life as it is Lived. Annual
Review of Psychology 54 (2003) 579–616
12. Ebner-Priemer, U. W., Trull, T. J.: Ecological Momentary Assessment of Mood Disorders
and Mood Dysregulation. Psychological Assessment 21 (2009) 463–475
13. Barrett L. S., Barrett, D. J.: An Introduction to Computerized Experience Sampling in Psy-
chology. Social Science Computer Review 19 (2001) 175–185
14. Ebner-Priemer, U. W., Sawitzki, G.: Ambulatory Assessment of Affective Instability in Bor-
derline Personality Disorder: The Effect of Sampling Frequency. European Journal of Psy-
chological Assessment 23 (2007) 238–247.
15. Capturing Momentary, Self-Report Data: A proposal for reporting guidelines. Annals of Be-
havioral Medicine 24 (2002) 236–243
16. Armistead, M. S., Looking for Bipolar Spectrum Psychopathology: Identification and Ex-
pression in Daily Life. Unpublished thesis, University of North Carolina at Greensboro
(2010)
17. Axelson D. A., Bertocci, M. A., Lewin, D. S., Trubnick, L. S., Birmaher, B., Williamson, D.
E., Ryan, N. D., Dahl, R. E.: Measuring Mood and Complex Behavior in Natural Environ-
ments: Use of Ecological Momentary Assessment in Pediatric Affective Disorders. Journal
of Child and Adolescent Psychopharmacology 13 (2003) 253–266
18. Silk, J. S., Dahl, R. E., Ryan, N. D., Forbes, F. E., Axelson, D. A., Birmaher, B., Siegle, G. J.:
Pupillary Reactivity to Emotional Information in Child and Adolescent Depression: Links to
Clinical and Ecological Measures. American Journal of Psychiatry. 164 (2007) 1873–1880
19. Whalen, D. J., Silk, J. S., Semel, M., Forbes, E. E., Ryan, N. D., Axelson, D. A., Birmaher, B.,
Dahl, R. E.: Caffeine Consumption, Sleep, and Affect in Natural Environments of Depressed
Youth and Healthy Controls. Journal of Pediatric Psychology 33 (2008) 258–367
20. Forbes, E. E., Hariri, A. R., Martin, S. L., Silk, J. S., Moyles, D. L., Fisher, P. M., Brown,
S. M., Ryan, N. D., Birmaher, B., Axelson, D. A., Dahl, R. E.: Altered Striatal Activation
Predicting Real-World Positive Affect in Adolescent Major Depressive Disorder. American
Journal of Psychiatry 166 (2009) 64–73
13

21. Bertocci, M. A.: Media Use by Children and Adolescents with and without Depression:
Going it Alone? Unpublished thesis, University of Pittsburgh (2010)
22. Barge-Schaapveld D. Q. C. M., Nicolson, N. A., van der Hoop, R. G., deVries, M. W.:
Changes in Daily Life Experience Associated with Clinical Improvement in Depression.
Journal of Affective Disorders 34 (1995) 139–154
23. Barge-Schaapveld D. Q. C. M., Nicolson, N. A., Berkhof, J., deVries M. W.: Quality of
Life in Depression: Daily Life Determinants and Variability. Psychiatry Research 88 (1999)
173–189
24. Barge-Schaapveld D. Q. C. M., Nicolson, N. A.: Effects of Antidepressant Treatment on the
Quality of Life: An Experience Sampling Study. Journal of Clinical Psychiatry 63 (2002)
477–485
25. Geschwind, N., Nicolson, N. A., Peeters F., van Os, J., Barge-Schaapveld D., Wichers, M.:
Early Improvement in Positive Rather than Negative Emotion Predicts Remission from De-
pression after Pharmacotherapy. European Neuropsychopharmacology 21 (2011) 241–247
26. Ben-Zeev, D., Young M. A., Madsen, J. W.: Retrospective Recall of Affect in Clinically
Depressed Individuals and Controls. Cognition and Emotion 23 (2009) 1021–1040
27. Ben-Zeev, D., Young, M. A.: Accuracy of Depressed Patients’ and Healthy Controls’ Ret-
rospective Symptom Reports: An Experience Sampling Study. The Journal of Nervous and
Mental Disease 198 280–285
28. Biller, B. A.: Examining the Utility of Ecological Momentary Assessment with Individual
Diagnosed with Depressive Disorder. Unpublished thesis, Pace University (2004)
29. Bower, B., Bylsma, L. M., Morris, B. H., Rottenberg, J.: Poor Reported Sleep Quality Pre-
dicts Low Positive Affect in Daily Life Among Healthy and Mood-Disordered Persons. Jour-
nal of Sleep Research 19 (2010) 323–332
30. Bylsma, L. M., Taylor-Clift, A., Rottenberg, J.: Emotional Reactivity to Daily Events in
Major and Minor Depression. Journal of Abnormal Psychology 120 (2011) 155–167
31. Campbell, J. A.: Caregivers’ Affective Attunement and Preadolescent Depression: An Eco-
logical Approach. Unpublished thesis, Chicago School of Professional Psychology (1998)
32. Conrad, A., Wilhelm, F. H., Roth W. T., Spiegel, D., Taylor, C.B.: Circadian affective, car-
diopulmonary, and cortisol variability in depressed and nondepressed individuals at risk for
cardiovascular disease. Journal of Psychiatric Research 42 (2008) 769–777
33. Delespaul, P., deVries, M., van Os, J.: Determinants of Occurrence and Recovery from Hallu-
cinations in Daily Life. Social Psychiatry and Psychiatric Epidemiology 37 (2002) 97–104.
