
SUPPORTING NURSING CARE ASSESSMENT PROTOCOLS
WITH SMARTPHONES
Ilídio C. Oliveira
1,2
, Nelson Silva
3
, Ivo da Veiga
1
and João P. S. Cunha
1,2
1
IEETA - Institute of Electronics and Telematics Engineering of Aveiro, Aveiro, Portugal
2
Dep. of Electronics, Telecommunications and Informatics, University of Aveiro, Aveiro, Portugal
3
Hospital Infante Dom Pedro, Aveiro, Portugal
Keywords: Nursing informatics, Mobile devices, Skin integrity.
Abstract: Technological advances in mobile phones make them appealing to support nursing care at the point of
treatment, especially by combining the easy-of-use, mobility and wireless communications. Novel
capabilities, such as picture capturing, enlarge the applications scope. In this work, we present the HOPE
system to facilitate nursing care documentation, by leveraging on standard off-the-shelf mobile phones. The
proposed system moves a substantial part of the work usually deferred and performed at desktop computers
to the moment and place of care. In addition, health professionals can document the clinical cases with
photos, using the mobile phone built-in camera, which is being applied in diabetic foot consultation. Basic
support for wound measurement is available. The information acquired is integrated in the patient’s
Electronic Health Record and can be shared using the mobile devices or the workstations. The proposed
system is in pilot use at two Portuguese hospitals targeting inpatient care and diabetic foot consulting.
1 INTRODUCTION
Care provision includes a significant amount of
effort on effective documentation of patient
conditions and performed actions. In nursing care,
documentation time is estimated to surpass half of
the nurse’s activities (Kossman and Scheidenhelm,
2008). The introduction of Electronic Health
Records (EHR) (Häyrinen et al., 2008) including the
nursing domain, led professionals, in many cases, to
defer the documentation activities, since the
available information systems are not well adjusted
to be used at the bed side (Stevenson et al., 2010);
(Andersen et al., 2009).
An emergent paradigm is the use of handheld
computers to support nursing care planning and
recording (Garrett and Klein, 2008); (Lu et al.,
2005). These devices meet the mobility requirements
of the practice and their integration with
organization wide information systems can raise the
efficiency of nursing care documentation (Lu et al.,
2005).
The convergence of handheld computers (or
Personal Digital Assistants) and mobile phone
features in the same devices originated the nowadays
popular smartphone concept. As a consequence,
there’s a mass expansion of the familiarity with
smartphones operation and significant decrease on
devices cost. This trend extends the opportunities to
use modern smartphones in nursing care and
telemedicine (Istepanian et al., 2006); (Ebner et al.,
2008). The combination of intrinsic support for
mobility, rich and intuitive user interfaces, and
wireless communications provide sound arguments
for their introduction in care settings, if articulated
with the existent “ecosystem” of health information
systems.
Mobile devices are being used to take pictures of
wounds and skin lesion to document clinical cases.
Such approaches can be found in teledermatology
projects (Ebner et al., 2008); (Pirris et al., 2010).
Nurses are also aware of its potential (Berglund et
al., 2007) but implementations are still lacking.
In this work, we present the HOPE system,
which uses smartphones to help nursing care
recording at the point of care. The smartphones are
not expected to replace the existing desktop-based
solutions, but act as a practical first line or recording
that can be performed at patient side. In addition, the
smartphone’s built-in camera is also used to capture
images of lesions, allowing for skin integrity
monitoring of inpatients and to monitor diabetic foot
81
C. Oliveira I., Silva N., da Veiga I. and P. S. Cunha J..
SUPPORTING NURSING CARE ASSESSMENT PROTOCOLS WITH SMARTPHONES.
DOI: 10.5220/0003783100810086
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2012), pages 81-86
ISBN: 978-989-8425-88-1
Copyright
c
2012 SCITEPRESS (Science and Technology Publications, Lda.)
lesions.
The motivating context for this work arose from
the nursing practice at Hospital São Sebastião
(HSS), located in Feira, Portugal. Presently, the
system has been also in pilot used at a second
Hospital (Hospital Infante Dom Pedro, Aveiro,
Portugal).
2 METHODS
2.1 Workflow 1: Patient Assessment
Protocol
The HSS hospital uses a comprehensive EHR, which
includes the nursing record too. The system provides
support for hundreds of data fields to follow
inpatient nursing care. The patient assessment
protocol, in particular, includes over 120 data fields,
from more subjective information, like social
context and habits, to more objective details, such as
biosignals, pain scales and wounds characteristics.
The assessment stage is performed each day (not
necessarily altogether) in the presence of the patient,
but the nursing staff opts to defer recording activities
to a later stage, and use paper notes as a memory
helper. This is justified by the absence of mobile
interfaces and the complexity of the desktop system.
In this context, the Health-On-Palm Environment
(HOPE) system has been proposed to facilitate
patients’ assessment routines by nurses. The
objective of HOPE is not to replace the existing and
comprehensive desktop system, but to move a subset
of those recording needs to the nurses’ smartphone.
The careful selection of which segments of the
nursing evaluation protocol were to be supported in
the mobile device became a critical success factor.
This definition has been achieved over multiple
interactions with domain experts, to avoid system
rejection due to insufficient involvement of domain
users (Stevenson et al., 2010).
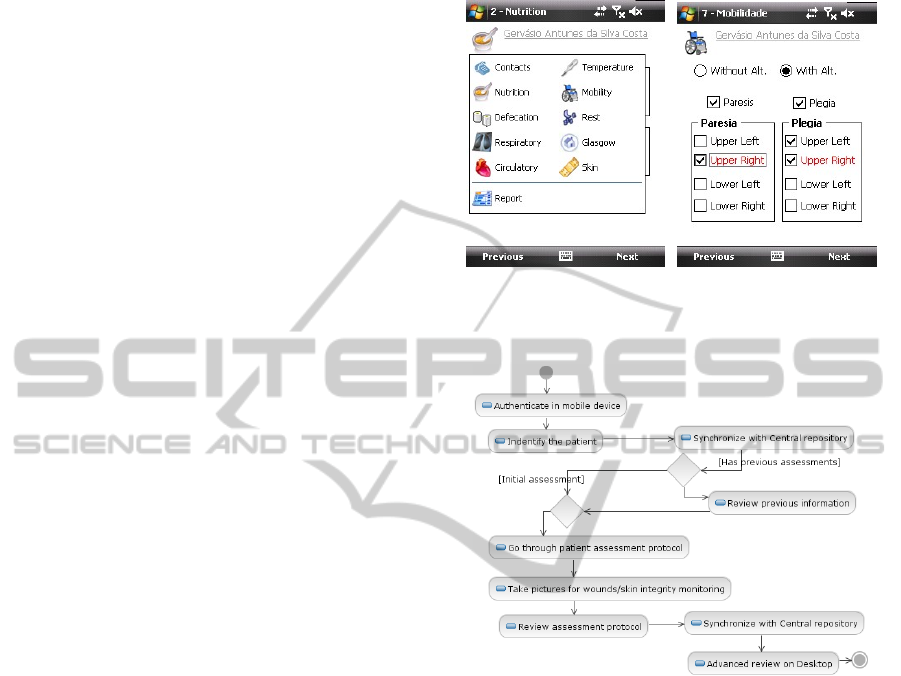
Using the HOPE system, the nurse starts by
authenticate himself on the mobile device (Fig. 1).
Patient details can then be easily retrieved from
the Hospital-wide EHR by entering the record
number on the device or by reading it from a bar
code (often available in stickers and bracelets) using
the built-in camera. The previous assessment context
is retrieved and can be accessed in the smartphone.