34. Depp, C. A., Mausbach, B., Granholm, E., Cardenas, V., Ben-Zeev, D., Patterson, T.L.,
Lebowitz, B.D., Jeste, D.V.: Mobile Interventions for Severe Mental Illness: Design and
Preliminary Data from Three Approaches. The Journal of Nervous and Mental Disease 198
(2010) 715–721
35. Doyle, P. M.: Mood Variability and Symptomatic Expression in Women with Bulimia Ner-
vosa and Comorbid Borderline Personality Disorder. Unpublished thesis, Northwester Uni-
versity (2009)
36. Ebner-Priemer U. W., Kuo, J., Welch, S. S., Thielgen, T., Witte, S., Bohus, M., Linehan,
M. M.: A Valence-Dependent Group-Specific Recall Bias of Retrospective Self-Reports: A
Study of Borderline Personality Disorder in Everyday Life. The Journal of Nervous and
Mental Disease 194 (2006) 774–779
37. Ebner-Priemer, U. W., Welch, S. S., Grossman, P., Reisch, T., Linehan, M. M., Bohus, M.:
Psychophysiological Ambulatory Assessment of Affective Dysregulation in Borderline Per-
sonality Disorder. Psychiatry Research 150 (2007) 265–275
38. Ebner-Priemer, U. W., Juo, J., Kleindienst, N., Welch, S. S., Reisch, T., Reinhard, I., Lieb,
K., Linehan, M. M., Bohus, M.: State Affective Instability in Borderline Personality Disorder
Assessed by Ambulatory Monitoring. Psychological Medicine 37 (2007) 961–970
14

39. Reisch T., Ebner-Priemer U. W., Tschacher, W., Bohus, M., Linehan, M. M.: Sequences of
Emotions in Patients with Borderline Personality Disorder. Acta Psychiatrica Scandinavica
118 (2008) 42–48.
40. Ebner-Priemer, U. W., Kuo, J., Schlotz, W., Kleindienst, N., Rosenthal, M. Z., Detterer, L.,
Linehan, M. M., Bohus, M.: Distress and Affective Dysregulation in Patients with Borderline
Personality Disorder: A Psychophysiological Ambulatory Monitoring Study. The Journal of
Nervous and Mental Disease 196 (2008) 314–320
41. Glaser, J.-P., van Os, J., Mengelers, R., Myin-Germeys, I.: A Momentary Assessment Study
of the Reputed Emotional Phenotype Associated with Borderline Personality Disorder. Psy-
chological Medicine 38 (2008) 1231–1239
42. Glaser, J.-P., van Os, J., Thewissen, V., Myin-Germeys, I.: Psychotic Reactivity in Borderline
Personality Disorder. Acta Psychiatrica Scandinavica 121 (2010) 125–134
43. Husky, M. M., Gindre, C., Mazure, C. M., Brebant, C., Nolen-Hoeksema, S., Sanacora, G.,
Swendsen, J.: Computerized Ambulatory Monitoring in Mood Disorders: Feasibility, Com-
pliance, and Reactivity. Psychiatry Research 178 (2010) 440–442
44. Links, P. S., Eynan, R., Heisel, M. J., Barr, A., Korzekwa, M., McMain, S., Ball, J. S.: Af-
fective Instability and Suicidal Ideation and Behavior in Patients with Borderline Personality
Disorder. Journal of Personality Disorders 21 (2007) 72–86
45. Links, P. S., Eynan, R., Heisel, M., Nisenbaum, R.: Elements of Affective Instability As-
sociated with Suicidal Behavior in Patients with Borderline Personality Disorder. Canadian
Journal of Psychiatry 53 (2008) 112–116
46. Nisenbaum, R., Links, P.S., Eynan, R., Heisel, M.J.: Variability and Predictors of Nega-
tive Mood Intensity in Patients with Borderline Personality Disorder and Recurrent Suicidal
Behavior: Multilevel Analyses Applied to Experience Sampling Methodology. Journal of
Abnormal Psychology 119 (2010) 433–439
47. Mokros, H. B.: Communication and Psychiatric Diagnosis: Tales of Depressive Moods from
Two Contexts. Health Communication 5 (1993) 113–127
48. Myin-Germeys, I., Peeters, F., Havermans, R., Nicolson, N. A., deVries, M. W., Delespaul,