The nurse will then complete the assessment
protocol, going through a wizard-like interaction
(Fig. 2). Errors in data entry (e.g.: inconsistent
values) are immediately revealed by changing field
colours. At any point, the data collected can be
uploaded to the central servers using the device
wireless networking capabilities.
Figure 1: Views on the step-by-step assessment protocol.
Left: steps to be completed. Right: signaling error with
color feedback.
Figure 2: Nursing assessment protocol executed in the
HOPE mobile system.
2.2 Workflow 2: Diabetic Foot Protocol
The HOPE application enables the use of the built-in
camera in the diabetic foot consultation. The patient
will initially receive treatment at a primary care
facility but, if suffering from severe conditions, s/he
will be referred to secondary care provider
(Hospital). After the patient acute conditions have
been stabilized, s/he will be followed at the primary
care again (Fig. 3).
Wounds related to the diabetic foot condition
take a long time to heal, usually spanning for several
months. During this time, the wound evolution can
be hard to monitor without a visual record, due to
the time span and the number of care professionals
involved (different teams and service points). Note
that wound assessment is being conducted at each
care organization, but little information is usually
shared, especially with respect to multimedia types.
HEALTHINF 2012 - International Conference on Health Informatics
82
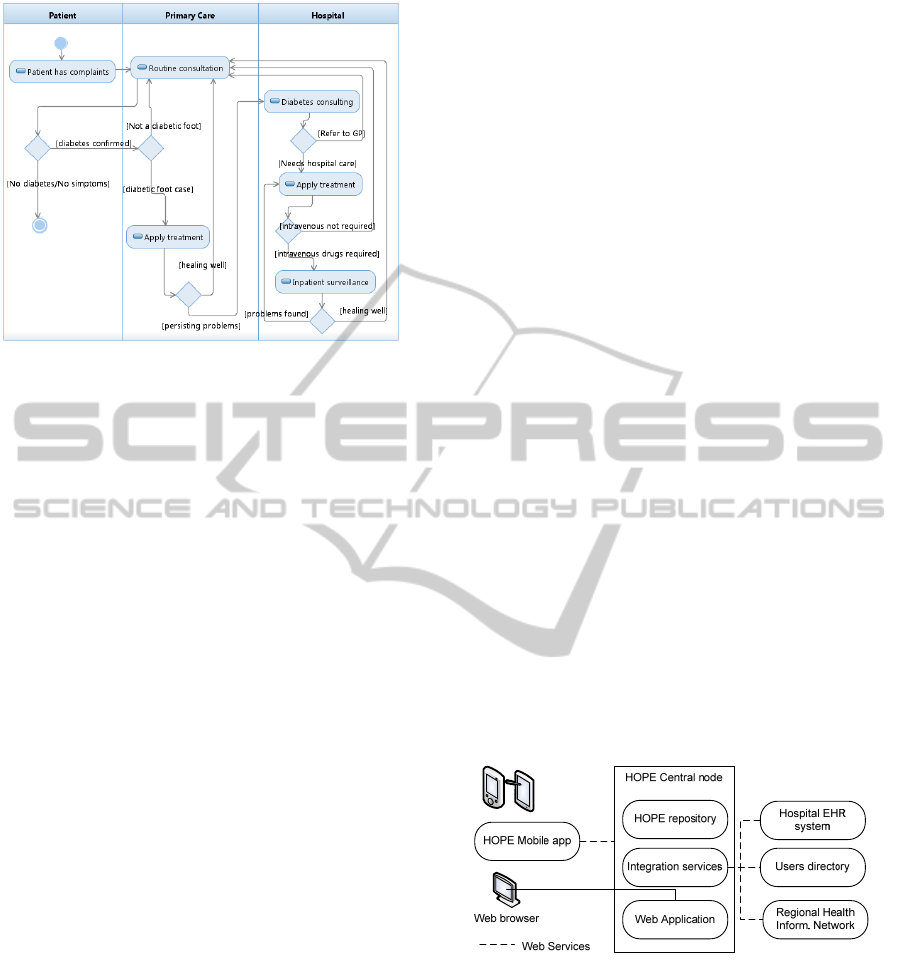
Figure 3: Diabetic foot distributed care workflow.
This clinical case brings a complying need for
visual evidence that can be supported by
smartphones. In addition, it requires a distributed,
collaborative workflow, which gave us the
opportunity to integrate the mobile application in the
more comprehensive Regional Health Network
(Oliveira et al, 2011).
2.3 Mobile Usability Requirements
The acceptance of mobile devices in care practice is
heavily connected to the practicability and user-
friendliness of the solutions (Stevenson et al., 2010);
(Andersen et al., 2009). Factors such as the small
screens size, tolerance to wireless network
availability and energy-aware applications become
essential requirements in software conception. In
this sense, the following design options have show
to play a significant role on HOPE acceptance:
Elimination of free text fields. Data entry is
based on values selected from close lists (Fig. 2).
When and if a note taking approach is necessary
then the nurse has the ability to record an audio note
(and later transcribe it to the desktop system).
Prompt visual field validation. Extensible field
validation is implemented to ensure robust data
entry. Inconsistencies in fields (e.g.: values out of
range) are visual marked by changed the field
background colour, a much less intrusive alarm than
popping message boxes (Fig. 2).
Automatic persistence and recovery. The nurse’s
work is being continuously persisted and can be
recalled at any point, especially in case of battery
failure.
Full support for on-line and off-line operation.
Although some features can only be completed in
the presence of network connectivity (e.g.: submit
the patient assessment), the overall operation is
available in off-line mode. Besides being battery-
savvy, this approach is required to tolerate the
intermittence of wireless coverage along the
Hospital.
Touch-based interactions. User interfaces were
optimized for stylus-less operations, allowing the
use of a finger as the main pointing and data entry
“device”.
Non-blocking operations. Potential lengthy
operations, such as data synchronization with the
central node, use non-blocking calls (multi-threaded)
avoiding the nurse to wait for the device to continue
the work.
2.4 System Architecture
The HOPE mobile application is implemented in
Windows Mobile and Android smartphones for data
recording and image acquisition. These are native
applications, programmed from the scratch for each
target platform with the standard SDK. The mobile
device is also used for local visualization (to access
previously entered information).
Besides the mobile application module, the
HOPE system relies on a Central node for collecting
the uploaded information and acting as a proxy to
the several Hospital Information systems. The
Central node includes the following modules: the
HOPE repository, Integration Services and the Web
application.
Figure 4: Modular system architecture.
The Repository holds the database specific to
support the HOPE workflows, like persisting the
wounds images. The Integration Services dialog
with the surrounding enterprise systems, namely to
authenticate nurses against the organization
reference Directory system and to retrieval patient
demographics. Integration services also handle the
interaction with the Regional Health Information
Network for the diabetic foot distributed workflow,
acting as a provider for the wounds information, and
SUPPORTING NURSING CARE ASSESSMENT PROTOCOLS WITH SMARTPHONES
83

a consumer, for patient and professionals
identification.
The Web Application module extends the mobile
device capabilities, providing helper tools to analyze
the captured images and a friendly environment to
explore wounds information in the diabetic
consulting (Fig. 4).
The interaction between the smartphone and the
central module is based in standard Web Services
which allows several smartphone operating systems
to be used. The interaction between the Central node
and the Hospital Information Systems and the
Regional Information Network is also based on the
Web Services stack.
Figure 5: Diabetic foot wounds images captured with the
smartphone (for the same patient) in two different
consultations.
2.5 Pictures Use in Skin Integrity
Monitoring
HOPE support to carry skin integrity and wounds
monitoring is included in two stages:
1) At the point of care, the nurse can take several
pictures of the region of interest which will be
associated with a particular patient and assessment
event. The nurse can do a basic review, for example,
to reject unsatisfactory photos. The body area being
considered is marked on the full body map,
facilitating an overview of the existence of photos, if
any (Fig. 6). Pictures from several assessment
moments (e.g.: several days) will be available for
visualization in the smartphone as in the desktop
(web module).