P., van Os, J.: Emotional Reactivity to Daily Life Stress in Psychosis and Affective Disorder:
An Experience Sampling Study. Acta Psychiatrica Scandinavica 107 (2003) 124–131
49. Havermans, R., Nicolson, N. A., deVries, M. W.: Daily Hassles, Uplifts, and Time Use in
Individuals with Bipolar Disorder in Remission. The Journal of Nervous and Mental Disease
195 745–751
50. Havermans, R., Nicolson, N. A., Berkhof, J., deVries, M. W.: Mood Reactivity to Daily
Events in Patients with Remitted Bipolar Disorder. Psychiatry Research 179 47–52
51. Peeters, F., Nicolson, N. A., Berkhof, J., Delespaul, P., deVries, M.: Effects of Daily Events
on Mood States in Major Depressive Disorder. Journal of Abnormal Psychiatry 112 (2003)
203–211
52. Peeters, F., Nicolson, N. A., Berkhof, J.: Cortisol Responses to Daily Events in Major De-
pressive Disorder. Psychosomatic Medicine 65(2003) 836–841
53. Peeters, F., Berkhof, J., Delespaul, P., Rottenberg, J., Nicolson, N. A.: Diurnal Mood Varia-
tion in Major Depressive Disorder. Emotion 6 (2006) 383–391
54. Peeters, F., Berkhof, J., Rottenberg, J., Nicolson, N. A.: Ambulatory Emotional Reactivity to
Negative Daily Life Events Predicts Remission from Major Depressive Disorder. Behavior
Research and Therapy 48 (2010) 754–760
55. Putnam, K. M., McSweeney, L. B.: Depressive Symptoms and Baseline Prefrontal EEG Al-
pha Activity: A Study Utilizing Ecological Momentary Assessment. Biological Psychiatry
77 (2008) 237-240
56. Stetler, C., Dickerson, S. S., Miller, G. E.: Uncoupling of Social Zeitgebers and Diurnal
Cortisol Secretion in Clinical Depression. Psychoneuroendocrinology 29 (2004) 1250–1259
15

57. Stetler, C., Miller, G. E.: Blunted Cortisol Response to Awakening in Mild to Moderate De-
pression: Regulatory Influences of Sleep Patterns and Social Contexts. Journal of Abnormal
Psychology 114 (2005) 697–705
58. Stiglmayr, C. E., Grathwol, T., Linehan, M. M., Ihorst, G., Fahrenberg, J., Bohus, M.: Aver-
sive Tension in Patients with Borderline Personality Disorder: A Computer-Based Controlled
Field Study. Acta Psychiatrica Scandinavica 111 (2005) 372–379
59. Stiglmayr, C. E., Ebner-Priemer, U. W., Bretz, J., Behm, R., Mohse, M., Lammer, C.-
H., Anghelescu, I.-G., Schmahl, C., Schlotz, W., Kleindienst, N., Bohus, M.,: Dissociative
Symptoms are Positively Related to Stress in Borderline Personality Disorder. Acta Psychi-
atrica Scandinavica 117 (2008) 139–147
60. Trull, T. J., Watson, D., Tragessser, S. L., Jahng, S., Wood, P. K., Piasecki, T.M: Affective
Instability: Measuring a Core Feature of Borderline Personality Disorder with Ecological
Momentary Assessment. Journal of Abnormal Psychology 117 (2008) 647–661
61. Jahng, S., Wood, P. K., Trull, T. J.: Analysis of Affective Instability in Ecological Momen-
tary Assessment: Indices Using Successive Difference and Group Comparison via Multilevel
Modeling. Psychological Methods 13 (2008) 354–375
62. Wichers, M. H., Peeters, F., Geschwind, N., Jacobs, N., Simons, C. J. P., Derom, C., Thiery,
E., Delespaul, P. H., van Os, J.: Unveiling Patterns of Affective Responses in Daily Life may
Improve Outcome Prediction in Depression: A Momentary Assessment Study. Journal of
Affective Disorders 124 (2010) 191–195
63. Wolff, S., Stiglmayr, C., Bretz, H. J., Lammers, C.-H., Auckenthaler, A.: Emotion Identifi-
cation and Tension in Female Patients with Borderline Personality Disorder. British Journal
of Clinical Psychology 46 (2007)347–360
16