2) Additional features are available outside the
smartphone, once the data has been synchronized
with the Central node. A web-based application
(HOPEweb) will allow the nurse to do basic
measurements and picture annotation (Fig. 7).
The measuring method in use does not require any
special hardware nor imposes picture acquisition
constraints. In fact, it is meant to work with of the
shelf mobile phones and tolerate variability in
picture quality standards. The nurse will place a
reference object in the same plan of the wound and
take a picture of these two elements with the smart
phone camera orthogonally aligned. Afterwards, in
the web module, the nurse or other professional will
identify the reference object and the system will
calculate measurements and areas of wounds based
on its size. The goal is not to supply a full wound
measurement solution, like in (Bowling et al., 2009),
but basic support for nursing care, in which the user
has to delimitate the areas of interest interactively.
2.6 Security Issues
The storage of EHR in mobile devices raises
concerns on patient data security and privacy (Lu et
al., 2005). In this context, the HOPE system is not
used for storing clinical data, except for the period
while the data has been recorded but not yet
uploaded.
Figure 6: Overview of the body locations documented
with photos (text labels indicate the type of wound being
signaled). Similar maps are used in the mobile device and
web application (the later being dislayed).
Figure 7: Wound measurement support using a reference
object and interactive user delimitation of areas. Pictures
can be organized in series for easy comparison.
HOPE uses the device memory card as the
HEALTHINF 2012 - International Conference on Health Informatics
84

primary storage device (although it can operate
without it). This may support scenarios towards the
individual assignment of storage tokens (memory
cards) to staff members. The physical association
between professionals and storage tokens may help
on raising users’ confidence, especially for settings
in which the smart phone itself can be shared among
professionals. Note, however, that separation of user
contexts is already implemented by Access Control
Lists associated to nurses’ logins.
3 RESULTS
The HOPE system has been deployed in two
Hospitals, in Portugal. In each Hospital, a pilot users
group was formed, with volunteer nurses. Although
at an early stage of introduction, it was possible to
validate the entire workflow, including the
integration with the external Hospital-wide
information systems (different at each organization).
For this validation, a group of twelve nurses from
medical awards is being involved in pilot used. The
nurses are asked to use the mobile application to
search for a patient, collect the answers to a short
clinical interview and document skin lesions with
photos. In the present stage, nurses’ feedback is
being collected by a key domain user, which is a
nurse which received extensive train on the
application; he supports his peers and informally
collects usage feedback. A more formal and
extensive assessment is required, and structured
questionnaires will follow.
Preliminary observation of execution times
doesn’t reveal relevant speed-ups in care
documentation activities using HOPE. Other
benefits, however, have been perceived and reported
by the pilot users. The ability to browse previous
information and to record the nursing protocols at
the point of care (by the patient) is referred as the
main benefit of the system. The HOPE solution was
found to provide a more practical user interaction
and bears the potential to reduce documentation
omissions induced by deferring data entry.
The pilot use of the skin integrity monitoring in
HOPE has raised the awareness of this kind of tool
for clinical applications in both Hospitals. The
specific case of diabetic foot monitoring with a
regional scope is being piloted. (Fig. 5).
Work in progress includes collecting further
evidence that HOPE can provide a safer and more
productive environment for nursing care, besides the
existing pilot users group.
4 CONCLUSIONS
The HOPE system has successfully introduced off-
the shelf smartphones in nursing practice. A key
issue towards system acceptance was the careful
selection of the subset of the information to be
supported in the device, along the synchronization
with Hospital central systems, including the patient
EHR. The novel use of the built-in camera allows
for skin integrity monitoring along several days for
inpatients, establishing basic tools for wounds
evolution assessment.
Besides the use of the HOPE system for inpatient
nursing care, the system is being used also in multi-
institution nursing protocols, such as the diabetic
foot, for longitudinal documentation of wounds
assessment.
ACKNOWLEDGEMENTS
The authors would like to acknowledge the fruitful
collaboration of the Hospitals’ staff, both and HSS
(Feira) and HIP (Aveiro) and the technical
contributions from J. Ribeiro and J. C. Santos.
REFERENCES
Andersen, P., Lindgaard, A. M., Prgomet, M., Creswick,
N. and Westbrook, J. I. 2009. Mobile And Fixed
Computer Use By Doctors And Nurses On Hospital
Wards: Multi-Method Study On The Relationships
Between Clinician Role, Clinical Task, And Device
Choice. J Med Internet Res, 11, E32.
Berglund, M., Nilsson, C., Révay, P., Petersson, G. and
Nilsson, G. 2007. Nurses' And Nurse Students'
Demands Of Functions And Usability In A Pda.
International Journal Of Medical Informatics, 76,
530-537.
Bowling, F. L., King, L., Fadavi, H., Paterson, J. A.,
Preece, K., Daniel, R. W., Matthews, D. J. and
Boulton, A. J. M. 2009. An Assessment Of The
Accuracy And Usability Of A Novel Optical Wound
Measurement System. Diabetic Medicine, 26, 93-96.
Ebner, C., Wurm, E. M., Binder, B., Kittler, H., Lozzi, G.
P., Massone, C., Gabler, G., Hofmann-Wellenhof, R.
and Soyer, H. P. 2008. Mobile Teledermatology: A
Feasibility Study Of 58 Subjects Using Mobile
Phones. Journal Of Telemedicine And Telecare, 14, 2-
7.
Garrett, B. and Klein, G. 2008. Value Of Wireless
Personal Digital Assistants For Practice: Perceptions
Of Advanced Practice Nurses. Journal Of Clinical
Nursing, 17, 2146-2154.
SUPPORTING NURSING CARE ASSESSMENT PROTOCOLS WITH SMARTPHONES
85

Häyrinen, K., Saranto, K. and Nykänen, P. 2008.
Definition, Structure, Content, Use And Impacts Of
Electronic Health Records: A Review Of The
Research Literature. International Journal Of Medical
Informatics, 77, 291-304.
Istepanian, R., Laxmiarayan, S. and Pattichis, C. 2006. M-
Health Emerging Mobile Health Systems, Springer.
Kossman, S. P. and Scheidenhelm, S. L. 2008. Nurses'
Perceptions Of The Impact Of Electronic Health
Records On Work And Patient Outcomes. Cin-
Computers Informatics Nursing, 26, 69-77.
Lu, Y.-C., Xiao, Y., Sears, A. and Jacko, J. A., 2005. A
Review And A Framework Of Handheld Computer
Adoption In Healthcare. International Journal Of
Medical Informatics, 74, 409-422.
Oliveira, I. C. and Cunha, J. P. S. Integration Services To
Enable Regional Shared Electronic Health Records.
In: Moen, A., Andersen, S. K., Aarts, J. and Hurlen,
P., Eds. User Centred Networked Health Care -
Proceedings Of Mie 2011, 2011 Oslo, Norway. Ios
Press, 310-314.
Pirris, S. M., Monaco, E. A. and Tyler-Kabara, E. C.,
2010. Telemedicine Through The Use Of Digital Cell
Phone Technology In Pediatric Neurosurgery: A Case
Series. Neurosurgery, 66, 999-1004.
Stevenson, J. E., Nilsson, G. C., Petersson, G. I. and
Johansson, P. E., 2010. Nurses' Experience Of Using
Electronic Patient Records In Everyday Practice In
Acute/Inpatient Ward Settings: A Literature Review.
Health Informatics Journal, 16, 63-72.
HEALTHINF 2012 - International Conference on Health Informatics
86
